
Abstract
The trend of cochlear implantation at a younger age has become increasingly prominent in recent years. However, early intervention also presents significant challenges to postoperative assessment. Parent-reported questionnaires have demonstrated notable advantages in outcome evaluation for infants and young children. In the present study, we investigate the auditory development of Mandarin-speaking children with cochlear implants (CIs) using the Chinese version of the Parents’ Evaluation of Aural/Oral Performance of Children (PEACH). A total of 187 children with CIs participated. According to their age at implantation, the children were classified into five groups: <12 months, 13–18 months, 19–24 months, 25–42 months, and >42 months. Evaluations were administered at CIs switch-on (baseline), and at 1, 2, 3, 6, 12, 24, 36, 48, 60 months post switch-on, resulting in 933 records. We employed a linear mixed-effects model to identify key factors influencing PEACH performance. Results show that the PEACH scores enter a stable plateau phase after approximately 20 months of CI use. Notably, children who received CIs at a younger age exhibited faster improvements in auditory functional performances. This advantage is particularly prominent in children implanted before 18 months of age. Analysis indicated that significant influencing factors include age at implantation, duration of CI use, development quotient, and preoperative residual hearing level. This study explores the longitudinal trends of early aural/oral performance in children with CIs. The findings emphasize the critical importance of early cochlear implantation for improving outcomes while revealing the challenges associated with the late-implanted children.
Introduction
The effectiveness of early intervention for congenital hearing loss has been widely confirmed. Numerous studies demonstrate that infants with severe-to-profound sensorineural hearing loss who receive cochlear implants (CIs) at an early age exhibit superior auditory, speech, and language outcomes compared to those implanted later (e.g., Ching et al., 2013; Dettman et al., 2021; Mitchell et al., 2020). This evidence highlights the benefits of early auditory stimulation to the brain and underscores the critical period for auditory neuroplasticity. In recent years, the trend of cochlear implantation at a younger age has become increasingly prominent, with US Food and Drug Administration (FDA) approval for implantation as early as 9–12 months of age in some regions (Warner-Czyz et al., 2022).
While early intervention offers significant advantages, it also presents considerable challenges for postoperative assessment. Variability in auditory outcomes, limited access to standardized monitoring tools, and the necessity for long-term evaluation underscore the importance of practical yet robust methods for tracking progress in young children. For these reasons, parent-reported questionnaires are widely adopted as effective tools for outcome evaluation (Bagatto et al., 2011; Ching & Hill, 2007). These questionnaires offer significant advantages: parents spend extensive time with their children in diverse auditory environments, uniquely positioning them to observe and evaluate auditory abilities over time, thus capturing real-world performance and providing authentic data that can be difficult to replicate in controlled clinical settings. They also allow for easy comparison of CI users’ performance to that of their normal hearing (NH) peers, facilitating the evaluation of auditory intervention effectiveness while accounting for age-related development. This evaluation method is low-cost, ideal for high-frequency data collection during long-term postoperative follow-ups, and enables consistent tracking of rehabilitation progress and identification of critical timepoints for intervention outcomes. Furthermore, the ease of use and adaptability of their multilingual versions make these questionnaires accessible across diverse populations (Ben-Itzhak & Adi-Bensaid, 2023; Bravo-Torres et al., 2020; Elawady et al., 2019; Goh et al., 2018).
Given these advantages, parent-report questionnaires such as the LittlEARS® Auditory Questionnaire (LEAQ), the Infant⁃Toddler Meaningful Auditory Integration Scale (IT⁃MAIS), and the Parents’ Evaluation of Aural/Oral Performance of Children (PEACH) are widely used for evaluating the outcomes of cochlear implantation in infants and young children (Ching & Hill, 2007; Coninx et al., 2009; Wang et al., 2013; Zhang et al., 2022; Zheng et al., 2009; Zimmerman-Phillips et al., 2000). They are particularly useful when assessing young children with limited linguistic abilities, where traditional methods like speech perception tests may not be feasible. While LEAQ and IT-MAIS have established Chinese norms and reference values for children with CIs (Liu et al., 2015, 2022; Yin et al., 2022), comprehensive PEACH performance in Mandarin-speaking children with CIs has not yet been extensively explored, even after the Chinese version of the PEACH rating scale (version 4.1) was validated in NH children (Zhang et al., 2022).
