
Abstract
Executive Summary
Home and community gardening is emerging as a beneficial intervention for resettled refugee populations. Using an interdisciplinary lens, we examined whether gardening influences mental health, food security, and economic well-being. A mixed methods study (n = 29) was conducted with quantitative surveys to assess indicators of mental health, food security, and economic well-being. Qualitative, semi-structured interviews explored gardener participants’ experience of gardening benefits (n = 10). Participants had on average been in the United States for seven and a half years, with most having lived in refugee camps prior to arrival. Findings showed gardeners reporting fewer symptoms of anxiety, depression, and trauma, and lesser food insecurity than non-gardeners, and similar indicators of economic well-being. Non-parametric regression analysis showed that being a gardener significantly predicted less psychological distress. Qualitative data substantiated these findings with gardeners reporting improved mental health, closer family, social relationships and connections with culture, and more access to fresh and organic food. The multiple, simultaneous benefits of gardening reported here provide strong support for building community-based health promotion programs to assist refugee integration, including long after arrival. The study further highlights the importance of examining these interrelated factors of mental health, food security, and economic well-being simultaneously and reevaluating the established goals of refugee resettlement, particularly in the United States.
We offer the following recommendations:
• Policymakers and refugee resettlement practitioners should integrate culturally appropriate community-based health promotion efforts in refugee programs long after the initial resettlement period.
• Researchers on refugee integration outcomes should include interdisciplinary perspectives that offer comprehensive understanding of processes related to health outcomes.
• Policymakers on refugee resettlement and integration should consider the linkages between mental health, food security, and economic well-being.
Keywords
Introduction
The current global refugee crisis is the largest since the World War II, reflecting an alarming rate of increase in displaced populations. By the end of 2022, 108.4 million people worldwide were forcibly displaced, with 35.3 million identified as international refugees (UNHCR 2023). Refugee resettlement is one of the durable solutions promoted by the UNHCR along with voluntary repatriation and integration into the country of first asylum. Resettlement is the transfer of refugees from an asylum country or a temporary space to a host country that has agreed to admit and ultimately grant them permanent residence with all the associated freedoms (DOS 2022). Resettlement programs vary in focus and size in the top resettlement states in North America and Europe. Several factors impact resettlement outcomes ranging from community attitudes toward refugees (Esses, Hamilton, and Gaucher 2017), to lack of new initiatives (Capps et al. 2015), to adequate health care, childcare, and employment opportunities that reflect refugees’ qualification and credentials (Kerwin and Nicholson 2021).
The United States is one of the signatories of the 1951 Convention Relating to the Status of Refugees, 1 which calls for the protection, integration, and provision of basic human rights of refugees. Support for refugee resettlement has varied in recent years, with sharp swings in admissions and admission ceilings (Kerwin and Nicholson 2021; UNHCR 2023, 39–40). In the United States, even prior to COVID-19, reductions in funding for resettlement and restrictions due to travel bans led to decreased admissions (Kerwin 2018).
As set forth in The Refugee Act of 1980, the primary goals of resettlement in the United States include economic self-sufficiency and integration of refugees with a “work first” approach (Brown and Scribner 2014). Refugee integration goes beyond ensuring that basic safety needs are met and is regarded as a dynamic, multi-dimensional process to help achieve long-term stability and adjustment to a new society (UNHCR 2002). However, some scholars suggest that the goal of self-sufficiency and integration overlooks the fact that most refugee arrivals have experienced severe and complex traumatic experiences with limited resources allocated for mental health and well-being (Kira 2010). Scholars suggest that effective integration must recognize the complex interplay of individual health needs and linkages between institutional and community factors (Reed, Kraly, and Bloemraad 2021, 120; McCann, et al. 2023). Refugees are known to face health disadvantages due to their exposure to harsh environments during displacements and the challenges of resettlement (Reed and Barbosa 2017; Kerwin and Nicholson 2021). They also experience prolonged mental health sequelae that impact their daily lives in the process of resettlement and integration (Fitzgerald and Arar 2018; Kira 2010).
Research suggests that gardening can be effective in helping establish stability for those forcibly displaced from their land (Clatworthy, Hinds, and Camic 2013) as well as increasing overall well-being in other minoritized, under-resourced populations (Dyg, Christensen, and Peterson 2020). Home and community gardening are the practices of growing food in private and in shared community-based spaces for the primary purpose of personal and family consumption. It may alleviate systemic challenges faced by resettled refugees and enhance quality of life (Cummings et al. 2008; Tracey et al. 2020). Specifically, studies conducted with immigrant and refugee populations in regions of North America, United Kingdom, and Australia demonstrate that gardening can be a source of social support that promotes a deep sense of community and a way of reconnecting with positive memories of their home country (Carney et al. 2012; Chase 2012; Gichunge and Kidwaro 2014; Gerber et al. 2017).
