
Abstract
Qualitative and descriptive studies suggest that school nurses can help mitigate student absenteeism. However, rigorous empirical evidence supporting specific attendance-related nursing activities is limited. Therefore, we conducted a clustered randomized controlled trial among 84 urban elementary schools to assess the cost-effectiveness of forming separate online communities of practice (CoPs) for licensed practical nurses (LPNs) and registered nurses (RNs) to improve student attendance. Using the ingredients method, we estimated average implementation costs of $764 per LPN school and $896 per RN school. Multilevel regression indicated statistically significant reduced odds of chronic absenteeism for all students (and a subgroup with chronic health conditions) and practically significant increased attendance for all students in LPN treatment versus control schools, but no significant RN CoP effects. Findings suggest online school nursing CoPs are a potential low-cost, light-touch approach to reduce student absenteeism, given context-appropriate structure, content focus, and adequate nurse participation.
Keywords
A growing consensus of educators, researchers, and policymakers has expressed alarm over a rise in chronic absenteeism (e.g., Cardona, 2024; Dee, 2024; Gee et al., 2023; Lee et al., 2023; The White House, 2023). Defined as missing at least 10% of the school year, chronic absenteeism is both an indicator and cause of many adverse educational and health outcomes among youth (Rankine et al., 2021). School nurses can play a critical role in fostering increased attendance by preventing and treating health conditions and ensuring that schools are safe and healthy environments (Darnell et al., 2019). The National Association of School Nurses (NASN, 2023) suggests that school nurses can help mitigate chronic absenteeism by following guidance for best practices and priority activities outlined in the organization’s recently updated School Nursing Practice Framework (Tanner et al., 2024). Support for their position comes from qualitative (Lee et al., 2023; Rankine et al., 2021), feasibility (Maughan et al., 2023), and case studies (Arimas-Macalino et al., 2019) that emphasize the importance of nurse participation on school attendance teams and standardized, data-driven practices situated in the Framework’s four domains: care coordination, leadership, quality improvement, and community and public health.
The NASN (2021) further argues that performing Framework-aligned school nursing practices minimally requires a bachelor-trained registered nurse (RN) license. Their rationale is that typical RN associate degree or licensed practical nurse (LPN) diploma programs do not fully prepare licensed nurses for the complexities of school nursing. Although LPNs comprise nearly 18% of school nurses in the United States, Willgerodt et al. (2024) suggest relying on LPNs can negatively impact long-term student outcomes due to their limited scope of practice (e.g., LPNs cannot formulate nursing diagnoses or modify care plans). Nonetheless, empirical support for the precise role of school nursing activities and licensure in improving attendance remains tenuous, largely owing to weak study designs and lack of rigor (Best et al., 2018; Yoder, 2020).
Among the more rigorous descriptive studies, Darnell et al. (2019) and M. A. Gottfried (2013) both found positive effects of nurse presence on student attendance; however, neither reported nurse licensure. In a recent cost-effectiveness analysis (CEA) of an LPN-based school nursing program, Leach et al. (2023) found no effects of nurse presence on student attendance or chronic absenteeism despite significant costs. Leach et al. (2023) attributed their findings partly to sparse LPN training in care coordination and leadership—areas in which school nurses typically devote nearly 60% of their time (Willgerodt et al., 2024). Overall, we have a limited understanding of the costs and effects of school-based LPNs vs. RNs on student outcomes, and the focus on nurse presence provides little practical guidance for improving student attendance (Leach et al., 2023). In general, despite a scholarly and professional emphasis on evidence-based school nursing practices (e.g., NASN, 2021, 2023; Resha, 2020; Shannon & Maughan, 2020; Tanner et al., 2024), empirical evidence supporting specific nursing activities and practices for improving student attendance and chronic absenteeism is scarce (Best et al., 2018; Leach et al., 2023; Rankine et al., 2021; Yoder, 2020). Thus, researchers have called for rigorous experimental study designs with large, representative student samples to further our understanding of school nurses’ role in addressing student attendance outcomes (Best et al., 2018; Leach et al., 2023; Yoder, 2020).
Communities of practice (CoPs) represent a potential approach for school nurses to collectively strengthen their practice (Mazyck et al., 2014). Wenger-Trayner et al. (2023, p. 11) define CoPs as “groups of people who share a concern or a passion for something they do and learn how to do it better as they interact regularly.” Nursing CoPs can foster knowledge sharing, forming a common professional identity and improving practice (Andrew et al., 2008). Swaithes et al. (2023) argued healthcare CoPs can overcome implementation obstacles through equitably mobilizing knowledge to develop solutions to problems of practice. To the extent that school nursing CoPs bolster implementing Framework-aligned best practices, especially those expected to improve attendance (e.g., Rankine et al., 2021), nurse participation may improve care delivery (e.g., Hennein et al., 2022), thereby reducing the academic impacts of student health conditions.
Online CoPs have become more prevalent in healthcare sectors, including nursing (Rolls et al., 2020), for overcoming geographical and cost barriers to sharing knowledge and promoting evidence-based practices (Noar et al., 2023; Shaw et al., 2022). The NASN (2024) began hosting online CoPs on its website in 2013 (Mazyck et al., 2014) and currently supports 34 online school nursing communities. Wenger-Trayner et al. (2023) suggest that online and in-person CoPs can be equally effective. Online school teaching CoPs can affect positive changes in practice (Xue et al., 2021) and may be more cost-effective than in-person formats for facilitating professional development (Ghamrawi, 2022). Unfortunately, despite the promise and prevalence of online nursing CoPs, literature reviews have noted a lack of empirical studies of nursing CoPs of any format (Terry et al., 2020; Woods et al., 2016), and we are unaware of any published studies of the academic impacts of online or in-person school nursing CoPs. In general, we have a limited understanding of the costs and effects of online healthcare-focused CoPs (Swaithes et al., 2023), and experimental studies linking healthcare CoPs to outcomes are rare (Noar et al., 2023).
To address the gaps discussed previously, we conducted a clustered randomized controlled trial (RCT) and accompanying CEA to assess the costs and effects of forming online school nursing CoPs in a sample of urban elementary schools. Specifically, we sought to identify the resource requirements and costs of implementing online CoPs in schools with an LPN or RN above and beyond those of providing an LPN or RN (without CoPs), relative to effects on student attendance and chronic absenteeism. We aimed to contribute to improved school nursing practice and help guide resource allocation decisions to promote increased student attendance by answering the following primary and secondary research questions (RQs):
RQ1. What are the resource requirements and costs of implementing online CoPs in LPN or RN schools above and beyond the costs of providing an LPN or RN? (Primary)
RQ2. How do student attendance and chronic absenteeism compare between LPN or RN schools that implement online CoPs and LPN or RN schools that do not? (Primary)
RQ3. How do attendance and chronic absenteeism for students with identified chronic health conditions compare between LPN or RN schools that implement online CoPs and LPN or RN schools that do not? (Secondary)
We expected increased attendance and reduced chronic absenteeism for all students in treatment schools, relative to control schools, with the largest effects for students with chronic health conditions in LPN CoP schools. Our hypothesis assumed that school nurses have more contact with students with chronic health conditions. We also inferred from the limited scope of LPN training and practice (e.g., NASN, 2021; Willgerodt et al., 2024) and conflicting licensure results of prior studies (e.g., Darnell et al., 2019; M. A. Gottfried, 2013; Leach et al., 2023) that LPNs may have greater potential than RNs for improving nursing practices related to student attendance.