Distinct from other tools like IT-MAIS and LEAQ, which were designed for children younger than two years of age, the PEACH questionnaire is designed for evaluating functional performance and monitoring auditory development in children from infancy through school age (Ching & Hill, 2007; Ching, Dillon, et al., 2018). Although its original version is available in both diary and rating scale formats (Ching & Hill, 2007), the rating scale version has been more widely adopted by clinicians and caregivers over the diary format because it effectively reduces respondent burden and administration time (Bagatto et al., 2011). Previous studies further indicate that normative data collected with the PEACH rating scale (Bagatto & Scollie, 2013) exhibit a very similar pattern to that obtained using the PEACH diary version (Ching & Hill, 2007), strongly supporting its widespread clinical use. The Chinese version of the PEACH scale (v4.1), adapted from the English scale, has also been established, further supporting its applicability to the population of Mandarin-speaking children with CIs.
The PEACH scale relies on parental observations to evaluate auditory performance across various listening situations, including quiet and noisy environments, interactive communication, and distant speech, thereby providing a comprehensive picture of children's everyday auditory capabilities (Ching & Hill, 2007). Its Quiet and Noise subscales, in addition to a total score, offer specific insights into auditory performance in real-world environments, invaluable for planning appropriate interventions. The PEACH scale's versatility and reliability have been consistently demonstrated (e.g., Bagatto et al., 2011; Goh et al., 2018; Zhang et al., 2022). It has been validated as a sensitive tool for evaluating the effectiveness of amplification or comparing performance under different amplification conditions (e.g., Bagatto & Scollie, 2013; Ben-Itzhak & Adi-Bensaid, 2023; Ching et al., 2010, 2016; Kumar et al., 2013; Zhang et al., 2014), with significant correlations established between PEACH scores and objective auditory measures such as Cortical Auditory Evoked Potentials (Ching et al., 2023; Golding et al., 2007). Moreover, PEACH has proven to be a significant evaluation tool in predicting later outcomes in speech perception (Ching, Zhang, et al., 2018), language, and psychosocial development (Wong et al., 2018). Its applicability is further enhanced by the availability of multiple language versions and their ease of use and adaptability (https://www.outcomes.nal.gov.au/peach). For the Chinese population, the PEACH scale (v4.1) has published normative data with confidence intervals directly applicable in clinical practice. Furthermore, this Chinese version has been validated to effectively reflect the language ability of Mandarin-speaking children, providing additional benefit for assessing children's aural/oral communication ability in real-life settings.