Most of the existing evidence, however, is through qualitative studies exploring social well-being and community connectedness through gardening with very limited quantitative or mixed methods studies (Hartwig and Mason 2016; Spano et al. 2020). Additionally, while studies have separately examined mental health and food security (Clatworthy, Hinds, and Camic 2013), few, if any, have simultaneously investigated mental health, food security, and economic well-being. In this mixed methods study, using a unique interdisciplinary perspective, we examined the impact of existing vegetable gardening practices in a sample of resettled refugees in a resettlement city in northeast United States. Our study differs from previous studies as we not only used a mixed methods design but also aimed to investigate differences in three main indicators of well-being — mental health, food security, and economic well-being. This focus is especially significant since resettled refugee populations often have high rates of psychological distress (Miller and Rasmussen 2017) and food insecurity (Nunnery and Dharod 2017), both of which can influence resettlement goals of economic self-sufficiency and integration.
Mental Health and Gardening among Resettled Refugees
The traumatic and combined contexts of forced displacement, flight, and resettlement can have profound and long-lasting consequences on resettled refugees (Jamil et al. 2007; Kira 2010; Kirmayer et al. 2011). Numerous studies on refugees resettled across the United States, Canada, and Australia document higher rates of negative mental health outcomes because of the traumatic contexts of forced displacement (Jamil et al. 2007; Kirmayer et al. 2011). Symptoms of mental health disorders, such as post-traumatic stress disorder (PTSD), anxiety, depression, and substance abuse, are commonly reported for resettled refugees (Jamil et al. 2007; Nickerson et al. 2010). However, multiple factors at the pre-migration and flight stages also determine mental health and well-being (Jamil et al. 2007; Kirmayer et al. 2011; Björn et al. 2013). For instance, reviews of studies consistently note that disruption of social support, harsh living conditions in camps, and post-migration factors in resettlement such as age, loss of social status, unemployment, language barriers, and uncertainties can impact mental health (Kirmayer et al. 2011; Fazel et al. 2012). Additionally, continuing violence in the home country and family separation are barriers to establishing new lives and a sense of belonging in the host country (Lie 2002; Miller and Rasmussen 2017). These experiences of losses and lack of safety can manifest in multiple expressions of mental health distress and persist over long periods, much after the initial “resettlement” period is over (Watters, 2001; Ehntholt et al. 2006; Mirkin and Kamya 2008; George, 2010; Murray et al. 2010; Nickerson et al., 2011; Kira et al. 2012).
Despite this prevalence and increased risk of psychological distress, scholars have long pointed to a wide gap between the need for and adequacy of services (Silove et al. 2017). Additionally, there is inadequate attention to preventive programs that can inhibit the onset of mental health symptoms (Weine 2011; Uphoff et al. 2020). Given the pervasiveness of distress and inherent barriers to accessing services, it is imperative that mental health practitioners re-imagine ways of providing appropriate care. Prevention efforts through community-based and culturally appropriate methods may lessen the necessity of clinic-based interventions when symptoms are more exacerbated (Miller and Rasco 2004).
One way in which multiple displacement stressors of social isolation and access to resources can be simultaneously addressed is through community-based programs, such as gardening (Clatworthy, Hinds, and Camic 2013). Gardening has been shown to successfully promote a stronger sense of community connection among some refugee and immigrant communities (Hadley and Sellen 2006; Hartwig and Mason 2016). This may be especially significant for refugees who struggle with maintaining connections to their traditional ways of being and growing food in a foreign environment. As we unpack associations between access to food and mental health symptoms (Nunnery and Dharod 2017), practitioners may consider investigating the effectiveness of gardening in promoting mental health. This paper examines how gardening as a practice can help refugees reestablish connections to a place-based identity and what this might mean for mental health and economic well-being.
Economic Well-Being and Food Insecurity Among Resettled Refugees
A major element of economic well-being is food security, or the condition of sufficient physical and economic access to safe and nutritious food that meets dietary needs for an active and healthy life (FOA 2006). The rates of food insecurity are far higher in resettled refugee populations, regardless of country of origin, than for non-refugees in the United States (Nunnery and Dharod 2017). Rates of 75 percent–85 percent of surveyed refugees are consistently reported across studies as compared to 14% of the general population (Hadley and Sellen 2006; Nunnery et al. 2015). These high rates may be due to several factors, including poverty (Peterman et al. 2010; Dharod et al. 2013), lack of access to familiar foods (Hadley et al. 2010), and language barriers preventing successful navigation of new environments (Haldeman et al. 2008). Studies in the United States show that food insecurity and hunger persist over time, in many cases years into the resettlement process (Hadley and Sellen 2006; Nunnery et al. 2015).
Achieving food security through market transactions is often cost-prohibitive for resettled refugees, particularly due to them lacking access to culturally appropriate food in affordable grocery stores as well as in emergency food outlets (Dickinson 2013). Food stamps, for example, provide limited access to culturally appropriate food, as they are oftentimes ineligible for use at grocery stores with more internationally sourced food offerings (Dickinson 2013). Focusing on emergency food approaches to address refugee food insecurity has also been shown to create patterns of dependency, as compared to a more community-based food security approach (Gallegos et al. 2008). Additionally, a recent study indicated that pre-migration factors such as lack of literacy, and post-migration issues unique to transnational families, such as sending remittances to families back home, may contribute to ongoing food insecurity among refugees (Nunnery and Dharod 2017). Food insecurity is linked to multiple chronic health diseases and an increased risk of poor overall health as well. There are also differences in vulnerability to health-related consequences of food insecurity, with women often experiencing the burden of these factors most heavily (Olson 2010). While separate bodies of literature highlight the mental health trauma of refugee experiences prior to and during resettlement, studies on food insecurity have rarely studied these intersections concurrently (Nunnery and Dharod 2017).