Method
Following the Cost Analysis Standards Project (CASP, 2021), we conducted separate analyses to estimate the costs and effects of implementing the same online school nursing CoPs. Though distinct, the cost and effectiveness analyses were related. As such, we will describe common design elements before separately describing our costs and effects methods. We estimated costs using Microsoft Excel and used R (v. 4.2.0; R Core Team, 2022) for data prep, randomization, and effectiveness analyses (for more details, see the “Analytic Approach” section and supplemental materials).
Design
This study comprised a clustered RCT of online school nursing CoPs and accompanying CEA of the costs of implementing online CoPs compared with business as usual (no CoPs), relative to measured effects on student attendance and chronic absenteeism. We did not register our study; however, we proposed the study design and eight total research questions in our research grant application (available online; see “Funding” and “Open Practices” statements for details). Although data availability and other issues limited our ability to address five of our proposed RQs, for transparency, we describe our analytic approach, results, and limitations for the omitted RQs in Supplemental Section 1.
Data Sources
We primarily used administrative data on student demographics, test scores, and attendance collected throughout the school year per normal routines and stored in the district’s student information system, Infinite Campus. Implementation data (online meeting logs, health manager’s session notes, and staffing agency invoices) and cost-related surveys of school nurse CoPs participants supplemented our administrative data.
Study Timeline
In July 2022, we presented a rough study outline to the district’s Accountability, Research, and Systems Improvement (ARSI) division and Institutional Review Board (IRB) Chair and received permission to apply for funding. Because CoPs did not directly involve students, the district approved our experimental study design—a marked departure from the district’s past stance on RCTs (Shand et al., 2024). Although our research grant proposal integrated implementation and analysis, in practice, about one year separated the two activities (see Figure 1). CoPs implementation (November 2022–May 2023) did not include grant funding or require formal district IRB approval because only district personnel participated. Our CEA required a Board of Education–approved data-sharing agreement with our university partner and both district and university IRB approvals. We initiated those processes after the Board accepted our grant award and received our final IRB approval in November 2023. Per ARSI, we submitted a single data request for all cost and effectiveness data in February 2024 after administering the cost survey. The following month, we received the data and began conducting the CEA.

Study Timeline.
Setting
Jefferson County Public Schools (JCPS) is a large, urban public school district located in Louisville, KY. With a $2 billion annual budget, JCPS is the largest district in the state and one of the largest in the country. In 2022–23, the district’s 6,052 teachers served 93,418 students across 164 school sites. That year, the district’s students were 37% Black, 36% White, 16% Hispanic/Latino, and 11% other races/ethnicities. Roughly one in six JCPS students were multilingual learners. More than 70% of the district’s schools were eligible for Title 1 funding, and nearly two-thirds of its students were eligible for free or reduced-price lunch (FRL). Just over 19% of JCPS students had at least one recorded health condition, and 14% required an individual education program.
JCPS used pandemic stimulus funds to expand school nursing district-wide in February 2021, relying on staffing agencies to supply additional nurses beyond the pre-COVID school nursing program (n = 35). The district’s Health Services department initially planned to place an RN in every Title 1 eligible school as part of the district-wide expansion; however, agency nurse availability scuttled those plans. Instead, Health Services prioritized placing nurses in schools with the greatest health needs first and filled all vacancies with the first available agency nurse, irrespective of licensure. With few exceptions, schools assigned an LPN (RN) at the outset of the expansion also received an LPN (RN) in subsequent school years. Thus, we use the terms “LPN school” and “RN school” here to refer to the licensure of a school’s nurse at the time of the study and not a predetermined licensure status for that school. Six zone-leader advanced practice registered nurses (APRNs) supervised the LPNs and RNs in their respective zones. District and agency-employed nurses shared common, licensure-specific job descriptions (see Supplemental Section 5), workday schedules, and training requirements. JCPS expected all district and agency LPNs and RNs to provide health services based on the respective Kentucky Board of Nursing (KBN, 2024a, 2024b, 2024c) LPN or RN scope of practice and Advisory Opinion Statement on Roles of Nurses in School Nursing Practice. JCPS adopted electronic health records (EHRs) in 2021–22 to facilitate Medicaid billing (Leach et al., 2023) and to enhance quality improvement (e.g., Davis et al., 2021) and care coordination (e.g., Baker & Gance-Cleveland, 2021). Unfortunately, EHRs were never fully implemented, and expected health data (e.g., nurse office visit and referral follow-up details) never materialized before JCPS discontinued their use in early 2024.
A retrospective CEA of the district’s 2018–19 school nursing program found no effects of LPNs on student attendance or chronic absenteeism (Leach et al., 2023). Implementation analysis revealed a lack of clear theoretical alignment between nursing practice and attendance and of standardized nurse onboarding and continuing education. Thus, Leach et al. recommended that JCPS develop an explicit theory of change (logic model) and create a corresponding standard operating procedure manual to support onboarding and continuing education of school nurses. By fall 2022, Health Services had completed and begun using both the manual and final logic model (see Supplemental Section 4). For details on the impetus of the LPN CEA and the contextual factors that enabled implementing the resulting programmatic changes, see Shand et al. (2024).
Sampling Procedure
We randomly assigned LPN and RN schools separately to treatment or control conditions using three strata: Comprehensive Support and Improvement status (CSI, non-CSI), employer (staffing agency, JCPS), and level (elementary, middle/high). CSI status is a federal designation for a state’s lowest-performing schools. CSI schools likely face different and/or additional challenges compared to non-CSI schools. We stratified by employers because agency nurses may be more transient than district employees. We stratified by level to obtain similar numbers of elementary (ES) and middle/high (M/HS) schools in the treatment and control groups. Although we initially planned to analyze both levels separately within a single study, our decision to treat M/HS as one level based on perceived similarities in nursing needs produced significant treatment vs. control group differences in enrollment and prior year health conditions, as well as imbalances in school-level composition in the M/HS sample. Variations in state testing between middle and high schools also prevented us from estimating common multilevel regression models for the ES and M/HS samples; thus, we focused here on elementary schools.
As shown in Figure 2, we excluded five elementary schools; one was part of a combined K–12 school, one switched from an LPN to an RN, one was in a transition year after a school merger, and two had no nurse assigned at the time of randomization. We excluded n = 385 students with fewer than 10 days of enrollment (e.g., Leach et al., 2023), and n = 10 students with incomplete attendance data. The total sample comprised n = 84 elementary schools (40 treatment, 44 control) consisting of n = 39,944 students (18,854 treatment, 21,900 control) in grades K–5. Each school had one nurse. A total of n = 29 of the schools had an LPN (14 treatment, 15 control). After sending out CoP invitations, we discovered a double entry for one elementary school in the spreadsheet used for the randomization, which resulted in a slightly unequal (26 treatment, 29 control) final sample of n = 55 RN schools. For consistency with Leach et al. (2023), we preferred an intent-to-treat approach, retaining treatment schools whose nurses did not participate in CoPs (see Figure 2), although we also conducted per-protocol sensitivity analyses, retaining only treatment schools whose nurses participated in CoPs, along with all control schools.

School Participant CONSORT Flow Diagram.