While the Chinese version of the PEACH scale has been validated (Zhang et al., 2022), a significant research gap exists in establishing comprehensive reference values for Mandarin-speaking children with hearing loss, including both CI users and those with hearing aids. Considering the unique strengths of the PEACH tool and this identified research gap, our study specifically aims to address this crucial need by exploring PEACH performance in a large sample of Mandarin-speaking children with CIs. This will complement existing tools for early auditory development, such as the LEAQ and IT-MAIS questionnaires.
The purposes of the present study were to: 1) investigate the developmental trajectories of PEACH performance in Mandarin-speaking children with CIs; 2) compare the auditory performance of children who received CIs with normative references established for Mandarin-speaking children; and 3) explore key factors influencing the PEACH outcomes for Mandarin-speaking children with CIs.
Methods and Materials
Participants
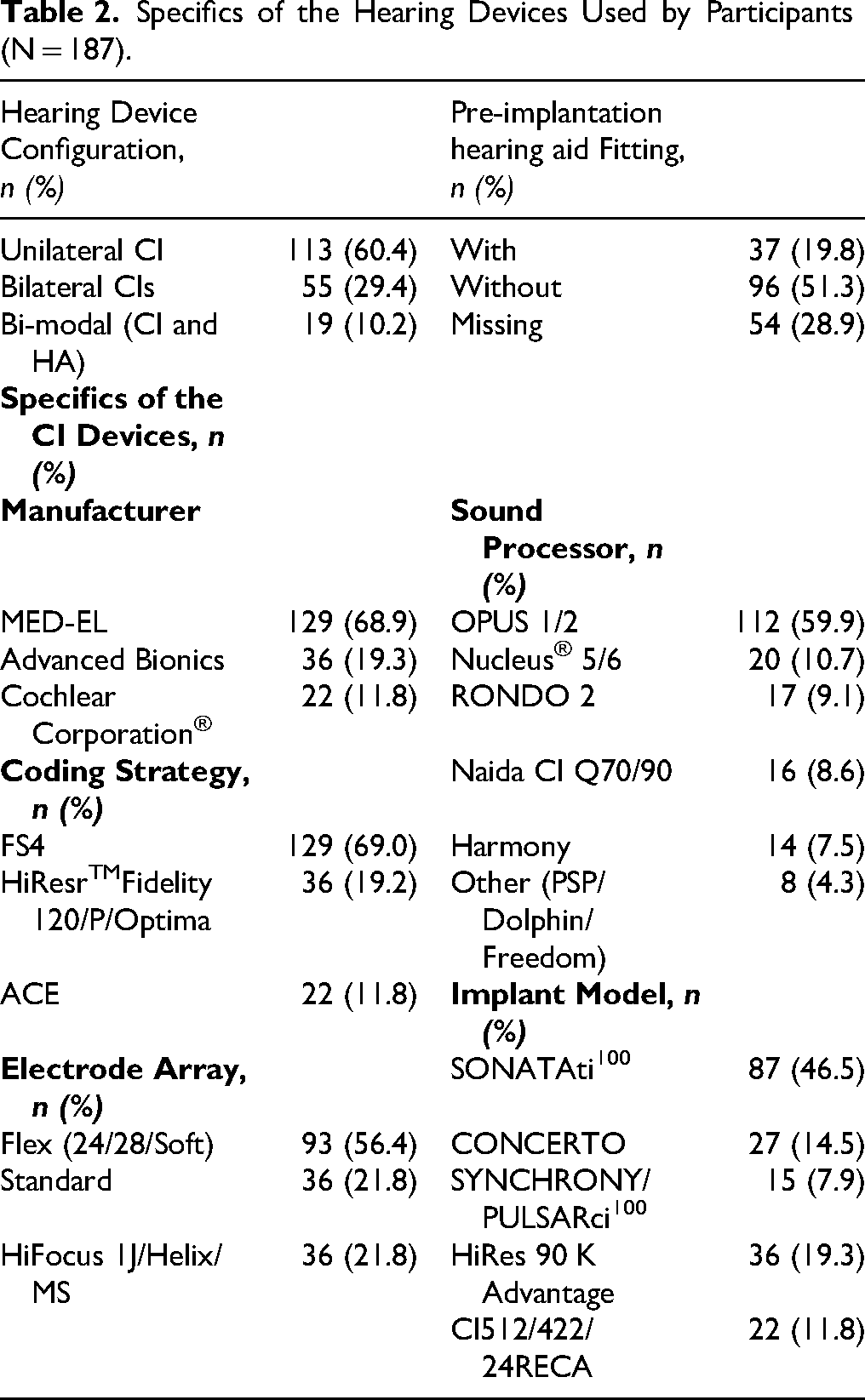
The participants were recruited from the Pediatric Audiology Center of Beijing Children's Hospital, Capital Medical University, between January 2013 and September 2024. A total of 933 assessment records from 187 children with CIs were included in the study. All participants met the eligibility criteria according to the cochlear implantation guidelines in China. Children with severe inner ear malformations (excluding enlarged vestibular aqueduct, EVA), auditory neuropathy, cochlear nerve deficiency, autism, and cerebral palsy were excluded from this study, as existing research has confirmed that these conditions can affect auditory development after implantation (Chao et al., 2023; Hu et al., 2022; Zhao et al., 2019). Children with EVA were, however, included, as their cochlear implantation outcomes have been shown to be comparable to those of children with normal inner ear anatomy (Benchetrit et al., 2022; Chen et al., 2011). Informed consent was obtained from the parents before their involvement in the study, and ethical approval was granted by the Institutional Review Board of Beijing Children's Hospital, Capital Medical University. Detailed demographic and clinical characteristics of the study participants, such as the distribution across age at implantation, audiological characteristics and etiology, device configurations, and pre-implantation hearing aid experience, are summarized in Tables 1 and 2.
Demographic Characteristics of the Participants (N = 187).

*ABR: Auditory Brainstem Response; ASSR: Auditory Steady-State Response. Inner Ear Anatomy: “Normal” indicates children with normal inner ear anatomy structures. Enlarged Vestibular Aqueduct is defined as midpoint diameter of the vestibular aqueduct ≥ 1.5 mm (Saeed et al., 2021; Valvassori & Clemis, 1978).
Specifics of the Hearing Devices Used by Participants (N = 187).
Fixed-Effects Estimates of the Linear Mixed-Effects Model for the PEACH Quiet Subscale.

*DQ: Developmental Quotient
#Refs.: reference category. Group >42 months was used as the reference group in the analysis.
Fixed-Effects Estimates of the Linear Mixed-Effects Model for the PEACH Noise Subscale.
