
Abstract
Although quality center-based child care is helpful in promoting school readiness for dual language learners (DLLs), little is known about the nonparental child care that young DLL children experience. DLL status is often confounded with immigrant status, ethnicity, and poverty. Using nationally representative data from the Early Childhood Longitudinal Study–Birth Cohort, we examined child care experiences with repeated cross-sectional analyses at 9, 24, and 52 months for DLL and non-DLL children. After accounting for demographic and contextual factors, we found few differences in the quality and type of child care experienced by DLL children and children who hear only English in the home. Child care experiences were more related to country of origin, ethnicity, or immigrant status than DLL status. Nonparental caregivers were more likely to speak the child’s home language in home-based care than center care. Findings illustrate the importance of distinguishing among DLL status, socioeconomic status, ethnicity, country of origin, and immigrant status when considering the child care experiences of DLLs.
Keywords
The child care experiences of children in the United States have been widely studied in general, but we know less about the experiences of a growing segment of the population—young children whose families speak a language other than English in the home. Dual language learners (DLLs) are defined in this study as young children from homes in which a language other than English is spoken (exclusively or in addition to English). DLLs are the fastest-growing segment of the child population in the United States (Calderón, 2007), and their educational achievement has historically lagged behind monolingual English-speaking peers (August & Shanahan, 2006; Espinosa, 2010; Rumberger & Tran, 2010). For children with limited English proficiency, especially those growing up in poverty, the quality, type, and amount of nonparental care can make significant contributions to kindergarten readiness and help narrow the achievement gap throughout schooling (Goldenberg, Nemeth, Hicks, Zepeda, & Cardona, 2013; Gormley, Gayer, Phillips, & Dawson, 2005; Gormley, Phillips, & Gayer, 2008). Indeed, in several studies, DLL children have been found to reap the greatest benefits from pre-K programs (Burchinal, Magnuson, Powell, & Soliday Hong, 2015; Gormley et al., 2005; Gormley et al., 2008; Magnuson, Meyers, Ruhm, & Waldfogel, 2004; Peisner-Feinberg & Schaaf, 2011; Weiland & Yoshikawa, 2013).
However, before examining the effect of various types of early care and educational (ECE) programs on DLL children’s outcomes, we must first have a good understanding of the child care experiences of DLL children and then ask if these ECE experiences are different from children who hear only English at home. Also, because DLL status is obviously related to other potentially confounding variables (e.g., poverty status, parental education, immigrant status, country of origin, ethnicity) and the research and policy discourse is often concerned specifically with “DLLs,” it is important to tease apart the effect of DLL status per se on child care experiences while controlling for these other contextual variables. Thus, we examine use of nonparental child care, the quality of such care, and the languages spoken in care for DLLs during infancy, toddlerhood, and preschool, using nationally representative, cross-sectional ECLS-B data, with special care to control for other confounding variables. A deeper understanding of DLL children’s child care experiences will eventually help the design of ECE policies that promote improved outcomes for this growing group of DLL children (Garcia & Jensen, 2009).
Child Care Use: Family and Contextual Factors
Several conceptual models explain factors related to child care usage. All begin by recognizing that child care decisions are made within the context of family and community characteristics, culture, parent preferences, opportunities, and constraints (Chaudry, Henly, & Myers, 2010; Forry et al., 2013; Fram & Kim, 2008; Kim & Fram, 2009; Pungello & Kurtz-Coates, 1999; Weber, 2011). The child care selection model posited by Pungello and Kurtz-Costes (1999) helped guide the specific variables chosen for analysis in this study. Pungello and Kurtz-Costes identified four factors most important in explaining family usage of ECE services: maternal characteristics, child characteristics, parental child care preferences, and contextual factors present in the home and community. Since Pungello and Kurtz-Costes focused on infants and toddlers and included the general population of parents, we have extended the model to cover preschool-age children, focusing on families who speak a language other than English in the home. We used this conceptual framework with the empirical literature cited here to select the variables in the current investigation, with special attention to factors closely linked with, but separate from, DLL status (i.e., family socioeconomic status [SES], ethnicity, immigration status, and country of origin).
Language and Culture
Although much research has examined family and child factors associated with ECE use among the general population (Burchinal et al., 2015; Hirshberg et al., 2005; Loeb, Fuller, Kagan, & Carrol, 2004), few studies have examined factors associated with ECE experiences among DLL families. Some studies examining the child care patterns of DLL families have found that parents whose dominant language is not English are less likely than English-speaking families to use formal child care arrangements and more likely to use informal care, such as relatives and family child care (Cannon, Jacknowitz, & Karoly, 2012; Halle et al., 2009; Hirshberg, Huang, & Fuller, 2005). However, availability appears to be a factor in usage patterns for DLL parents, as they are more likely to enroll children in more formal, center-based ECE program when a greater supply is available (Hirshberg et al., 2005). Whether the caregiver speaks the home language also appears to influence child care choices among DLL families. Many parents of DLLs express a preference for child care providers who speak the child’s home language (Ward, Oldham LaChance, & Atkins, 2011). Yet, DLL families also express a desire for their children to learn English while maintaining their native language, which can affect child care choices (Vesely, 2013).