Communities of Practice (CoPs) Intervention
The JCPS health manager is an experienced nurse practitioner and published researcher who has sought to advance school nursing science by conducting local scholarship of practice (e.g., Resha, 2020) and disseminating generalizable research findings (e.g., Best et al., 2018). At the time of our study, the health manager had served in public school nursing for 21 years and had begun a postdoctoral fellowship centered on implementing evidence-based nursing practices. Faced with drastically increased nurse onboarding and ongoing support needs and the challenge of team building across a geographically expansive district, the health manager chose to implement online CoPs within the larger program improvement effort based on their perceived low cost, ease of implementation, and replicability. The Figure 3 logic model assumed online school nursing CoPs could foster standardized implementation (e.g., Swaithes et al., 2023) of Framework-aligned best school nursing practices, thereby improving healthcare delivery (e.g., Hennein et al., 2022). The logic model further assumed that enhanced school nursing practice resulting from CoP participation (e.g., Andrew et al., 2008; Mazyck et al., 2014) would improve student attendance outcomes (e.g., Rankine et al., 2021) through, for example, bolstering school attendance team participation and increasing student healthcare referral follow-ups.

Online School Nursing Communities of Practice (CoPs) Logic Model.
Beginning in November 2022, the health manager formed and facilitated separate LPN and RN CoPs to improve practice toward achieving a common goal (Hennein et al., 2022)—namely reducing absences. Treatment nurses received email invitations to join a common, licensure-specific CoP (one each for LPNs and RNs). The health manager encouraged CoP participation but did not mandate or incentivize nurses to join (e.g., Wenger-Trayner et al., 2023). LPNs (RNs) attended CoPs on the first and third (second and fourth) Wednesdays of each month, with occasional adjustments based on the school calendar. The health manager canceled one LPN and two RN sessions due to extenuating circumstances, and we reclassified another RN session as training. The health manager intended CoP sessions to last 30 minutes; however, all but one (an RN session curtailed because the health manager was traveling) exceeded the planned duration. Table 1 provides schedule details for the ten LPN and eight RN CoP sessions.
Communities of Practice (CoPs) Schedule for School Year 2022–23

Note. LPN = licensed practical nurse; RN = registered nurse; SP = session began with a short presentation; DR = session began with a data review; we considered RN sessions denoted by SP or DR top-down, and other RN sessions bottom-up.
Session attendance rates are based on the number of LPNs (RNs) attending divided by 14 (26) invited LPNs (RNs).
Participating RNs received an otoscope.
We treated this non-interactive state webinar attended by treatment RNs as training and not an additional RN CoP session.
Both CoPs focused on chronic absenteeism-related Framework domain components (e.g., Rankine et al., 2021) and incorporated guidance from the Model for School Nurse-Led Case Management (NASN, 2021) to improve care for students with chronic health conditions. LPN CoP sessions focused on care coordination components selected by the health manager in a top-down organizational structure (c.f., Hennein et al., 2022). Meetings began with a case study on equitably meeting students’ health care needs. LPNs discussed follow-up actions based on the study scenario and then spent the remaining time networking and sharing knowledge. RN CoP sessions covered aspects of all four Framework domains, especially quality improvement. Although the health manager initially selected topics for all eight RN sessions (i.e., top-down structure), four sessions deviated from planned content to focus instead on issues identified by the RN participants (i.e., bottom-up structure). Meetings began with a short presentation or school-level health data review (top-down) or the identification of a current problem of practice (bottom-up). Data reviews included coaching and dialogues on health disparities. Sessions closed with discussions of evidence-based action plans. The health manager documented content details and nurse time and attendance after each session. We corroborated time and attendance with corresponding meeting logs from Zoom or Google Meet.
Estimating the Costs of CoPs
To answer RQ1, we conducted separate cost analyses for LPNs and RNs. We used the ingredients method (Levin et al., 2018) to fully document the economic cost of forming CoPs in resource or opportunity cost terms, over and above the costs of typical school nursing practice (business-as-usual), with each resource—personnel time, physical facilities, materials and equipment, etc.—deemed an “ingredient” of the intervention. We analyzed administrative data on implementing CoPs, including time logs and attendance records for both CoPs and control nurses, to determine changes in time use for nurses and resources such as space and materials required above and beyond business-as-usual.
While our cost analysis relied in part on self-reported survey data, the relatively low survey response rate represents a limitation. To address this, we triangulated across multiple sources of information rather than relying solely on survey responses. In addition to the survey (see Supplemental Section 3), we incorporated administrative records on scheduled intervention time and intervention attendance records, as well as qualitative information from interviews with the JCPS health manager. For the survey-based component, we grouped respondents into high-, medium-, and low-intensity implementation categories, each representing roughly one tercile based on time reported engaged in direct CoP activities and indirect follow-up activities, with cutoffs set based on where there were sharp changes in time reported, and extrapolated average costs from each group to the full sample.
Our approach helped mitigate the effect of nonresponse, though we recognize the potential for bias if nurses who invested more time in CoPs were disproportionately likely to respond. Although approximately equal numbers of treatment and control school nurses responded to the survey, we were unable to test for differential nonresponse or engage in more sophisticated imputation based on nurse characteristics because the district IRB would not permit us to ask additional questions that would be potentially identifying. However, to test the robustness of our estimates, we conducted additional sensitivity analyses, including a bounding exercise in which we imputed the high and low time values for all missing survey responses. This produced a plausible range of total costs, allowing us to benchmark our primary estimates against more conservative and more expansive scenarios. Taken together, these steps suggest that our estimates likely represent a high estimate of the true incremental cost of CoPs, with a reported range that can help decision-makers consider how costs may vary based on levels of nurse engagement.
We also carefully considered the role of training and other induced costs. Although CoP treatment nurses reported participating in additional trainings, these were also common in the control group, suggesting they may not represent incremental costs attributable to CoPs. The main exception was an end-of-year school health webinar sponsored by the state education agency, which we included as an induced cost for RN participants. Overall, available evidence suggests that CoPs primarily shifted how nurses carried out their existing responsibilities rather than adding substantial new time burdens.
We then assigned a national average price, expressed in 2024 dollars, for each ingredient based on (a) the U.S. Bureau of Labor Statistics’ (BLS, 2022) Occupational Outlook Handbook, adjusted for inflation to 2024 prices, (b) estimates of educational facilities costs amortized over 30 years and divided into an hourly rate (Wang et al., 2020), (c) estimates of the costs to school districts of Internet access (Chang & Kushner, 2022), and (d) prices from national retailers for laptop computers and otoscopes, amortized over 5 and 15 years, respectively, at a 3% interest rate. We added fringe benefits based on BLS estimates for state and local government employees. We tabulated (a) pooled costs, (b) total costs separately for the RN and LPN treatment, (c) average cost per school, and (d) the marginal cost for adding one more LPN, including direct and induced participation costs but excluding planning and facilitation time by the health manager. Our cost spreadsheets, which include notes on prices, sources, assumptions, and adjustments, are available in the supplemental materials.
Estimating the Effects of CoPs
Measures and Covariates for Multilevel Regression Models (MLMs)
Outcome Measures
Student-level dependent variables (DVs) were 2022–23 treatment year attendance (0–100%) and chronic absenteeism (0 = no, 1 = yes).
Covariates
Student-level covariates were prior year (2021–22) attendance or chronic absenteeism; minority status (0 = no, 1 = yes); sex (female/male); FRL-eligible (0 = no, 1 = yes); special education status (0 = no, 1 = yes); multilingual learner (0 = no, 1 = yes); and health condition identified prior to 2022–23 (0 = no, 1 = yes). School-level covariates were prior year attendance or chronic absenteeism percent; health condition percent (percent of students with ≥1 prior health condition); 2022–23 need index (a weighted index of FRL [0.50], mobility [0.30], special education [0.15], and multilingual learner [0.05] percentages); 2022–23 minority percent; 2022–23 enrollment (K–5); math novice percent and reading novice percent (percent of students with the lowest rating on the 2021–22 Kentucky State Assessment). Our school-level covariate of interest for all RQ2 and RQ3 models was Treat (control, treat).
