
Abstract
One major responsibility of K–12 teachers in United States public schools is to meet the needs of disabled students. While many preservice and in-service teacher training programs present educators with information related to service delivery as outlined in a student’s Individualized Education Program or 504 plan, they rarely address how to talk about disability with all students. This qualitative study examines 50 in-service teachers’ experiences related to disability training and explores the implications of this training on teachers’ disability discussion practices. Findings reveal that teacher training is primarily focused on compliance and “fixing” disability; training and prior experiences affect how teachers define disability; and training affects the framework that teachers use when discussing disability with their students. Based on the findings of this study, we offer recommendations to help programs reimagine training and view disability as a minoritized identity. Results of this study address a significant gap in preparing teachers for disability discussion.
Keywords
“Disability is definitely a challenging conversation to have. The reason is because when you hear disability, it is frowned upon in our society. Kids start making jokes and things when they hear the word ‘disability.’ And that can make kids uncomfortable.” —High School English Teacher “I think with ableism, students in general know so little about the topic. So, we do an exercise thinking about ramps in the city. So for the rest of the year, they’ll come back and be like, ‘Yeah, I was thinking about [name of street] and, like, it took me four blocks to find a ramp to get up onto the curb,’ and stuff like that. So, that kind of thinking is a good seed to grow. That lens is important.” —Middle School Social Studies Teacher
As these quotes reveal, teachers can conceptualize, and thereby discuss, disability in a variety of ways. In some cases, teachers avoid discussion because they do not want to offend disabled 1 students (Hansen et al., 2023). In other instances, teachers may choose to engage students in conversation about disability as a minoritized identity. While several factors may inform a teacher’s choice to discuss disability with their 2 students, teacher training is one area that may account for the variation in teacher responses. For the purposes of this paper, we use the terms “discuss(ing) disability” and “classroom discussion” interchangeably to denote any content relayed to students about disability; this includes structured lessons and presentations as well as informal whole-class or one-on-one discussions.
Since the reauthorization of the Individuals with Education Act (IDEA) in 2004, disability accountability standards and required disability training for teachers in the United States have increased (Individuals with Disabilities Education Act [IDEA], 2022). One of the major responsibilities of K–12 teachers is to meet the needs of students with disabilities in their classrooms. This often includes ensuring appropriate delivery of disability services as outlined in a student’s Individualized Education Program (IEP) or 504 plan (IDEA, 2022). Teachers receive training in these aspects of their jobs through teacher education programs (TEPs) and professional development (PD). These programs, however, rarely address how to talk about disability with all students (Cosier & Pearson, 2016).
Instead, many TEPs and PD sessions focus on compliance (i.e., service delivery and IDEA) and present disability through a deficit-oriented lens (Cosier & Pearson, 2016; Valle & Connor, 2011). More specifically, disability is medicalized, and the focus is on how to “fix” or “correct” attitudes and behaviors deemed non-normative (Ashby, 2012; Valle & Connor, 2011). When disability is portrayed in this way, it can affect teachers’ perceptions of disability and impact how they present or discuss disability-related content in the classroom. Additionally, yoking disability to IDEA and service delivery undermines efforts to situate disability in a social justice framework (Pugach et al., 2021), as it “leads to an aversion of an intersectional analysis where disability is understood as a complex part of a myriad of identity categories” (Bacon & Lalvani, 2019, p. 390).
When considering the impact of disability discussion on the educational experiences of disabled students, research (C. Mueller, 2019; C. O. Mueller, 2021; Orr & Goodman, 2010) has demonstrated that being presented with deficit-based perspectives can harm students’ sense of self-worth. In an investigation of the identity development of nine disabled students (C. O. Mueller, 2021), participants identified major gaps in their schooling experience that shaped their disability identity, which included a lack of discussion of disability or inclusion in the curriculum, lack of disability community, and lack of school staff or teachers with disabilities. Orr and Goodman’s (2010) interviews with 14 postsecondary students with learning disabilities found that “13 of the 14 participants spoke of feeling ‘stupid,’ ‘embarrassed,’ and/or ‘ashamed’” because of negative K–12 educational experiences related to their disability (p. 215).
To create classrooms where disabled students feel included rather than stigmatized, it is necessary to consider teachers’ accounts of disability-related training and learn more about the lens they use when discussing disability (i.e., disability as compliance or as human difference). In response, our qualitative study investigates the questions: What type of training do in-service teachers report receiving regarding disability? What, if anything, is the relationship between training and the ways that teachers define disability? What, if anything, are the implications of this training as it relates to discussing disability in K–12 classrooms? The aim of this research is to understand the relationship between teacher training, conceptions of disability, and related classroom discussion.
Teacher Training Programs in the United States
Under the Higher Education Act, the U.S. Department of Education is responsible for approving accrediting organizations that evaluate the quality of TEPs (Rodriguez et al., 2024, p. 45). Each state maintains a set of federally recognized accrediting agencies, and the agencies then are responsible for the accreditation of the TEPs that lead to licensure. TEPs can be run by institutions of higher education (IHEs) or by other organizations. According to a report published by the American Association of Colleges for Teacher Education (2022), “There were 1,700 teacher preparation providers in 2018–19; nearly 1,500 of these providers were colleges and universities. The remaining 200 providers were non-profit organizations, school districts, and other entities approved by their states to offer alternative teacher preparation programs” (p. 7).
Although federal legislation has influenced state policy increasingly in the last 20 years (e.g., No Child Left Behind in 2001; the Every Student Succeeds Act in 2015), it is ultimately the role of state agencies to assess the quality of education or training provided by each TEP (Sindelar et al., 2019; United States Department of Education, 2024). While most states require that teacher candidates pass specific standardized tests that assess knowledge of general subject matter, instructional techniques, pedagogy, and methodology, each state is free to determine their own licensure requirements (Rodriguez et al., 2024, p. 46). General education teacher licenses in the United States are typically organized by grade bands (e.g., early childhood, elementary, middle school, and high school) and, for secondary education (i.e., middle and high school), by subject matter (e.g., English/language arts, science, mathematics, social studies, language). Special education licensure can follow one of two paths: as a stand-alone certificate or as an additional license that can be earned after obtaining a general education license (Blanton et al., 2017). 3
In general education preparation, coursework requirements can vary widely. In their investigation of state licensure requirements for general education teachers, the National Center on Learning Disabilities (NCLD, 2019) found that “seven states have specific coursework requirements for teaching students with disabilities at the elementary and secondary level. Two states have comprehensive standards related to teaching students with disabilities. Two states require specific clinical experiences with students with disabilities. One state has standards, coursework, and clinical preparation requirements” (NCLD, 2019, p. 12). Thus, the number of courses that a general education teacher encounters prior to entering the classroom—and the content addressed in these courses—is not consistent across TEPs. For example, Servizzi (2015) sought to understand the number of required special education courses taken by general education majors in Indiana. After examining the syllabi of 14 different TEPs in Indiana, Servizzi found that, of the total, “10 (71.4%) require[d] one course, three (21.4%) require[d] two courses, and one (6.7%) require[d] three courses” (p. 486). Similarly, Cosier and Pearson (2016) noted that in California, “one of the largest and most highly rated K–8 general education TEPs in the state only require[d] one course associated with exceptional learners” (pp. 3–4). Special education teacher preparation coursework commonly includes instruction on intervention strategies, diagnostic assessment, and facilitation of student access to the general education curriculum (McCray & Waitoller, 2024). As previously stated, special educators may also be required to obtain a general education degree, which means that they would also encounter general education coursework.
