
Abstract
This systematic review and meta-analysis examined the efficacy of auditory training and cognitive training to improve cognitive function in adults with hearing loss. A literature search of academic databases (e.g., MEDLINE, Scopus) and gray literature (e.g., OpenGrey) identified relevant articles published up to January 25, 2018. Randomized controlled trials (RCTs) or repeated measures designs were included. Outcome effects were computed as Hedge’s g and pooled using random-effects meta-analysis (PROSPERO: CRD42017076680). Nine studies, five auditory training, and four cognitive training met the inclusion criteria. Following auditory training, the pooled effect was small and statistically significant for both working memory (g = 0.21; 95% CI [0.05, 0.36]) and overall cognition (g = 0.19; 95% CI [0.07, 0.31]). Following cognitive training, the pooled effect for working memory was small and statistically significant (g = 0.34; 95% CI [0.16, 0.53]), and the pooled effect for overall cognition was large and significant (g = 1.03; 95% CI [0.41, 1.66]). However, this was dependent on the classification of training approach. Sensitivity analyses revealed no statistical difference between the effectiveness of auditory and cognitive training for improving cognition upon removal of a study that used a combined auditory–cognitive approach, which showed a very large effect. Overall certainty in the estimation of effect was “low” for auditory training and “very low” for cognitive training. High-quality RCTs are needed to determine which training stimuli will provide optimal conditions to improve cognition in adults with hearing loss.
Introduction
Ageing is associated with a gradual decline in hearing (Liu & Yan, 2007) and cognitive function (Bishop, Lu, & Yankner, 2010). Approximately 500 million people live with hearing loss globally, and this figure is expected to rise with the ageing population (Wilson, Tucci, Merson, & O'Donoghue, 2017). Prevalence of dementia (including Alzheimer’s disease) has increased rapidly in recent years and is currently the second leading cause of death in Australia (Australian Bureau of Statistics, 2017). Estimates suggest that more than 30% of older adults live with moderate hearing loss (Lin et al., 2013), which may be associated with, or compounded by, progressive cognitive decline (Loughrey, Kelly, Kelley, Brennan, & Lawlor, 2017; Taljaard, Olaithe, Brennan-Jones, Eikelboom, & Bucks, 2016). Hearing loss is the highest modifiable midlife risk factor for dementia in later life (Livingston et al., 2017). Early management or prevention of hearing loss (World Health Organization, 2017) and cognitive decline (Shah et al., 2016) are more cost-effective than delayed treatment; have been reported as patient, family, and clinician priorities for research (Henshaw, Sharkey, Crowe, & Ferguson, 2015b); and are likely to improve quality of life for older adults.
Cross-sectional and longitudinal studies report increased risk of mild cognitive impairment, all-cause dementia, and Alzheimer’s disease among older adults with hearing loss (Jayakody, Friedland, Eikelboom, Martins, & Sohrabi, 2017a; Lin et al., 2011a, 2011b, 2013). Improvements in cognition have been suggested following management with hearing aids (Dawes et al., 2015) and cochlear implants (Jayakody et al., 2017b; Mosnier et al., 2015). However, meta-analytic evidence of 33 studies showed that for individuals with treated and untreated hearing loss, cognitive function (e.g., attention, short-term memory, executive function) was poorer compared with adults with normal hearing (Taljaard et al., 2016). Hearing impairment was also associated with worse performance across all cognitive domains (Taljaard et al., 2016). These results provide evidence of an association between hearing loss and cognitive decline in older adults. Despite amplification with hearing aids being shown to be effective at improving listening abilities, and hearing- and health-related quality of life for adults with hearing loss (Ferguson et al., 2017), more research is needed to determine the therapeutic potential of additional or alternative techniques (e.g., auditory training or cognitive training) to elicit optimal conditions for neural plasticity and associated improvements in cognitive function.
Auditory training refers to active engagement with sounds, whereby trainees learn to make distinctions between sounds presented systematically (Schow & Nerbonne, 2006). Traditionally, the goal of auditory training is to improve (bottom-up) sensory refinement of (often speech) sounds. However, there is a growing body of literature assessing auditory training-related top-down (cognitive) control processes important for listening, particularly in challenging listening situations (Ferguson & Henshaw, 2015; Pichora-Fuller & Levitt, 2012). Cognitive training refers to engagement with standardized, cognitively challenging tasks, to improve (or “exercise”) different cognitive functions (Lampit, Hallock, & Valenzuela, 2014). Both approaches aim to exploit neural plasticity to improve function. There are also some training programs available that combine auditory and cognitive stimuli, for example, the Earobics program (Ingvalson, Young, & Wong, 2014).
