
Abstract
Introduction:
Gait speed provides an integrated index of physical performance; changes in gait speed could reflect deterioration in the underlying medical disorder or a response to medical/surgical interventions. Slower gait speeds reflect the overall level of impairment, especially in patients with chronic lung disease.
Methods:
We retrospectively reviewed the medical files of 119 patients who completed the pulmonary rehabilitation program at the University Medical Center in Lubbock, Texas, and collected demographic, pulmonary function, and 6-minute walk test information. Gait speed was calculated using the 6-minute walk test information.
Results:
The patients in this study had a mean age of 68.8 ± 10.1 years. Most patients (95) had chronic obstructive pulmonary disease/asthma. The mean forced expiratory volume in the first second of expiration (FEV1) was 1.3 ± 0.7 L (47.2% ± 19.7% predicted). The baseline gait speed was 41 ± 15 m/min before rehabilitation and 47 ± 15 m/min after rehabilitation. Baseline gait speed, body mass index, and FEV1 predicted postrehabilitation gait speed (P < .05 for each variable). Ten patients had a gait speed >60 m/min before rehabilitation; this number increased to 29 postrehabilitation. Using multivariable analysis, it was found that only the baseline gait speed predicted a speed of more than 60 m/min postrehabilitation. Seventy-four patients had an increase in 6-minute walk distance of greater than 30 m.
Conclusions:
Patients with chronic lung diseases have slow gait speeds. Most patients improve their speed with rehabilitation but do not increase their speed above 60 m/min and remain frail by this criterion. However, the majority of patients increase their walk distance by 30 m, a distance that represents a minimal clinically important distance.
Introduction
Comprehensive pulmonary rehabilitation improves exercise performance and health-related quality of life and reduces the frequency of hospitalization and health care costs. 1 In exercise testing methods, bicycles, treadmills, and/or simple walking can be used. Potential outcome measurements include the maximum workload, maximum oxygen consumption (VO2 max), a constant rate endurance test set at a percentage of peak work, 6-minute walk distance, and lower extremity strength testing. Gait speed measurements provide a simple method for patient testing, largely independent of time and setting. Studies with older community-based patients have demonstrated that gait speed measurements are good predictors of the development of disability, institutionalization, and hospitalization. 2,3 Patients with chronic lung disease have reduced gait speed. Pulmonary rehabilitation increases the 6-minute walk distance and therefore gait speed in many participants.
We undertook this study to determine the average gait speed of participants in our pulmonary rehabilitation program and the effect of rehabilitation on gait speed. This information should help us characterize both our patients and outcomes with our current rehabilitation program. In addition, baseline demographic and functional parameters were analyzed to identify the possible predictors of significant improvement in gait speed, which might relate to long-term prognosis.
Methods
Patients
This study included all patients who completed pulmonary rehabilitation at the University Medical Center in Lubbock, Texas, in 2010, 2011, and in the first half of 2012. These patients were referred to the rehabilitation center by their private physicians and met Medicare criteria for eligibility for pulmonary rehabilitation. The data set included all patients who completed at least two 6-minute walk tests and did not limit patient selection to particular diagnoses. We collected information on demographics, medical diagnoses, current symptoms (dyspnea), pulmonary function, and comorbidity (Charlson index). The dyspnea index was taken from the Guidelines for Pulmonary Rehabilitation. 26 There are 14 questions about dyspnea in routine situations, ranging from “at rest” to “walking up a hill” with responses ranging from 1 (minimal) to 4 (unable to do). During each rehabilitation session, vital signs and machine times were recorded. Patients exercised on treadmills, stationary bicycles, arm ergometers, and recumbent stair steppers. The program was individualized to obtain optimal performance and endurance; in general, the goal was to exercise for at least 40 minutes in total on the 4 exercise modalities. Patients also did exercises with light arm weights and participated in educational sessions. Patients completed 6-minute walk tests at the beginning of the rehabilitation program, every 4 weeks during the program, and at completion of rehabilitation. The 6-minute walk protocol followed the guidelines recommended by The American Thoracic Society. 4 The patients walked at their usual walking speed and were told that they should walk as far as possible during the test. The distance was recorded in feet, and the gait speed was calculated using the time and the distance after conversion into meters and reported as meters per minute (m/min). This study was approved by the Institutional Review Board at Texas Tech University Health Sciences Center in Lubbock, Texas.