Overall, the lack of uniformity in TEPs and licensure requirements can lead to significant discrepancies in the type of disability-related coursework that general and special education teachers encounter in their respective TEPs. As a result, it is extremely difficult to determine the model(s) of disability that teachers may encounter during their training period, as well as how training informs their classroom approaches to disability discussion. In response, this research aims to better understand what type of training teachers report receiving and how this informs their practice related to disability discussion.
Disability Studies in Education and Disability Critical Race Studies
Disability studies in education (DSE) and disability critical race studies (DisCrit) provide the theoretical grounding for this research. While DSE offers insight into models of conceptualizing disability, DisCrit provides a framework for understanding how teachers situate disability in relation to identity and intersectionality.
Disability Studies in Education
DSE challenges deficit-oriented views of disability as related to education and dismantles the narrative that disability is an undesirable condition that requires fixing, curing, or overcoming (Baglieri & Lalvani, 2020; Connor et al., 2015; Cosier & Pearson, 2016). DSE was, in part, conceptualized by special educators who felt confined by the traditional field of special education and appreciated perspectives on disability offered by the broader field of disability studies (Baglieri et al., 2011). Given its point of origin, DSE “offers much to the traditional field of special education, providing various lenses through which to view disability that, in turn, influence how we conduct research, the ways that we teach, and the place of students with disabilities in schools” (Baglieri et al., 2011, p. 275). Theoretically, “disability as deficit” is rooted in the medical model of disability (Valle & Connor, 2011). This model assumes that disability is a fixed condition requiring intervention, and people with disabilities must adapt to society. In doing so, the medical model perpetuates ableism, “a system of discrimination and exclusion that oppresses people who have . . . disabilities” (Rauscher & McClintock, 1996, p. 198).
Conversely, the social model of disability shifts the focus of disability from the person to the environment. DSE ascribes to the social model by highlighting how the physical environment creates barriers for disabled people and how attitudes surrounding disability prevent disabled people from full participation in society (Huang & Brittain, 2006; Oliver, 2004). The social model also disentangles disability from impairment (i.e., a difference related to the physical, emotional, or mental structure of the body). According to the social model, impairment is not the root cause of marginalization or exclusion; instead, physical, socioemotional, and academic barriers prevent the full inclusion of anyone who is disabled. The social model recognizes disability as a minoritized social identity with a shared history of oppression (Mackelprang & Salsgiver, 2016). Even today, disabled people encounter discrimination related to education, healthcare, transportation, housing, and employment (Kittay, 2011).
Disability Critical Race Studies
Disability identity—like other social identities—is not monolithic. Rather, it is best understood through the lens of intersectionality, which describes how interlocking systems of oppression frame individuals’ social worlds (Carey et al., 2018; Crenshaw, 1989). The inequity that a disabled person encounters is never the result of a distinct, single factor. Instead, it is informed by the various other social identities (race, class, sexuality, gender, body size, religion) that a person possesses, as well as the privilege or oppression associated with each of these identities (Carey et al., 2018; Hankivsky, 2014).
In 2013, Annamma et al. conceptualized the field of DisCrit to explore the intersection of race and disability. Drawing on tenets of disability studies and critical race theory, DisCrit “explores ways in which both race and ability are socially constructed and interdependent . . . [and] examine[s] the processes in which students are simultaneously raced and dis/abled” (p. 8). DisCrit both exposes and problematizes how ableism and racism inform the experiences of students of color on micro and macro levels, especially as compared to their white peers.
DisCrit also examines how racism and ableism fuel disproportionality, or the overrepresentation of minoritized students in special education (Annamma et al., 2013). Put another way, “disproportional representation is identified when students of certain ethnicities appear in special education programs or disability categories in greater percentages than they occur in the general population of students” (Maydosz, 2014, p. 82). Teacher bias, rooted in a misunderstanding of the cultural norms of students of color, can lead white teachers to unnecessarily refer students of color for disability services (Bruce &Venkatesh, 2014; Maydosz, 2014; Skiba et al., 2002). As a result, disability status has created a sanctioned form of segregation within the U.S. public school system (Artiles, 2003; Cruz et al., 2021; Ferri & Connor, 2005; Harry et al., 2007). Although some researchers have pushed back against the claim that students of color are overrepresented in special education (see Morgan et al., 2012), Artiles (2019) has noted that mixed findings may be the result of the way that disproportionality has been theorized—namely with disability and race presented as objective entities. DisCrit offers a way to engage the cultural-historical complexities underlying the representation of students of color in special education (Artiles, 2019).
DSE, DisCrit, and Teacher Training
Research has shown that teacher training programs tend to present disability as a fragmented, rather than intersectional, identity (Carey et al., 2018; McCray & Waitoller, 2024; Sapon-Shevin, 2017). By doing so, training programs run the risk of overlooking how identities work in concert to influence students’ experiences in school, which is a key tenet of DisCrit (Annamma et al., 2013; McCray & Waitoller, 2024). Pugach et al.’s (2021) analysis of literature on social justice–oriented TEPs revealed that 42% (n = 22) omitted disability entirely; 26% (n = 14) addressed disability minimally; and 17% (n = 9) addressed disability briefly (as it surfaced in results). Only 15% (n = 8) of the studies addressed disability substantively. Additionally, the researchers reported that most studies addressed disability as an instructional challenge or diagnostic characteristic rather than as part of an intersecting identity.
Since an intersectional understanding of disability identity can help teachers recognize how students may experience multiple forms of marginalization, teachers must be provided with opportunities to reflect on how they “read” student identities in combination (Sapon-Shevin, 2017). Take, for example, a student who is Black and autistic. If a teacher were to respond to one of these identities rather than considering both in tandem, they may risk misinterpreting the interlocking system of oppressive factors underlying any educational disparities that this student could encounter (Carey et al., 2018; Sapon-Shevin, 2017).
Within the context of K–12 education, preservice and in-service teacher training is often situated in the medical model of disability (Ashby, 2012; Baglieri & Lalvani, 2020; Ferri & Bacon, 2011). As Ashby (2012) explained: [Pre-service teachers] are generally taught the common characteristics associated with the 13 federal categories of disability, including etiology and methods of assessment, along with strategies for remediating such differences. Disability is presented as a fixed and identifiable construct, an immutable part of the person. (p. 91)
Pathologizing difference also reinforces the socially constructed binary of normal/abnormal, as teachers are typically taught that there are two kinds of students: “regular” students and “special” students, with “regular” presented as the ideal (Ashby, 2012; Valle & Connor, 2011). This sends the message that the goal of special education services is to make disabled students more like their nondisabled peers (Baglieri & Lalvani, 2020).
Teacher training programs can reinforce ableist messages both directly and indirectly (K. K. Thorius et al., 2024). In some instances, preservice and in-service teachers may be instructed that ignoring or not acknowledging disabilities is best for the students, which can reinforce disability stigma (Baglieri & Lalvani, 2020; C. O. Mueller, 2021). In other cases, rather than acknowledging and appreciating individual differences, teachers are informed that there are cookie-cutter approaches to making school accessible and welcoming to all (Moriña & Carballo, 2017). Additionally, the field of special education has been critiqued for training teachers who “unwittingly collude in a complex of disturbing practices that do not benefit those [they] claim to help” (Brantlinger, 2006, pp. 241–242). This could look like teaching students with autism to mask and act in neurotypical ways under the guise of engaging in “appropriate” social behaviors. Roegman et al. (2018) noted that special education teachers can encounter different subjectivities, or ways they should act, during their training.
