
Abstract
Internet-based interventions have been developed to improve access to audiovestibular health care. This review aimed to identify outcomes of Internet interventions for adults with hearing loss, tinnitus, and vestibular disorders. Electronic databases and manual searches were performed to identify studies meeting eligibility for inclusion. Fifteen studies (1,811 participants) met the inclusion criteria, with nine studies targeting tinnitus distress, five considering hearing loss, and one for vestibular difficulties. Only the tinnitus and hearing loss Internet intervention studies were eligible for data synthesis. Internet-based interventions for hearing loss were diverse. Overall, they showed no significant effects, although a statistically significant moderate effect (d = 0.59) was found after removing the study with the highest risk of bias (as a result of high attrition). Most Internet-based interventions for tinnitus provided cognitive behavioural therapy. They yielded statistically significant mean effect sizes for reducing tinnitus distress compared with both inactive (d = 0.59) and active controls (d = 0.32). Significant effects were also present for the secondary outcomes of anxiety, depression, insomnia, and quality of life (combined effect d = 0.28). Only Internet-based interventions for tinnitus evaluated the 1-year postintervention effects indicated that results were maintained long term (d = 0.45). Scientific study quality was appraised using the Grading of Recommendations Assessment, Development and Evaluation approach and found to vary from very low to moderate. This review indicates the potential of Internet interventions for tinnitus to provide evidence-based accessible care. There is a need for additional high-quality evidence before conclusive results can be established regarding the effects of audiovestibular Internet interventions.
Introduction
Health-care provision aims to ensure clinically and cost-effective treatments are provided (Greenhalgh, 2017). Delivery of high-quality evidence-based health care is challenged by factors such limited finances, enough health-care workers, work pressures, and a lack of resources (Hignett et al., 2018). Evidence-based health care is also hampered by a research-to-policy gap, attributed to the low uptake of new interventions (Cairney & Oliver, 2017). Barriers associated with this disparity include lack of timely research outputs and research methodological shortcomings (Oliver, Innvar, Lorenc, Woodman, & Thomas, 2014). Moreover, health-care service delivery models have recently evolved from being more practitioner-centered to patient-centered, placing emphasis on patient engagement and shared decision-making (Richards, Montori, Godlee, Lapsley, & Paul, 2013). The greater use of digital technologies is an example of an attempt to overcome treatment barriers related to pressures on current health-care systems (Lupton, 2013).
Internet interventions are emerging as a means to provide affordable and accessible health care to promote self-management and engagement (Andersson, 2018). An Internet-based intervention is primarily a self-guided prescriptive program operated through a website. The intervention attempts to create positive change and improve knowledge and understanding of health-related conditions through the use of interactive web-based components (Barak, Klein, & Proudfoot, 2009). The information is generally divided into different modules with a set time frame for completion. Some Internet-based interventions are provided together with professional support (guided), whereas others do not offer the support (unguided). Guidance can be synchronized (e.g., real-time chats), asynchronized (e.g., not occurring at the same time such as when using e-mail), or using a blended approach by combining various approaches.
Internet interventions have been developed within the field of audiovestibular health care. This includes rehabilitation programs for those with hearing loss (Malmberg, Lunner, Kähäri, Jansson, & Andersson, 2015), tinnitus (Andersson & Kaldo, 2004), and vestibular rehabilitation (Geraghty et al., 2017). Although individual studies have been conducted, knowledge of the overall efficacy and effectiveness of Internet interventions for audiovestibular health care is required. A broad-spectrum systematic review focusing on identifying telehealth applications in audiology including screening, diagnostic, and intervention applications was published in 2010 (Swanepoel & Hall, 2010). In this review, seven telehealth intervention studies were identified that related to hearing aid fitting, cochlear implant programming, tinnitus therapy, and hearing aid counseling. The Swanepoel and Hall review included all study designs and was not limited to higher quality randomized controlled trial (RCT) designs. Since this review, additional studies of Internet interventions related to hearing loss rehabilitation and vestibular rehabilitation have been published. Therefore, an updated review with a focus specifically on audiovestibular Internet-based interventions evaluated with higher levels of evidence (RCTs) is warranted.
Other intervention-related systematic reviews do exist. They have, however, not been specific to Internet interventions for auditory disorders but have focused on wider applications. These include the use of eHealth for hearing aids, such as off-line, mobile-based applications and Internet-based platforms (Paglialonga, Nielsen, Ingo, Barr, & Laplante-Lévesque, 2018), and tele-audiology for the rehabilitation of hearing-impaired adults using hearing aids (Tao et al., 2018). Moreover, no review specific to Internet-based interventions for tinnitus was found, although an overview was provided of Internet-based tinnitus trials performed prior to 2015 (Andersson, 2015). Existing reviews on vestibular rehabilitation (Kundakci, Sultana, Taylor, & Alshehri, 2018; Martins e Silva et al., 2016; Ricci et al., 2010) have also not focused on Internet-based vestibular rehabilitation.
Determining the effects of Internet-based interventions for audiovestibular difficulties is important in order to establish their efficacy and effectiveness prior to considering whether they can be implemented in hearing health-care systems. The aim of this review was to investigate the outcomes of Internet interventions for adults with hearing loss, tinnitus, and vestibular disorders with the following specific questions:
What are the outcomes of Internet-based interventions in reducing hearing disability, tinnitus distress, and vestibular difficulties in adults? What are the outcomes of Internet-based interventions for adults regarding the associated difficulties of anxiety, depression, insomnia, and quality of life? Are the outcomes of Internet-based interventions for hearing disability, tinnitus and vestibular disorders maintained 1-year postintervention?
Methods
Protocol and Registration
This systematic review was prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO number CRD42018094801). The methods selected were guided by the Preferred Reporting Items for Systematic reviews and Meta-analyses (Moher, Liberati, Tetzlaff, Altman, & Prisma Group, 2009; see Supplementary Material File 1). The protocol can be found at (Beukes, Manchaiah, Baguley, Allen, & Andersson, 2018).
Eligibility Criteria
Inclusion and Exclusion Criteria for the Review.