The concept of neural plasticity is of most importance for older adults who frequently experience gradual neurodegeneration as part of normal ageing (Cabeza, Anderson, Locantore, & Mcintosh, 2002). Neural plasticity is the adaption of anatomical structures (e.g., neurons, glial cells, synapses) and physiological processes (e.g., auditory perception, memory consolidation) following active engagement in an activity requiring the use of perceptual or cognitive resources (Cai, Chan, Yan, & Peng, 2014; Tremblay, 2007). When an individual acquires new knowledge/skills in response to training, the information can either strengthen existing neural pathways and networks or lead to the creation of new neural circuits and synapses (Wall, Xu, & Wang, 2002). During computer-delivered auditory training and cognitive training, an individual is exposed to repeated stimuli and required to practice activities that train auditory perception (Tremblay, 2007) and cognitive abilities (Shah, Weinborn, Verdile, Sohrabi, & Martins, 2017). Active engagement in training may therefore produce plastic changes in the brain by exposing older adults to novel stimuli and leading to improvements in auditory or cognitive function.
To determine whether auditory or cognitive training is effective, researchers can examine improvements in the tasks that are trained (on-task learning) and the transfer of learning to untrained (off-task) outcomes (Ferguson, Henshaw, Clark, & Moore, 2014), with the latter holding the most promise for real-world benefits that extend beyond the training task (e.g., general cognitive performance or practical skills for daily living; Henshaw & Ferguson, 2014). The efficacy of home-based interventions is also reliant on participant adherence to training (Chisolm et al., 2013). After all, an intervention can only ever be effective if it is used. It is therefore important that researchers report, and systematic reviews summarize, the extent to which participants adhere to auditory and cognitive training regimes and whether these interventions initially elicit on-task learning that transfers to improvement in off-task cognitive outcomes.
There has been a steady increase in research examining the potential of home-based computer-delivered auditory training for improving speech perception (and potentially cognition) in adults with hearing loss. Initial research reported beneficial effects of computer-delivered auditory training on speech perception and cognition in people with hearing loss (Sweetow & Henderson Sabes, 2006), and the methodological parameters of the intervention (home-based, remotely monitored) appealed to researchers and clinicians (Henshaw, Clark, Kang, & Ferguson, 2012). The increased popularity of these interventions led Henshaw and Ferguson (2013a) to review the evidence. Although most of the 13 studies reported improved speech intelligibility postintervention, only one study included standardized cognitive outcome measures, and the overall quality of evidence for studies included in the review was weak (Henshaw & Ferguson, 2013a). The authors concluded a need for well-designed and well-conducted randomized controlled trials (RCTs) to provide a more reliable estimate of the therapeutic potential of computer-delivered auditory training for improving auditory perception and cognitive function in those with hearing loss (Henshaw & Ferguson, 2013a). Since that review, more high-quality RCTs (Ferguson et al., 2014; Saunders et al., 2016) and other studies (e.g., Ferguson & Henshaw, 2015; Henshaw & Ferguson, 2014; Krishnamurti, Tingle, Bannon, & Armstrong, 2015) have examined computer-delivered auditory training and its effects on outcomes including cognition, but findings are mixed; therefore, a systematic review and meta-analysis of the results is warranted.
Computer-delivered cognitive training improves (on-task) cognition in healthy older adults (Lampit et al., 2014) and in people with mild cognitive impairment (Hill et al., 2016) and Parkinson’s disease (Lawrence, Gasson, Bucks, Troeung, & Loftus, 2017). Preliminary evidence in hearing loss suggests that computer-based cognitive training may improve (on-task) working memory (Bansal, 2014; Oba, Galvin, & Fu, 2013), executive function, verbal memory, and attention in cochlear implant recipients (Bansal, 2014). Research has also shown an association between cortical areas that contribute to auditory perception and performance of specific cognitive abilities (e.g., attention and working memory) in those with hearing loss. Anderson, White-Schwoch, Parbery-Clark, and Kraus (2013b) compared the beneficial effects of auditory-based cognitive training (“Brain Fitness”) with an active control group and reported improved neural response timing to speech in noise and improved short-term memory and speed of processing posttraining. Reviews by Akeroyd (2008) and Lunner, Rudner, and Ronnberg (2009) also suggested that working memory is most frequently associated with an individual’s improved speech recognition in noise and response to hearing aid processing of speech. Computer-delivered cognitive training may therefore improve cognition and auditory perception by training cognitive domains (e.g., working memory) associated with improved processing of speech in people with hearing loss.