Leading researchers in special education have recognized and responded to this critique. In a recent editorial article from Exceptional Children, K. K. Thorius et al. (2024) acknowledged the ways that some special education theories and practices have been predicated on fixing or changing disabled students, as well as the tensions that have arisen in the field of special education because of these epistemologies. The authors set several goals for the field, including “situating disability and special education as a civil rights and equity issues” (p. 100). By doing so, Thorius et al. aimed to rectify the belief that teacher education and special education programs “are striving for a society without disabled people” and urged researchers to conduct scholarly activity that addresses disability-based oppression and recognizes disability as an intersectional, dynamic identity (p. 101).
Again, not all teacher training is rooted in the medical model of disability, and evidence suggests that training programs rooted in the social model of disability are impactful. For example, qualitative research on six special education teachers’ identity emergence (K. A. Thorius, 2016) indicated that special education teachers who are exposed to inclusive discourse on disability shifted their focus from fixing students to addressing the existing environment. “Inclusive” special educators do not deny impairment; instead, they reframe the idea of difference as being problematic (K. A. Thorius, 2016). In doing so, they consider any educational, social, or physical barriers that a student could encounter because of their impairment and proactively create spaces or experiences that work with, rather than against, student impairments.
Methods
In this interview-based qualitative study, we aimed to provide a rich, detailed description of 50 in-service teachers’ experiences related to disability training and its implications for their respective practices (Creswell, 2009). This paper is drawn from a larger mixed-methods study that examines training, attitudes, and practices of in-service teachers as related to disability discussion.
Participants
After receiving Institutional Review Board approval for this study, we recruited participants through the use of an interest survey. We disseminated the interest survey in the United States via personal connections, social media, and snowball sampling. Selection criteria included individuals currently working as in-service teachers in grades K–12, and recruitment occurred from September 2020 to March 2021. While we collected data from 52 participants from this research project, data from two participants were not used in the current paper because they did not attend either undergraduate or graduate TEPs, resulting in 50 total participants.
Although we did not collect U.S. region-specific data from participants, 37 were public school teachers (74%), seven taught in private or independent schools (14%), two taught in parochial schools (4%), three taught in charter schools (6%), and one participant selected “other” as their school site (2%). Relatedly, 32 participants reported working in suburban schools (64%), 16 worked in urban schools (32%), and 2 participants (4%) did not provide setting-related data. Forty-nine of the 50 interviewees provided information about their race and ethnicity. Of those 49, 13 identified as people of color (26%), and 36 identified as white (72%), which is more diverse than U.S. national teacher demographics (21% teachers of color and 79% white teachers) (National Center for Education Statistics, 2020). Appendix A provides additional participant demographic information.
Research Team
The research team was comprised of six individuals: three university faculty members and three university students. One student member of the team was in a graduate program working toward a master’s degree in school counseling, and two of the student members were undergraduate students majoring or minoring in education. All members identify as women. Additional demographic characteristics include members’ race (white; n = 5; Asian American; n = 1) and disability identity (nondisabled, n = 5; disabled, n = 1). Additionally, two of the university faculty members are former K–12 special education teachers.
Procedures
Preinterview Surveys
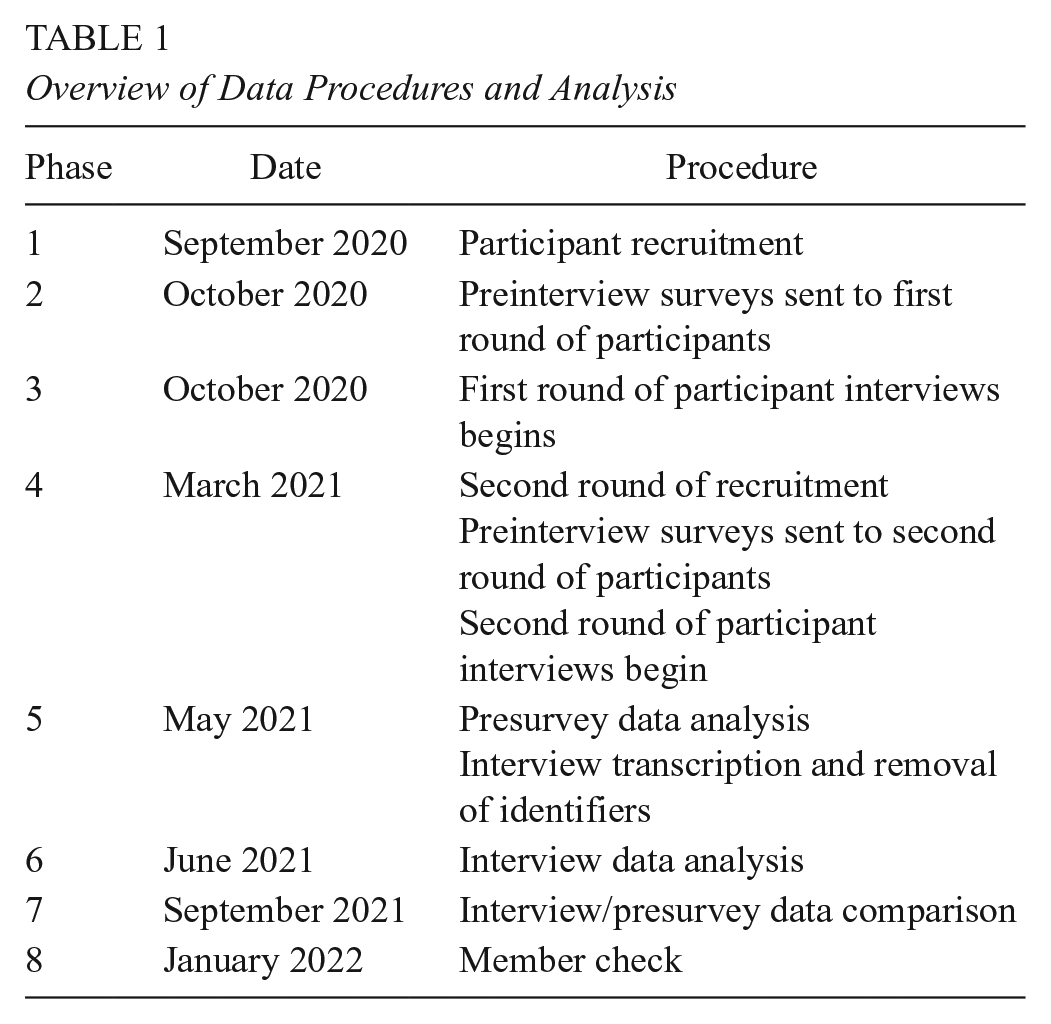
Data collection and analysis progressed through eight phases (see Table 1). After recruitment (Phase 1), participants responded to two surveys (Phase 2). The first survey asked them the extent to which they agreed or disagreed with four definitions of disability. Two of the four definitions aligned with medical model definitions of disability (Disability is a fixed condition (i.e., something that you always have, regardless of context; a person with a disability should adapt to fit into society), and two aligned with social model definitions (Disability is context-dependent [i.e., your surroundings dictate your degree of disability]; society should adapt to meet the needs of a person with a disability). Participants responded using a 4-point Likert scale ranging from strongly disagree to strongly agree.