In much of the research to date, it is often unclear whether differences observed in DLLs’ child care use are due to family decisions related to home language or due to other factors related to child care usage, such as recent immigration, poverty, low parental education, and limited English proficiency (Capps, Fix, Ost, Reardon-Anderson, & Passel, 2005; Fortuny, Capps, Simms, & Chaudry, 2009). In the United States, many families with home languages other than English are likely to live in poverty and be born outside the United States (Zong & Batalova, 2015). Poverty and immigrant status are related to lower rates of child care use, especially to center-based care (Burchinal et al., 2015). Also, findings that “immigrants” (Karoly & Gonzalez, 2011; Magnuson, Lahaie, & Waldfogel, 2006; Miller, Votruba-Drzal, & Coley, 2013) or “Latinos/Hispanics” (Delgado, 2009) are less likely to use nonparental child care are useful, but such findings refer to ethnicity or immigrant status, not language status. Also, child care usage is linked specifically to family country of origin, regardless of ethnicity or DLL status. Mexican (and some other “Latino”) families are less likely to use center-based ECE programs, while immigrants from many Asian countries are actually more likely to use formal, center-based child care (Santhiveeran, 2010). Some have suggested that lower rates of center-based ECE services for Latino immigrants could be due more to their low-income status relative to other immigrant groups (rather than language status per se; Han, Lee, & Waldfogel, 2012). For these reasons, we examine specifically whether DLL status is related to child care usage at different ages, after controlling for all the other related factors.
Family Demographic Characteristics
Most families use some form of nonparental child care during their children’s early years. Beginning in the child’s first year, >50% of all children experience nonparental child care, and by the preschool years, >75% of children are in some type of nonparental child care (Federal Interagency Forum on Child and Family Statistics, 2011). SES is a strong predictor of child care usage (Burchinal et al., 2015). Not surprising, families are most likely to use child care when parents are employed; increases in maternal employment over the past 40 years largely account for the high proportion of children in child care (Burchinal et al., 2015). Furthermore, families are more likely to use child care, center-based care in particular, when mothers have more education (Early & Burchinal, 2001; Fuller, Holloway, & Liang, 1996; Fuller, Holloway, Rambaud, & Eggers-Pierola, 1996; Johansen, Leibowitz, & Waite, 1996; National Institute of Child Health and Human Development Early Child Care Research Network [NICHD ECCRN], 2006), when families have more income (Early & Burchinal, 2001; NICHD ECCRN, 2006), or when the mother is single (NICHD ECCRN, 2006). Ethnicity has also been linked to child care participation in the general population. Black parents are more likely than White parents to select center-based ECE programs for their children (Liang, Fuller, & Singer, 2000; Magnuson & Waldfogel, 2008), whereas U.S.-born Latino/Hispanic parents are less likely than White parents to enroll their children in formal, center-based arrangements (Buysse, Castro, West, & Skinner, 2005; Magnuson & Waldfogel, 2008). Children are also more likely to experience higher-quality care when parents have higher incomes and more education (Burchinal et al., 2015).
Child Characteristics
Child age is related to child care type. Infants and toddlers are more likely to experience care in home-based settings (e.g., by relatives or in family child care homes), whereas preschoolers are more likely to experience center-based care (Early & Burchinal, 2001; NICHD ECCRN, 2006). Some studies suggest that child gender is also a factor, with boys more likely to be enrolled in center-based ECE services rather than parental care (Fuller, Holloway, & Liang, 1996).
Quality of ECE Programs and Language of Instruction
As quality of care is important for positive outcomes (Friedman-Krauss, Barnett, & Nores, 2016; Weiland & Yoshikawa, 2013), it is important to examine (as we do) the quality of the ECE services experienced by DLL children compared with children who speak English at home. Quality of care for DLLs has not been studied as much as use of ECE programs. Some research suggests that DLL children, when they do attend child care programs, are more likely than non-DLLs to experience poor-quality care (Karoly & Gonzalez, 2011; Matthews & Ewen, 2006). If indeed DLL children are systematically exposed to lower-quality care in early childhood, that is likely a contributing factor to the achievement gaps observed during kindergarten. Finally, language of instruction in ECE settings appears to play a role in outcomes for DLL children (Goldenberg et al., 2013). The use of the home language during interaction and instruction in child care contributes to DLLs’ overall development (Barnett, Yarosz, Thomas, Jung, & Blanco, 2007; Chang et al., 2007; Durán, Roseth, & Hoffman, 2010). Thus, we also report on the languages used in the ECE settings for the DLL children.
Current Study
A number of gaps exist that limit a deep understanding of child care usage patterns and experiences among DLL families. First, none of the previous studies discussed is a prospective, nationally representative examination of children from infancy to entry to kindergarten. Second, some studies have grouped very heterogeneous cultural groups of Spanish-speaking individuals (e.g., Mexican-origin families in the Southwest vs. Puerto Rican families in New York vs. Cuban families in Miami—groups that are very different in culture, resources, and immigration histories) into one panethnic category, such as “Latino,” when child care values, access, and resources are likely to be quite different across these groups (Hirshberg et al., 2005; Liang et al., 2000; Loeb et al., 2004). Third, much of the work examining ethnic and language group differences in child care choices has focused on Mexican-origin families (Crosnoe, 2012), and even when national samples of Latinos/Hispanics are examined, they often overrepresent Latinos from Mexico, as in the Early Childhood Longitudinal Study–Kindergarten Class (Fram & Kim, 2008; Magnuson et al., 2006; Turney & Kao, 2009). Most important, the literature on child care use among DLLs has often failed to sufficiently distinguish among ethnic status, immigration status, country of origin, and DLL status—four related but clearly different constructs (Liang et al., 2000; McWayne, Campos, & Owsianik, 2008). So it is not clear whether differences observed in child care usage are due to language status in the home or to ethnicity, country of origin, or immigration status.
To address these gaps in previous research, we use nationally representative data from the Early Childhood Longitudinal Study–Birth Cohort (ECLS-B) to describe the child care experiences of DLL and English-only (EO) children during infancy, toddlerhood, and the preschool years. These are the most recent nationally representative data that measure home language, immigrant status, demographics, and child care experiences from infancy through the preschool years in a sample designed to include children from multiple countries of origin. These data allow us to examine DLL status while taking into account immigration history, ethnicity, and other demographic characteristics. Using the ECLS-B, we compare DLL and monolingual English-speaking children’s child care experiences to identify potential differences in use of child care, type of care, quality of care, and use of home language by the providers for DLL children when they were infants, toddlers, and preschoolers. The following research questions were addressed:
Question 1: After accounting for other relevant variables (family demographics, immigration status, country of origin), is home language related to whether a child experiences nonparental care and, if so, to the type and quality of that care in infancy, toddlerhood, and the preschool years?