CoP Participation
The health manager kept detailed CoPs time and attendance logs. We verified time and attendance using meeting logs from Zoom or Google Meet.
Analytic Approach
Education RCTs commonly report post-randomization balance tests (e.g., Gregory et al., 2024; Hart et al., 2024; Lawson et al., 2024; Murphy et al., 2024). However, Senn (1994) argued that such tests are unnecessary and instead recommended including all predetermined covariates in subsequent analyses irrespective of statistically significant baseline differences. The recently updated Consolidated Standards of Reporting Trials (CONSORT; Hopewell et al., 2025) also discouraged post-randomization balance tests. Thus, we followed Senn’s recommendation.
We used the R package lme4 (Bates et al., 2015) to estimate separate attendance and chronic absenteeism MLMs to answer RQs 2 and 3 following the strategy used by Leach et al. (2023). First, we estimated null models (no covariates, random intercepts) and intraclass correlations (ICC1s) and computed design effects (DE), with DE > 1.5 supporting further MLM estimation per Lai and Kwok (2015). Given acceptable DEs, we next estimated random intercepts only MLMs adding student-level covariates to the null models, then MLMs adding school-level covariates to those student-level, random intercepts only covariate models, and finally random intercepts MLMs with student- and school-level covariates that also allowed student attendance or chronic absenteeism slopes to vary randomly.
Per Leach et al. (2023), we conducted an analysis of variance (ANOVA) to compare nested models (e.g., Bliese, 2022) and did not make alpha adjustments for our ANOVAs or MLMs. We used the lmer(REML = False) command during the model selection process (e.g., Bolker, 2015) for our linear mixed-effects MLMs with continuous attendance outcomes. We then obtained preferred model estimates using lmer(REML = True) and Satterthwaite-adjusted p-values from the lmerTest package (Kuznetsova et al., 2017), per Luke’s (2017) recommendation for reducing Type I errors with small samples. We used the glmer(family = binomial(logit)) command for our generalized linear mixed effects MLMs with binary chronic absenteeism outcomes. We report β coefficients for our attendance models and both β and odds ratios (ORs), i.e., Exp(β), for our chronic absenteeism models. We scaled all continuous school-level covariates in our glmer MLMs. We determined statistical significance by p < .05, although we assessed the practical significance of any coefficients of interest with p < .10 (e.g., Smith et al., 2024) based on Luke’s (2017) admonition to make an educated appraisal of MLM estimates rather than relying solely on p-values, even conservatively estimated ones, for decision-making.
Because we also wanted to estimate 95% CIs for the Treat coefficients in our MLMs, we tested assumptions of heteroscedasticity and normal distribution of residuals for our preferred final models (e.g., Winter, 2013). Although Leach et al. (2023) used the confint command to obtain profile likelihood 95% CIs for both lmer and glmer MLMs, we used the ci(ci_method = "satterthwaite") command from the R package parameters (Lüdecke, Ben-Shachar, Patil, & Makowski, 2020) to estimate 95% CIs consistent with our lmer attendance model p-values obtained from lmerTest. We preferred to “keep it maximal” (Barr et al., 2013) and estimate full-covariate MLMs consistent with Leach et al.’s (2023) approach and Senn’s (1994) recommendation to include all predetermined covariates. However, if attendance and chronic absenteeism percent were strongly correlated (|r| > .95), we included only the prior year covariate corresponding to a model’s student-level DV. For MLMs with convergence or singularity errors, we estimated reduced-covariate models based on eliminating common non-significant coefficients among MLMs used to answer a given RQ. We group (grand) mean-centered continuous student (school) level covariates.
Analytic samples and missing data
Controlling for prior year attendance, chronic absenteeism, and health conditions in our MLMs effectively excluded n = 10,429 students missing data from 2021–22 (see Table 2 for details). Similar percentages of treatment (26.13%) and control (26.09%) school students had unavailable prior-year data. These students, primarily kindergartners (n = 6,755), had not enrolled in JCPS in 2021–22 and therefore were missing all prior year data. Imputing prior year values for students missing all data, particularly health conditions, did not seem appropriate.
Missing Data and Study Attrition Information by Condition

Note. LPN = licensed practical nurse; RN = registered nurse.
Students not enrolled in the district in the 2021–22 school year and therefore missing all prior year data. All students enrolled in the district in both the 2021–22 and 2022–23 school years had complete data for both years.
Students enrolled in a treatment or control school on November 1, 2022, who did not finish the 2022–23 school year at that school.
Nurses assigned to a treatment or control school on November 1, 2022, who left that school before the end of the 2022–23 school year.
Student and nurse attrition
Table 2 shows similar percentages of treatment and control school student attrition (i.e., students enrolled in a study school on November 1, 2022, but not enrolled in that school at the end of the 2022–23 school year). We found no statistically significant differences in student attrition percentages between treatment and control schools among the LPN (t(26.58) = 1.42p = .17) and RN samples (t(50.95) = 0.27, p = .79). Nurse attrition only occurred among agency-supplied nurses and was more common in control schools (see Table 2 for details). Among the four treatment school nurses who left the district during the CoP intervention, two (one LPN, one RN) had not participated in CoPs prior to leaving, and the other two (one LPN, one RN) had participated in one session each.
Results
Costs
Based on CoPs attendance records and survey responses from roughly 25% of treatment and control group nurses, we concluded that CoPs costs were incremental to business-as-usual, because CoPs supplemented but did not displace training attended by nurses in both groups (e.g., automated external defibrillator training). We observed direct costs of CoPs participation, as well as the health manager’s planning and facilitation time, from administrative records to estimate the intent-to-treat and hypothetical (assuming full nurse participation) costs shown in Table 3. We divided by the number of schools in each condition to arrive at an average cost per school of $764 for the LPN CoP and $896 for the RN CoP. Sensitivity analyses based on extreme ranges of imputing missing cost survey responses produced costs ranging from $426 to $1,346 per school for LPNs and $358 to $1,674 per school for RNs. The supplemental cost spreadsheets provide details of all cost calculations.
Economic Costs of Forming Online School Nursing Communities of Practice

Note. LPN = licensed practical nurse; RN = registered nurse.
Effectiveness
The Figure 2 CONSORT flow diagram shows the number of LPN CoP (n = 14; 5 CSI, 7 agency nurses) and control (n = 15; 6 CSI, 9 agency nurses) schools, and RN CoP (n = 26; 4 CSI, 26 agency nurses) and control (n = 29; 6 CSI, 27 agency nurses) schools. As shown in Table 1, LPNs (M = 0.65, SD = 0.06) had higher session attendance rates than RNs (M = 0.39, SD = 0.07). Randomly assigned RNs (62%) were less likely than LPNs (71%) to participate in CoPs and averaged about two-thirds the number of sessions and minutes (see Table 4). Table 5 provides means and standard deviations of all school-level variables. Table 6 shows student demographic information for the combined sample (n = 39,944 students). As seen in Table 7, school-level attendance and chronic absenteeism percent were strongly correlated (r = −.99); therefore, we included only the one corresponding to the student-level outcome for each model. DEs ≥ 2.99 and ICC1s between .05 and .11 for all null models respectively supported MLM (Lai & Kwok, 2015) and suggested small to medium effects (LeBreton & Senter, 2008). See Supplemental Section 2 for DEs, ICC1s, and student demographic information for the LPN (n = 10,074 students; 5,183 treatment, 4,891 control) and RN (n = 19,941 students; 8,744 treatment, 10,697 control) analytic samples.
Nurse Participation in School Year 2022–23 Communities of Practice by Licensure

Note. LPN = licensed practical nurse, RN = registered nurse.