To summarize, older adults frequently experience hearing loss and cognitive decline, and research shows a behavioral and potential pathophysiological association between the two. Home-based computer-delivered auditory training and cognitive training may provide optimal conditions to elicit neural plasticity and improve cognitive function in older adults with impaired hearing. However, the original systematic review by Henshaw and Ferguson (2013a) examined only auditory training interventions, and only one study included cognitive outcomes, which did not permit a meta-analysis of results. Moreover, there is no published systematic review or meta-analysis of cognitive training for improving cognition in adults with hearing loss. It therefore remains unclear whether auditory training or cognitive training is most efficacious for improving cognition in this population.
The primary aim of this systematic review and meta-analysis is to determine if auditory training or cognitive training can improve cognitive function in adults with hearing loss. The secondary aims are to determine which intervention is most efficacious for improving cognition in this population, whether beneficial effects are seen for on-task (trained) and off-task (untrained) outcomes, and whether participants adhere to an intervention with limited supervision.
Methods
Search Strategy
This systematic review was conducted in accordance with the Preferred Reporting of Systematic Reviews and Meta-Analyses (PRISMA) statement (see Supplementary Table 1; Moher, Liberati, Tetzlaff, & Altman, 2009) and was prospectively registered with PROSPERO (ID: CRD42017076680). Key terms were systematically searched in online databases (e.g., MEDLINE, Scopus) for published articles, gray literature (e.g., OpenGrey), and completed trials in preparation for publication (e.g., Clinicaltrials.gov). Search parameters were from first date of publication to January 25, 2018 and limited to adult participants and English language (see Supplementary Table 2). Reference lists of published articles were also searched.
Study Selection
Studies were included in the systematic review if they (a) recruited adult participants with postlingual hearing loss with or without hearing aids or cochlear implants, (b) evaluated home-based computer-delivered auditory training or cognitive training, (c) used an RCT or repeated measures design, and (d) used primary outcomes measured by standardized neuropsychological tests of cognitive function. For the purposes of this review, interventions were classified as either auditory or cognitive training based on the underlying training task constructs. Two lead authors (B. J. L. and D. M. P. J.) screened article titles and abstracts in line with selection criteria and identified preliminary articles for inclusion. Both authors then independently screened selected articles to determine the final studies for inclusion. Disagreements were resolved through discussion.
Data Extraction
The data extracted from each study included participants, interventions, comparisons, outcomes, and study design (PICOS; Moher et al., 2009). Participant adherence to a training intervention was also extracted. Cognitive outcomes were categorized in accordance with neuropsychological handbook recommendations (Strauss, Sherman, & Spreen, 2006) and following methods from previous reviews of cognitive training (Hill et al., 2016) and cognition/hearing loss in older adults (Taljaard et al., 2016). Only three studies reported outcomes beyond those immediately postintervention. One cognitive training study reported outcome results at 1 month (Oba et al., 2013) and another at 2 weeks and 6 months (Henshaw & Ferguson, 2013b) postintervention; this difference in follow-up time did not permit examination of a pooled intervention effect. One auditory training study reported outcomes at 6 months postintervention (Saunders et al., 2016). Corresponding authors were contacted when study information, participant characteristics, and necessary data to compute an effect size were not reported.
Quality of Evidence
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) system was used to assess the quality of evidence (Schünemann, Brozek, Guyatt, & Oxman, 2017). The GRADE system evaluates the quality of evidence across studies for each outcome included in a systematic review and is summarized by an overall “certainty of evidence” grading. Gradings range from “very low” to “high” and represent the extent of certainty in an outcome result as a reliable estimate of an intervention’s true effect (Schünemann et al., 2017).