Existing studies indicate profound and positive impacts of gardening on populations that have experienced significant trauma and forced displacement (Clatworthy, Hinds, and Camic 2013). However, these studies are limited in some critical ways. First, as we mentioned earlier, most studies have separately examined indicators of economic well-being, mental health, and food insecurity. We propose that these are interrelated and, therefore, must be examined simultaneously through an interdisciplinary lens. In this study, we combined perspectives from disciplines of economics, mental health, and food studies, to develop our research questions. The second limitation is that existing studies have typically either used quantitative indicators or qualitative descriptions of experiences. Our use of mixed methods approach allows us to understand quantitative differences in indicators supplemented by qualitative reports.
In this study, we ask — Does home and community gardening promote mental health, food security, and economic well-being in resettled refugees? We sought to answer this through two sub-questions reflecting a mixed methods design. The first sub-question where we used quantitative indicators was: Is there a difference in indicators between participants who are involved in home and community gardening and those who are not? The second sub question using open-ended questions asked only those who were gardeners: What is the experience and reported benefits of community gardening in resettled refugees?
Methods
A cross-sectional, descriptive, concurrent mixed methods approach was used where both quantitative and qualitative questions were asked at the same point of data collection (Johnson and Onwuegbuzie 2004). While the quantitative portion of the study aimed to understand differences between gardeners and non-gardeners on indicators of mental health, food security, and economic well-being, the qualitative questions sought to understand the benefits of gardening. Therefore, only participants who were engaged in gardening answered the qualitative questions. The eligibility criteria for participation included: a. Entry into the United States as a refugee; b. Age above 18 years; and c. Currently residing in the Central New York region area where the researchers were situated. We gathered data from 29 gardeners and non-gardeners over a period of five months in 2019. Participants were given a $25 cash incentive to participate in the study.
Data Collection
The study implementation included extensive efforts to engage with the community of refugees, non-profit organizations, and leaders of the refugee community who helped us gain access to potential participants. The research team, including the authors of this study and two Research Assistants (RA), did not have lived experiences as resettled refugees themselves and were also not proficient in the languages spoken by the participants. The authors had expertise in their respective fields of study — mental health, food studies, and economics — and had several years of experience providing clinical services and community-based health promotion programs to racially minoritized and immigrant populations in the area where the study occurred. Authors’ pre-existing relationships with the resettled refugee community members, in-person meetings with agencies serving refugee communities, and field visits to farms, farmers’ markets, and local agencies allowed for building trust prior to data collection by the research team.
Upon approval from the Institutional Review Board (IRB), surveys and consent forms developed by researchers were translated by a local agency also led by a community leader with a refugee background. Recruitment occurred through word of mouth, snowball, and convenience sampling. Requests for recruitment were made in-person through visits to the agencies and places where resettled refugees congregated (non-profits serving refugees, farmers’ market, and gardening classes). Only four gardener participants were recruited from a local program on agricultural training for resettled refugees. The training program was free and intended to assist those who wanted to grow their produce either for self-consumption or for income generation. These participants had access to a plot of land provided by the program and participated in workshops, planting, and harvesting together. All other gardener and non-gardener participants were recruited from three different refugee-led agencies serving various needs of resettled refugees including health care, education, and community support.
Regular research team meetings with the principal investigators (PIs) and RAs were conducted to brainstorm and solve emergent challenges and understand the nature of data being collected as soon as they were collected. Data collection extended between August 2019 to November 2019, which is the growing season in the region where the study occurred. We intentionally surveyed both gardener and non-gardener participants during this season, to better distinguish whether access to gardening could help understand any differences in mental health and food security outcomes. The initial plan was to collect data over a period of two years (two growing seasons). We collected data from 29 participants in the first year, with a goal to complete data collection from a total of 50 gardeners and non-gardeners in the second year. However, the COVID-19 pandemic and related restrictions in the following year made it impossible to return to field visits and in-person, interpreter-assisted data collection. The COVID-19 pandemic also changed the context of data collection with significant impacts on mental health (Kiteki et al. 2022), food security (O’Hara and Toussaint 2021), and economic stability specifically in minoritized groups (Kantamneni 2020) as noted in literature.
Measures
The study included the following surveys to collect quantitative data from all participants. Mental health was assessed using the Refugee Health Screener (RHS-15; Hollifield et al. 2013) to identify symptoms of anxiety, depression, and post-traumatic stress disorder. The RHS is a culturally validated tool typically used to screen mental health symptoms in resettled refugees. The survey prompts respondents to respond to the degree to which 14 indicators of distress have been “bothersome” in the last month. Indicators include body pains, sadness, thoughts, helplessness, scaredness, faintness, nervousness, restlessness, incidents of crying, reliving the trauma, physical reactions, emotional numbness, incidents of being startled, and challenges with coping. The final item has a “distress thermometer” where participants describe the amount of distress in the last week on a scale of 0 (no distress) to 10 (extreme distress). A total score greater than or equal to 12 or the distress thermometer rating greater than or equal to five indicates a positive screening for distress. In this current study the Cronbach alpha was 0.850 showing high internal reliability.