Analysis
Descriptive information was analyzed using means ± standard deviations, medians with interquartile ranges, or counts and percentages. Comparisons between groups were made with t tests, paired t tests, or chi-square tests. Multivariable regression was used to predict gait speed after rehabilitation; logistic regression was used to predict which patients would have a gait speed ≥60 m/min after rehabilitation. These data were analyzed with SPSS version 20 (IBM, Inc, Armonk, New York). P values ≤ .05 were considered statistically significant.
Results
This study included 119 patients with a mean age of 68.8 ± 10.1 years. In all, 62 (52.1%) patients were men, and most patients (95; 79.8%) had obstructive airway disease (chronic obstructive pulmonary disease [COPD]/asthma). Other diagnoses included pulmonary fibrosis (14; 11.8%), obstructive sleep apnea (7; 5.9%), and miscellaneous diagnoses (3; 2.5%). The mean forced expiratory volume in the first second of expiration (FEV1) was 1.3 ± 0.7 L (47.2% ± 19.7% predicted). The mean comorbidity index was 0.92 ± 1.0. Ninety-seven percent of the patients reported significant dyspnea with median scores of 24 (interquartile range 16-33). The mean time in rehabilitation was 19.3 ± 7.4 weeks; this time included absences due to acute illness and unavoidable personal and family responsibilities. There were no differences between patients with asthma/COPD and patients with other diagnoses in age, comorbidity, and baseline walk distance (P value > .05 for all comparisons by t tests). Patients with COPD/asthma did have lower FEV1 percentage predicted values and lower body mass indices (BMIs; both comparisons with P values < .05; data not shown).
Baseline and postrehabilitation 6-minute walk distances, gait speeds, and exercise times are reported in Table 1.The mean gait speed increased from 41 ± 15 m/min to 47 ± 15 m/min. The factors that predicted postrehabilitation gait speed are listed in Table 2. Figure 1 depicts the changes in gait speed after rehabilitation plotted against the baseline gait speed unadjusted for other factors. A least squares linear regression line through these points indicates that patients with the slowest initial gait speeds had the largest increases in gait speed postrehabilitation (β = −.363/1 m/min increase in baseline speed; P < .001), but this effect was small. Ten patients had a gait speed of more than 60 m/min at the start of rehabilitation; 29 patients had a gait speed >60 m/min after rehabilitation (P < .001). We choose this number as an index of frailty, meaning that patients above this level were less likely to be classified as frail. Univariate analysis of factors associated with an increase in gait speed to more than 60 m/min is reported in Table 3. Multivariable logistic regression demonstrated that only the initial gait speed predicted an increase of more than 60 m/min (odds ratio 1.22, 95% confidence limits 1.11-1.34, P < .001). In all, 74 (62.2%) patients had a 30-m increase in 6-minute walk distance, and 74 also had a 50-m increase in walk distance after rehabilitation.
Functional Characteristics of Patients.
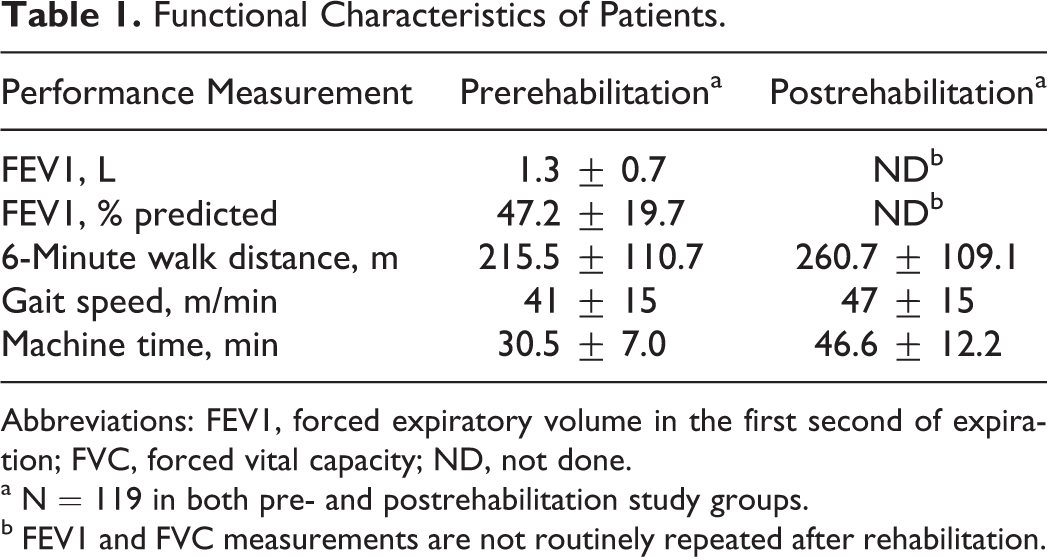
Abbreviations: FEV1, forced expiratory volume in the first second of expiration; FVC, forced vital capacity; ND, not done.