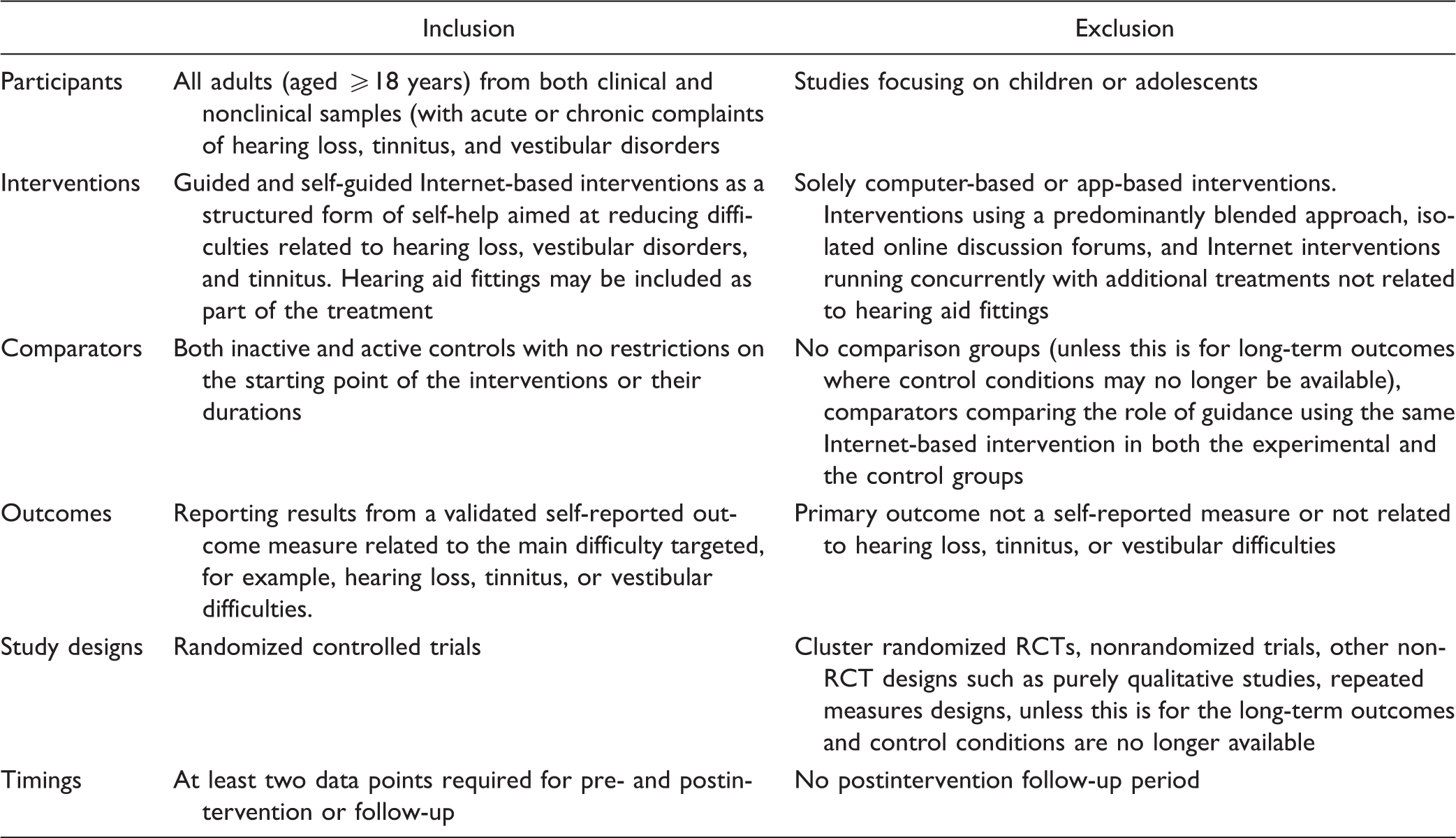
Information Sources
A systematic search was undertaken between June and July 2018 and again between October and November 2018 by the first author and an independent research assistant. This included the following electronic research databases: EBSCOhost including Allied and Complementary Medicine and Cumulative Index to Nursing and Allied Health Literature, PubMed (Including MEDLINE), Embase, and the Cochrane Central Register of Controlled Trials database. Manual searches comprised of trial registers at clinical.gov and Cochrane Ear, Nose and Throat Disorders Group Trials Register, hand-searching key journals and the reference lists from the included studies, gray literature in google scholar, and contacting stakeholders and research experts in the field.
Search strategy
A peer-reviewed search strategy was used using medical subject headings terms to target four key domains: (a) condition (e.g., hearing loss, tinnitus, and vestibular disorders), (b) intervention (e.g., intervention, treatment, therapy, program, strategy, self-help, rehabilitation), (c) mode of delivery (e.g., Internet, online, web-based), and study designs (randomized) were developed together with an information specialist at Anglia Ruskin University. The use of search terms and its Boolean combinations were adapted for each search engine to suit its requirements. Supplementary Material File 2 provides an example of the MEDLINE search strategy that was used to search titles and abstracts and the number of records returned.
Study Selection
Two authors (E. W. B. and V. M.) independently screened the studies to identify which met the inclusion criteria by viewing the abstracts. The full texts of the identified studies were subsequently read to determine eligibility. Interreviewer agreement using Cohen’s κ was .84 (standard deviation [SD]: 0.04), indicating strong agreement (κ of .80–.90; Cohen, 1960). Disparities were resolved through discussion with a third reviewer (G. A.).
Data Collection Process
Data from included studies were recorded on data extraction forms using the PICOTS format (University of York. Centre for Reviews and Dissemination, 2009). Data were extracted by E. W. B. and verified by V. M. The completed extraction forms were provided to all the authors for cross-checking. Where data were missing or unclear from the published studies, the publication authors were contacted. All authors responded and provided clarification.
Data Items
The Cochrane data collection form for intervention studies with an RCT format was used to develop the extraction forms. The forms were tailored for the research questions of this review. The form was piloted by E. W. B. and verified by V. M. If both intention-to-treat and per-protocol data were presented, the intention-to-treat estimation was used. The data variables collected can be found in Supplementary Material File 3.
Risk of Bias in Individual Studies
The risk of bias for the included studies was assessed using the Cochrane Collaboration’s tool (RoB 2) for randomized trials (Higgins et al., 2016). Included studies were assessed for bias across the following five domains: (a) bias arising from the randomization process, (b) bias due to deviations from intended interventions, (c) bias due to missing outcome data, (d) bias in measurement of the outcome, and (e) bias in selection of the reported results. Each item was judged as yes, probably yes, probably no, no, and no information by two reviewers (E. W. B. & V. M.). Any discrepancies were resolved by discussion and then by consulting with a third reviewer (G. A.). An overall risk of bias judgment was made as low risk of bias, some concerns, or a high risk of bias for each domain.
Summary Measures
Studies with more than one active treatment arm were aggregated and analyzed separately. The characteristics of the included studies were summarized according to the characteristics of the PICOTS design. The standardized mean difference (Cohen’s d effect size) was used as different scales of measurements were used to measure the same outcome. A positive effect size indicated that the Internet intervention group achieved better outcomes than the control group. Forest plots were constructed to visualize the effect sizes, confidence intervals, and heterogeneous nature of the included studies (Egger, Davey Smith, Schneider, & Minder, 1997).