Household food security, defined as access by all members at all times to enough food for an active, healthy life, was assessed using USDA’s (2012) Adult Food Security Survey Module. The survey measured food security on a continuum from high to very low based on food longevity, food affordability, skipping meals, eating less, hunger and weight loss. The survey prompts respondents to think about the last 12 months while answering questions on above indicators on a Likert scale ranging from “often true” to “never true” for them or their household. The economic well-being of the sample was assessed primarily through questions on household income levels, reliance on public benefits (such as Supplemental, Nutritional Assistance Program (SNAP), education levels, and current employment.
Additionally, participants who identified as currently gardening were asked about their experiences of gardening through a semi-structured interview schedule. The interview schedule included questions on where they gardened, what they grew, with whom they gardened, and a question on the benefits of gardening. For gardener participants, the total time for completing surveys and the interview portion was between 45 and 90 minutes. For non-gardener participants, completing the surveys required about 30–45 minutes. Given the language barrier, professional interpreters assisted in administering the surveys and the total duration of data collection depended on ease of interviewer-interpreter-interviewee communication.
Interviews were audio recorded, transcribed in participants’ languages, translated into English, and verified for accuracy by the interviewers. Translated interviews were analyzed using content analysis, which is a qualitative data analytic strategy in which texts (in this case, responses to interview questions in this study) are grouped together based on themes (Elo and Kyngas 2008). Two members of the research team conducted a content analysis of the responses to interview questions on benefits of gardening. Responses were then organized around themes that emerged across all interviews. Two other research team members, who also interviewed participants, reviewed the organization of themes until data saturation, where no other new themes were identified in the available data. Analytic strategy conducted for this study is in line with mixed methods studies where findings from qualitative questions are transformed to facilitate better mixing or connection with quantitative data (Onwuegbuzie and Teddlie 2003). An in-depth analysis of all qualitative data from this study has been published elsewhere (Minkoff-Zern et al., 2023).
Results
Descriptive Results