Question 2: Among DLL children, what variables relate to whether they are in child care settings in which the caregiver speaks the child’s home language?
Method
Participants
The ECLS-B is a nationally representative sample of 14,000 children born in the United States in the year 2001. The children were recruited from diverse socioeconomic and racial/ethnic backgrounds with oversamples of Asian and Pacific-Islander children, American Indian and Alaska Native children, Chinese children, twins, and low birth weight children. About 21% of the recruited sample reported using a language other than English at home. Children were followed from their recruitment (prior to 9 months old) into kindergarten. Additional details on the full ECLS-B sample are available (IES National Center for Education Statistics, n.d.). As required by ECLS-B data usage agreements, sample sizes are rounded to the nearest 50. All descriptive statistics and analysis results have been computed separately by wave of data collection based on the sampling weights for that wave, so reported findings are representative of the cohort of children born in the United States in 2001. Table 1 provides demographic information.
Descriptive Statistics by Language Status and Age

Note. ITERS = Infant/Toddler Environmental Rating Scale; FDCRS = Family Day Care Rating Scale; ECERS-R = Early Childhood Environmental Rating Scale–Revised Edition.
It is important to note that the sample sizes necessarily vary from analysis to analysis, depending on how many children are present in the sample at each wave (9, 24, 52 months) and how many are in child care at each wave. Some analyses pertain just to those children who are in care at a certain time frame, affecting the n values as well. Also for child care quality analyses, only a 25% random sample of child care settings was assessed for quality by the ECLS-B. Finally, for questions about language used in the child care setting, there are different informants (parent vs. teacher), with differing amounts of missing data for relative versus center-based care.
Measures
Data were collected through direct assessments of the children, observations of parent–child interactions, and interviews with the primary caregiver, typically the mother, when the children were 9 months old, 24 months old, and around 52 months (just prior to kindergarten). Parents/guardians were asked to provide information about their children and themselves. The parent interview included two instruments: the interview and the Parent Self-Administered Questionnaire. The first was conducted in person by trained field interviewers using computer-assisted personal interviewing (CAPI) as part of the home visit. The Parent Self-Administered Questionnaire was a paper/pencil instrument, presented during the parent CAPI for the respondent to complete and return in a provided envelope, and it contained 23 questions on topics that some people might prefer to answer privately. All the data for this study were from the CAPI. The interviews were translated into Spanish and the languages of many of the major Asian countries, and they were conducted as such when parents indicated that they preferred the non-English version. Parent interviews included questions related to home language and heritage country and whether the target child experienced nonparental care for at least 10 hours per week and, if so, the type, quantity, and language use while in care.
Home language
The ECLS-B included questions about home language use. Two home language groups were created—English only and other language used at home (exclusively or in some combination with English)—from questions that parents answered about the languages spoken at home. Parents were asked, “What is the primary language spoken in your home?” To answer, they chose from a list that included English and 22 other languages. They were then asked if another language was spoken in the home and, if so, to indicate the primary language spoken in the home by selecting among the list of English and 22 other languages. For the purposes of this article, DLL status was determined as indicating that a language other than English was a primary language spoken in the home, regardless of whether that was the sole language used by the family at home or used in combination with some English. Sample size limitations did not allow us to categorize language used in the home into more discrete categories (i.e., varying amounts of English and a heritage language spoken in the home). To control for the key categorical covariates (i.e., ethnicity, country of origin, immigrant status) and use them as interaction terms, we could not reduce the home language groups any further.
Child care use
The parent interviews included questions about the child care experiences of the target child when the child was 9 and 24 months of age and during the winter of the final preschool year—about 52 months of age on average. Center-based care was indicated when parents positively answered either of two questions: “Is [child] currently attending Head Start on a regular basis?” or “Is [child] now attending a day care center, nursery school, preschool, or pre-kindergarten program on a regular basis?” Relative care was indicated when parents answered this question positively: “Is [child] now receiving care from a relative other than a parent on a regular basis, for example from grandparents, brothers or sisters, or any other relatives?” Nonrelative child care home was indicated when parents positively answered this question: “Is [child] now receiving care in a private home on a regular basis from someone who is not related to him/her?”
Care quality
A 25% random subset of families with 10+ hours/week of care was selected by the ECLS-B to have their child care setting observed to obtain quality ratings in the 24-month and preschool data collection waves. Children who lived in Alaska, Hawaii, or on reservations or who attended a care setting in which neither Spanish nor English was spoken were not eligible for observation. Child care quality was assessed by three widely accepted measures of child care quality. The Early Childhood Environmental Rating Scale–Revised Edition (Harms, Clifford, & Cryer, 2005) measures quality of center care for preschool classrooms. It consists of 43 items that yield an overall score and subscale scores measuring learning activities, listening and talking, program structure, interaction, personal care routines, and furnishings. The Family Day Care Rating Scale (Harms & Clifford, 1989) measures quality in family day care settings and is similar in structure to the Early Childhood Environmental Rating Scale–Revised Edition, with 40 items. The Infant/Toddler Environmental Rating Scale (Harms, Cryer, & Clifford, 1990) was used at the 24-month visit and examines interactions with adults and peers, exposure to materials and activities, the extent to which routine care needs are met, and the furnishings. We used the total quality score on the Infant/Toddler Environmental Rating Scale (α = .86), which contains 29 items. On all measures, items are scored from 1 to 7, with higher scores indicating better-quality care (1 = inadequate, 3 = minimal, 5 = good, 7 = excellent).