Synthesis of Results
The meta-analysis was performed using Comprehensive Meta-Analysis software version 3 using the random effects model (Borenstein, Rothstein, & Cohen, 2005). A quantitative synthesis was included following considering whether it was possible to combine the individual studies included in the systematic review. This included a power analysis and assessment of heterogeneity (Valentine, Pigott, & Rothstein, 2010). Power calculations based on the random-effects model formula by Valentine et al. (2010) indicated that eight studies with an average of 45 participants were required to have 80% power to detect a small effect size (d = 0.30) at α = .05 with moderate heterogeneity. The following heterogeneity criteria were met: (a) included studies addressed similar questions, (b) there was a low risk of reporting and publication bias, (c) consistent outcomes were reported between studies, and (d) sensitivity analysis was performed where heterogeneity was high.
Quantitative synthesis was used to determine the mean difference with a 95% confidence interval for the pooled analysis for the included studies. The mean between-group postintervention scores (or mean change from baseline to follow-up for 1-year + outcomes) and SDs were used for these calculations (Borenstein, 2009). Due to the paucity of control groups during the ≥1-year follow-up phase for the trials (often due to the control group later also undertaking the Internet intervention), within-group mean gain effects were calculated for those who had undergone the treatment and had follow-up measures 1-year postintervention. In the case of repeated measures data, the correlation between pre- and follow-up assessment was estimated at r = .90, based on the average test–retest reliability of the tinnitus-specific outcome measures used by the individual studies. The standardized mean difference (Cohen’s d effect size) was used to pool data using different scales of measurements to measure the same outcome using a random-effects model. A positive effect size indicated that the Internet intervention group achieved better outcomes than the control group. Effect sizes of d < 0.5 represent a small effect, d ≥ 0.5 ≤ 0.8 a medium effect, and d ≥ 0.8 a large effect size (Cohen, 1992).
Consistency between studies was explored using the Q value and I2 statistic values. The I2 statistic results were broadly categorized on a range of 0% to 100% (25% low, 50% moderate, and 75% high) as suggested by Higgins, Thompson, Deeks, and Altman (2003). A p value of < .1 was considered statistically significant. If substantial heterogeneity was identified, this was explored through the prespecified subgroup analyses and sensitivity analyses, where sufficient data permitted τ2 was used to measure variance.
Risk of Bias Across Studies
Selective outcome reporting was applied by identifying whether there were any differences between the protocols and the final study of eligible studies. Authors were contacted to obtain additional information where required. Missing data were analyzed to determine whether it is missing at random or not, to determine the most appropriate way of dealing with the missing data (Shuster, 2011). Publication bias was explored using funnel plots. Orwin’s fail-safe N procedure was used to numerically identify bias. Duval and Tweedie’s trim and fill iterative procedure were used to remove the most extreme studies from the positive side of the funnel plot and recompute the effect size (Borenstein, Hedges, Higgins, & Rothstein, 2009).
Additional Analyses
Where sufficient data were available, data synthesis was performed for each Internet intervention (hearing loss and tinnitus). Additional subgroup analyses were conducted for:
Outcomes: primary and secondary (anxiety, depression, insomnia, and quality of life) at postintervention Long-term effect: 1-year postintervention effects for the primary outcomes Study designs: separating those with inactive and active comparators.
A sensitivity analysis was conducted by excluding those studies with a high risk of bias, thereby determining the robustness of the conclusions from the included studies. Assessing how outcomes of studies from specific (collaborating) research groups influence the summary effect size was also undertaken.
Confidence in the Cumulative Estimate
Judgments about the quality of the evidence for each research question were rated according to the Grading of Recommendations Assessment, Development and Evaluation protocol (Balshem et al., 2011). The level of evidence was scored to be high quality, moderate quality, low quality, or very low quality. These judgments were made independently by two reviewers (E. W. B., V. M.). The lower the score, the less confidence in the effect estimate; the higher the score, the more confidence there is that the true effect lies close to that of the estimate of the effect.
Results
Study Selection
Figure 1 shows the search results and included studies. Following determination of eligibility, 15 studies with 1,811 adult participants were included. Of these, five were hearing loss Internet interventions (350 participants), four were two-arm efficacy trials with inactive controls (Manchaiah, Rönnberg, Andersson, & Lunner, 2014; Molander et al., 2018; Thorén, Svensson, Törnqvist, Carlbring, & Lunner, 2011; Thorén, Öberg, Wänström, Andersson, & Lunner, 2014), and one was a two-arm effectiveness trial using an active control (Malmberg, Lunner, Kahari, & Andersson, 2017).
Flowchart of identified and included studies.
There were nine Internet interventions for tinnitus included (1,165 participants). Eight were two- to four-arm efficacy trials using a mixture of inactive and active controls (Andersson, Stromgren, Strom, & Lyttkens, 2002; Beukes, Baguley, Allen, Manchaiah, & Andersson, 2017; Hesser et al., 2012; Jasper et al., 2014; Kaldo et al., 2008; Nyenhuis, Zastrutzki, Jäger, & Kröner-Herwig, 2013; Weise, Kleinstauber, & Andersson, 2016) of which one reported only long-term results (Beukes, Allen, Baguley, Manchaiah, & Andersson, 2018) and one was an effectiveness trial (Beukes, Andersson, Allen, Manchaiah, & Baguley, 2018).
Only one Internet-based intervention two-arm effectiveness trial for vestibular rehabilitation met the inclusion criteria (Geraghty et al., 2017). Potential studies were most often excluded due to not fulfilling the criteria of being randomized or the intervention not being sufficiently Internet-based. A summary of the studies excluded is provided in Supplementary Material File 4.
Study Characteristics
Characteristics of the Included Studies.