Twenty-nine participants were interviewed, out of which 19 participants were gardeners and 10 participants were non-gardeners. Of the 19 gardener participants, 4 of them were in an agricultural training program and were involved in growing and harvesting produce together. The rest gardened in their home gardens either in their backyard or in shared yards. A total of 12 gardeners reported gardening with family, friends, or neighbors across these settings. The average age of participants was 49.10 years, ranging from 20 to 80 years with average years in resettlement of 7.5 years, ranging from 3 to 15 years for non-gardeners and 2–14 years for gardeners. The majority of the participants were from Bhutan (69%), 10.3% were from Somalia and the rest from Syria, Burundi, Congo, Cuba, and Nepal. All participants listed conflicts in homeland and threats of persecution as reasons for their resettlement. Though gender expansive categories were provided, all participants identified as female (48%) and male (52%). Most of them (75.9%) were married and 72.4% reported having children. A little more than half of the sample (55%) responded as having some educational course certification with only 3% having an associate degree. Only 21% of the participants indicated they were fully employed and 79% unemployed. Table 1 shows demographic details listed separately for gardeners and non-gardeners. Notably, a greater number of gardeners (63.2%) reported having no prior experience with gardening or farming in their home country.
Demographic Details of Gardener and Non-Gardener Participants.
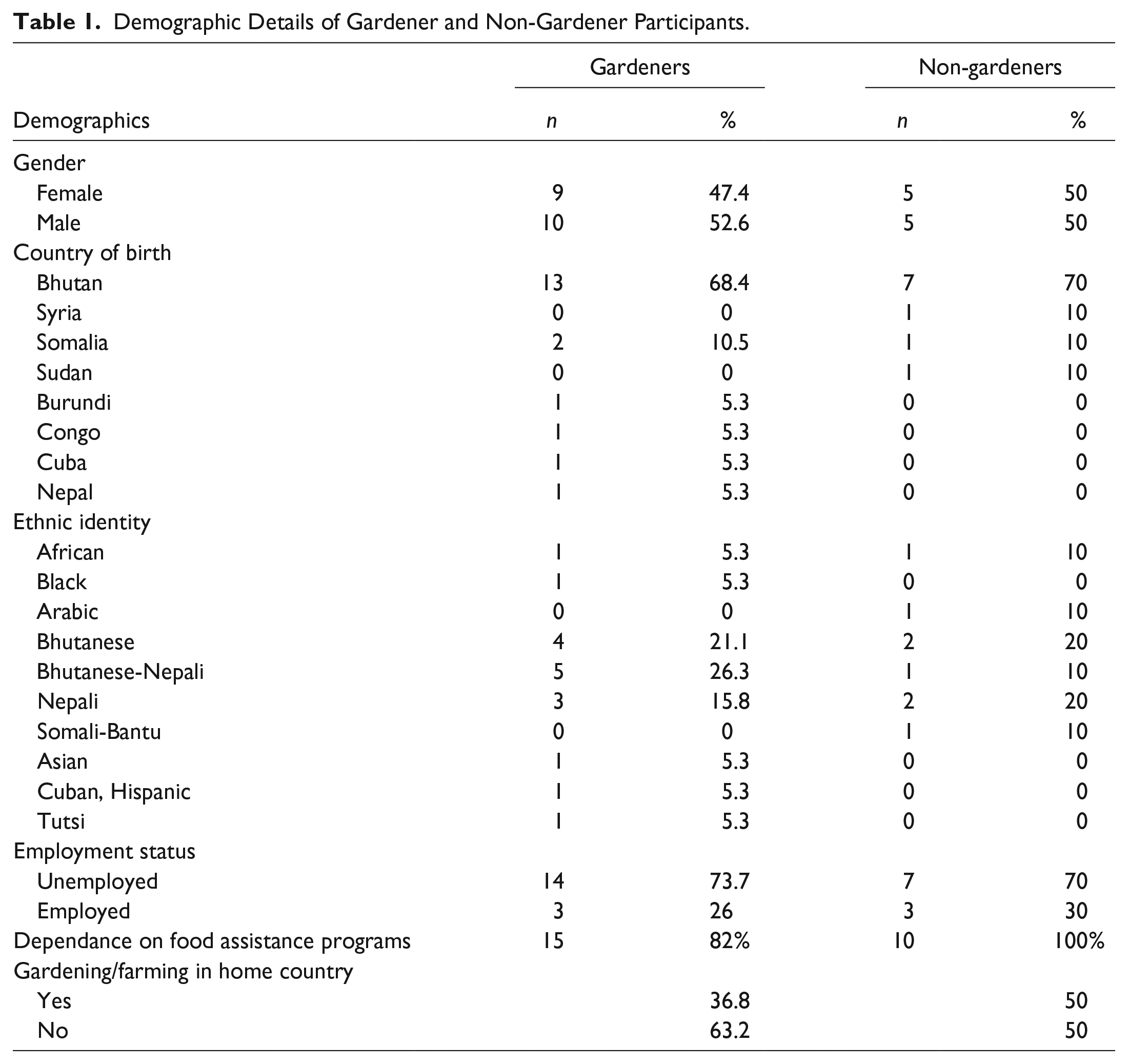
The findings also showed that the range of income was similar between gardener and non-gardener groups. The gardener group reported a household income in the range of $920–$1,020 per month in the last two months and non-gardeners a range of $980–1080. There were more stark difference between the two groups, however, in reported factors related to food insecurity. Specifically, more non-gardeners reported food shortage (89%), dependence on food assistance programs (100%), skipping meals (38%), and going hungry (25%) in the previous 12 months. Finally, clear differences in descriptive statistics emerged in mental health symptoms between the two groups. Figure 1 shows differences in mental health symptoms across all items of the RHS-15 questionnaire between gardeners and non-gardeners. As indicated, across all items, more non-gardeners reported symptoms of anxiety and depression including body pains (44%), sadness (33%), too many thoughts (56%), and faintness and restlessness (44%). Additionally, more non-gardeners reported symptoms of reliving trauma (33%) and emotional numbness (33%).
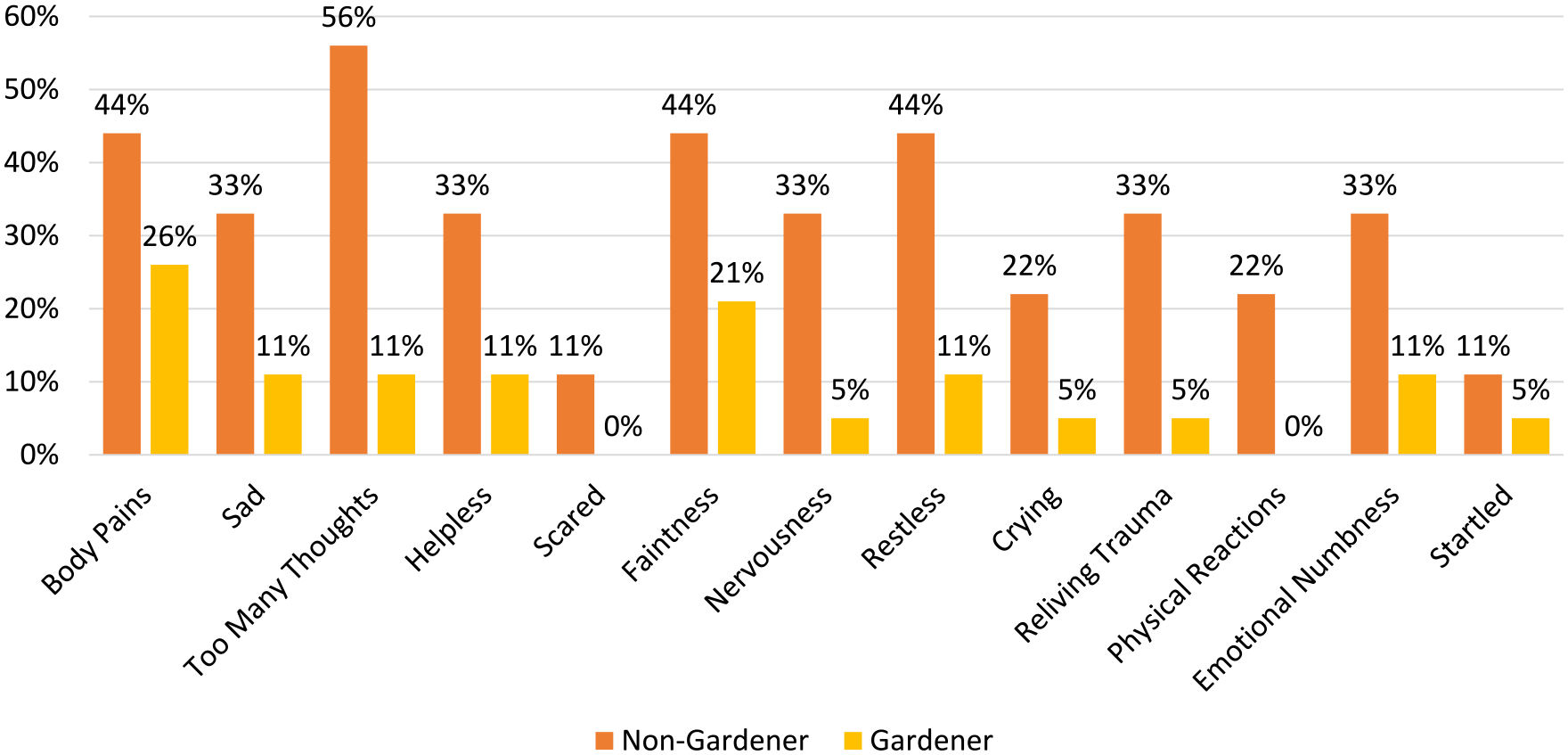
Differences in Symptoms of Mental Health Between Gardeners and Non-Gardeners.