Language of child care
Parents who reported speaking a language other than English at home were asked to describe the language used in the child care setting. They were asked if the adult caregiver in relative care or child care homes spoke the family’s primary language. Teachers in the randomly selected child care quality subsample were asked what was the primary language used in the child care setting. We used parental report for relative and child care homes because it was available for all children. We used the caregiver’s report regarding center care because parents may not know what languages are spoken in the classroom. It is important to note that both measures fail to indicate the amount of heritage language actually used daily in the child care setting. For parent report, it is more whether the caregiver can speak the home language (not what language she or he does use), and for the teacher measure, it indicates a rough perception of the language used (not an observed percentage of time that the language is actually used).
Key covariates
Mothers were asked if they were born in the 50 U.S. states or the District of Columbia, and this was used to create the immigrant status variable. Parents were also asked about country/territory of origin: “In what country or territory were you born?” Only countries/territories that had >50 people included in them could be examined, given ECLS-B data usage agreements. The following countries/territories were examined: Mexico, Puerto Rico, Cuba (each sample size: 50 < n < 1,250) and India, China, Japan, Korea, and Vietnam (each: 50 < n < 550).
Child gender, race, and ethnicity, as well as family income and maternal and paternal education, were assessed through the CAPI. The target child’s gender was obtained from the child’s birth certificate, and during the 9-month interview, parents confirmed gender by responding to the following: “I have [child] recorded as [male/female]. Is that correct?” The child’s race and ethnicity were determined at the 9-month interview; parents were asked to describe the child’s ethnicity by selecting one or more from a list that included 14 categories. They were also asked, “Is [name] of Spanish, Hispanic, or Latino origin?” and, if so, “Which one or more of these groups is [name]?” (choosing from Mexican/Mexican American/Chicano, Puerto Rican, Cuban, or another Spanish/Hispanic/Latino group). A similar process was used for children of Asian descent, asking if country of origin was India, China, Vietnam Korea, or Japan. Family income was assessed in all waves of data collection; parents were asked, “What was your total household income last year, to the nearest thousand?” and “What was the total income of all persons in your household over the past year, including salaries or other earnings, interest, retirement, and so on for all household members?” To assess parental education, parents were asked the following: “What is the highest grade or year of school that you have completed?” “Do you have a high school diploma or its equivalent, such as a GED?” (if so, “Which do you have, a high school diploma or a GED?”), and “Are you currently attending or enrolled in any courses from a school, college, or university?” Parental education was computed as the mean of the mother’s and father’s reported educational levels (if only one parent was present, the primary parent report was used). Finally, we included, as covariates, information from questions about household composition—including whether the household included the mother and father and how many children were <18 years old.
Data Analysis
Descriptive statistics were computed for the two language groups, and inferential analyses addressed our research questions. Separate cross-sectional analyses examined whether the child care experiences at 9, 24, and 52 months varied by DLL status. Cross-sectional analyses were conducted instead of longitudinal analyses for conceptual and practical reasons. Conceptually, this approach describes child care use for DLLs at the three distinct age periods during early childhood (infancy, toddlerhood, preschool) rather than focusing on changes in ECE experiences across these periods. Practically, longitudinal analyses were not possible if models allowed categorical factors such as ethnicity or immigration to relate to change in the use of child care over time. To the extent that there are family characteristics that differentiate who enrolls children in care or in different types over time, longitudinal analyses that would not accommodate those changes might yield biased estimates for related factors such as DLL status. Our focus on whether factors such as ethnicity and immigration status related to child care use differ depending on DLL status could be examined in cross-sectional analyses but not in longitudinal analyses, because the number of families with changes in child care use over time within these cells was too small in some cells for stable estimation in longitudinal analyses.
Logistic regressions were used to analyze the part of Question 1 that had to do with whether the target child was in child care (1 = yes, 0 = no) at 9, 24, and 52 months. For children whose parents reported any nonparental care at a given data collection wave, logistic regressions again analyzed the part of Question 1 pertaining to the primary type of care used to compare children in relative care (1) with children in all other types of care (0), children in child care homes (1) with children in all other types of care (0), and children in child care centers (1) with children in all other types of care (0). Multiple regressions were used to analyze quality of care. Similar logistic regression analyses were used for Question 2 about predictors of language used in the care setting (1 = home language, 0 = not).
All analyses focused on whether child care experiences differed among DLL children and children whose families only spoke English, and they included related family characteristics as covariates: whether the mother was native born or immigrated to the United States, the region of origin (Mexico, Puerto Rico, Cuba, India, China, Japan, Korea, or Vietnam), the child’s gender and race/ethnicity, the family’s income, and parental education. Interactions between DLL status and both immigrant status and Hispanic background were included to test whether differences related to DLL status were larger when families were immigrants or when families were from Hispanic backgrounds. Ideally, we would have also crossed DLL status with country of origin, but there was too little variability in DLL status among families within many of the country-of-origin groups to test for differences in DLL effects across country of origin.
All variables were mean centered, including the categorical variables. This resulted in effect-coded parameter estimates in which the main effect for a given predictor was estimated at the mean for continuous variables included in interactions with that predictor and across all levels of categorical variables included in interactions with that predictor. Effect sizes were computed. The odds ratios (ORs) were computed from logistic regressions of categorical child care variables (e.g., use of child care, type of child care, whether the caregiver spoke the home language). For example, the OR for DLL status from an analysis of whether the child experienced child care at 9 months would be computed as the odds of attending child care for DLLs at 9 months over the odds of attending care for non-DLLs. Standardized mean differences (d) were computed from the multiple regressions (e.g., quantity and quality of care). Standardized mean differences represent the difference between two groups in standard deviation units in the outcome variable.
Results
The descriptive statistics presented in Table 1 list demographic characteristics and child care experiences for families of DLLs and EO children. The families of DLL children tended to report lower levels of parental education and family income and were more likely to have a mother who immigrated to the United States or who reported one of the selected heritage groups as the family’s region of origin.