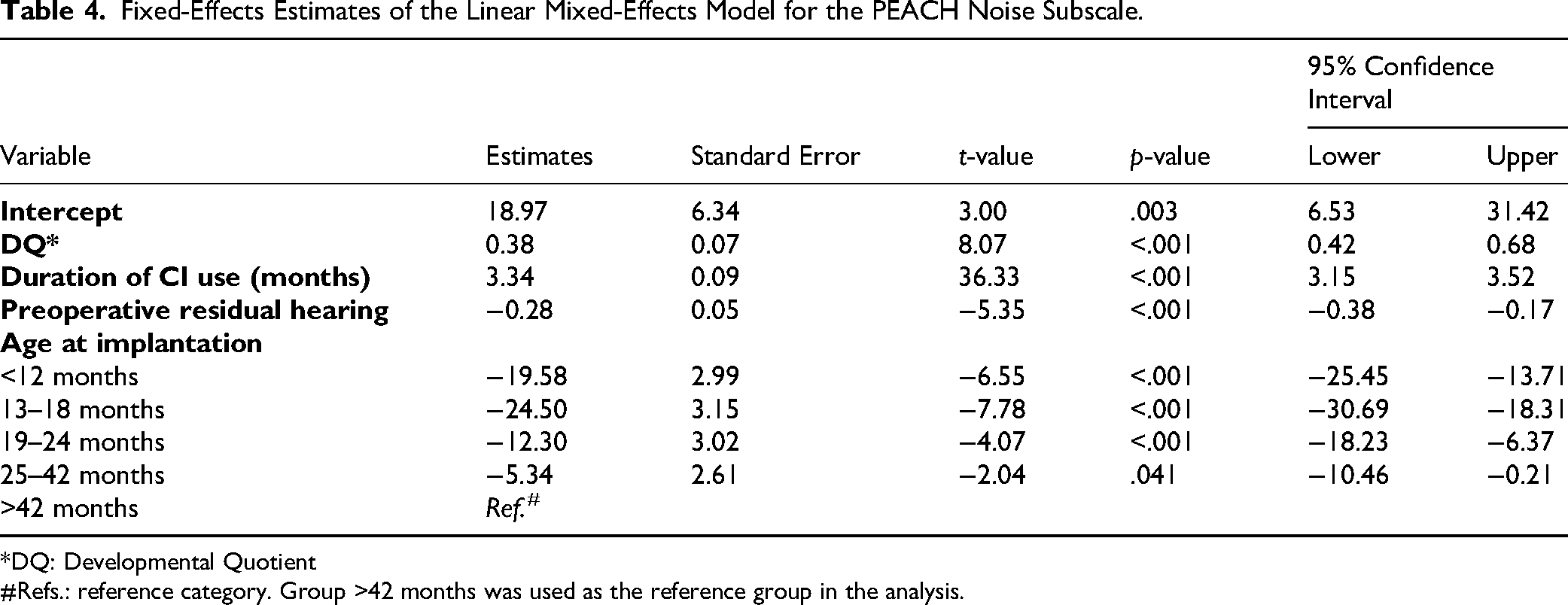
*DQ: Developmental Quotient
#Refs.: reference category. Group >42 months was used as the reference group in the analysis.
Fixed-Effects Estimates of the Linear Mixed-Effects Model for the PEACH Total Scale.

*DQ: Developmental Quotient
#Refs.: reference category. Group >42 months was used as the reference group in the analysis.
Evaluation Material and Procedure
To assess developmental status, children were evaluated using the Chinese revision of the Gesell Developmental Schedules before implantation. This version, adapted from the original 1974 edition, was translated and standardized in China between 1990 and 1992 by the Beijing Intelligence Development Collaborative Group to align with Chinese sociocultural contexts. The scale covers five domains—adaptability, gross motor, fine motor, language, and personal-social, and yields a Developmental Quotient (DQ = developmental age/chronological age × 100) (Beijing Intelligence Development Collaborative Group, 1992; Knobloch & Pasamanich, 1974). This assessment provided a baseline measure of general developmental status, which was considered in subsequent analyses.