Statistical Analysis and Publication Bias
Data analysis was completed using Comprehensive Meta-Analysis version 3.3.070 (Borenstein, Hedges, Higgins, & Rothstein, 2011). For studies that used RCT designs, the change score method from pre- to postintervention was used to calculate the absolute magnitude of change between intervention and control groups. For repeated measures designs, pre- and postintervention means and standard deviations and the correlation between these scores were used to calculate the degree of change during the intervention. When studies did not report means and standard deviations, t statistics and probability levels for between-group tests were used to compute effect sizes (Ray & Shadish, 1996). Effect sizes for each outcome were then computed as Hedge’s g (Borenstein et al., 2011). For studies that reported multiple conceptually related outcomes for individual cognitive domains, effect sizes were calculated by computing the mean effect within each domain and adjusting the mean variance by 0.8 to correct for intercorrelation among outcome. Domain effect sizes and adjusted variances were then pooled using a random-effects model, with 95% confidence intervals (Borenstein et al., 2011; Hedges & Vevea, 1998). Mixed effects Q tests for between-groups analysis of variance was used to compare auditory training and cognitive training pooled effects (Borenstein et al., 2011). Egger’s regression asymmetry test and Fail-Safe
Heterogeneity and Sensitivity Analyses
Cochrane’s Q and I2 statistics were used to examine heterogeneity. A difference between an observed and true effect is measured by a statistically significant Q statistic (Huedo-Medina, Sánchez-Meca, Marín-Martínez, & Botella, 2006). However, the Q statistic may overestimate this difference in small sample sizes. If Q was statistically significant, the I2 statistic estimated the percentage of variation across the samples due to heterogeneity. I2 values of 0% to 40% (low), 41% to 60% (medium), and 61% to 100% (high) were used to categorize levels of heterogeneity (Moher et al., 2009). For pooled effect estimates with statistically significant heterogeneity, sensitivity analyses were conducted to examine whether removing studies with anomalous characteristics (e.g., intervention type, participant subgroups) would account for the heterogeneity and impact pooled effects.