Regression Analysis
Given the small sample size, a non-parametric, bootstrap, 2 and kernel 3 method of estimation in Stata was used to assess significant differences in indicators (StataCorp 2021). Unlike linear regression, which assumes a linear relationship between the outcome and the covariates, nonparametric regression makes no assumptions about the functional form of the relationship. This characteristic makes it more flexible and applicable to a wider range of data types, including continuous, count, and binary outcomes.
The regression model included scores on the RHS, food insecurity, and employment status as dependent variables with identification as a gardener being the independent variable. Table 2 shows the observed and bootstrapped estimates for the three dependent variables in the regression model. The model indicates a significant effect of gardener status on RHS score. That is, being a gardener significantly predicted lesser mental health distress as reported in the RHS. The bootstrap method was used to estimate standard errors and construct confidence intervals with 50 replications. The percentile method was used to construct 90% confidence intervals. Taken together, the descriptive results and regression analysis show that there was a statistically significant difference in RHS scores with gardeners reporting far fewer symptoms of anxiety, depression, and PTSD compared to non-gardeners.
Non-Parametric Regression Analysis Showing the Effect of Gardening Status on Study Variables.
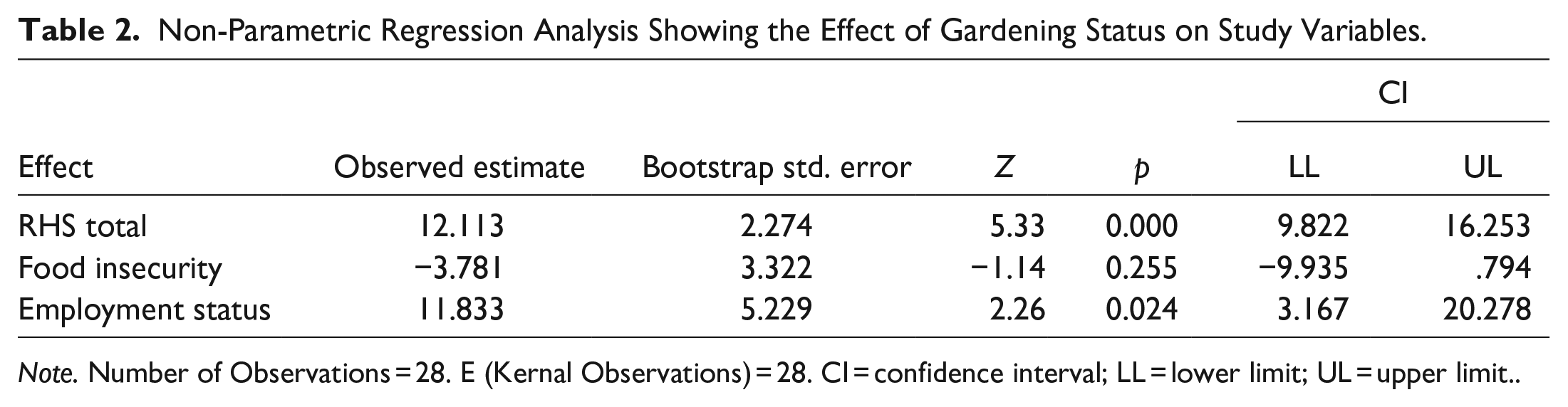
Note. Number of Observations = 28. E (Kernal Observations) = 28. CI = confidence interval; LL = lower limit; UL = upper limit..
Benefits of Gardening
Participants who identified as current gardeners were further interviewed on what they saw as the benefits of gardening. As described earlier, using a content analysis strategy, the number of participants reporting similar themes was counted and similar domains of benefits of gardening were organized. Overall, they reported on mental health benefits, closer relationships with family and the gardening community, physical labor, connecting with culture and identities, access to fresh and organic food, and decreasing financial burdens. A full analysis of the qualitative data is provided elsewhere (Author citation).