Use of Child Care
The first set of analyses asked whether DLL and EO families differed in their use of child care when the target child was an infant, toddler, and preschooler. Descriptively, the proportion of DLL children in child care was slightly lower than the proportion of EO children in child care at all ages. About one-third of the DLL children and half of the EO children were in child care at 9 and 24 months, whereas about two-thirds of DLL children and three-fourths of EO children were in child care at 52 months. Logistic regressions compared children who were in ECE programs for any amount of time per week and children who were cared for exclusively by their parents. Results are shown in Table 2. The second row of Table 2 shows the main effect of home language; the next rows show the coefficients for the covariates; and the last set of rows shows the coefficients for the interactions involving DLL and both Hispanic and maternal immigrant groups.
Comparison of Children in Child Care or Exclusively Parental Care
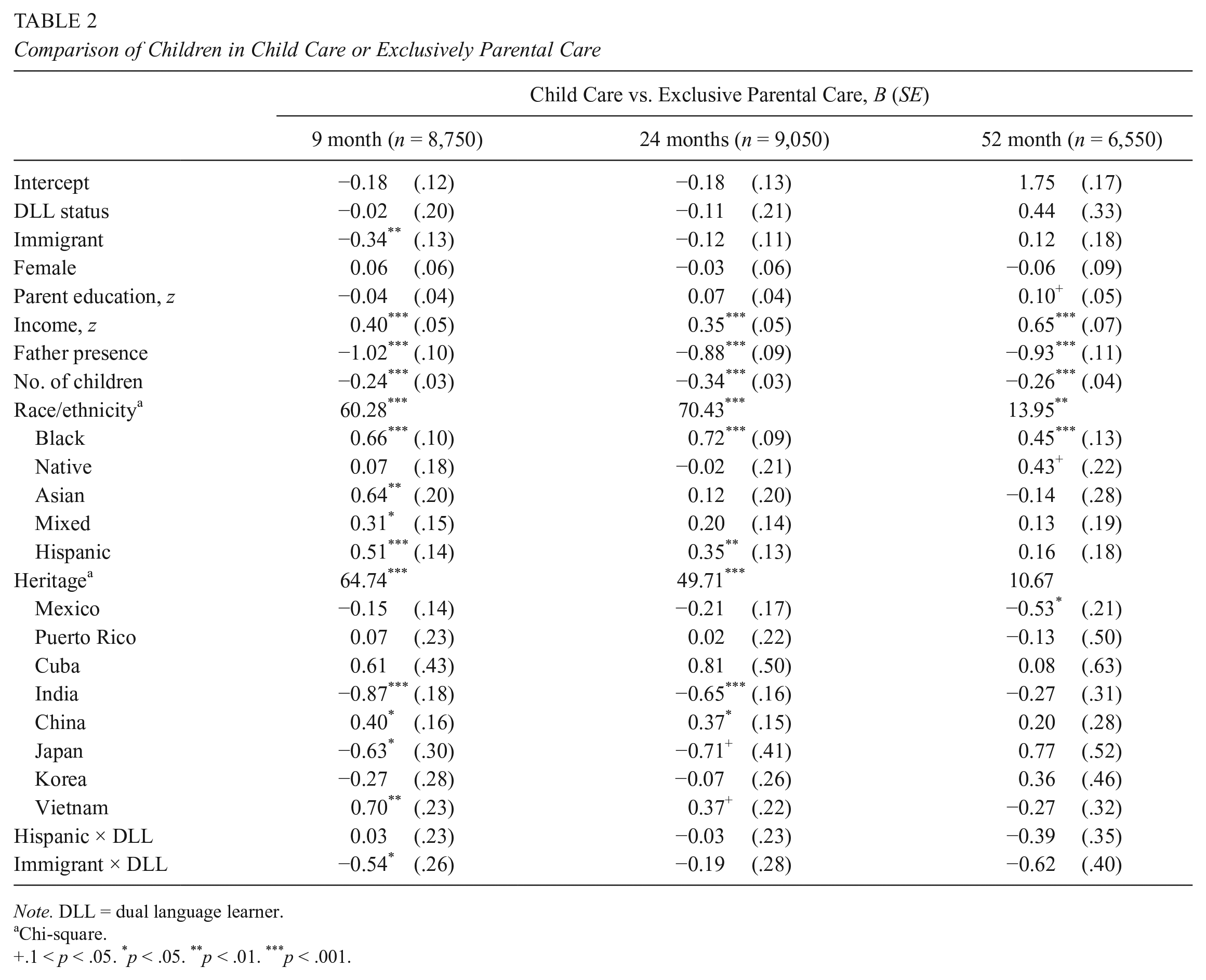
Note. DLL = dual language learner.
Chi-square.
+.1 < p < .05. *p < .05. **p < .01. ***p < .001.
As shown in Table 2, the only statistically significant DLL finding involved an interaction between immigrant and DLL status in the use of nonparental care at 9 months (B = −0.54). There were no reliable differences between DLL and EO families in whether children received nonparental care at 9, 24, or 52 months, after adjusting for the other variables in the model. Mothers who immigrated to the United States were less likely to use child care at 9 months (OR = 0.71), and this difference was even larger for DLL parents (OR = 0.41). Neither the main effects for immigration status nor the interactions involving DLL status were statistically significant at subsequent ages, suggesting that use of nonparental care did not differ in DLL and EO families later. Other variables (ethnicity, income, father presence, and country of origin) were more important in predicting use of nonparental care than DLL status. For example, Black and Hispanic families, some Asian families, and those with more income were more likely to use care, whereas those from India, those with fathers, and those with more siblings at home were less likely to use nonparental care.