School-Level Descriptive Statistics by Condition (n = 84 schools; 40 treatment, 44 control)

Note. M = mean; SD = standard deviation.
Student-Level Demographics by Condition (n = 39,944; 18,854 treatment, 21,090 control)

Note. M = mean; SD = standard deviation; FRL = free- or reduced-price lunch eligible.
Means, Standard Deviations, and Correlations for School-Level Covariates (n = 84 schools)

Note. M = mean; SD = standard deviation.
p < .05.
RQ2
Table 8 provides results of model fit tests for the licensure-by-outcome models used to answer RQ2. Table 9 reports our preferred LPN and RN attendance and chronic absenteeism MLMs. Students in LPN CoP schools had a statistically significant 15.63% reduction in the odds of chronic absenteeism (OR = .84, β = −.17, SE = .07, 95% CI [−.30, −.03], p = .01) compared to control school students. This result was robust to reduced-covariate (OR = 0.84, β = −0.17, SE = 0.07, 95% CI [−0.31, −0.03], p = .01) and per-protocol (OR = 0.82, β = −0.20, SE = 0.07, 95% CI [−0.33, −0.06], p = .003) sensitivity analyses. See Supplemental Section 2 and Table S4 for details of reduced covariate (excluding health condition percent, need index, and math novice percent) and per-protocol (excluding non-participating CoP schools) analyses.
ANOVA Results by RQ2 Outcome for LPN (n = 10,074) and RN (n = 19,941) Samples

Note. LPN = licensed practical nurse; RN = registered nurse. Preferred models in
Attendance models used lmer(REML = False) for model comparisons reported here and lmer(REML = True) to obtain estimates reported in Table 9.
Student level attendance or chronic absenteeism slopes allowed to vary randomly.
Tests whether including Treat in the preferred model improved model fit for preferred models where Treat was statistically significant (see Table 9 for model details).
p < .05
Multilevel Model Results for LPN (n = 10,074) and RN (n = 19,941) Samples

Note: LPN = licensed practical nurse; RN = registered nurse; β = regression coefficient; SE = standard error; SD = standard deviation; AIC = Akaike information criterion; BIC = Bayesian information criterion.
Group mean-centered.
Grand mean-centered.
p < .10, *p < .05.
LPN treatment school students also had higher attendance (β = 0.33, SE = 0.19, 95% CI [−0.04, 0.71], p = .098) than their LPN control school peers. Although the attendance coefficient was not statistically significant, it met Smith et al.’s (2024) threshold for assessing practical significance (i.e., p < .10). The point estimate in our most conservatively estimated (REML = T, Satterthwaite-adjusted p-values; Luke, 2017) full-covariate model suggests a .58-day increase in attendance for all students in LPN CoP schools based on a typical 175-day school year. This effect is robust to conservatively estimated reduced-covariate (β = .35, SE = .18, 95% CI [.004, .70], p = .06) and per-protocol (β = .39, SE = .23, 95% CI [−.06, .83], p = .11) sensitivity analyses. As seen in Supplemental Table S4, less conservative model estimation (REML = T; often preferred per Bates, 2025) and/or reporting only 95% CIs in lieu of p-values, especially profile likelihood 95% CIs (suggested by Lüdecke, Ben-Shachar, Patil, Waggoner, & Makowski, 2020), affects the actual (p < .05) or implied (95% CI excluding zero) statistical significance of the Treat coefficient. Notably, the CoP treatment effect remains relatively stable across various model specifications and sensitivity analyses (.32 < βTreat < .39; i.e., attendance gains between .56 to .68 days). These gains are consistent with statistically significant results reported from other low-cost and/or light-touch attendance intervention RCTs (e.g., .13 days, Rogers et al., 2017; .40–.45 days, Himmelsbach et al., 2021; .50–.56 days, Robinson et al., 2018; .6–1.1 days, Rogers & Feller, 2018). For the reasons just described, we consider our LPN CoP attendance findings practically significant.
We did not observe any significant RN CoP effects on attendance or chronic absenteeism. Model assumption tests revealed non-normal residual distribution and slight evidence of heteroscedasticity for our LPN and RN attendance MLMs; however, these seemed insufficient to warrant removing outliers or performing variable transformations. Our chronic absenteeism models did not appear to violate MLM assumptions (see Supplemental Section 2 for sensitivity analyses and assumption test details).
RQ3
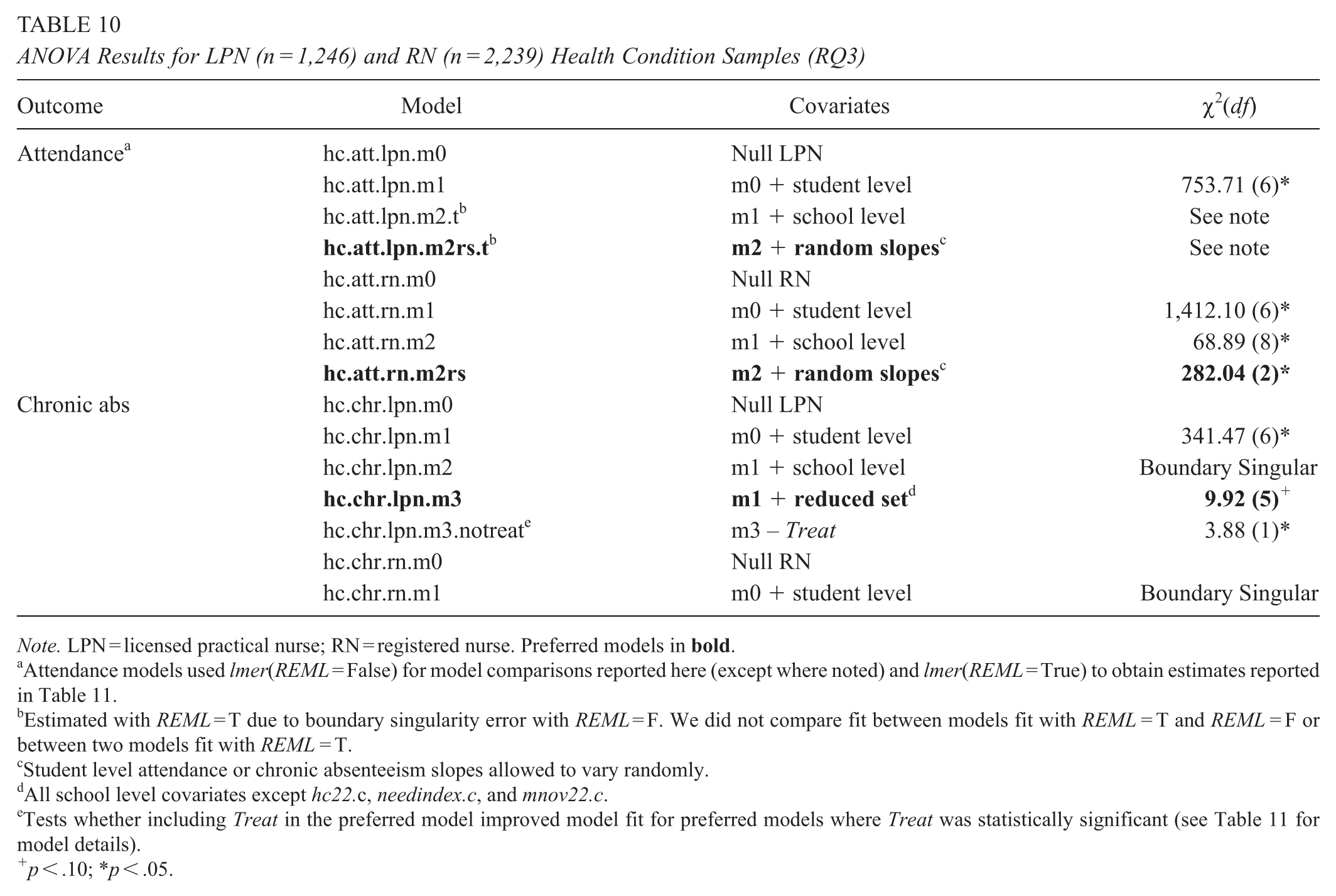
Table 10 provides model comparison results for students with previously identified health conditions in LPN (n = 1,246) and RN (n = 2,239) schools. Our LPN attendance models with school-level covariates produced boundary singular warnings with REML = F. We estimated those models with REML = T and report results from a full-covariate, random intercepts-random slopes model consistent with our preferred RQ2 LPN attendance model, although we were not able to compare model fit for MLMs estimated with REML = T (e.g., Bolker, 2015). The full-covariate LPN chronic absenteeism model produced a boundary singular warning; therefore, we estimated a reduced-covariate model. As shown in Table 11, the Treat coefficient in the reduced-covariate model was statistically significant (OR = .73, β = −.31, SE = .15, 95% CI [−.63, −.002], p = .04), indicating a 26.84% reduction in the odds of chronic absenteeism. MLM assumption tests revealed no violations (see Supplemental Section 2). The Treat coefficient (β = .42, SE = .46, 95% CI [−.49, 1.33], p = .38) in our preferred LPN attendance model was also larger in magnitude than that in our RQ2 all-student model but not statistically significant. We observed no significant differences in attendance between RN treatment vs. control schools, and model fit issues prevented examining CoP effects on chronic absenteeism in RN schools.