The mental health benefits of gardening were noted by a majority of participants who gardened (63%, n = 12). Many reported that gardening helped in staying busy and productive, and prevented negative thoughts. A 33-year-old female gardener from Nepal noted, “It does help with everything. . .. when I am busy all the time I don’t have any, you know, free time to think about some other negative things.” A 66-year-old female gardener who identified as Bhutanese — Nepali reported, “It’s easier to forget things mentally like when I am doing the gardening and everything. . . I forget my problems.” Yet another participant, a 66-year-old male gardener from Burundi, noted that staying productive through gardening gave him a sense of importance that he was contributing to the well-being of the family, “I’m not sitting at home doing nothing. . . it’s giving that sense that I’m productive. . . Yeah, so it’s something that is really kind of very important mentally for me. . .Yes. I can, I can produce something and. . .can contribute to the well-being of the family.”
Many participants (63%, n = 12) also noted strengthening of connections with family and the community members with whom they gardened. Participants observed a feeling of togetherness as they worked and enjoyed the benefits of their labor. For instance, a 62-year-old Bhutanese female gardener observed, “We’ll all go together and then whatever we get from the garden we’ll all eat it together and that’s why it’s better. . .We get to see each other, and other friends come there too, and it’s a good environment there.” For some (34%, n = 7), the ability to grow their own food, particularly vegetables that were specific to their cuisine, helped in connecting with their identities, home country, and culture. As noted by a 61-year-old, Bhutanese-Nepali male gardener, “It makes me really happy because I know this (gardening) for a long time and I’ve been doing this for a long time, so when I see it’s growing, it just makes me so happy, and it reminds me of home.”
Forty-two percent (n = 8) of the gardeners discussed the benefits of physical labor and its connection to their general wellbeing. The physical labor of gardening not only helped distract from negative thoughts but provided the added benefit of improving physical health. The interrelated factors improved participants’ overall mental health and well-being. These findings offer some insight into the substantial differences in symptoms of anxiety, depression, and trauma that was indicated in the quantitative findings between gardeners and non-gardeners. Further, participants reported access to fresh, organically grown vegetables, which they identified as being healthier than other options in stores. Most of the gardeners worked in their home gardens or in small community plots and used their produce for their own consumption. One of them, a 64-year-old Bhutanese-Nepali female gardener said, “I’m happy- the fact that I get to eat the fruits and vegetables, the fresh fruits and vegetables that I grow- and I also like I don’t have to eat the frozen food.. So it makes me happy.” While participants noted this also helped in improving their well-being overall, qualitative data substantiated the food security survey as well. As noted above in the quantitative surveys, fewer gardeners than non-gardeners reported food shortage and food insecurity, pointing to the ways that their produce supplemented other sources of food for consumption. A few (21%, n = 4) reported a tangible economic benefit of saving money by growing their own vegetables. As noted by a 61-year-old Bhutanese female gardener, “It does help with finances because I saved some money instead of going to the grocery stores. I can go to the farm and grab some vegetables from there and with the money I saved I can utilize that money for some other purposes - to buy rice or other products.” Thus, while not directly influencing economic self-sufficiency (because it was not always a way to earn income), some participants were able to save money by growing their own food, specifically during the growing and harvesting season when this data was collected.
Discussion
Using a mixed methods study and an interdisciplinary lens, we sought to investigate whether gardening would simultaneously influence mental health, food security, and economic self-sufficiency in a sample of resettled refugee adults. Quantitative survey results from all 29 participants demonstrated that gardeners compared to non-gardeners reported significantly fewer symptoms of mental health distress and lesser food insecurity. Qualitative data from a subsample of 19 participants who gardened provided more information on direct benefits of gardening to mental health and well-being and other benefits related to social and community relationships, physical labor, access to fresh food, and connecting with culture and identities. Most demographic characteristics were similar between the two groups, except that gardeners were older, and fewer of them had prior experience of gardening or farming before resettlement. Income levels, type of profession, and employment status, however, were similar between gardeners and non-gardeners. Taken together, these findings suggest the potential for home and community gardening, specifically vegetable gardening, to simultaneously address the multifaceted needs of resettled refugees.
While statistically, we did not find differences in indicators of economic well-being (such as education levels, employment status, and income levels), participants did report easing of financial stress in their interviews. This reduction of financial stress reportedly improved family relationships and was a way in which adults could provide for their children. In light of the COVID-19 pandemic, scholars have reported on the significance of home and community gardening opportunities to offset food insecurity due to supply chain disruptions (Lal 2020, 871). For our participants, it was not just about access to food but also the opportunity to grow and prepare culturally appropriate food, which may have resulted in intangible benefits not evident in their economic indicators. Participants in our study also noted that while growing food did not supplement their income sources directly, they were able to connect with their cultural identities, form a sense of belonging with other community members, and productively contribute to the well-being of their families. While there are certainly other obstacles to gardening as a comprehensive strategy for addressing refugee food insecurity, including seasonality, product limitations, lack of sustainable infrastructure to support continual access to land and resources (Abramovic 2019), we argue that through gardening refugees can address a multitude of livelihood challenges, including and beyond food insecurity. In the resettled refugee community, investing in these types of promotion programs can positively impact well-being and place in society (Miller and Rasco 2004; Gichunge and Kidwaro 2014; Jean 2015; Hughes 2019).