Overview of Data Procedures and Analysis
Participants were also asked to respond to survey items regarding the type of disability-related teacher training they received (undergraduate, graduate, and professional development). Survey options included: We talked about diagnoses/types of disabilities (i.e., medicalized/focus on how to make child fit into educational environment); we talked about disability as a social identity/ableism/Universal Design for Learning; we didn’t discuss disability during my teacher training; I didn’t go through a (graduate/undergraduate) training program; and other (with opportunity to respond). Participants were also provided an opportunity to elaborate on their responses. These data were later used to triangulate participant interview responses.
The second survey was an optional demographics questionnaire that included 12 items intended to describe the sample. Demographic questions included gender, race, age, disability, subject area, grade level, classroom type (e.g., general education, self-contained classroom, etc.), personal connection to disability (e.g., having a friend or family member who is disabled), and years in service (results described in Appendix A). We offered a broad definition of disability when presenting demographic options to participants (i.e., sensory, mobility, neurodivergent, learning, mental health, vision, hearing, immunocompromised).
Interviews
The core data for this investigation were derived from semistructured interviews. Interview data were collected between October 2020 and April 2021. Participants were interviewed via Zoom by a member of the research team, and interviews typically lasted between 30–60 minutes. We developed a 12-question interview protocol (Appendix B) based on an analysis of relevant literature. The purpose of the interviews was to gain a greater understanding of how teachers defined disability, the type of disability-related training they received, and how they spoke of enacting disability-related discussions in their classrooms. We were highly cognizant of the racial demographics and related representation of participants. After conducting the first 30 interviews (Phase 3), we noted a lack of representation of participants of color. In response, we actively recruited in-service teachers of color to participate in interviews using social media, snowball sampling, and personal connections (Phase 4). All participants were gifted a $75 Amazon gift card for participation, with funding provided by an internal university grant. Participants granted permission to audio-record the interviews, which enabled later verbatim transcription. During transcription, each participant was assigned a six-digit code. Transcripts were stripped of all identifiers.
Data Analysis
One member of the research team analyzed participant responses to the preinterview survey items (Phase 5). This included determining participants’ definitions of disability as “medical” or “social” (based on the extent to which they agreed or disagreed with medical and social model definitions of disability) as well as synthesizing responses regarding the type of training participants reported receiving. These data were not shared with other members of the research team until after the axial coding process was complete.
To analyze the corpus of qualitative data, two different members of the research team engaged in initial, axial, and iterative coding (Miles et al., 2014; Srivastava & Hopwood, 2009). We used Atlas.ti, a computer-based data analysis program, to code the data and calculate intercoder agreement (Lincoln & Guba, 1985) using Krippendorff’s alpha coefficient (Phase 6).
Initial Coding
We started by familiarizing ourselves with the data set, which included reading all interviews and taking analytic memos. Next, we independently coded the first four interviews, comparing codes and memos and calculating intercoder agreement. After discussing discrepancies in codes and revising the codebook, we recoded the first four interviews and added an additional four interviews for analysis. We repeated the procedure (discussing, revising, recalculating, and revisiting), then added eight additional interviews for analysis. During the third cycle, when coding the same sections of data independently (16 of the 50 interviews, or 32% of the entire corpus of data), we achieved high intercoder agreement (α = .90; α ≥ .80 indicates acceptable reliability; Krippendorff, 2018). When acceptable reliability was reached, we divided and coded the remaining 36 interviews. The initial coding process yielded 73 codes.
Axial Coding
Next, we engaged in axial coding, where we aimed to reassemble data split during the coding process (Miles et al., 2014; Strauss & Corbin, 1998). During axial coding, we paid particular attention to codes capturing participants’ respective definitions of disability. First, we discussed what constituted a “medical” or “social” definition of disability. Medical definitions contain language that defines disability as a deficiency, disability in relation to diagnosis and/or compliance (i.e., IEPs, 504s, and legal aspects of disability), and/or a focus on a person fitting into the existing environment. For example, we categorized the following statement as medical: “IEPs. Support teachers. Accommodations. Yeah, things like that, like the more official legal side of things.” Social model definitions contained language related to barriers a person might encounter as related to disability (e.g., social, emotional, physical, academic), language related to the environment adapting to fit the person, and/or language related to disability as a form of human difference. For example, we categorized the following definition as “social”: I think about access and equity of access, and as I think about disability as a societal construct. Those sorts of things come to mind. They’re just another facet of our existence in some way. . . . There’s a world in which if certain accommodations or provisions aren’t provided, it creates disability. Versus a world in which if people think or act or expand their view of things, it minimizes the extent to which something is a disability.
We then compared our categorization of each participant’s interview response to their survey responses (the extent to which they agreed or disagreed with four definitions of disability). We found direct alignment between how we coded their definition of disability (e.g., as “medical” or “social”) and their responses to the survey items (Phase 7).
We applied a similar process for determining whether each aspect of a participant’s recollections of their training (e.g., undergraduate, graduate, and professional development [PD]) by comparing participants’ presurvey survey responses regarding their training to researchers’ categorization (Phase 7). In all but five cases, researcher and participant perceptions aligned. These five participants indicated they received social model PD. However, interview data reflected that none of the trainings focused on disability as a minoritized identity. While we did not initially consider them representative of social model training, we maintained the social model descriptors and provided additional context in the findings section of this paper. Overall, the axial coding process yielded 11 conceptual categories. examples include how teachers define disability: nature of disability discussion; personal/prior experience with disability; training related to disability discussion; and what teachers still need to conduct disability discussion.
Reflexive, Iterative Coding
Next, we engaged in a reflexive, iterative coding process (Srivastava & Hopwood, 2009), which is “at the heart of visiting and revisiting the data and connecting them with emerging insights, progressively leading to refined focus and understandings” (p. 77). We used Srivastava and Hopwood’s (2009) three-question framework as the basis for this stage of the analytic process: (1) What are the data telling me? (explicitly engaging with theoretical, subjective, ontological, epistemological, and field understandings); (2) what is it I want to know? (according to research objectives, questions, and theoretical points of interest); and (3) what is the dialectical relationship between what the data are telling me and what I want to know? (Refining the focus and linking back to research questions).
At this stage, there appeared to be variation between participant training and disability definition, whereas participants in group one (medical-medical) did not speak of having significant prior experience with disability, and results from group two were mixed (some, but not all, experiences were significant). We also found some variation between subject area, training, and disability definition; these data were then integrated into the larger data set to refine the findings. Finally, we used the “code-document table” function in Atlas.ti, which allowed us to cross-tabulate disability discussion patterns across the three groups. This yielded the following themes: training primarily situated in the medical model; training and prior experiences affect how teachers define disability; and training affects disability-related discussion.
Trustworthiness
We drew on several reliability procedures (Gibbs, 2007). First, we conducted interviews until they reached saturation of concepts in terms of their properties and dimensional variation (Corbin & Strauss, 2014). We also used Atlas.ti to calculate reliable intercoder agreement (Lincoln & Guba, 1985). Additionally, in January 2022 (Phase 8), we conducted a member check with all participants. During this check, we individually emailed participants and asked them to confirm whether the researcher’s understanding of their training and definition of disability aligned with participants’ perceptions. The body of the email contained information regarding how the researchers grouped the participant’s training experience(s) and definition of disability. To facilitate responses to the member check, participants were asked to complete a two-question survey that asked for their participant ID and whether they agreed or disagreed with the researchers’ assessment of their definition and training. Participants had the option of selecting “yes” (they agreed), “no” they did not agree, or “other,” where they could record an open-ended response. Forty-four of the 50 participants responded to the member check (85%), and all responded affirmatively.