ANOVA Results for LPN (n = 1,246) and RN (n = 2,239) Health Condition Samples (RQ3)
Note. LPN = licensed practical nurse; RN = registered nurse. Preferred models in
Attendance models used lmer(REML = False) for model comparisons reported here (except where noted) and lmer(REML = True) to obtain estimates reported in Table 11.
Estimated with REML = T due to boundary singularity error with REML = F. We did not compare fit between models fit with REML = T and REML = F or between two models fit with REML = T.
Student level attendance or chronic absenteeism slopes allowed to vary randomly.
All school level covariates except hc22.c, needindex.c, and mnov22.c.
Tests whether including Treat in the preferred model improved model fit for preferred models where Treat was statistically significant (see Table 11 for model details).
p < .10; *p < .05.
Multilevel Model Results for LPN (n = 1,246) and RN (n = 2,239) Health Condition Samples
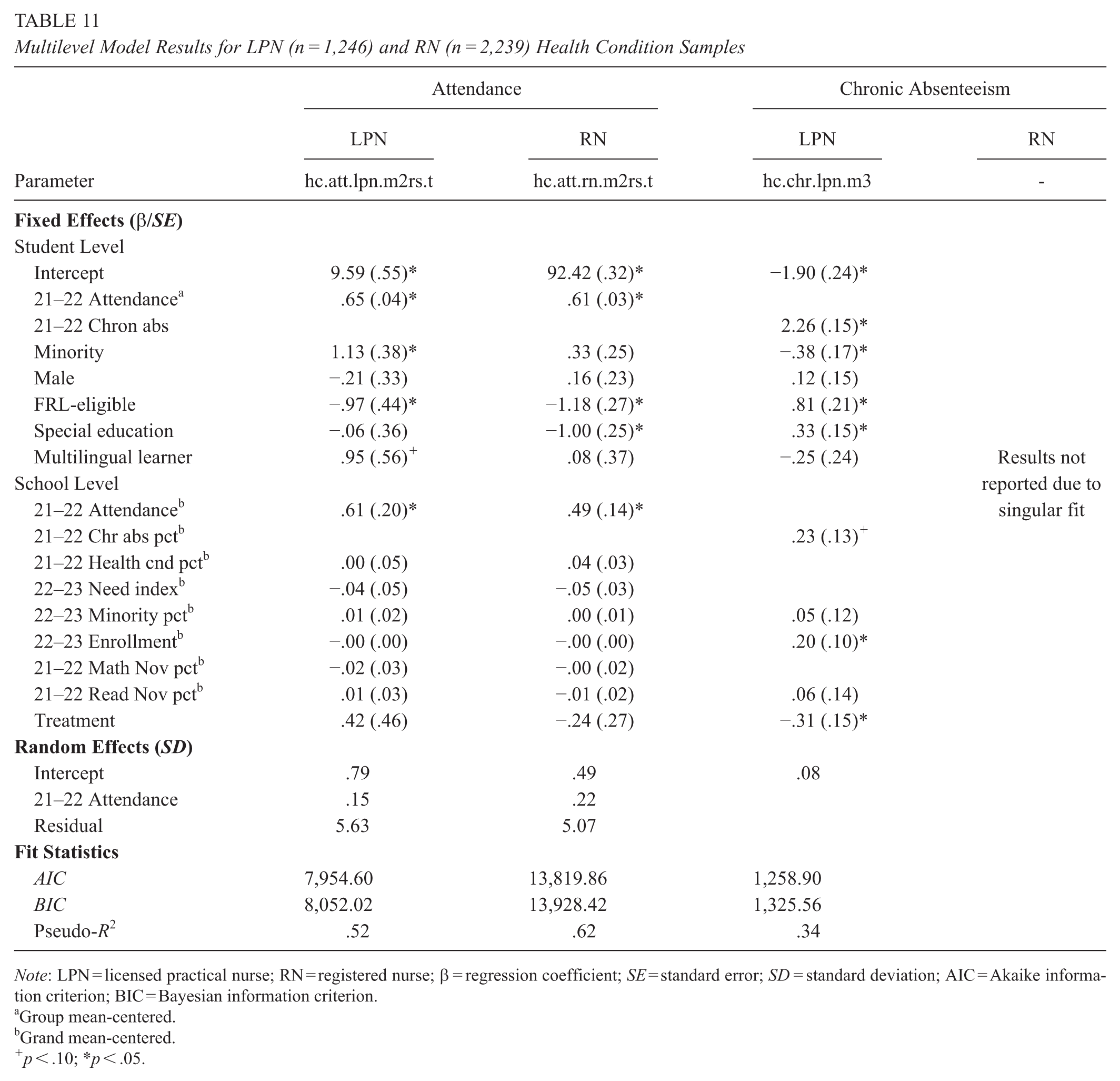
Note: LPN = licensed practical nurse; RN = registered nurse; β = regression coefficient; SE = standard error; SD = standard deviation; AIC = Akaike information criterion; BIC = Bayesian information criterion.
Group mean-centered.
Grand mean-centered.
p < .10; *p < .05.
Cost-Effectiveness Ratios
Assuming a 175-day school year, 95% CIs suggest the average $764 per school cost of forming an online LPN CoP produced a best-case 1.24-day attendance increase and 25.86% lower odds of chronic absenteeism and a worst-case .07-day attendance decrease and 3.33% lower chronic absenteeism odds for all students in grades 1–5 relative to control school peers. Reduced odds of chronic absenteeism ranged from −46.56% (best case) to −.02% (worst case) for students with health conditions in those same schools. To permit comparisons with prior studies (e.g., Rogers & Feller, 2018), we used the hypothetical total cost and intent-to-treat MLM point estimate obtained using REML = F (β = .32, SE = .16, 95% CI [.01, .63], p = .05)—that is, our highest cost and smallest effect estimates (see Tables 3 and S5, respectively)—to compute the cost per student attendance day gained in LPN CoP schools. For $12,726, a .32% attendance increase over a 175-day school year for 5,183 LPN CoPs students yielded 2,910.64 additional attendance days at a cost of $4.37 per incremental day gained. Substituting the LPN CoPs’ lower ($5,968.08) and upper ($23,390.01) bound total cost estimates from our sensitivity analyses (details in the supplemental cost spreadsheets Sensitivity Analyses tab) produced a cost range of $2.05 to $8.04 per incremental student attendance day gained.