One of the findings of our study that warrants further investigation was the higher number of non-gardener participants who had previously gardened in their home country prior to resettlement. We did not directly ask these participants why they were not currently gardening. However, based on field notes in the recruitment and data collection process, we gathered that this may have been due for some to not having access to information about available resources in the community or not having access to seeds for produce that is part of their diet. There may be other limiting factors as well, such as age, time, space, and ability status of participants.
While our study has several important contributions including an interdisciplinary, mental health promotion focus, community engagement in study implementation, and mixed methods design, the restrictions emerging from the COVID-19 pandemic limited our ability to collect data from a larger sample. The short window for data collection and the disruption resulted in a smaller sample with an unequal number of gardeners and non-gardeners. This limits our ability to draw robust conclusions about reasons for differences in the mental health and food security surveys. Additionally, while we followed guidelines for interpreter-assisted interviews and the data collection was strengthened through community engagement, language barriers may have inhibited more in-depth responses (Wallin and Ahlström 2006). Also, we examined the impact of gardening practices that were already in place in the community where we could not control for variability such as the type of gardening (home versus community), with whom participants gardened (family or non-family members), or their reasons for gardening (personal consumption or income-generation). Further experimental studies that can control for these factors are needed to unpack associations. Experimental studies may be able to carefully track other indicators such as the amount of food produced and its associated financial benefits, time spent in gardening (and with whom), and the setting of gardening (communal versus private). Additionally, given that other factors such as age at which resettlement occurs and the length of resettlement in the host country are known to influence health and well-being (Hocking and Sundram 2022), future studies with a larger sample may be able to examine the relative influence of gardening in older versus younger cohorts of resettled adults. As some scholars argue (for instance, Edelman et al. 2014) the framework of food sovereignty, which includes access and rights to means of nutritious food, may also be beneficial in the study of culturally appropriate and responsive pathways to food prod-uction and consumption in displaced populations (Minkoff-Zern et al., 2023).
Policy Recommendations
The study’s findings have important implications for mental health practitioners and policy stakeholders involved in refugee resettlement. They argue for the incorporation of programs and interventions that simultaneously address multi-systemic stressors. Our study lends support for a “whole of person” approach in understanding the interactions between economic sufficiency, food security, and physical and mental health and well-being (McCann et al. 2023, 155). Scholars have noted that the singular focus of the work-first approach in resettlement programs and policies is problematic and instead, programs that provide comprehensive support to address integration-related challenges enjoy better long-term outcomes, including financial stability (Brown and Scribner 2014). Our findings, along with others that have demonstrated the impact of community-based programs, provide further evidence for a better integration of these programs in refugee resettlement. With resettlement programs in the United States still rebuilding after years of drastic cuts and impact of the COVID-19 pandemic, we argue that this is prime time for a re-thinking of supportive services to include community-based promotion programs.
It is worth noting that our study participants were well beyond the initial resettlement phase when they may have had access to empowerment programs. Reports of challenges in mental health distress, food insecurity, and levels of under and unemployment even after years in resettlement highlight the need for long term, durable practices in refugee integration. Additionally, culturally responsive practices that emphasize existing resources and strengths could further protect against multiple stressors inherent in this process. These programs and initiatives must be supported by resettlement and integration policies that leverage existing community resources, provide additional funding for long-term support in refugee integration, and recast resettlement goals to include overall well-being.
Considering our findings, we suggest the following recommendations for comprehensive services and policies in refugee resettlement:
Refugee resettlement programs must support community based mental health promotion efforts for an extended duration, not just in the initial few months. These efforts must include stakeholders in the community such as leaders of locally run service-oriented programs, practitioners who specialize in culturally responsive mental health interventions, experts with knowledge of local food systems. Such programs should operate alongside employment and education assistance programs.
Interdisciplinary, community-oriented action research must be encouraged through local, state, and federal funding for comprehensive understanding of interrelated factors such as mental health, food security, and economic well-being, and their impact of resettlement outcomes.
Resettlement policies must support comprehensive health promotion programs that include capacity building of practitioners and service providers in refugee resettlement work. These capacity building initiatives must include relevant culturally responsive curriculum in training programs in the fields of mental health, food studies, and economics.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by The Fahs-Beck Fund for Research and Experimentation and The Lerner Center for Public Health Promotion, Syracuse University, New York.
1
2
Bootstrapping is a statistical technique used to estimate the uncertainty associated with a statistic of interest (e.g., mean, median, and correlation) using only the available sample data. Bootstrapping is particularly useful in situations where it is difficult to obtain large sample sizes, where the underlying distribution of the data is unknown or non-normal, or where traditional statistical assumptions (such as independence or normality) may not be satisfied (![]() ). It allows researchers to make inferences about a population based on a sample, without making strong assumptions about the distribution of the population or the data-generating process.
). It allows researchers to make inferences about a population based on a sample, without making strong assumptions about the distribution of the population or the data-generating process.
3
By using a kernel function in STATA, “npregress” kernel estimates the mean of the outcome variable based on the nearby observations, with the weights given by the kernel function. The “npregress” kernel is a useful tool for modeling the relationship between covariates and outcomes when the relationship is unknown or nonlinear which is most often the case is small data sets (![]() ).
).