a N = 119 in both pre- and postrehabilitation study groups.
b FEV1 and FVC measurements are not routinely repeated after rehabilitation.
Predictors of Postrehabilitation Gait Speed.

Abbreviations: BMI, body mass index; FEV1, forced expiratory volume in the first second of expiration; rehab, rehabilitation.

The change in gait speed at the end of rehabilitation in meters per minute against the baseline gait speed in meters per minute.
Univariate Analysis of Factors Associated With an Increase in Gait Speed of More Than 60 m/min.

Abbreviations: BMI, body mass index; FEV1, forced expiratory volume in the first second of expiration.
Discussion
Our patients had a mean age of 69 years, severe chronic lung disease with a low average FEV1, and slow gait speeds, which placed them in the frail category used for geriatric assessments. They completed rehabilitation with increase in 6-minute walk distances, in gait speeds, and in time spent exercising during rehabilitation sessions. Most patients still had gait speeds <60 m/min after rehabilitation. However, 62% had an increase in walk distance of 30 m or more which has been considered a minimal clinically important distance in a study that evaluated survival in a COPD cohort. 5,6 This difference in criteria thresholds may indicate that the threshold of 60 m/min is not obtainable for many patients with chronic lung disease. Therefore, they remain frail and limited but might have improved outcomes based on survival.
Gait speed increases with height, lower extremity strength, and VO2 max and decreases with age, the presence of depressive symptoms, and poor physical health status. 7 Buchner reported that the mean gait speed in 152 community-dwelling adults (aged 68-85) was 79 ± 11 m/min and that fitness had a limited effect on gait speed. 6,7 The study also demonstrated that depression and poor health status, reflected in the Sickness Impact Profile Physical Dimension score, negatively impacted gait speed. Patients completing 6 months of exercise in this community-based project had no increase in gait speed. Lopopolo et al did a meta-analysis of studies on therapeutic exercise in community-dwelling older adults and concluded strength training, combination training (aerobic plus other), high-intensity training, and high-dosage training all increased gait speed, but the correlations were low (all rs < .2). 8 Patients in our rehabilitation program showed multiple differences from these healthy community dwellers, including slow gait speeds, more comorbidities, and reduced health-related quality of life (unpublished data: Chok Limsuwat, MD, January 15, 2014). However, they did increase their gait speeds with aerobic training during pulmonary rehabilitation.