Discussion
We conducted the first school nursing CEA to incorporate a rigorous, experimental design; the first study to investigate the costs and effects of specific nursing activities aimed at improving attendance outcomes for all students; and the only known empirical study to separately analyze school-based LPNs and RNs. In doing so, we answered calls for school nursing research to investigate licensure effects (Darnell et al., 2019; Leach et al., 2023) and move beyond descriptive studies (Best et al., 2018), weak designs (Pawils et al., 2023; Yoder, 2020), studies involving only students with chronic health conditions and/or from disadvantaged backgrounds (Yoder, 2020), and a focus on nurse presence (Leach et al., 2023). Our study also responded to calls for CEAs (Swaithes et al., 2023) and experimental studies (Noar et al., 2023) of online healthcare CoPs. We followed Yoder’s (2020) recommendations by using standard administrative outcome data consistent with prior research (e.g., Leach et al., 2023) and studying isolated intervention effects rather than investigating online CoPs as part of an integrated, whole-school intervention. We also sought to serve as an exemplar for MLM reporting by providing extensive supplemental materials aligned with Meteyard and Davies’s (2020) recommended best practices.
Our finding that an online LPN CoP was a cost-effective way to increase attendance and decrease the odds of chronic absenteeism for all students seems important for two key reasons. First, improving attendance, especially preventing chronic absenteeism, is crucial for recovering COVID-related learning loss and improving long-term educational and career outcomes (e.g., Cardona, 2024; Dee, 2024; Gee et al., 2023). The well-known deleterious effects of poor attendance and chronic absenteeism on academic outcomes (e.g., M. A. Gottfried, 2013, 2014) also extend to classmates of students who routinely miss school (M. A. Gottfried, 2019; M. Gottfried & Ansari, 2022). Thus, even small gains in attendance and chronic absenteeism, such as those we observed in LPN CoP schools, may broadly impact academic outcomes across classrooms and schools. We would expect greater positive impacts when student gains are school-wide, as in our study, rather than for smaller subgroups (e.g., students with chronic health conditions).
Second, rising chronic absenteeism requires an “all-hands-on-deck” solution (The White House, 2023), as evidenced by the fact that LPN CoP gains in our study were situated within worsening district-wide attendance and chronic absenteeism. However, the looming pandemic stimulus funding fiscal cliff (e.g., Roza & Silberstein, 2023) means districts will likely have to abandon the all-too-common strategy of addressing attendance needs by layering on new initiatives (e.g., Yan & Aberli, 2024). Even in the best of times, Yan and Hollands (2018) argue that school budget decisions should favor a set of coherent, feasibly implemented programs that have (1) clear alignment with district priorities; (2) impact evidence, ideally local (Hollands et al., 2024); (3) low per pupil costs; and (4) political support. Notably, online school nursing CoPs seem to meet criteria (1) and (4) prima facie, and we have shown they can satisfy (2) and (3).
For perspective, our estimated cost of ~$4 per attendance day gained in LPN CoP schools compares favorably with previously reported costs for a guardian postcard intervention ($6/day, Rogers & Feller, 2018; $11/day, Robinson et al., 2018; $56–$179/day, Himmelsbach et al., 2021), social workers and truancy officers ($50–100/day; Rogers & Feller, 2016), and mentors ($400/day; Guryan et al., 2021). To the extent that school nursing CoPs enhance implementing best practices (e.g., Swaithes et al., 2023), such as attendance team participation (e.g., Rankine et al., 2021), they follow Yan and Aberli’s (2024) recommendation to prioritize allocating resources toward continuously improving existing programs. In states like Kentucky, which makes upward adjustments to district per pupil funding based on yearly growth in average daily attendance (Kentucky Department of Education, 2024), effective school nursing CoPs can offset their own implementation costs if the increased revenue owing to attendance gains exceeds the variable costs associated with those gains in attendance.
Our mixed findings raise the question of why LPN but not RN CoPs were effective for reducing absences. We supposed CoPs might benefit LPNs more than RNs in terms of improving attendance-related practice; however, we expected favorable student outcomes in all treatment schools. Although it is possible that RN CoPs cannot improve attendance, we can instead offer two plausible explanations why the RN CoP as implemented was not cost-effective: content focus and participation. Content-wise, both CoPs focused on Framework components associated with absenteeism (Rankine et al., 2021); however, LPNs focused solely on care coordination, whereas RNs addressed multiple domains. Extant research commonly links student outcomes to care coordination interventions (Best et al., 2018). School nurses interviewed by Rankine et al. (2021) identified care coordination more frequently than other domains as crucial for reducing chronic absenteeism. These studies demonstrate a rationale for the relative importance of care coordination activities for improving student attendance, although their respective qualitative interview analysis (Rankine et al., 2021) and integrative review (Best et al., 2018) designs somewhat temper the argument from an evidence-based perspective. If attendance is more strongly related to care coordination than the other Framework domains, we might expect care coordination–based CoPs to be more effective at improving attendance, irrespective of nurse licensure. Additionally, multidomain CoPs may simply require more time than single-focus CoPs to demonstrate effects. Lastly, although EHRs can support improved care coordination (Baker & Gance-Cleveland, 2021), JCPS primarily implemented EHRs to improve health data collection and reporting, two noted quality improvement barriers (Davis et al., 2021). Thus, the failure of expected EHR data elements to materialize may have more negatively impacted the data-focused RN CoP.
Substantially lower RN participation relative to LPNs also likely contributed to the RN CoP-producing null effects. Building a sense of community is vital to CoPs’ success (Wenger-Trayner et al., 2023) and depends on the participation of all members (Bindels et al., 2014; Hennein et al., 2022). Low RN participation may have stymied community building and, consequently, their CoPs’ impact on attendance. If CoPs require a minimum dosage to enhance implementation of best practices and facilitate knowledge sharing (e.g., Swaithes et al., 2023), RNs may not have met that threshold. Although Rankine et al. (2021) include attendance team participation under the Framework’s leadership domain, they argue that interdisciplinary teams (i.e., care coordination) and attendance data availability (i.e., quality improvement) contribute to effectively addressing chronic absenteeism. If nurse attendance team participation is crucial to overcoming those barriers, lower RN vs. LPN participation (see Supplemental Section 1) may have weakened RN CoP effects, albeit incomplete attendance team participation data prevented a more conclusive analysis.
Finally, although bottom-up structures can foster a greater sense of ownership among CoP members (Bindels et al., 2014) and boost CoP success and sustainability (Wenger-Trayner et al., 2023), top-down (or hybrid) structures may be better suited to promoting content uptake and/or participation for LPNs than RNs, based on typical job roles. For example, the KBN (2022) limits the LPN scope of practice primarily to contributing, suggesting, and reporting, whereas RNs analyze, interpret, formulate, establish, implement, delegate, direct, initiate, and evaluate with “broad accountability.” The dependent LPN role as defined by the KBN seems prima facie more amenable than the independent RN role to top-down CoP organization. We remind the reader that JCPS specifically aligns its LPN and RN job descriptions with the respective KBN scope of practice (see Supplemental Section 5).