Results
Search Results
In total, 3,317 titles and abstracts were systematically screened in online databases. Fifty-three studies were retrieved for full-text evaluation. Forty-four were excluded as they did not include standardized neuropsychological outcomes measuring cognition (30), were not a home-based training intervention (7), did not include auditory or cognitive training (1), were a case-control design (2), were a review article (2), did not include participants with only postlingual hearing loss (1), or were a duplicate sample (1). Figure 1 provides the PRISMA flow chart for search results.
PRISMA flow chart of search results.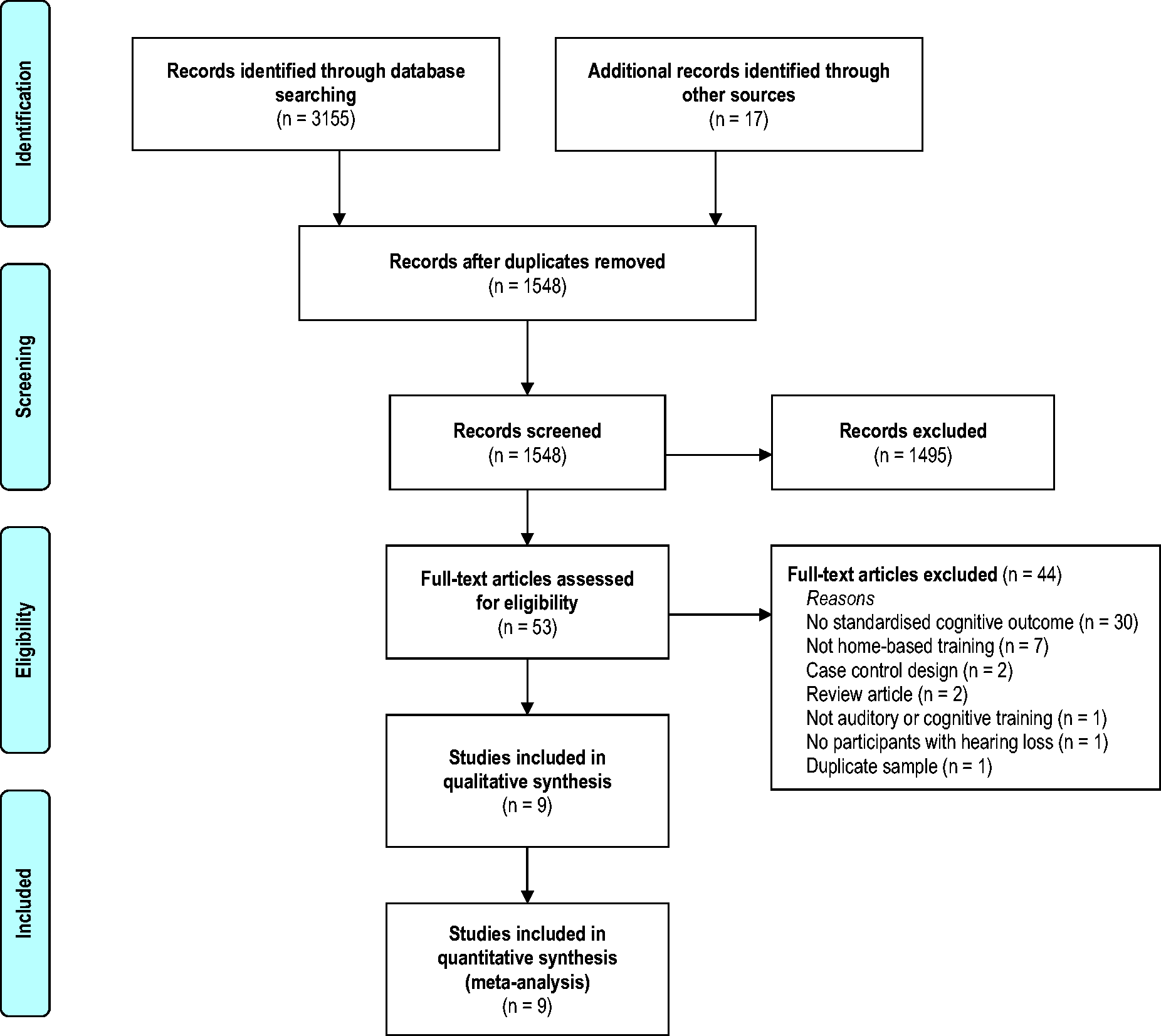
Study Characteristics
Summary of Included Auditory Training Studies.

Note. dB = decibels; IHR-STAR = Institute for Health Research System for Testing Auditory Responses; IQ = intelligence quotient; M = mean; PTA = pure tone average; SD = standard deviation; SNHL = sensorineural hearing loss.
aStudy information collected from systematic review by Henshaw and Ferguson (2013a) and confirmed with original publication.
Summary of Included Cognitive Training Studies.
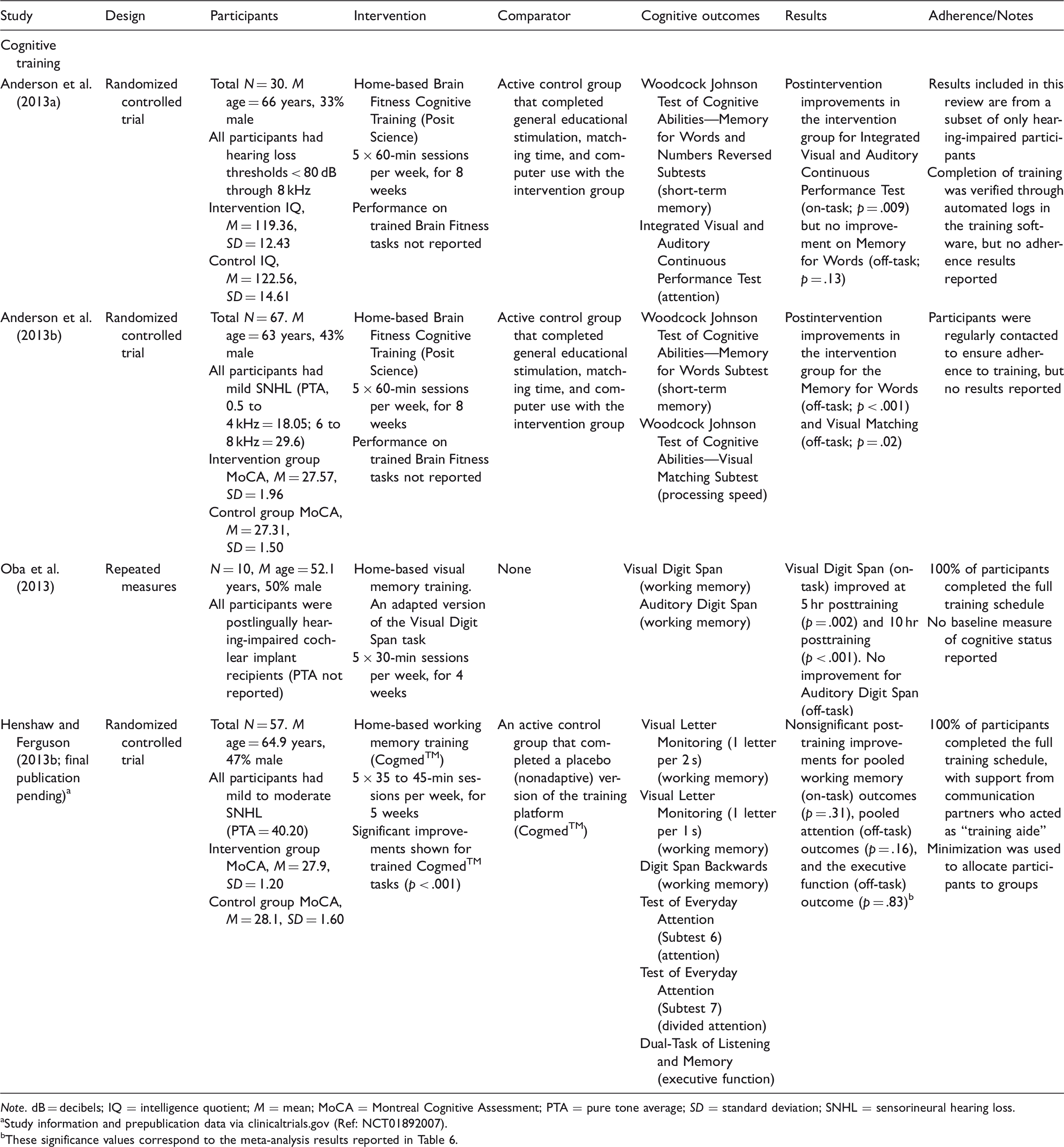
Note. dB = decibels; IQ = intelligence quotient; M = mean; MoCA = Montreal Cognitive Assessment; PTA = pure tone average; SD = standard deviation; SNHL = sensorineural hearing loss.
Study information and prepublication data via clinicaltrials.gov (Ref: NCT01892007).
These significance values correspond to the meta-analysis results reported in Table 6.
Five studies examined auditory training (Ferguson et al., 2014; Henshaw & Ferguson, 2014; Krishnamurti et al., 2015; Saunders et al., 2016; Sweetow & Henderson Sabes, 2006) and four examined cognitive training (Anderson et al., 2013a, 2013b; Henshaw & Ferguson, 2013b; Oba et al., 2013). Six studies were RCTs (Anderson et al., 2013a, 2013b; Ferguson et al., 2014; Henshaw & Ferguson, 2013b; Saunders et al., 2016; Sweetow & Henderson Sabes, 2006), and three adopted repeated measures