Findings
We organized our findings into three themes and related subthemes, which reveal that training played a significant role in shaping participants’ definitions of disability and affected how they enacted disability-related discussions in their respective classrooms.
Theme 1: Participants Described Training as Primarily Situated in the Medical Model
All 50 participants reported receiving some type of medical model teacher training, either in their undergraduate TEPs, graduate TEPs, or through in-service training (sometimes referred to as “professional development”) presented through their respective school systems. Figure 1 provides additional details on programmatic and in-service teacher training patterns. It is also important to note that some participants could not recall the type of training they received or felt that disability was minimally discussed during their training, and some participants attended either an undergraduate TEP or a graduate TEP but not both.

Type of disability-related training based on program.
Undergraduate and Graduate TEP Training
When describing what they learned about disability through their undergraduate or graduate TEPs, participants often used the emic terms “classification,” “compliance,” and “diagnosis” as well as definitions connecting disability to elements of the IDEA (i.e., IEPs, 504s, and accommodations). As a representative statement from a participant revealed: First thing that comes into my mind is special education courses that I’ve taken and an overview of how to classify things . . . like, if I was working with a student that I thought was having some challenges, thinking, “where would that student fall in [term of diagnosis]” or “where would my concerns lie?” (Elementary)
No participants reported receiving only social model training in their undergraduate TEPs, though 11 (22%) reported receiving dual social-medical training as undergraduates. At the graduate level, overarching training patterns appeared mixed. Fifteen participants (30%) reported receiving only medical model training in their graduate TEP, while 17 (34%) spoke of receiving only social model training. Four participants (8%) felt that their training was a mix of the social and medical models of disability.
Participants exposed to the social model, either in conjunction with the medical model during their undergraduate TEP or at some point during their graduate TEP, described the social model framing of disability as revelatory. When reflecting on her undergraduate experience, a participant said, “My college professors definitely helped a lot because I walked into college with certain thoughts about disability, and I went out with completely different ones. Even just vocabulary. Like, I’d never heard of ableism before” (Middle School English). Similarly, another participant felt that her graduate TEP exposed her to disability-related concepts that she did not encounter during her undergraduate TEP: [In graduate school] we talked a lot about rhetoric, and I just never learned about that, it was never brought up to me. I guess before I didn’t think about [disability identity] because it just wasn’t brought to my attention. And then because it was brought to my attention, I kind of had this aha moment that, “This is wrong. This shouldn’t be this way,” and it motivated me to change. I just saw examples and situations that I never saw before, pretty much why it changed my lens. (Middle School Mathematics)
Data revealed that when participants encountered the social model, many experienced a way of thinking about disability that they had never previously considered.
In-Service Teacher Training (Professional Development)
As related to in-service training on disability, survey data show that thirty participants (60%) felt that disability was presented through a medical model lens, whereas only one (2%) indicated that their disability training incorporated the social model. Four participants (8%) were trained using both models, and 15 (30%) felt that disability discussion was limited or nonexistent in their in-service training.
Disability Absent From In-Service DEI Training
Though five of the fifty participants’ survey responses indicated that they had received social model professional development (PD), interview data reflected that none of the trainings specifically focused on disability as a minoritized identity. Instead, participants spoke of sessions where the focus was on inclusion of all identities, such as sessions on “responsive classroom,” a social-emotional approach to teaching and classroom culture.
Forty-four participants explicitly stated that they received DEI training from their schools but that disability training was nonexistent during this PD. Instead, the training focused on other aspects of diversity: We’ve spent a lot of time working and getting training on how to talk about things with students who might feel discriminated against or that they’re in a situation because of their identities or whatever it happens to be. But disability wasn’t part of that. (High School Mathematics).
Another participant said: I’m on the DEI Council Initiative, so I’m really excited about DEI. And it’s, you know, unfortunate disability has not been something that we’ve brought to the forefront and thought about as part of a DEI type of situation. . . . But I talk about basically all other minoritized groups, and I guess that’s just the one that we never talk about. (High School Social Studies)
The remaining six participants reported that they had not received DEI-related training in their schools. Participants most commonly spoke of the medical model PD they received. As they explained, training focused on either the legal aspects of disability—“So, if a student has an IEP or a 504” (Middle School Mathematics)—or on “cover[ing] all their bases”: Our special ed department is very good and they’re all about informing all their teachers about, you know, practices with disabilities. What happens, to be honest with you, is they are a little bit, I don’t want to say afraid of being sued by parents but it’s a very litigious society that we’re in right now, and I think that’s why they want to kind of cover all their bases and make sure that we know we’re doing the right thing when it comes to students with disabilities. (High School English)
Participants also felt that they were instructed to minimize the appearance of disability within the classroom environment, with a focus on “keeping things secret and one-on-one working with students with disabilities and not necessarily about inclusion in terms of talking to other students about [disability] or talking about it generally during a class period” (High School History).
Theme 2: Training and Prior Experiences Affect How Teachers Define Disability
Of the total sample, 14 participants (28%) were trained solely through the medical model (undergraduate TEP, graduate TEP, and/or in-service) and used medical model definitions of disability. They formed a subgroup we termed “medical-medical” (MM) in line with their training (medical) and the medical model definition they provided. Ten participants (20%) were trained solely through the medical model but offered social model definitions of disability. They formed a subgroup we termed “medical-social” (MS) to capture the contrast between their training (medical) and the disability definition they provided (social). All members of this group also spoke of having significant prior experience with disability (e.g., relationships with disabled family members/friends and/or self-identifying as disabled). Finally, 26 participants (52%) received training in the social and medical models during some portion of their training (undergraduate TEP, graduate TEP, and/or in-service) and used social model definitions of disability. They formed a subgroup we termed “dual-social” (DS) to account for their training in both models and their social model definition of disability. Figure 2 provides an overview of the relationship between teachers’ self-reported training and their definition of disability. We provide additional information on each group in the following subsections.

The relationship between teacher training, prior experience, and disability definition.
Medical Model Training and Medical Model Definition (MM)
Fourteen participants (28%) reported that they did not encounter the social model in their respective TEPs or in any professional development they received as an in-service teacher. During their interviews, these participants defined disability in terms of deficit, or someone not being able to do what would be considered “normal.” Representative definitions of disability or being disabled included “someone with a disadvantage in some regard, physically mentally, emotionally (Middle School Math),” “something that keeps someone from doing what, like an average person can do” (high school world language), and “a person who has parts of their body not functioning as it should. . . . My first image was someone in a wheelchair, but I also think about mental disabilities. Maybe their cognitive abilities are not the same as other people” (Middle School English).
When asked to reflect on their experiences with disabled individuals prior to teaching, participants in the MM group expressed that these experiences were either limited (n = 8) or involved peripheral relationships with relatives or classmates (n = 4). One participant noted that she “was never with students with disabilities during her K-12 schooling” (Elementary). In other cases, participants recalled that students with and without disabilities were coeducated, but their interaction was minimal. As another participant said: I don’t have a lot of relatives or friends in my circle who have disabilities . . . so I didn’t really interact with people with disabilities often, well disabilities that I knew of—let me be very clear about that, because there are disabilities that are not necessarily visual. (Middle School Science)
Participants categorized into the MM group did not speak of significant ties to the disability community and provided definitions of disability that centered on what the disabled individual was not capable of doing, especially as compared to the “norm.” While two participants in this group identified as disabled in the demographic survey, they did not share that their disability held any significance as related to their definition of disability, their prior experience with disability, or the way that they discussed disability with their students.