Patients with chronic lung disease have respiratory limitations that correlate with reduced exercise capacity. They have reduced FEV1s and dynamic hyperinflation during walking and often require a significant fraction of their VO2 max for routine activities. 9 –12 They also have frequent comorbidity, including cardiac disease, muscle atrophy, depression, and anxiety, which also reduces physical performance. Vivodtzev et al evaluated 92 patients with COPD to determine factors that influenced their constant work rate exercise cycling time. 13 Multivariate analysis demonstrated that the oxygen consumption per unit time (VO2) at the inflection point of the VO2-VCO2 relationship and leg fatigue scores predicted endurance time but only explained 25% of the variability in the model. Troosters et al studied rehabilitation in patients with COPD and found that the major factor predicting no improvement (defined by less than a 25% increase in walk distance) was respiratory limitation based on the ratio of ventilation to maximum voluntary ventilation. 14 We evaluated our patients by measuring changes in gait speed, with increase of more than 60 m/min and increase of more than a minimal clinically important difference. Only 25% of patients had a final gait speed of more than 60 m/min, but 62% had a 30-m increase in walk distance. These results indicate that the clinical anchor used to evaluate rehabilitation has an important effect on this assessment. Many of our patients meet frailty criteria and likely remain frail after rehabilitation. Frail patients with COPD have increased mortality. 15 Consequently, this frailty construct helps evaluate patients and may identify additional opportunities for intervention. Unfortunately, frailty indices do not have uniform criteria and are difficult to apply in routine patient care. 16
Several protocols can provide reliable estimates of gait speed, and the distances used vary from 4 to 10 m to the distance traveled during the 6-minute walk test. The 6-minute walk test provides an overall measure of gait speed during routine walking and is a measure of aerobic fitness. Gait speed and distance are mathematically related; gait speed provides a simpler test approach and has been used in multiple studies on frailty. The gait speed during the 6-minute walk test is similar when calculated during the1- to 2-minute interval, the 3- to 4-minute interval, and the 5- to 6-minute interval, suggesting that the walking pace during this test is remarkably constant. 17 The gait speed measured during a 4-m walk correlates well with a 10-m walk and a 6-minute walk; the gait speed measured in a 6-minute walk correlates well with the gait speed measured during a timed Get Up and Go test. 18 –20 Ilgin et al calculated gait speeds from 6-minute walks and reported that it correlated with the severity of COPD, health-related quality–of-life questionnaires, dyspnea severity, and leg fatigue. 21 Kon et al measured gait speed in patients with COPD over 4 m and found remarkable variability in gait speed at any given level of pulmonary function measured by the FEV1. 19 Consequently, gait speed provides a performance index that is not easily predicted by spirometry. Gait speed calculations are virtually always available in a clinic or rehabilitation setting, and Ilgin et al suggest that clinicians and investigators need to correlate these measurements with morbidity, mortality, and treatments effects, including rehabilitation and corticosteroids. The speed measured using shorter distances can reasonably be extrapolated to the 6-minute walk distance for other comparisons, if needed.
Many studies in patients with chronic lung disease have used the 6-minute walk test for functional assessment. This test presents practical difficulties because of the time required and the need for additional health care workers to make these measurements either in clinic or at a pulmonary function laboratory. A 10-m walk test provides an excellent method for measuring functional status in clinic patients. Peters et al compared gait speeds over both 4 and 10 m and found excellent test–retest reliability and a high correlation between the 2 tests in healthy older adults. 22 These investigators recommended the 10-m walk as the most valid assessment for a 1 time indicator of health status. Karpman measured the time required for a 4-m test in an outpatient clinic. 23 This test required approximately 90 seconds to complete and had a high level of acceptability by both clinic staff and patients. Short walk tests have been used in multiple clinical disorders with functional impairment. For example, Dalgas et al reported a strong correlation between walking speeds measured over 10 m and a 6-minute walk in patients with multiple sclerosis and stroke. 24 Hobart et al reported a 20% improvement in gait speed of more than 25 feet was clinically meaningful in patients with multiple sclerosis. 25 Finally, gait speed based on short distances is a good predictor of future problems with disability and institutionalization. 2
Our study has some limitations. This study population included only patients who completed rehabilitation. We do not have information on patients who were referred to rehabilitation and either declined to participate or did not complete the rehabilitation program. The study population was heterogeneous and was analyzed as 1 group. However, both patient groups (with obstructive airway disease and other diagnoses) showed significant increase in gait speed. Our study population showed relatively slow gait speeds, which reflect the severity of their diseases, but this study population probably represents the typical patients referred to rehabilitation. Finally, gait speed was measured over a longer distance unlike the distances used in geriatric studies, but gait speeds are fairly uniform during 6-minute walks and correlate well with speeds measured over shorter distances.
Conclusions
Our patients did have an increase in gait speed and walk distance during pulmonary rehabilitation. Patients with higher FEV1s had larger increases in gait speed during rehabilitation; patients with increased BMIs had less improvement during rehabilitation. These factors suggest that weight loss and improved airway function might improve rehabilitation outcomes. Gait speed measurements provide a good method to measure performance during rehabilitation and should probably be measured frequently using a 10-m protocol for convenience to monitor progress. Patients who do not improve within 4 weeks need reassessment to evaluate their cardiopulmonary limitations.
Footnotes
Authors’ Note
This article was presented by Ryan McClellan in a meeting at Southern Society for Clinical Investigation, New Orleans, Louisiana, February 22, 2013.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.