Type of Care
The next set of analyses asked whether DLL and EO children differed in terms of the type of care that they attended as infants, toddlers, and preschoolers (relative, family child care, center). These analyses focus on the primary child care setting reported by parents and exclude children who were cared for solely by their parents; thus, sample sizes in the logistic regressions are smaller than in Table 1. Descriptively, about half to two-thirds of DLL children and only one-third to less than half of the EO children in child care were cared for by their relatives as infants and toddlers. Table 1 also shows a clear normative shift from home-based care for infants and toddlers to center care for preschoolers for DLL and EO children. Separate analyses were conducted for each type of care for each age, through the same overall model as described earlier that adjusted for demographic characteristics, country of origin, and maternal immigration status. Coefficients are shown in Table 3, and they compare children in one type of care with children in all other types of care.
Type of Child Care and DLL Status

Note. Values are presented as B (SE), unless noted otherwise. Analyses included only children in child care, and comparisons were made within each type of care, comparing children in relative care to children in all other types of care, children in child care homes with children in all other types of care, and children in centers with children in all other types of care. DLL = dual language learner.
Chi-square.
+.1 < p < .05. *p < .05. **p < .01. ***p < .001.
Relative care
The use of relative care differed among DLLs and EOs at 9 and 24 months but not at 52 months. DLL children were more likely than EO children to be in relative care at 9 months (OR = 3.42) and at 24 months (OR = 1.84), as evidenced by the significant coefficients for DLL group in the row labeled “DLL.” In addition, DLL status interacted with Hispanic ethnicity at 9 months (B = −0.76) and with maternal immigration status at 9 months (B = −1.23) and 24 months (B = −0.81). The Hispanic × DLL interaction indicated that use of relative care at 9 months was rarer among Hispanic DLL families than among non-Hispanic DLL families. Similarly, the Maternal Immigration × DLL interaction indicated that use of relative care at 9 and 24 months was rarer among immigrant DLL mothers than among U.S.-born DLL mothers.
Child care homes
DLL and EO children differed in their use of family (nonrelative) child care homes at 9 and 24 months but not at 52 months. Overall, DLL children were less likely than EO children to experience a child care home at 9 months (OR = 0.33) and 24 months (OR = 0.39). However, the differences between DLL and EO children’s use of child care homes varied depending on the mother’s immigration status. Among DLL families, immigrant mothers were much more likely than U.S.-born mothers to place their 9-month-old children (B = 1.52) and 24-month-old children (B = 1.05) in a child care home.
Center care
No differences emerged between DLL and EO children in use of center care at any age. As noted, other variables (e.g., ethnicity, income, and education) were more associated with type of care than DLL status. For example, Black families and some Asian groups (those from India and China) were more likely to use center-based care at 52 months. This highlights the need to examine country of origin and to avoid panethnic generalizations (i.e., “Asian”) because there is important variation in ECE use within “Asian” groups, and that variation matters more for ECE use than DLL status.
Child Care Quality
Next, we asked whether DLL and EO children differed in the quality of their child care experiences. These analyses involved the 25% random subsample of children in child care that had quality data; thus, sample sizes are smaller than those shown in Table 1. The unadjusted means for the quality measures show similar means for DLL and EO children in center care at 24 months (Infant/Toddler Environmental Rating Scale—the infant/toddler center measure) and at 52 months (Early Childhood Environmental Rating Scale–Revised Edition—the preschool-age center-based measure) but lower means for DLL children than EO children for those in relative and home-based care at 24 and 52 months. Results from these analyses with covariates are shown in Table 4. DLL and EO children did not differ significantly in the quality of care at 2 years or in the quality of center care at 52 months. The quality of home-based care at 4.5 years was significantly lower for DLL than for EO children (d = 0.65), especially for DLL children who were not Hispanic (B = 1.47), but the relatively small number of children in home-based care at this age raises questions about the findings for this setting and age. As noted earlier, variables such as parental education and ethnicity were stronger predictors of child care quality than DLL status was.
Child Care Quality and DLL Status

Note. Analyses included only children in child care. DLL = dual language learner; ITERS = Infant/Toddler Environmental Rating Scale; FDCRS = Family Day Care Rating Scale; ECERS-R = Early Childhood Environmental Rating Scale–Revised Edition.
+.1 < p < .05. *p < .05. **p < .01. ***p < .001.
Home Language Use in Child Care
Our second research question had to do with what proportion of DLL children in ECE programs are in settings where the caregiver speaks the child’s home language and what predicts the use of the home language in the child care setting. These analyses involved only DLL children. Descriptively, more than three-fourths of the DLL children in child care had a provider who spoke their home language when they were infants and toddlers, but that proportion fell to 42% when they were preschoolers. These proportions varied depending on the type of care. At 2 years, the caregiver spoke the home language for 93% of the 400 DLL children who were cared for by a relative and 86% of the 200 DLL children who were cared for in a child care home by a nonrelative adult. Similarly, at 52 months, the caregiver spoke the child’s home language for 89% of the DLL children in relative care and 90% of the DLL children in child care homes. In contrast, the child’s home language was a strong language used in the classroom for only 23% of the 150 DLL children attending centers at 24 months and 26% of the 750 DLL children attending centers at 52 months.
Results from multiple regression analyses on predictors of using the home language in care are provided in Table 5. These results suggest that type of care and whether the child was Hispanic were strong predictors of whether the child had a provider who spoke his or her home language. Most of the DLL children were cared for by a caregiver who spoke the same language if they were in relative care or home-based care but not if they were in center-based care. Results indicated that, as compared with DLL children in relative care, DLL children were significantly less likely to have a provider who spoke the home language if they were in a child care home at 9 months (OR = 0.33) or a child care center at 9 months (OR = 0.05), 24 months (OR = −0.02), or 52 months (OR = 0.04). Hispanic DLL children were more likely to have providers who spoke Spanish than were other DLL children to have providers who spoke their home languages at 9 months (OR = 4.10), 24 months (OR = 2.75), and 52 months (OR = 3.03).
Bilingual Care Among DLL Children in Child Care

Note. Values are presented as B (SE), unless noted otherwise. Analyses included only children in child care. DLL = dual language learner.