Medical Model Training and Social Model Definition (MS)
Ten of the participants (20% of the sample) spoke of solely receiving medical model training but offered social model definitions of disability; they formed a subgroup we termed “medical-social” (MS). Their definitions of disability addressed disability in relation to societal norms or understanding disability as a form of human difference: “I try to think of it as doing what you need to do, but in a different way” (High School English). Similarly, another participant focused on difference versus deficit: “As far as school goes, it’s a different way to learn. You might approach things different ways, but it’s not negative” (Elementary).
Interview data also indicated that all members of this group had significant prior experience with disabled individuals or identified as disabled. Several participants in this group spoke of having disabled parents or siblings, and they described how these experiences shaped their understanding of what it meant to be disabled. One participant shared that having a disability increased her empathy for others, as it “helped [her] become a better listener” (High School English and Social Studies). Another participant reflected on the ways that being disabled shaped her sense of self: I didn’t know that there were multiple different types of disabilities. I only knew about mine because I was going through it. And it really played a lot on my mind because I had a lot of self-doubt hearing that I wouldn’t be able to do certain things [which] actually began to make me believe that I couldn’t do certain things. You know, so it was very difficult. (Middle School Science)
In all cases, the prior experiences described by all members of this group appeared to be highly formative in framing their understanding of being disabled.
Dual Model Training and Social Model Definition (DS)
Twenty-six participants (52% of the sample) were categorized into the “dual model training and social model definition” group. These educators received medical and social model training and used a social model perspective when defining disability. When asked to define disability, participants continually used the emic terms “norm(s)” and “barriers,” such as “encountering barriers to fully being able to access the curriculum” (High School Science). In line with considering the relationship between disability and environment, a participant shared: I would say disability is anything that is outside what is regarded as the norm, so like we’re living an eyesight world, right? Things were written in text, so you have a disability if you can’t see. But if you, I don’t know, go to a house that’s all Braille, then you know I would have a disability, because I can’t read Braille. (Elementary)
In this way, the participant noted the ways that context and environment can inform what it means to be disabled. Compared to participants categorized into the MM group, who continually used the term “normal” in their definition of disability, participants in the group termed DS appeared to consider how norms were socially constructed.
We also accounted for participants’ prior experiences with disability, and these experiences were mixed. Twelve participants spoke of formative prior experiences (i.e., friend or family member with a disability or self-identifying as disabled). As one participant explained, her sister’s disability played a critical role in her career path: “Growing up, my sister had a specific learning disability in reading. . . . That was a big reason why I eventually pursued a degree in special education” (middle school special education). Conversely, the remaining 14 felt that their prior experiences with disability were limited or nonexistent. Participants expressed that disabled students were not visibly present in their own K–12 schooling—or that they were not aware that disabled students might be in their classes. As one participant said: When I was going through school, I never really knew anybody who . . . had in my head what I viewed as . . . a disability. I was always in . . . Honors and AP (Advanced Placement) classes and . . . I never saw anybody getting extra time on anything, so I had my own type of stereotype in my head of what it meant to have a disability. (Middle School English)
Participants categorized into the DS group with limited prior experience with disability spoke specifically of the ways that training dispelled stigma and brought to light an understanding of disability that they had not previously considered. Thus, social model training may have played a role in raising participants’ awareness of disability and disrupting narratives of what it means to be “disabled.”
Relationship Between Demographics, Training, and Disability Definition
We were also interested in understanding the relationship between participant demographics, training type, and disability definition. When comparing demographic data (e.g., grade level; school setting; classroom), the percentage of teachers in each group was consistent. One notable difference, however, was that participants categorized into the DS group were newer to teaching than the MM or MS groups. Additionally, there were slightly more social studies (39%), science (42%), and special education (27%) teachers in the DS group than in MM (21% social studies; 35% science; 7% special education) or MS (30% social studies; 30% science; 10% special education). See Figure 3 for demographics related to years in practice by group and Table 2 for subject area demographics by group (MM, DS, and MS). In Appendix C, we provide additional demographic data by group.

Years in practice by group.
Overview of Participant Subject Area Categorized by Group
What subject area(s) do you currently teach?

n Columns may exceed total number of participants because participants could select all that apply.
% Columns may add up to greater than 100%; participants could select all that apply.
“Other” responses were “engineering,” “executive functions,” “religion,” “religious studies,” “sports marketing,” and “theater and seminar.”
Theme 3: Training Affects Disability-Related Discussion
We then compared teachers’ self-reported use of disability discussion in the context of their training and definition of disability (e.g., MM, DS, and MS). Figure 4 provides an overview of disability discussion patterns across the three groups, and representative examples of how members of the MM, DS, and MS groups addressed each discussion topic can be found in the Supplemental File.

Disability discussion pattern by group.
Data indicated that teachers categorized into DS and MS spoke more frequently about engaging in disability discussion as related to student questions (65% and 55%, respectively), as compared to only 27% of participants in the group termed MM. Participants in the DS and MS groups also spoke of the importance of leaving space for students to ask questions, both about classroom content and the world around them.
Additionally, participants in the group termed DS were more likely than those in the MM or MS groups to discuss disability “in relation to identity and self-advocacy” and “talk about a specific disability” with their students, and they tended to engage in disability-related conversations both frequently and openly. Conversely, when participants in the group we termed MM did discuss specific disabilities, the focus was on minimizing differences.
Finally, it was noteworthy that more participants in the group termed MM talked about disability in relation to individual student accommodations, as compared to DS and MS participants. Participants categorized into the MM group noted that conversations about accommodations were more likely to occur one-on-one with a student rather than in front of an entire class. In the interviews, these participants’ examples of disability-related discussion were centered on disability in relation to service delivery rather than disability as a minoritized identity.
Discussion
The purpose of this research was to understand the relationship between teacher training, conceptions of disability, and related classroom discussion. Given the lack of previous empirical work investigating the connections between teacher training and disability discussion, this research offers key insights into the type of training that is needed to promote an understanding of disability as a form of human difference rather than a deficit. As study data reveal, teacher training plays a critical role in teachers’ perceptions of disability and their related classroom discussion. Findings indicate that current training is primarily situated in the medical model, training and prior experiences affect how teachers define disability, and teachers who have some exposure to the social model of disability are more likely to view and discuss disability as a form of human difference instead of a medicalized condition.
Prior Experience With Disability
One of the most salient findings pertained to disability discussion patterns by group. Participants categorized into two of the three groups—DS and MS—offered social model definitions of disability. For those in the group termed MS, use of the social model definition appeared to be due to their (self-reported) significant prior experiences with disability. However, participants in the group termed MS enacted disability discussion differently than participants who were exposed to social model training. Although participants in the MS group may have defined disability in the same way as participants categorized into the DS group, they did not offer as many instances of talking about disability in response to student questions or teaching disability self-advocacy as related to their DS counterparts (see Supplemental File). Some participants in the group termed MS indicated an underlying concern or discomfort with disability-related discussion (i.e., being afraid of saying the wrong thing and offending a disabled student).