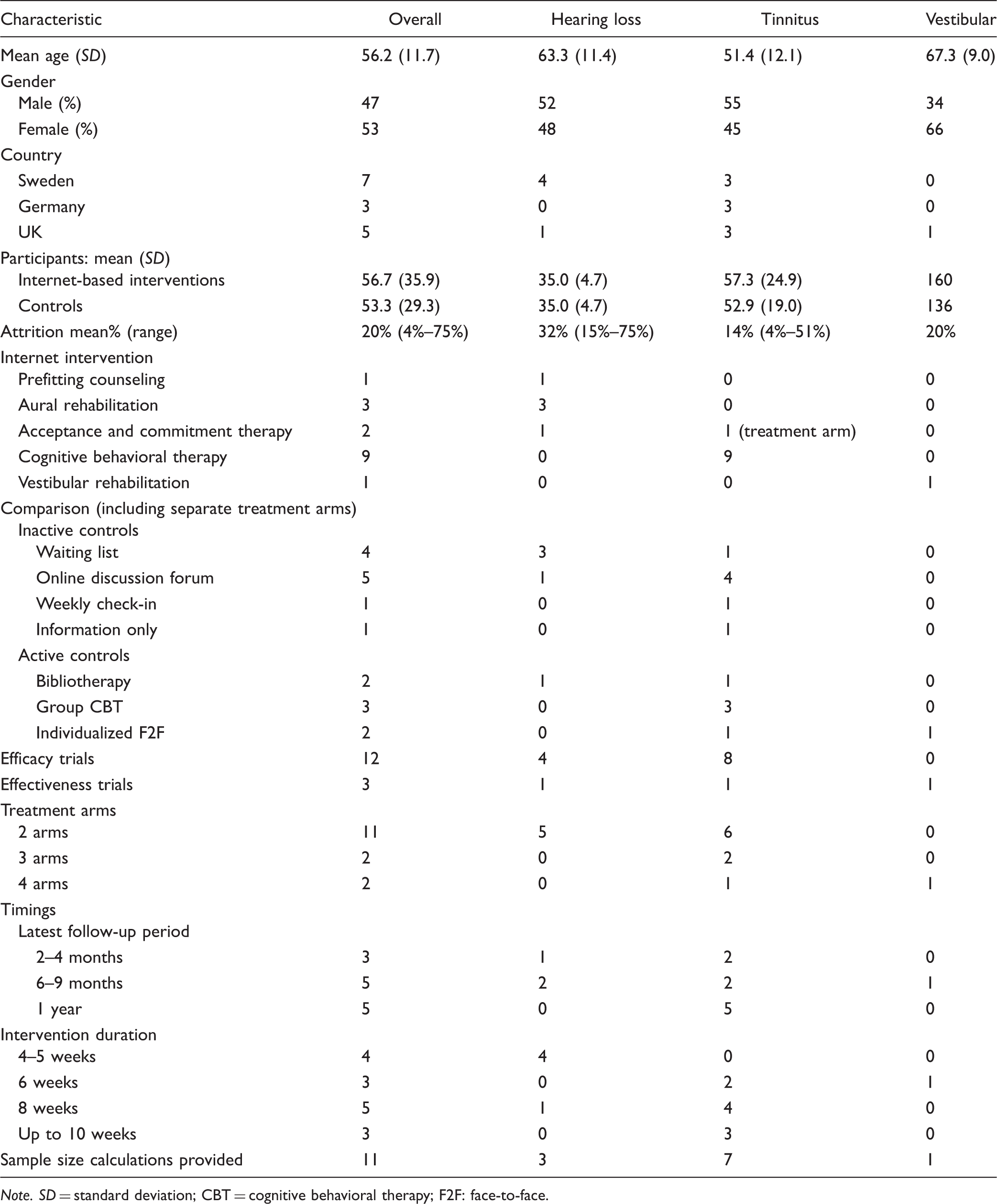
Note. SD = standard deviation; CBT = cognitive behavioral therapy; F2F: face-to-face.
The majority of the hearing loss interventions focused on aural rehabilitation. One was aimed at prehearing aid counseling (Manchaiah et al., 2014), one aimed to address associated psychological distress using acceptance and commitment therapy (Molander et al., 2018), one was for recent hearing aid users (Malmberg, Lunner, Kahari, & Andersson, 2017), and two for experienced hearing aid users (Thorén et al., 2011; Thorén et al., 2014).
Most of the tinnitus interventions were CBT and only one study included a treatment arm providing acceptance and commitment therapy (Hesser et al., 2012).
The vestibular Internet intervention was vestibular rehabilitation for adults aged 50 years or older experiencing motion-provoked dizziness in primary care (Geraghty et al., 2017). A multicenter effectiveness trial was undertaken comparing the Internet intervention with usual care. Results indicated that the Internet group had less self-reported dizziness and dizziness-related disability at 3 and 6 months postintervention compared with the usual care group. There was a greater reduction in anxiety at 3 months but not 6 months postintervention for the Internet group compared with the usual care group. There were no significant differences between the groups with regard to depression.
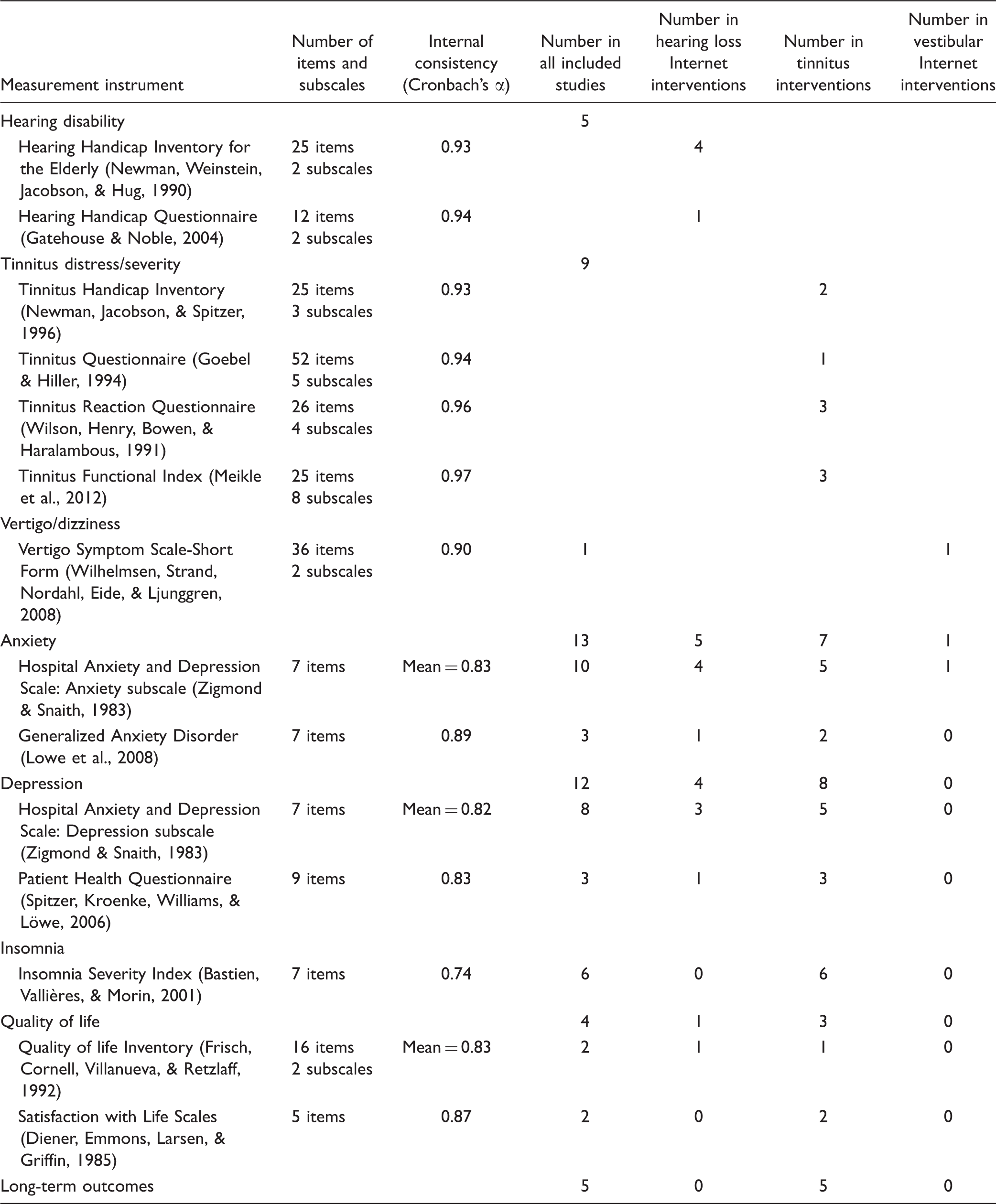
Outcome Measures Used in the Included Studies.