This study used the Chinese version of the PEACH scale (Zhang et al., 2022), which was adapted from the English v4.1, to evaluate the functional auditory performance of children with CIs. Evaluations were administered longitudinally at CI switch-on (baseline), and at 1, 2, 3, 6, 12, 24, 36, 48, 60 months post-switch-on. During each assessment interval, audiologists guided the parents to recall how often they observed their child's auditory behavior over the last week in real-life situations. The PEACH rating scale consists of 12 items. Items 1–2 relate to device use and loudness discomfort, while items 3–12 are used to assess the auditory behaviors in quiet and noisy environments. Parents rate responses to each item on a 5-point scale (corresponding scores from 0 to 4 points) with the following descriptions: Never (0%), Seldom (1–25%), Sometimes (26–50%), Often (51–75%), and Always (76–100%). At each interval, the scores for items 3–12 were summed to obtain a total score. These items were also grouped into two subscale scores for quiet (sum of ratings for items 3, 5, 7, 9, and 11) and noisy listening conditions (sum of ratings for items 4, 6, 8, 10, and 12). The scores were then converted into percentage scores by dividing by the whole scale or for each subscale. When a child achieved a 100% PEACH score, another assessment was performed at the next interval to confirm a stable plateau had been reached.
Statistical Analysis
Statistical analysis was performed using SPSS software (version 26, IBM Corp., Armonk, NY, USA). Normally distributed data are reported as mean and standard deviation (M ± SD), whereas non-normally distributed data are reported as median and interquartile range [Median (IQR)]. To delineate the developmental trajectories of children's functional auditory performance, the PEACH percentage scores were arcsine transformed and then a logit function was fitted to the data using a least-squares method to minimize error. The PEACH scores were then compared to standardized normative data derived from Mandarin-speaking children (Zhang et al., 2022).
Participants were categorized into five age groups based on their age at implantation: <12 months, 13–18 months, 19–24 months, 25–42 months, and >42 months. This classification reflects established critical periods for central auditory development, with maximum neuroplasticity occurring within the first 3.5 years of life (Sharma et al., 2002). The 18-month boundary was specifically chosen based on large-scale evidence from Dettman et al. (2016).
To evaluate the functional auditory performance of children with CIs relative to their NH norms, we adopted the regression model from Zhang et al. (2022) to calculate age-expected NH scores. Children with CIs were considered as ‘within the normal range’ if their score fell within 2 standard deviations of the NH norms. Specifically, we calculated the proportion of children whose PEACH scores met this threshold at four chronological age milestones: 24, 36, 48, and 60 months, stratified by age-at-implantation groups (<12 months, 13–18 months, 19–24 months, 25–42 months, and >42 months).
To explore the factors influencing the total PEACH score before reaching a stable plateau, a linear mixed-effects model was fitted for PEACH score records within 24 months after CI switch-on. Previous literature has demonstrated that PEACH scores exhibit two distinct phases: a rapid growth period followed by a plateau phase (Bagatto & Scollie, 2013; Zhang et al., 2022). We employed a piecewise linear regression approach to identify the transition point, which was found at approximately 19 months of CI use. Given our assessment interval of 24 months, we defined the rapid growth phase as the period before 24 months of CI use. A total of 801 PEACH score records collected within 24 months of CI use were entered into the linear mixed-effects model.
Initially, all potential predictor factors were included in the model to assess their impacts on the PEACH outcomes. The model incorporated random intercepts to account for individual variability and random slopes where appropriate. A stepwise backward elimination procedure was used to refine the model. The significance level for retaining a variable in the final model was set at p < 0.05. This approach allowed for a parsimonious model, retaining only those variables that significantly contributed to explaining the variance in the outcome while controlling for random effects. Since the linear mixed-effects model accommodates missing values, no special treatment was applied to the missing data in this study.
To further explore the effect of listening environment on auditory performance development, we depicted scatter plots and fitted curves of auditory performance in quiet and noisy environments against chronological age. Two linear mixed-effects models were then constructed using scores from the quiet and noise environments, respectively.
Results
Device Use and Loudness Discomfort
For PEACH rating scale Item 1 (“How often has your child worn his/her hearing aids and/or cochlear implant?) and Item 2 (“How often has your child complained or been upset by loud sounds?”), parental ratings showed that the vast majority of children were able to use the CIs full-time (182 out of 187, 97.3%) within one month and did not experience discomfort to loud sounds (173 out of 187, 92.5%). The few children who had not achieved full scores on these two items at the one-month assessment quickly reached full scores in later follow-ups. The number of children achieving full scores on these two items increased to 184 and 181 at the 2-month assessment and reached 185 and 183 by 3 months. At 6 months, only one child had not attained full scores on those two items, and by the 9-month assessment, all participants had achieved maximum scores. This indicates that the pediatric subjects participating in the study quickly adapted to the CIs within a short period after activation. Furthermore, they were able to use the CIs consistently throughout the day and experienced no discomfort.