For this reason, findings indicate that significant prior experience may help shape perceptions of disability, but social model training is needed to bridge the gap between beliefs and actions in practice. This concept is commonly referred to as a teacher’s “disposition” (Schussler, 2006). In short, while teachers may hold certain beliefs about teaching, learning, and students, they may experience difficulty enacting those beliefs if they are not provided with explicit skills and the opportunity to reflect on their understanding of disability and related, unearthed biases they may hold.
Although four participants categorized into the MM group reported having prior experience with disability—and in the case of two participants, identified as disabled—they were never exposed to the concept of disability as a minoritized identity, much less given the tools to enact disability-related discussion in their classrooms. Instead, disability was presented as non-normative and undesirable. These findings build on the work of Cosier and Pearson (2016), who noted the lack of praxis between DSE and teacher education. The findings from this study point to a need for TEPs to leverage practices that address disability as a marginalized identity and equip prospective teachers with the “language, theory, and knowledge or disability history to be able to explain why inclusive histories are so important for both students with and without disabilities” (p. 3). Research (Kahn & Lewis, 2014; Pit-ten Cate et al., 2018; Sharma & Nuttal, 2016) has highlighted that “teacher preparation and attitudes have been cited as major factors contributing to either the success or failure of students with disabilities” (Kahn & Lewis, 2014, p. 885). If training programs continue to be situated in the medical model, they run the risk of deepening dispositions where disability is perceived as deficit as well as jeopardizing the academic success of disabled students.
Considering these findings, it is equally important to complicate the idea that some participants had “no prior experience” with disability. Given that approximately one in four people in the United States are disabled (Centers for Disease Control and Prevention, 2023), it is likely that all participants have engaged with someone with a disability at some point in their lives. As scholars (Kittay, 2011) have indicated, disabling environments are ubiquitous in our daily lives. However, since ableism often goes unchallenged, participants may not have noticed or recognized the presence of disabled individuals, as reflected in the present study.
Importance of Addressing Teachers’ Implicit Biases
Findings also indicate the need to address disability as an intersectional social identity, especially as it relates to teachers’ implicit biases. As defined in the DisCrit framework, disproportionality is compounded by the racial biases that underly certain disability categories. Students of color are more likely to be placed in “lower status” disability categories (e.g., intellectual disability and emotional disturbance) than their white peers (Fish, 2019; Hansen et al., 2023). These categories are considered lower status (compared to diagnoses like speech-language impairment, autism spectrum disorder, and other health impairment) because they are associated with greater social stigma and juvenile incarceration (Fish, 2019; Hansen et al., 2023). Since it is possible that some teachers have not had an opportunity to consider their biases, especially related to the medical model training they may have received, preservice and in-service teachers need to be presented with opportunities to unpack their beliefs and actions in practice. If they have never interrogated their dispositions regarding disability or race, they may not know how to evaluate their actions in practice (Sapon-Shevin, 2017).
Content Area Does Not Appear to Dictate Disability Definition
Data also revealed some demographic differences across the three groups of participants. Most notably, there were a few more social studies (39%) and science teachers (42%) and several more special education teachers (27%) categorized into DS than those in MM (21% social studies, 35% science, 7% special education) or MS (30% social studies, 30% science, 10% special education). These data suggest two things. First, they show that content area does not appear to dictate one’s disability definition, and equally importantly, they indicate that STEM (science, technology, engineering, and math) training does not necessarily correspond with a medical model approach to disability. Although medical model material may be embedded in STEM content (e.g., teaching about Down syndrome as a negative deviation from “normal” in biology class), teacher training rooted in the social model may balance a deficit-oriented approach. Findings from the current study also show that it is possible for special educators to not only navigate the tension between fixing the student or addressing the external barrier but also teach disabled students how to self-advocate.
Disability Identity Absent From Teacher Professional Development
Furthermore, data showed in-service professional development did not include disability as a minoritized identity. Forty-four participants (88%) shared that training on disability as a minoritized identity was nonexistent during the DEI training they received, with training instead centered on holistic inclusive approaches (i.e., responsive classroom). Part of the siloed nature of disability may be due to the legal aspects of special education, namely ensuring appropriate service delivery. As current research (C. O. Mueller, 2021; Roegman et al., 2018) has indicated, a compliance-based approach can perpetuate ableism, as it solidifies the idea that students with disabilities are non-normative and in need of fixing. Not including disability as a form of diversity furthers the rift between general education and special education. More specifically, it can reinforce the argument that disabled students are more “work” than nondisabled students and are the responsibility of the special education teacher, even when they are educated in a mainstream classroom (Baglieri & Lalvani, 2020). Thus, it is imperative that DEI spaces include disability to show all teachers that disabled students are “their” students and to raise necessary conversations about disability as related to other minoritized identities.
Recommendations
Research data indicate that the medical model is still pervasive in teacher training and highlight the relationship between training and disability discussion patterns. Even if teachers have self-acknowledged, significant prior experience with disability or maintain social model perspectives, they may need pedagogical tools to enact their beliefs. Based on the findings of this study, we offer the following recommendations to teacher training programs, PD, and schools.
Conduct Disability and DEI Audits
Teachers and administrators should be encouraged to examine their schools through the lens of disability. As related to accessibility, Baglieri and Lalvani (2020) have compiled a disability checklist that teachers can use to examine their respective school settings (pp. 91–92). Items include:
Doors may be opened using automatic openers.
Tables, desks, and counters have at least 27 inches clearance from the ground to bottom.
There is an adult in your school who can communicate and interpret using American Sign Language
In cases where the TEP, PD, or school addresses DEI, they can—and should—consider how and where disability is presented. Teachers and college professors can audit their syllabi and consider where and how disability is presented. Additionally, since disability is a diverse, intersectional identity, there are ways to bring disability into DEI. As previously stated, general education teachers rarely discuss disability (or disability identity) outside of their required, standalone class on working with disabled students. To rectify this issue and concretize disability’s place within a larger social justice framework, disability discussion should be infused across multiple general education courses; general and special education teacher educators could benefit from working together to learn about disability as an essential component of DEI (Hansen et al., 2024).
In addition to integrating scholarly work on disability as a minoritized identity, many disabled activists have discussed the intersection of race and disability by problematizing the ways that #disabilitytoowhite and highlighting the experiences of BIPOC (Black, Indigenous, People of Color) disabled individuals. Questions to consider when assessing the presentation of disability:
Is disability only discussed in relation to student services (i.e., IEPs, 504s, and related accommodations)?
Is disability explicitly included in discussions regarding minoritized identities?
Are the perspectives of disabled individuals included? If so, are the experiences of BIPOC disabled individuals included?
Is disability included in programmatic, school, and/or district DEI initiatives?
In addition to completing the checklists and considering the questions, teachers should be encouraged to discuss their responses. In cases of inaccessibility or where disability may have been absent from larger conversations about DEI, they should explore why these perspectives are missing and what they can do to make sure disabled voices are included.