Risk of Bias Within Studies
The estimated risk of bias for the included studies was assessed using the Cochrane Collaboration’s tool (RoB 2) for randomized trials (Figure 2). There were two studies (13%) that had a high risk of bias (Andersson et al., 2002; Manchaiah et al., 2014). This was due to high attrition rates in these studies leading to a risk of bias due to missing outcome data and possible deviations from the intended interventions due to poor adherence. No bias in the selective reporting of results was identified. Some concerns were identified regarding the measurement of the outcome, as it was not always clear whether the data analyst was blinded for group allocation.
Estimated risk of bias across all included studies.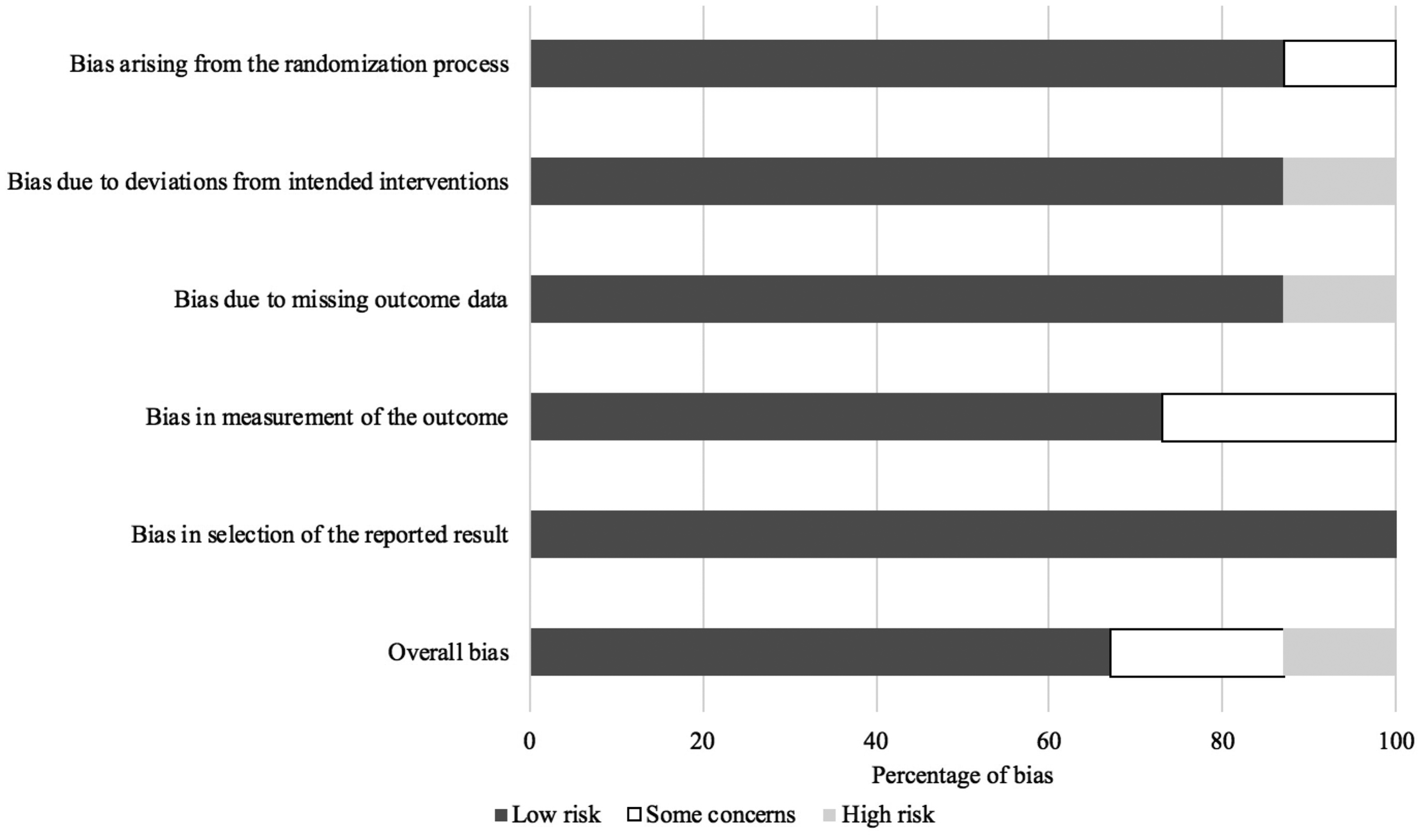
Risk of Bias Across Studies
Inspection of the funnel plots and Duval and Tweedie’s trim and fill procedure did not reveal any major publication bias in any of the meta-analyses conducted. As a formal test of funnel plot asymmetry, rank correlation testing indicated a nonstatistically significant Kendal’s τ rank correlation test (τ = −0.07, p = .71). The effect sizes adjustment for publication bias using the trim-and-fill procedure was implemented and imputed for three studies to adjust the point estimate from 0.40 to 0.32. Orwin’s fail-safe indicated that 54 studies were required to bring the effect size to >0.1.
Synthesis of Results
Of the 15 studies meeting the inclusion criteria, 14 were suitable for quantitative data synthesis. The study related to the vestibular Internet intervention (Geraghty et al., 2017) was excluded from the data synthesis due to a deviation of normality in the data. Calculating means and SDs from these data was not appropriate. There were five hearing loss Internet interventions included (four with inactive controls and one with an inactive control).
Summary of the Included Studies.