designs (Henshaw & Ferguson, 2014; Krishnamurti et al., 2015; Oba et al., 2013). For one completed clinical trial (Henshaw & Ferguson, 2013b, final publication pending), data were obtained from the authors at the point of upload to clinicaltrials.gov (Ref: NCT01892007). Saunders et al. (2016) reported data for four groups, comparing two forms of LACE™ auditory training with a placebo training group and a control group. Results for Saunders et al. (2016) were therefore reported as four individual effect estimates.
Neuropsychological Tests Used to Measure Cognition Among Included Studies.

Quality of Evidence
.GRADE Summary of Evidence for Auditory Training.

Note. CI = confidence interval; g = Hedge’s g; GRADE = Grading of Recommendations Assessment, Development and Evaluation; NA = unable to grade inconsistency with only one study contributing to summary effect.
Four studies including seven subgroups.
Certainty of evidence downgraded one level because a proportion of studies were graded as high risk of bias across multiple criteria.
Study effects were consistent, and nonsignificant heterogeneity supported the overall consistency within the pooled effect.
Indirectness was not downgraded considering studies adopted similar intervention parameters and outcomes.
Certainty of evidence downgraded one level for imprecision because few studies with small N participants were included in pooled effect.
Certainty of evidence downgraded one level for indirectness because intervention parameters varied between studies.
Certainty of evidence downgraded one level for inconsistency because there was a moderate degree of heterogeneity within the pooled effect.
The study included in this effect was a high-quality randomized control trial with no risk of bias.
Five studies including eight subgroups.
GRADE Summary of Evidence for Cognitive Training.

Note. CI = confidence interval; g = Hedge’s g; GRADE = Grading of Recommendations Assessment, Development and Evaluation; NA = unable to grade inconsistency with only one study contributing to summary effect.
Certainty of evidence downgraded one level because a proportion of studies were graded as high risk of bias across multiple criteria.