Infuse Disabled Perspectives Into Training
It is imperative that training programs forefront the voices of disabled individuals. DSE offers myriad readings on ableism, disability rhetoric, and the social model of disability. Memoirs like Judy Heumann’s (2020) Being Heumann: The Unrepentant Memoir of a Disability Rights Activist; Alice Wong’s (2020) edited book, Disability Visibility: First-Person Stories from the Twenty-First Century; Keah Brown’s (2019) The Pretty One: On Life, Pop Culture, Disability, and Other Reasons to Fall in Love with Me; Haben Girma’s (2020) Haben: The Deafblind Woman Who Conquered Harvard Law; and Rebekah Taussig’s (2020) Sitting Pretty: The View from My Ordinary Resilient Disabled Body offer first-person accounts that show the range in variation in people’s experiences with disability. These texts can be incorporated as assignments or department- or college-wide book selections in universities with TEPs, and they can be chosen for teacher and/or school community working groups to discuss. Programs can also host film screenings that highlight the experiences of disabled people, such as the documentaries Crip Camp and Intelligent Lives. Additionally, programs can invite disabled activists to speak about their perspectives and the barriers they may have encountered, including their K–12 schooling experiences. Doing so may work to counteract medical model perceptions of disability that teachers may encounter.
Prioritize an Understanding of Universal Design for Learning
TEPs and PD are responsible for and often emphasize specific strategies for instructing students with disabilities. One option to consider is Universal Design for Learning (UDL), a proactive approach to planning, instruction, and assessment that involves anticipating educational, physical, and social/emotional barriers before they arise and providing all students (disabled and nondisabled) with multiple means of engagement, representation, and expression (CAST, 2018). UDL has the potential to expand the options to meaningfully include disabled students in the general education setting rather than relying on more exclusionary settings.
Rather than (or in addition to) teaching specific instructional strategies for teaching disabled students that may result in further medicalizing disability through a focus on remediation, TEPs and PD can introduce UDL as a framework to improve and optimize teaching and learning at all grade levels and in all subject areas. UDL guidelines can be applied to the design of instructional goals, methods, materials, and assessments (Meyer et al., 2014) to build flexible paths for learning.
To avoid pre- and in-service teachers viewing UDL as “just another” set of strategies, scholars (e.g., Cosier & Pearson, 2016; Freedman et al., 2019) have advocated specifically linking UDL to DSE to provide theoretical backing and frame the importance of using UDL within the context of the social model of disability. Importantly, UDL is a strengths-based framework, not one focused on remediation of weaknesses. Additionally, a recent meta-analysis of learners’ academic achievement in UDL environments (King-Sears et al., 2023) yielded a moderate positive combined effect for learners receiving UDL-based treatments (g = 0.43). A focus by teacher educators and providers of PD can support teachers to view disability as socially constructed rather than as a deficit (Sandoval Gomez & McKee, 2020).
Limitations
The most salient limitation of this research is self-report bias (Lincoln & Guba, 1985), as all data were gathered directly from the participants. Self-selection and nonrespondent bias are additional limitations of this research; it is possible that those who chose to respond to the call to participate were those who felt strongly about disability, either professionally or personally. This research was also mainly informed by interview data; thus, triangulation is limited (Maxwell, 2005). Although the percentage of secondary English teachers was consistent across the three groups, the overall sample skewed toward this content demographic.
Additionally, a component of this project is retrospective (i.e., asking participants to recall prior training). Retrospective study design poses two additional threats: (1) recall effect and (2) spoiler effect (Street & Ward, 2010). The more time that has passed since a participant experienced the event being studied, the greater the chances are of recall effects skewing the results of a study (Street & Ward, 2010). Spoiler effect can occur when “results are inadvertently skewed by researchers’ prior knowledge of the outcomes associated with a sequence of events” (Street & Ward, 2010, p. 827). Overall, while data strongly indicate that training played a significant part in shaping participant perceptions of disability and disability-related discussion, we cannot definitively prove that this is the case.
Conclusion
Building on the work presented in this research, future studies can work to generalize findings through quantitative survey measures, especially as related to subject area and disability discussion patterns. Additionally, training programs can draw on pre-post intervention surveys to determine the effectiveness of the recommendations—how, if at all, pre- and in-services teachers’ perspectives on disabilities change because of encountering a particular type of disability training. Taking this a step further, future work can also investigate the ways in which teachers enact their social model beliefs in the classroom, with an eye toward the impacts on disabled and nondisabled students. Also, while this research attended to elements of intersectionality and representation of disability in DEI spaces, the current study focused on teacher training as related to the presentation of disability. Future research can build on these findings by employing a deeper and more nuanced investigation of disability-related training using a DisCrit lens.
For classroom spaces to be fully inclusive and for disability to be valued as a minoritized identity, it is imperative that teachers receive social model training. Much work remains to be done in schools; in the United States, a focus on compliance and a tendency to present disability as medicalized and in need of “fixing” is particularly problematic. Looking more broadly, the negative response to disability during the height of the pandemic (e.g., when data for this research was collected) also underscores the need to raise disability awareness. During this time, disabled people were disproportionately affected by COVID-19, primarily due to their increased risk of poor outcomes from the disease, adverse social impacts of efforts to mitigate the pandemic, and reduced access to routine health care and related services (Shakespeare et al., 2021). Additionally, ableist language and disregard for the disabled were especially visceral. One such example is rhetoric intended to ease the concerns of the nondisabled U.S. population, as “public health officials, journalists, and politicians . . . have said explicitly, or implied, that whatever current form of Covid is under discussion can be regarded as . . . a little less worrying because it mainly sickens and kills elderly, chronically ill, and disabled people” (Pulrang, 2022). As highlighted in the present study, a key place to counter negative perceptions of and conversations regarding disability is within teacher training, as teacher educators—and future teachers—can present disability through an asset-oriented frame.
Working with TEPs to integrate social model training before teachers enter the classroom can provide them with a lens to identify marginalizing practices and the confidence to address disability in the classroom. Similarly, continued PD and support by school administrators around social model training can fortify teachers as they implement inclusive education and navigate disability discussions in school environments that are often deficit-driven and medicalized. Most importantly, infusion of the social model into training programs reinforces the idea that disabled students are everyone’s students, and they are entirely capable of success.
Supplemental Material
sj-docx-1-ero-10.1177_23328584241245089 – Supplemental material for From Deficit to Difference: Understanding the Relationship Between K–12 Teacher Training and Disability Discussion
Supplemental material, sj-docx-1-ero-10.1177_23328584241245089 for From Deficit to Difference: Understanding the Relationship Between K–12 Teacher Training and Disability Discussion by Christa S. Bialka, Nicole Hansen, Irene P. Kan, Danielle Mackintosh and Rebecca Jacobson in AERA Open
Footnotes
Appendix A
Appendix B
Appendix C
Acknowledgements
The authors would like to thank the participants for their time and insight, as well as the reviewers and editors for their valuable feedback.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work received funding from Villanova University’s Falvey Library Scholarship Open Access Reserve (SOAR) Fund.
Open Practices
1.
The authors use identity-first (e.g., disabled person) and person-first language (e.g., person with disability) throughout this paper to recognize disability as a complex social identity and to reflect the variety of ways that disabled people self-identify.
2.
Gender-inclusive pronoun.
3.
Authors
CHRISTA S. BIALKA is an associate professor in the Department of Education and Counseling at Villanova University;
NICOLE HANSEN is an assistant professor at Seton Hall University in the Department of Educational Studies;
IRENE P. KAN is a professor and cognitive neuroscientist with expertise in the cognitive architecture and neural bases of human memory and executive functions;
DANIELLE MACKINTOSH earned her master’s in school counseling at Villanova University and currently works as an elementary school counselor;
REBECCA JACOBSON is a secondary English teacher who earned her bachelor’s degree in education and English at Villanova University;
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.