Note. Those with more than one active treatment arm have been subdivided to evaluate the effect of each treatment arm. Data from T3, T4, and H4 corrected in meta-analysis due to significant group differences between groups. Difference scores together with the pooled SDs were used for effect size calculations. F2F = face-to-face; HHIE = Hearing Handicap Inventory for the Elderly; IACT = Internet-based acceptance and commitment therapy; IAT = Internet-based auditory training; IAR = Internet-based aural rehabilitation; ICBT = Internet-based cognitive behavioral therapy; IPC = Internet-based prefitting counseling; IQR = interquartile range; IVR = Internet-based vestibular rehabilitation; F = female; GAD-7 = Generalized Anxiety Disorder; HADS = Hospital Anxiety and Depression Scale; HHQ = Hearing Handicap Questionnaire; M = male; PHQ-9 = Patient Health Questionnaire; QOLI = Quality of life Inventory (Frisch et al., 1992); RCT = randomized controlled trial; SWLS = Satisfaction With Life Scales; TFI = Tinnitus Functional Index; UK = United Kingdom; VSS-SF = Vertigo Symptom Scale-Short Form; SD = standard deviation; NA = not applicable; CI = confidence interval; GCTB = Group-based CBT; IO = Information only; TRQ = Tinnitus Reaction Questionnaire; ISI = Insomnia Severity Index; THI = Tinnitus Handicap Inventory; TQ = Tinnitus Questionnaire; ICT = Internet-based CBT; CBT = cognitive behavioral therapy.
Results of individual studies
The summary of the effects for the primary and long-term outcomes is found in Table 5 and in Figures 3 and 4. The quality of ratings (Grading of Recommendations Assessment, Development and Evaluation) ranged from very low to moderate. Subgroup analysis showed no difference when grouping studies from similar research groups, although the majority of studies were predominantly from a Swedish research group.
Forest plot of the overall effect of Internet-based interventions on hearing disability. CI = confidence interval. Forest plot of the overall effect of Internet-based interventions on tinnitus distress. CI = confidence interval; IACT: Internet-based acceptance and commitment therapy; ICBT = Internet-based cognitive behavioral therapy; IO = Information only; GCBT = Group-based CBT. Summary of Findings for the Primary and Long-Term Outcomes. Note. GRADE = Grading of Recommendations Assessment, Development and Evaluation; CI = confidence interval. For the full references, please refer to Table 4.


Outcomes of Internet-based interventions in reducing hearing disability
Results for Internet-based interventions in reducing hearing disability need to be interpreted with caution due to a lack of power and high heterogeneity. No significant favor was found for hearing loss Internet-based interventions over both inactive and active control conditions (see Figure 3). When hearing loss Internet interventions were compared with other inactive controls, high heterogeneity (I2 = 63%) was present. During sensitivity analysis, removing the study with the highest risk of bias largely due to high attrition rates (Manchaiah et al., 2014) improved heterogeneity (I2 = 0%). A moderate effect was obtained d = 0.59 (0.29–0.90), indicating study quality did affect the overall outcome. There was only one hearing loss Internet intervention with an active bibliotherapy control which did not indicate a significant favor for either intervention.
Outcomes of Internet-based interventions in reducing tinnitus distress
A medium overall effect size for the tinnitus studies was found at d = 0.50 (0.37–0.63) with low heterogeneity (I2 = 21%) favoring Internet-based interventions (p < 0.001). Significant favor (p < 0.001) of tinnitus Internet-based interventions over both inactive control conditions of d = 0.61 (0.47–0.72) and active controls of d = 0.35 (0.18–0.52) was found (see Figure 4).
The choice of outcome measure did not alter these results when grouping studies using the Tinnitus Questionnaires with similar constructs (e.g., removing those using the Tinnitus Questionnaire which has more items).
Additional Analysis
Outcomes of hearing loss Internet-based interventions in reducing associated difficulties
A small pooled effect size was found at d = 0.21 (0.05–0.37) for improving associated difficulties, favoring the hearing loss Internet interventions over the control conditions (see Figure 5 and Table 6). A small pooled between-group effect size for reducing depression using hearing loss Internet interventions was found at d = 0.29 (0.05–0.30). This indicated a significant favor over inactive controls at d = 0.41 (0.13–0.70), but no significant difference was found when comparing to the active bibliotherapy control trial. In terms of reducing anxiety, an equivalent finding between Internet interventions and the control groups was found both overall and when comparing to either inactive or active controls. Only the active control trial (Molander et al., 2018) assessed the effect on quality of hearing loss and found a large effect at d = 0.88 (0.35–1.40) compared with the bibliotherapy control group.
Forest plot of the associated effects of hearing loss Internet interventions. CI = confidence interval. Summary of Findings for the Secondary Outcomes. Note. GRADE = Grading of Recommendations Assessment, Development and Evaluation; CI = confidence interval. For the full references, please refer to Table 4.

Outcomes of tinnitus Internet-based interventions in reducing associated difficulties
A small pooled effect size was found at d = 0.29 (0.21–0.36) for improving associated difficulties, favoring the tinnitus Internet interventions over the control conditions (see Figure 6 and Table 6). Internet-based interventions for tinnitus significantly reduced anxiety and depression, indicating small effect sizes for these outcomes. This finding remained for studies using inactive controls but was not significant when using active controls.
Forest plot of the associated effects of tinnitus Internet interventions. CI = confidence interval.
The pooled between-group effect size for reducing insomnia from Internet interventions for tinnitus was d = 0.42 (0.27–0.57), indicating a significant favor of the Internet-based interventions over both inactive (d = 0.47) and active (d = 0.31) control conditions. There was no significant effect for quality of life.
Outcomes of Internet-based interventions in reducing tinnitus distress 1-year postintervention
For the trials using pre–post data (inactive controls where the control group was not followed up or also later undertook the Internet intervention), the overall within-group effect was small at d = 0.43 (0.27–0.59), and significant heterogeneity (I2 = 85%) was present. This finding remained for studies using inactive controls and indicated equivalent results in one study using group-based CBT as an active control.
Discussion
This review is the first to our knowledge evaluating the evidence base for Internet interventions for audiovestibular disorders. It investigated not only the primary effects but also the secondary and long-term effects of such interventions. As auditory-vestibular disorders are often associated with reduced quality of life, insomnia, anxiety, and depression investigating whether the interventions can improve these secondary effects was included in the review. The review identified 15 studies meeting the reviews’ inclusion criteria consisting of 1,811 adult participants. The majority of studies were tinnitus Internet interventions (nine studies) based on CBT, followed by five hearing loss Internet interventions (one prefitting, three posthearing aid fitting, and one for physiological distress) and one vestibular rehabilitation Internet intervention. Potential studies were most frequently excluded, as they did not fulfill the criteria of evaluating effects in a randomized format (e.g., Kaldo-Sandstroüm, Larsen, & Andersson, 2004; Pyykkő, Manchaiah, Kentala, Levo, & Juhola, 2017) or the intervention provided was not sufficiently Internet-based (e.g., Ferguson, Brandreth, Brassington, Leighton, & Wharrad, 2016). It is encouraging that more applications of Internet-based interventions exist when considering all these additional study designs (e.g., Paglialonga et al., 2018). The rest of the discussion focuses on the identified effects.