Developmental Trajectories of PEACH Total Scores in Relation to Age at Implantation
The analysis indicated that age at implantation significantly affected total PEACH scores (p < .001). Children demonstrated distinct developmental patterns, as depicted in Figure 1, which shows the development trend of the PEACH total scores for children with CIs across different age-at-implantation groups, along with their deviations from the normative curve. Notably, children implanted earlier displayed faster initial improvements in auditory functional performance, rapidly approaching NH benchmarks within the first two years post-implantation. This advantage of early implantation was particularly evident before 18 months of age. In contrast, children who received CIs later exhibited slower progression and lower total scores, indicating less pronounced auditory improvement.

Developmental trajectories of PEACH total scores across different age-at-implantation groups, with a comparison to the normative curve. Note: PEACH total scores (y-axis) are plotted against chronological age (months, x-axis). The data are grouped by age at cochlear implantation, as defined in the inset legend. Individual colored symbols represent the raw assessment scores for each participant, while the corresponding lines indicate the fitted growth curves with 95% confidence intervals. The solid black curve represents the normal-hearing normative developmental trajectory from Zhang et al. (2022).
Comparisons of PEACH Scores in Quiet Versus Noisy Environments Across Age-at-Implantation Groups
The PEACH scores of quiet and noise subscales revealed distinct developmental patterns for children with CIs under different auditory environments. As shown in Figure 2, scores in quiet environments were clearly higher than those noisy environments during the early stage. As age increased, both curves rose, and the gap between them narrowed, with scores in the two listening environments approaching one another, although a slight divergence emerged in the later assessments (Figure 2A). The later implanted group (25–42 months and >42 months) initially demonstrated a wider disparity between quiet and noisy performance, as shown in Figure 2B. Overall, the results indicated that children performed better in quiet than in noise at early stage, but the disadvantage in noise diminished as they grew older, particularly for those who received their implants earlier.

Comparison of PEACH scores in quiet versus noisy conditions and across age-at-implantation groups. Note: The quiet and noise subscale scores (%, y-axis) are plotted against chronological age (months, x-axis). Panel A (top) illustrates the overall comparison in quiet (blue) and noise (red) conditions, with scatter plots representing all data points and solid lines indicating fitted curves. Panel B (bottom, enclosed by the dashed frame) shows a similar quiet versus noise comparison of the PEACH scores but is classified into five subgraphs for each age-at-implantation group (<12 months, 13–18 months, 19–24 months, 25–42 months, >42 months).
Across both quiet and noisy conditions, four variables were identified as independently and positive predictors of PEACH scores: higher DQ, longer duration of CI use, better pre-operative residual hearing, and younger age at implantation. Notably, the analysis of the quiet subscale did not reveal a statistically significant difference in PEACH scores between the 25–42 months and post-42 months implantation groups (p = .236; Table 3). However, a significant difference was observed between these two groups in the noise condition (p = .041; Table 4).
Comparison of Auditory Performance with Normative Reference
We quantified, across five implantation age groups, the proportion of children whose PEACH scores fell within the normal-hearing range at 24, 36, 48, and 60 months of chronological age. At 24 months, 50% of children implanted before 12 months reached normative auditory performance, whereas all other groups showed minimal or no attainment. By 36 months, children implanted before 24 months showed marked improvements, while those implanted later continued to lag with limited progress. At 48 months, all children implanted before 24 months met the normative threshold. The 19–24 and 25–42 months groups improved to 50% and 59%, respectively. However, only 5% of children in the >42 months group met the threshold. By 60 months, nearly all children implanted ≤42 months achieved PEACH scores greater than 75%, whereas the >42 months group reached just 22%. These patterns are clearly shown in Figure 3.

Proportion of children with CIs meeting normal-hearing PEACH scores across critical developmental time points. Note: Proportion of children with CIs whose PEACH total scores fell within the normative range at four critical chronological ages milestones: 24, 36, 48, and 60 months. The children are grouped by age at implantation: <12 months (green), 13–18 months (red), 19–24 months (blue), 25–42 months (orange), and >42 months (grey). The exact proportions are displayed above each corresponding bar. The normative PEACH scores were obtained from a validated Mandarin-speaking dataset (Zhang et al., 2022).