Chi-square.
p < .05. **p < .01. ***p < .001.
Discussion
The current study compared the child care experiences of children living in homes where a language other than English was spoken and children who were exposed to only English at home, through a large, diverse, nationally representative data set: the ECLS-B. These analyses suggest that there were relatively few differences in the child care experiences among DLL children and non-DLL children after accounting for important differences related to SES, immigration, ethnicity, and country/region of origin. Some interactions emerged, suggesting differences in child care experiences among DLL children related to the immigration status of the mother and ethnicity. These findings are discussed in comparison with prior research on the use of ECE services for DLL children.
Prior research has often concluded that Latinos/Hispanics, immigrant families, or DLL children are less likely to attend child care at all and, if they do, they tend to prefer family- or home-based care over centers (Buysse et al., 2005; Chernoff, Flannagan, McPhee, & Park, 2007; Halle et al., 2009; Hirshberg et al., 2005; Iruka & Carver, 2006; Magnuson & Waldfogel, 2008; Matthews & Ewen, 2007). The unadjusted bivariate analyses in this study also found that DLLs were less likely to be in care, more likely to use relative care, and less likely to use center care. The regression analyses, however, suggested that these differences were due to conflating DLL status with other family characteristics, such as ethnicity, country of origin, immigrant status, and SES. These analyses yielded little to no evidence that DLL status is the distinguishing factor in families’ use of child care within this nationally representative data set. This finding has implications for researchers and policy makers, suggesting that discussions may need to be more nuanced. Whereas policy discussion in ECE programs often tends to focus on DLL status, our findings suggest that ECE use is more strongly related to factors other than home language.
Several findings pertaining to these other family characteristics and whether children were enrolled in child care may be of particular interest. Results indicated that Latino/Hispanic children were actually more likely to be in care at 9 and 24 months than the rest of the sample, when controlling for the other variables. Families in which the mother was an “immigrant” were less likely to be in nonparental care than nonimmigrant families but only at 9 months and not during the toddlerhood or preschool periods. Country/region of origin was related to use of child care for one group—families from Mexico—suggesting that Mexican American families, as compared with other families, were less likely to use any child care during the preschool period. Given complexity and interactions related to ethnicity, immigration status, and country/region of origin, results from our analyses suggest that it is not the case that “DLLs” or “Latinos,” in general, are using ECE services at lower rates throughout the early childhood years.
Similarly, in contrast to prior work, relatively few differences related to DLL status were found in type of care, after adjusting for family characteristics. DLL children were more likely to be in relative care than EO infants at 9 months and less likely to be in child care homes at 24 months. Children whose mothers were immigrants were more likely than other children to be in center care as preschoolers, after accounting for the other family variables. Latino/Hispanic status was never associated with type of care attended at any age; however, being of Mexican origin was associated with a greater likelihood of attending relative care and with less chance of being in a center at 52 months.
As with type of care, few differences between DLL and EO children emerged in analyses of quality of care. The quality of home-based care among preschoolers was lower among DLL children than EO children, but it is important to note this type of care was not commonly used by either group of children at that age. Again, when controlling for other relevant contextual variables, we do not find the quality of child care attended by DLL children to be lower in the most commonly used settings, as others have found using samples of convenience that may not have variability on these other family factors (Karoly & Gonzalez, 2011; Matthews & Ewen, 2007).
As in prior studies, this study shows that, overall, DLL children are exposed to the home language in child care less and less as they get older. Among children enrolled in child care, DLL children, especially Hispanic DLL children, were very likely cared for by someone speaking their home language as infants and toddlers. By 52 months, only 42% of DLLs experience at least some amount of the heritage language in care. This reduction in use of the home language reflects the change from relative care as the most frequent type of care for infants and toddlers to center care as preschoolers. Relatives were most likely, and caregivers in centers least likely, to use the home language. Recent scholarship emphasizes the importance of at least some use of the home language in ECE programs (Barnett et al., 2007; Chang et al., 2007; Durán et al., 2010), and this is an important area for future research—to better understand the actual language experiences that DLL children are having across care settings and the associated child outcomes.
Several interactions provide further evidence that researchers need to carefully separate and investigate contextual nuances when examining child care issues among different groups of ethnic minorities, DLLs, or immigrants. For example, although DLL status showed no main effect on children being in nonparental care during infancy, there was an interaction with immigrant status indicating that immigrant mothers who were DLLs were less likely to use some kind of child care at 9 months. Similarly, use of relative care at 9 months was greater among non-Hispanic DLL families than among Hispanic DLL families. Also, selection of relative care at 9 and 24 months was greater among U.S.-born DLL mothers than among immigrant DLL mothers. Finally, quality of home-based care was lower among DLLs at 52 months but only for non-Hispanic DLLs. Clearly, such interactions among DLLs status, immigration status, and ethnicity indicate the need to avoid drawing broad conclusions regarding the child care experiences of all DLLs.
In summary, this study shows few systematic differences between families of DLLs and those of monolingual English children in their child care use. Thus, it does not appear to be DLL status per se that is related to families’ child care choices. Country of origin showed stronger relations with child care use than did Hispanic or DLL status. This suggests that researchers examining cultural differences in child care need to specify not only the specific heritage groups they are studying (i.e., avoiding panethnic categories such as “Latino” or “Hispanic” or “Asian”) but also which cultural construct they are examining: Is it cultural values, having roots to a particular country, immigration status, DLL status, or ethnicity that is driving family child care decisions? In infancy, relative care may be related to both availability and cultural and linguistic consistency. The finding that bilingual care is rarely found in child care centers may be a deterrent to the participation of DLLs during the earliest years. It is also possible that a desire to expose children to English may underlie DLL child care choices during the year prior to kindergarten.