Implications for School Nursing Practice
Our results suggest JCPS should expand the care coordination–based online LPN CoP district-wide. The structures are already in place, and the incremental economic cost of adding LPNs is small (~$684 per school, including LPN participation costs but excluding facilitator planning and implementation time that we already accounted for). Related budget expenditures, perhaps more relevant to program decision-makers, are practically zero because CoP sessions occur during normal working hours and JCPS Health Services considers participation part of expected job duties for all nurses. Furthermore, organization-wide participation is a core CoP component for facilitating changes in practice (Hennein et al., 2022). Our recommendation comes with the caveat that efforts to determine the mechanisms of CoP effectiveness should accompany any expansion. For example, although nurse turnover and recall bias limit the value of retrospective attempts to ascertain CoP-related changes in practice, Health Services could embed regular discussions on the topic in future sessions to provide real-time feedback. Data from the district’s planned EHR reimplementation may give greater insight into the relationship between specific practices and/or referral follow-ups and student attendance. Finally, by actively tracking nurse attendance team participation, Health Services could more reliably analyze the role of attendance team participation in improving student outcomes.
Given the district’s focus on continuous improvement, we recommend the sustained implementation and evaluation of the RN CoP. Ideally, Health Services could reexamine the multidomain RN CoP model supported by EHR data. Because EHRs can facilitate expanded Medicaid billing (Leach et al., 2023), EHR use has the potential to simultaneously increase the effects and offset the costs of school nursing CoPs. Depending on its evaluative capacity, JCPS could implement and evaluate RN CoPs with alternative content focus and/or organization structures.
Other districts should consider forming online school nursing CoPs, especially those with LPN-based school nursing programs. We suggest districts start relatively small (Wenger-Trayner et al., 2023), proceed in an iterative implement-evaluate approach like that of JCPS, and expand effective CoPs. We echo Best et al. (2018) in encouraging districts to disseminate school nursing CoPs’ evaluation results as widely as possible, irrespective of the nature of their findings, to build a CoP knowledge base and strengthen future implementation and evaluation efforts broadly.
Limitations & Future Directions
Our CEA focused on a single-year instance of online CoPs in elementary schools in a large, urban district and their effects on attendance and chronic absenteeism. Although Swaithes et al. (2023) argue that such studies can produce generalizable CoP knowledge, future research should not only seek to replicate our findings but also investigate the cost-effectiveness of other school nursing CoP formats (e.g., in-person), levels (e.g., middle/high school), settings (e.g., rural), and/or outcomes (e.g., health or academic), including long-term effects. Because EHRs include nurse office visit details related to referrals, the lack of expected EHR data limited our ability to both track referral follow-ups and identify specific practices by which the online LPN CoP improved attendance and chronic absenteeism and may have biased costs downwards. Similarly, although our cost survey asked about CoP-related changes in practice, its purpose was to identify implementation costs rather than attendance-related nursing practices. Incomplete treatment year and missing prior year participation data precluded including nurse attendance team participation as a covariate in our MLMs and/or analyzing participation as an outcome of CoPs. Studies with more granular data can disentangle the key mechanisms for CoPs effectiveness, perhaps leading to the development of standardized vignettes or modules (e.g., Smyth et al., 2021) to facilitate forming effective online school nursing CoPs.
We could not directly compare the cost-effectiveness of online LPN vs. RN CoPs due to nonrandom assignment by licensure and a lack of business-as-usual RN program costs. Future studies should estimate school-based RN program costs and effects. If districts are hesitant to randomly assign by licensure based on the NASN’s (2021) recommendation for bachelor-trained RNs, researchers could use matched samples (e.g., Leach et al., 2023). A better understanding of LPN vs. RN costs and effects would be useful to budget decision-makers faced with the looming stimulus funding fiscal cliff and, in view of ongoing nursing shortages and regional licensure differences, available hiring choices. Along similar lines, we also do not know about the relative cost-effectiveness of agency nurses on student health and academic outcomes. We observed less agency nurse attrition among treatment vs. control schools, although we cannot causally attribute higher retention to CoP participation. To the extent that stable school nurse presence facilitates better student health and academic outcomes, increased nurse retention seems desirable. Thus, future studies should investigate the relationships between school nurse CoP participation and retention and between nurse retention and student health and academic outcomes.
Our preferred intent-to-treat approach with imperfect CoP participation perhaps casts some doubt on our findings, especially for RNs. As mentioned earlier, however, our results were robust to per-protocol models that excluded treatment schools whose nurses did not participate in CoPs. Because our study investigated a fixed number of schools, we did not conduct ex ante power analyses; however, our LPN analyses were likely underpowered (<50 schools; e.g., Meteyard & Davies, 2020), which can increase the chance of Type I errors, or false positive results that are not replicable (Dumas-Mallet et al., 2017). However, Heckman et al. (2022) argue post hoc power analyses are unhelpful, especially for estimating the chance of Type II errors (false negatives), and instead recommend reporting 95% CIs, which we have done, along with following Luke’s (2017) MLM estimation recommendations for reducing Type I error rates with small samples. Absent ex ante power analyses, our mixed LPN and RN results represent potential Type I and II errors, respectively, further highlighting the need for replication studies. Future MLM-based school nursing CoP studies should use larger samples (i.e., more schools) and strongly encourage full, voluntary nurse participation.
Conclusion
The prospect of online school nursing CoPs as a low-cost, light-touch strategy to improve student attendance is timely for educators faced with rising chronic absenteeism and shrinking budgets. We found that a care coordination–focused online LPN CoP was cost-effective for improving elementary student chronic absenteeism (p < .05) and attendance (p < .10). Contrary to expectations, a multidomain online RN CoP did not improve attendance outcomes. Findings suggest CoPs require context-appropriate structure and content focus and adequate participation to maximize their impact. We recommend forming online school nursing CoPs in an iterative implement-evaluate approach, expanding effective models and disseminating evaluation findings irrespective of effectiveness. Furthering our understanding of the mechanisms through which school nursing CoPs mitigate student absenteeism calls for more research.
Supplemental Material
sj-docx-1-ero-10.1177_23328584251395727 – Supplemental material for The Cost-Effectiveness of School Nursing Communities of Practice on Elementary Student Attendance and Chronic Absenteeism: A Clustered Randomized Controlled Trial
Supplemental material, sj-docx-1-ero-10.1177_23328584251395727 for The Cost-Effectiveness of School Nursing Communities of Practice on Elementary Student Attendance and Chronic Absenteeism: A Clustered Randomized Controlled Trial by Stephen M. Leach, Robert Shand, Eva Stone, Thomas J. Reece and Emily K. Reece in AERA Open
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A research grant from the National Association of School Nurses supported this work.
Open Practices Statement
Authors
STEPHEN M. LEACH, PhD, is a grant developer at Jefferson County Public Schools, 3332 Newburg Road, Louisville, KY 40218; email:
ROBERT SHAND, PhD, is an associate professor in the School of Education at American University, 4801 Massachusetts Avenue NW 459, Washington, DC, 20016; email:
EVA STONE, DNP, APRN, is the manager of district health for Jefferson County Public Schools, 3301 Stober Road, Louisville, KY 40213; email:
THOMAS J. REECE, PhD, is a researcher at Jefferson County Public Schools, 3332 Newburg Road, Louisville, KY 40218; email:
EMILY K. REECE, PhD, is an epidemiologist at Jefferson County Public Schools, 3301 Stober Road, Louisville, KY 40213; email:
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.