Factors Influencing PEACH Total Scores
To investigate the factors influencing the total PEACH score, a linear mixed-effects model analysis was conducted (Table 5). Analysis indicated age at implantation was a critical factor. Compared to children implanted after 42 months (reference group), those implanted at a younger age demonstrated significantly higher PEACH scores. Children implanted before 18 months of age showed the greatest benefit, with effect estimates of −23.33 (SE = 4.80, 95 % CI [−32.82, −13.85], t = −4.86, p < .001) for the 13–18month group; and −20.18 (SE = 4.61, 95 % CI [−29.30, −11.07], t = −4.38, p < .001) for the < 12 months group. It is followed by those implanted between19–24 months (Estimates = −13.01, SE = 4.64, 95% CI [−22.19, −3.83], t = −2.81, p = .006). Compared to those implanted after 42 months, children implanted between 25–42 months showed a trend toward better outcomes, though this difference did not reach statistical significance (Estimates = −6.01, SE = 4.06, 95% CI [−14.05, 2.04], t = −1.48, p = .142).
Results also indicated that duration of CI use (Estimates = 4.90, SE = 0.13, 95% CI [4.64, 5.16], t = 36.86, p < .001) and DQ (Estimates = 0.53, SE = 0.10, 95% CI [0.33, 0.74], t = 5.19, p < .001) were significant, positive predictors of auditory performance. Conversely, preoperative residual hearing level negatively influenced PEACH outcomes (Estimates = −0.33, SE = 0.08, 95% CI [−0.49, −0.18], t = −4.26, p < .001), indicating that higher degree of pre-implant hearing loss was associated with reduced auditory performance outcomes.
To further illustrate group differences, we derived the estimated marginal means from the linear mixed-effects model after adjusting for relevant covariates. The estimated marginal means for the five age-at-implantation groups were 34.84 (<12 months), 31.69 (13–18 months), 42.01 (19–24 months), 49.01 (25–42 months), and 55.02 (>42 months), respectively. These means were calculated with covariates held at their preoperative residual hearing (86.83), DQ (70.74), and duration of CI use (5.16 months). The standard errors (SE) for these estimated marginal means ranged from 2.02 to 3.78, with a 95% CI [30.84, 62.50].
Discussion
The present study examined the longitudinal auditory development in Mandarin-speaking children with CIs based on the PEACH rating scale and compared their performance to normative data from Mandarin-speaking children with NH. This investigation highlights the distinct developmental trajectories observed across different age at implantation and identifies key factors influencing PEACH outcomes. The findings offer insights into the critical role of early intervention in achieving optimal auditory rehabilitation outcomes.
Developmental Trajectories Across Age at Implantation
The analysis consistently revealed that the age-at-implantation significantly influenced the development trajectories of PEACH score. As indicated in Figure 1, children implanted before 18 months of age exhibited the steepest improvement, closely approaching normative curve. In contrast, children who received CIs at 19–24 and 25–42 months demonstrated slower but steady progress, while those implanted after 42 months showed minimal improvement and greater individual variabilities. This evidence strongly supports the concept of a sensitive period, roughly within the first 3.5 years, during which the brain is highly receptive to auditory input. This sensitive period promotes superior neural development and speech and language learning (Kral & Sharma, 2012; Sharma et al., 2002).
The present study also indicated that the listening environment significantly influences PEACH performance. Specifically, as shown in Figure 2, children exhibited better performance on the quiet subscale at the initial stages. Over time, scores in noise improved, and the gap between quiet and noise performance narrowed. However, late-implanted children continued to show significantly lower scores in noise compared to the quiet condition. The linear mixed-effects model indicated that there was no significant difference between the 25–42 months and > 42 months groups in quiet (p = .236) but a significant difference in noise (p = .041). We speculate that this finding may be associated with reduced cortical noise adaptation in children who received CI later. The worse performance in noise highlights the need for targeted training, particularly for these late-implanted children. Prior studies have also shown that tone perception in noise remains more challenging for late-implanted children (Chen et al., 2014; Chen & Wong, 2017). The present study underscores the critical importance of early implantation and highlights the persistent challenges associated with delayed implantation.
Factors Influencing PEACH Outcomes
The linear mixed-effects model analysis provided significant insights into the key predictors influencing the PEACH outcomes. Age at implantation, duration of CI use, DQ, and preoperative residual hearing level were identified as significant factors.