Summary of the Outcomes of Hearing Loss Internet-Based Interventions
A variety of approaches were used to provide hearing rehabilitation at different stages of the patient pathway and to address different difficulties encountered. A prefitting intervention was one approach (Manchaiah et al., 2014) and aural rehabilitation for recently fitted (Malmberg et al., 2017) and experience hearing aid users (Thorén et al., 2011; Thorén et al., 2014) were other approaches. There was also an intervention to address the associated psychological distress based on acceptance and commitment therapy (Molander et al., 2018). Drawing firm conclusions regarding these interventions is not possible due to the lack of power and high heterogeneity. No significant effect was found for Internet-based interventions; however, conducting a sensitivity analysis without the Manchaiah et al.’s (2014) study, which had high attrition, produced a significant moderate effect of d = 0.59 (0.29–0.90). These results indicate that although the evidence is not yet available, there are indications that Internet interventions for hearing loss can be of value and further high-quality studies in this field are indicated.
There are many challenges associated with developing these interventions due to the extensive professional input hearing loss rehabilitation requires. This input is also required at many stages of the patient journey. Moreover, Internet-based interventions may not be suitable for all types of interventions and populations, as some people, may not yet have come to terms with having a hearing loss. A state-of-the-art review regarding eHealth for adults with hearing aids found an increase in the development of eHealth resources for education and information regarding hearing loss and hearing aids, screening and assessments, hearing rehabilitation, and auditory and cognitive training (Paglialonga et al., 2018).
A small pooled effect size was found for improving secondary outcomes, favoring the hearing loss Internet interventions over the control conditions. A small effect size for reducing depression and equivalent finding between Internet interventions and the control groups for reducing anxiety was found. Only the active control trial (Molander et al., 2018) assessed the effect on quality of hearing loss and found a large effect compared with the bibliotherapy control group.
Much previous research related to auditory rehabilitation has focused on hearing aid use and the improvements these can bring to quality of life (Contrera et al., 2016), memory, depression, and cognitive status (Castiglione et al., 2016). When comparing those with and without long-term hearing aids (n = 666), hearing aids were found to reduce hearing handicap and promote physical health but not promote cognitive function, mental health, and social engagement (Dawes et al., 2015). The quality of auditory rehabilitation received in addition to the use of hearing aids may be a key factor.
The use of evidence-based Internet-based rehabilitation may enable greater access to this rehabilitation. Much work is still required to optimize Internet interventions to provide an effective rehabilitation pathway for hearing loss. Reduced diversity regarding the use of outcome measures and improvements in monitoring of the long-term effects will further build on the knowledge base of auditory rehabilitation for hearing loss (Barker, MacKenzie, Elliott, & de Lusignan, 2015). Incorporating eHealth for some aspects of hearing rehabilitation has many services and cost advantages, even if a blended approach is taken (Saunders, Brice, & Alimoradian, 2019). This may be an area where involving service users in the development of these interventions is key (as done by Ferguson, Leighton, Brandreth, & Wharrad, 2018). Working at overcoming present barriers and unifying intervention approaches to improve the feasibility and efficiency of such interventions should be the focus of subsequent research (Tao et al., 2018).
Summary of the Outcomes of Tinnitus Internet-Based Interventions
Overall, a more unified approach was present for Internet-based interventions for tinnitus in comparison to those for hearing loss and vestibular rehabilitation. All the Internet tinnitus interventions used CBT as the theoretical underpinning. A medium effect for tinnitus Internet-based interventions was found (d = 0.50), which was slightly higher at d = 0.59 for inactive controls than d = 0.32 for those with active control conditions.
The summary effects found for tinnitus Internet interventions were in line with those from a systematic review regarding tinnitus management (Hoare, Kowalkowski, Kang, & Hall, 2011) where an improvement was reported in 9 of the 10 trials comparing CBT for tinnitus (F2F and online) versus non-CBT controls. The results of this review are also similar to an earlier systematic review finding a significant effect for CBT tinnitus interventions in comparison with both inactive controls (g = 0.70) and active controls (g = 0.55; Hesser, Weise, Westin, & Andersson, 2011). The result of this review is slightly better than those reported in an earlier review by Martinez-Devesa, Perera, Theodoulou, and Waddell (2010) of d = 0.24 for inactive controls and d = 0.10 for active controls. A moderate overall effect size (g = 0.58) was also reported when reviewing Internet-based tinnitus interventions compared with inactive controls with a smaller effect of g = 0.13 for those compared with active controls (Andersson, 2015). When comparing guided Internet-based versus F2F CBT for psychiatric and somatic disorders, equivalent results were also found (Carlbring, Andersson, Cuijpers, Riper, & Hedman-Lagerlöf, 2018).
Similar to the hearing loss Internet interventions, a small pooled effect size was also found for favoring tinnitus Internet interventions over control conditions for improving associated difficulties. Internet-based interventions for tinnitus significantly reduced anxiety, depression, and insomnia. There was no significant effect for quality of life. This finding may partly relate to the lack of appropriate quality of life measures for tinnitus, making valid measurements of this aspect difficult.
Previous systematic reviews regarding CBT for tinnitus also reported small effect sizes that were marginally higher at g = 0.35 for mood measures when combining anxiety and depression measures (Hesser et al., 2011) and d = 0.37 for depression (Martinez-Devesa et al., 2010). In contrast, a review of tinnitus management strategies reported that only two of the seven studies found an improvement in depression and one of the three found an improvement in anxiety (Hoare et al., 2011). This review expanded on these reviews by considering secondary intervention effects as well. Of interest was that a much larger effect on the sensation of well-being (d = 0.91) was reported by Martinez-Devesa et al. (2010) for CBT tinnitus interventions, although this was calculated from tinnitus outcome measures and not using quality of life assessment measures. These results indicate that Internet interventions have potential to address associated difficulties that accompany hearing-related problems. Ways of maximizing these improvements should be sought (Donahue, Dubno, & Beck, 2010).
Overall results are maintained long term (1-year postintervention) for studies relating to tinnitus Internet interventions that generally used within-group comparisons. The longest follow-up for studies of Internet interventions for hearing loss and vestibular difficulties was 6 months. In a previous review, the longer term effects (3–18 months) of CBT tinnitus interventions were found to be higher at g = 0.60, although effect sizes decreased slightly over time (Hesser et al., 2011). More studies to evaluate the long-term outcomes of Internet interventions are required to monitor these effects even longer term. Future studies should also examine the applications of Internet-based interventions as a component in blended approaches, where Internet interventions are used as one component of care.