Limitations
First, none of our analyses allow for causal inferences. Second, although this study used a nationally representative sample, included three important periods within early childhood with respect to child care, and teased apart DLL status from SES, ethnicity, country of origin, and immigrant status, there are limitations that need to be addressed in future studies. In the ECLS-B, center-based care included child care centers, private nursery schools, community preschools, prekindergarten programs, as well as Head Start. These different types of center-based care have been shown to vary on important features such as teacher qualifications, quality of instruction, and family engagement (Barnett et al., 2007). Since this category of child care includes all forms of center-based care, it is not possible to disentangle whether child care use for DLL families was related to availability, affordability, or other characteristics of the programs.
Third, it is important to note that the ECLS-B is >15 years old and that child care availability is dynamic and may have shifted over time. The ECLS-B may still be the only large nationally representative longitudinal data set that permits controlling for related demographic variables and disentangling DLL status from ethnicity, country of origin, and immigrant status. Nevertheless, economic and cultural changes since that time may also change child care experiences for DLLs. Economic conditions during the years of the ECLS-B (2001–2006) likely influenced the need for and availability of child care. This was a time when economic conditions were relatively robust and child care options were increasing, but that changed in 2008. Furthermore, with the recent expansion of federal and state funding for ECE services that target children who are from immigrant, low-income DLL families, there may be more nonparental care available for DLLs than in the past (Burchinal et al., 2015). Indeed, the proportion of DLL children in Head Start (Moiduddin, Aikens, Tarullo, West, & Xue, 2009) and in the North Carolina Prekindergarten Program (Peisner-Feinberg & Schaaf, 2011) has increased over the past 10 to 15 years. Studies have also found that access for low-income families accounts for much of the enrollment differences between children with immigrant parents and those with U.S.-born parents (Hernandez, Denton, & MaCartney, 2008). It may be that families of DLLs are becoming more aware of the child care services in their communities and deciding to take advantage of ECE services like the majority of families in the United States.
Fourth, this data set yielded information about the languages that caregivers spoke and their stated language usage, but no detailed information about the language actually used in the child care setting was available. There is no guarantee that children in settings where the caregiver spoke the home language experienced high-quality home language input, and we know nothing about what language the children may have used in the setting. Recent studies on language exposure and usage during the preschool years are suggesting that language usage is critical to overall language development, not just exposure (Hammer et al., 2014). Furthermore, data collection procedures for the ECLS-B study asked only families who reported speaking a language other than English in the home about the language of the child care setting. Yet, it is possible that children from EO households had a caregiver who spoke another language.
Fifth, future examination of immigrant status should provide additional details about the immigration experience, including specifying how long the mother had been in the United States. Knowing whether the mother is a recent immigrant or whether she has been in the United States for many years is likely related to additional contextual information, such as opportunities for forming social networks, acquiring English, and building on social capital acquired in the country of origin. Also, we tried to interpret only the more clear and robust patterns. The relatively small numbers of DLL children within specific countries of origin limited our ability to understand the quality of ECE services for DLL children by country of origin, which may be importantly related to ECE usage patterns. Finally, the ECLS-B quality-of-care measure tapped only global quality, which does not include suggested practices to meet the needs of DLL children, such as use of the home language by the provider, materials available in other languages, and bilingual assessment practices, among others (Peisner-Feinberg et al., 2014).
Conclusions
Our results suggest that researchers and practitioners need to revisit the simple notion that a large and sometimes vaguely defined group, such as “Hispanics,” “Latinos,” “immigrants,” or “DLLs,” is reticent to send its children to center-based care and instead prefers family-based and informal child care arrangements. We show that this is not always the case. The country or region of origin, the racial or ethnic group, as well as the educational level and immigration status of the mother and the family’s income had larger main effects (and, in some cases, involved interactions) on child care attendance among DLLs. Future research needs to tease apart ethnicity from country of origin, Latino/Hispanic status, DLL status, and income and actually measure cultural constructs such as family orientation and preference for first language use in child care to understand exactly which groups with which values prefer different types of care. More generally, to fully understand the child care experiences of DLLs, closer examination of the quality of care and the linguistic and cultural features of different types of care is needed. Knowledge about whether the caregiver speaks a DLL child’s first language is not enough. Studies are needed that describe the actual languages used and how they are used by teachers and DLL children in various kinds of child care settings and how these settings and language patterns relate to developmental outcomes for DLLs.
Footnotes
Authors’ Note
This article was completed as part of the secondary data analysis activities of the Center for Early Care and Education Research: Dual Language Learners, funded by the Office of Planning, Research and Evaluation in the Administration for Children and Families, U.S. Department of Health and Human Services.
Authors
LINDA M. ESPINOSA, professor emeritus, University of Missouri–Columbia. Research interests focus on bilingual development during the preschool years and evaluating early care and educational settings that promote long-term achievement of young dual language learners.
DORÉ R. LAFORETT, advanced research scientist, Frank Porter Graham Child Development Institute, University of North Carolina at Chapel Hill. Research focuses on policy and practices that support development of young dual language learners.
MARGARET BURCHINAL, senior researcher, Frank Porter Graham Child Development Institute, University of North Carolina at Chapel Hill. Senior statistician for many national studies of child care and influences on development and school achievement.
ADAM WINSLER, associate chair of graduate studies, Applied Developmental Psychology, George Mason University. Research on development of diverse groups of children, including dual language learners and low-income populations, and influence of early care settings.
HSIAO-CHUAN TIEN, programmer analyst, Carolina Population Center, University of North Carolina at Chapel Hill. Expert social science analyst.
ELLEN S. PEISNER-FEINBERG, senior scientist, Frank Porter Graham Child Development Institute, School of Education, University of North Carolina at Chapel Hill. Research interests include effects of child care on children’s development and school achievement.
DINA C. CASTRO, professor, College of Education, University of North Texas. Research focuses on policies and practices to promote bilingual development and improve quality of early care and education for dual language learners, immigrants, and low-income populations.