Consistent with the observed developmental trajectories, earlier implantation was significantly related to better auditory outcomes. As shown in Figure 1, we observed that early-implanted children initially had lower scores but demonstrated a steeper growth trajectory, eventually approaching the performance plateau of NH children. In contrast, late-implanted children (especially those implanted after 42 months) appeared to reach a lower plateau in PEACH scores compared to their NH peers. These findings were further supported by Figure 3, which illustrated that children implanted before 18 months of age achieved normative performance early, emphasizing the importance of timely intervention. While the improvements in later-implanted groups (25–42 months) suggest the potential for substantial rehabilitation despite initial delays, the limited progress in children implanted after 42 months underscores the urgency of early diagnosis and intervention. Collectively, these results not only underscore the critical importance of early auditory intervention for achieving optimal outcomes but also indicate the necessity of providing additional rehabilitation strategies (e.g., intensive auditory training, or personalized rehabilitation plans) to enhance performance in late-implanted children.
Our study showed that the duration of CI use had a significant impact on auditory performance. Longer duration of CI use was consistently associated with higher PEACH scores, emphasizing the importance of maintaining consistent auditory input for optimal auditory development.
A higher DQ was strongly associated with better PEACH scores, highlighting the role of preoperative cognitive abilities in predicting auditory outcomes. This finding aligns with prior research (Yang et al., 2017), indicating that children with higher preoperative cognitive skills tend to demonstrate better auditory and language outcomes following CIs.
Additionally, the analysis showed that poorer preoperative residual hearing level was associated with reduced auditory and language outcomes following CIs, a finding consistent with other research (Zanetti et al., 2015), which highlights the importance of preserving residual hearing. Other factors, such as caregiver's education level and living environment, were not statistically significant in this study. This suggests that intrinsic and medical factors may play a more dominant role in determining auditory function outcomes (Marnane & Ching, 2015). Our initial hypothesis suggested that children in rural areas might demonstrate worse auditory outcomes post-CI due to potentially limited access to healthcare resources and fewer counseling sessions, hence leading us to include living environment as a variable. However, the subsequent analysis revealed no significant differences among rural, town, and city residents. This finding may be attributed to the recent improvements in healthcare resource homogenization across regions in China.
Limitations
Although this study provides robust statistical data through the longitudinal evaluation of a large cohort of 187 children with CIs, several limitations should be acknowledged. First, the limited characterization of hearing loss etiology, especially genetic factors, hindered a thorough analysis of their effects on the auditory performance. Future studies will incorporate more detailed etiological profiling to better elucidate intervention outcome predictors. Second, although we provided detailed information regarding the participants, the documentation of hearing aid interventions prior to cochlear implantation remained insufficiently detailed. This limitation may have introduced confounding bias in assessing factors affecting PEACH scores. In subsequent investigations, we will implement more rigorous protocols for recording comprehensive pre-implantation hearing aid intervention information. Third, our study included a majority of participants (60.4%) who received unilateral cochlear implantation, primarily due to economic constraints faced by families during the study's recruitment period in China. While all participants presented with bilateral profound hearing loss, the unilateral CI configuration may impact outcomes compared to bilateral or bimodal users. Fourth, the study included children fitted with various CI device models from different manufacturers. While manufacturer-specific coding strategies were consistently applied within each brand, the diversity of devices and programming parameters, which were determined by family preference and device specifications, these variables could be considered as factors affecting outcomes and may be acknowledged when interpreting future outcomes.
Conclusion
This study delineates the developmental trajectories of functional auditory performance, as measured by the Chinese PEACH scale, in Mandarin-speaking children with CIs across different ages at implantation. Furthermore, it elucidates the key associated influencing factors on these outcomes. The findings underscore the critical importance of early cochlear implantation for achieving optimal auditory rehabilitation, while also highlighting the persistent challenges faced by children with delayed implantation. This study provides reference values for interpreting PEACH assessment results in Mandarin-speaking children with CIs and offers evidence-based guidance for clinical intervention decision-making, emphasizing the need for tailored rehabilitation strategies to support optimal outcomes across diverse populations.
Footnotes
Acknowledgements
We gratefully thank all the children and their families for participation in this study. The authors sincerely thank Meiling Yan for her meticulous and indispensable assistance with the manuscript formatting and reference checking.This work was supported by Beijing Nova program [20250484804]; National Key Research and Development Program of China [grant number 2023YFF1203504].
Author's note
Professor Teresa Y.C. Ching is also affiliated with the Macquarie School of Education, Macquarie University, and the NextSense Institute, NextSense, both in Sydney, New South Wales, Australia, as well as the School of Health and Rehabilitation Sciences, The University of Queensland, Brisbane, Queensland, Australia
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key Research and Development Program of China, Beijing Nova Program, (grant number 2023YFF1203504, 20250484804).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.