Summary of the Outcomes of Vestibular Internet-Based Interventions
Only one vestibular rehabilitation Internet intervention met the inclusion criteria. This was for a vestibular rehabilitation intervention for adults aged 50 years or older experiencing motion-provoked dizziness in primary care (Geraghty et al., 2017). There was a greater reduction in anxiety at 3 months but not 6 months postintervention for the Internet group and no significant differences between the groups with regard to depression. Data synthesis of this intervention was not possible and as only one study was identified, no clear conclusions can be drawn regarding the effects of Internet interventions for vestibular difficulties.
An Internet-based self-help resource for patients with Ménière’s disease was developed (Pyykkő et al., 2017) but did not meet the inclusion criteria for this review. Previous systematic reviews regarding the effectiveness of vestibular rehabilitation have found the benefits of these interventions, although only a few studies (n = 4–9) have been included in these reviews (Kundakci et al., 2018; Martins e Silva et al., 2016; Ricci et al., 2010). Even though these findings are encouraging, there is a clear need for further development of interventions to assist with vestibular difficulties, especially considering the high prevalence of these difficulties.
Study Implications and Future Directions
Internet interventions have the potential to improve accessibility and affordability of hearing health-care services and as a result have been the central focus of discussions about future hearing health-care delivery (Donahue et al., 2010). These interventions can be used as a replacement of routine care in certain conditions such as tinnitus (e.g., Beukes, Andersson, Allen, Manchaiah, & Baguley, 2018) or as supplementary care in conditions such as hearing loss (e.g., Thorén et al., 2011; Thorén et al., 2014; Malmberg et al., 2017). Attrition rates were variable (4%–75%) with an overall attrition rate of 20%. This is slightly higher than the average dropout rate of 16% for Internet versus F2F CBT for psychiatric and somatic disorders (Carlbring et al., 2018). Very similar dropout rates were found when comparing rates between those doing the Internet intervention and those in the active control conditions such as group-based therapy as also reported in the systematic review by Carlbring et al. (2018). Future Internet interventions should be mindful of incorporating strategies to improve attrition rates. It is clear from this review that more studies are required, particularly to address hearing loss and vestibular rehabilitation. Interesting, no Internet-interventions targeted the combination of hearing loss, tinnitus, or imbalance, yet often more than one audiovestibular condition is often found to occur in the same individual. To maximize outcomes of Internet interventions, it is important that future interventions implement elements and approaches and theoretical applications that are known to improve outcomes. Including a process evaluation can assist in identifying factors that contribute to the outcomes obtained (Moore et al., 2015). To date, there is only one example of a hearing-related Internet-based intervention including process evaluation (Beukes, Manchaiah, Baguley, Allen, & Andersson, 2018). Moreover, studies are needed to examine the cost–benefit and cost–utility analyses of Internet interventions for hearing-related conditions. Reporting of adverse and unwanted effects of Internet interventions was not prominent within the included studies. Presenting these data is important for future trials to be able to review their effects more holistically.
Limitations
This synthesis should be interpreted with caution, bearing in mind that high-quality evidence is not yet available for Internet interventions in the field of hearing disorders. Moreover, only published studies were included, and although publication bias was not found. The studies included were conducted in only three countries (Germany, Sweden, and the United Kingdom), making wider generalizations difficult. Only six studies monitored the long-term effects. Search limitations include that the inclusion criteria was limited to publications in English due to time and financial constraints. Due to the limited number of high-quality interventions present, data synthesis for the hearing loss interventions was slightly underpowered. Two studies with high risk of bias were included which contributed to study heterogeneity which further affected data synthesis. When further Internet interventions for tinnitus, hearing loss, and vestibular disorders have been developed and evaluated, reviews for each disorder in isolation are recommended.
Conclusions
This review indicates a lack of enough high-quality evidence to draw firm conclusions, although the potential of Internet interventions as a form of rehabilitation for auditory-vestibular difficulties is clear. The results from this review need to be interpreted considering the quality of the papers included, which ranged from very low to moderate quality evidence. Only two effectiveness studies were present, indicating that more research is required to establish how Internet interventions can be applied clinically and later implemented (Folker et al., 2018). This review can be used as an indication of research needs in view of the later implementation of these Internet interventions for audiovestibular disorders.
Supplemental Material
Supplemental Material1 - Supplemental material for Internet-Based Interventions for Adults With Hearing Loss, Tinnitus, and Vestibular Disorders: A Systematic Review and Meta-Analysis
Supplemental material, Supplemental Material1 for Internet-Based Interventions for Adults With Hearing Loss, Tinnitus, and Vestibular Disorders: A Systematic Review and Meta-Analysis by Eldré W. Beukes, Vinaya Manchaiah, Peter M. Allen, David M. Baguley and Gerhard Andersson in Trends in Hearing
Supplemental Material
Supplemental Material2 - Supplemental material for Internet-Based Interventions for Adults With Hearing Loss, Tinnitus, and Vestibular Disorders: A Systematic Review and Meta-Analysis
Supplemental material, Supplemental Material2 for Internet-Based Interventions for Adults With Hearing Loss, Tinnitus, and Vestibular Disorders: A Systematic Review and Meta-Analysis by Eldré W. Beukes, Vinaya Manchaiah, Peter M. Allen, David M. Baguley and Gerhard Andersson in Trends in Hearing
Supplemental Material
Supplemental Material3 - Supplemental material for Internet-Based Interventions for Adults With Hearing Loss, Tinnitus, and Vestibular Disorders: A Systematic Review and Meta-Analysis
Supplemental material, Supplemental Material3 for Internet-Based Interventions for Adults With Hearing Loss, Tinnitus, and Vestibular Disorders: A Systematic Review and Meta-Analysis by Eldré W. Beukes, Vinaya Manchaiah, Peter M. Allen, David M. Baguley and Gerhard Andersson in Trends in Hearing
Supplemental Material
Supplemental Material4 - Supplemental material for Internet-Based Interventions for Adults With Hearing Loss, Tinnitus, and Vestibular Disorders: A Systematic Review and Meta-Analysis
Supplemental material, Supplemental Material4 for Internet-Based Interventions for Adults With Hearing Loss, Tinnitus, and Vestibular Disorders: A Systematic Review and Meta-Analysis by Eldré W. Beukes, Vinaya Manchaiah, Peter M. Allen, David M. Baguley and Gerhard Andersson in Trends in Hearing
Footnotes
Acknowledgments
The authors thank the information specialist, Andrea Packwood at Anglia Ruskin University and Vibhu Grover, from Lamar University for assistance with the search strategy and systematic searches.
Authors’ Contributions
EWB and VM conceptualized this study. All authors contributed to the design and provided input across all sections. EWB performed all data analysis and drafted the manuscript. All authors approved the final version.
Authors’ Note
All authors views are their own and do not reflect those of their supporting institutions. David Baguley is supported by the U. K. National Institute for Health Research, but his opinions are his own and do not reflect those of the National Institute for Health Research or Department of Health and Social Care.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.