Study effects were consistent, and nonsignificant heterogeneity supported the overall consistency within the pooled effect.
Indirectness was not downgraded considering studies adopted similar intervention parameters and outcomes.
Certainty of evidence downgraded one level for imprecision because few studies with small N participants were included in pooled effect.
The study included in this effect was a high-quality randomized control trial with no risk of bias.
Certainty of evidence downgraded one level for inconsistency because there was a large degree of heterogeneity within the pooled effect.
Adherence to Training
Percentage of participants who completed a recommended duration of auditory or cognitive training was used to assess adherence (Henshaw & Ferguson, 2013a). Six out of nine studies reported participant adherence. Sweetow and Henderson Sabes (2006) reported 73% of participants (65/89) completed the auditory training intervention, which involved 5 × 30-min training sessions per week for 4 weeks. Henshaw and Ferguson (2014) did not report the percentage of participants who completed the intervention but did state the average time spent completing auditory training was 197.8 min, which was less than the predetermined 210 min intervention. Ferguson et al. (2014) reported 80% (35/44) of participants completed the auditory training intervention. Saunders et al. (2016) reported 85% of their LACE-DVD group (58/68) completed the intervention, but this figure was self-reported adherence, and 84% of their LACE-C group (42/50) adhered with the full auditory training intervention. Oba et al. (2013) stated that 100% of participants (N = 10) completed the full cognitive training schedule. Henshaw and Ferguson (2013b) provided raw data indicating that 100% of participants, who were supported and monitored by their communication partner, completed their 5-week (25-session) cognitive training intervention. Three studies did not report adherence to training (Anderson et al., 2013a, 2013b; Krishnamurti et al., 2015), but Anderson et al. (2013a, 2013b) stated that participants were regularly contacted or monitored during the intervention to ensure they adhered to training parameters.
Auditory and Cognitive Training: Improvements for Trained Tasks
All auditory training studies, excluding one (Saunders et al., 2016), reported statistically significant improvement on the auditory tasks participants completed during interventions (see Table 1). Of the cognitive training studies, Henshaw and Ferguson (2013b) and Oba et al. (2013) reported statistically significant improvement on trained intervention tasks (see Table 2), whereas Anderson et al. (2013a, 2013b) did not report participant performance on training tasks.
Auditory and Cognitive Training: Improvements in Outcomes
Meta-Analysis Results for Auditory Training and Cognitive Training Studies.

Note. A/PS = attention/processing speed; CI = confidence interval; EF = executive function; g = Hedge’s g; p = significance level; Q = Cochrane’s Q; ST-M = short-term memory; WM = working memory.
Computer intervention compared with placebo group.
Computer intervention compared with control group.
DVD intervention compared with placebo group.
DVD intervention compared with control group.
p < .05. **p < .001.
On-Task and Off-Task Cognitive Outcomes
All cognitive outcomes contributing to the significant pooled effect of auditory training improving overall cognition were classified as off-task (untrained), indicating that auditory training provides a small transfer of learning to untrained cognition (see Table 6). For cognitive training, however, five pooled outcomes were classified as off-task and three pooled outcomes as on-task, given their substantial overlap with tasks that were trained (see Table 6). Compared with the studies that included on-task cognitive outcomes (Anderson et al., 2013a; Henshaw & Ferguson, 2013b; Oba et al., 2013), the off-task and untrained outcomes unique to Anderson et al.’s (2013b) intervention demonstrated the largest improvement following training.
Publication Bias
Publication bias statistics were calculated for statistically significant pooled effects including more than two studies. For the effect of auditory training on overall cognitive function, Egger’s regression was statistically significant (p = .02), indicating the presence of publication bias, and 25 studies with nonsignificant results would be needed to render this effect zero.
Egger’s regression was significant (p = .04) for the effect of auditory training on working memory, and Rosenthal’s Fail-Safe N indicated that 11 nonsignificant results were needed to undermine the significant effect. For the effect of cognitive training on overall cognition, Egger’s regression was not significant (p = .18), and 160 nonsignificant results would be needed to render this effect zero.
Sensitivity Analyses
Changes in Pooled Effect Sizes Following Sensitivity Analyses.

Note. CI = confidence interval; g = Hedge’s g; p = significance level; Q = Cochrane’s Q.
p < .05. **p < .001.
Discussion
The present study is the first systematic review and meta-analysis to provide pooled effect estimates of both auditory training and cognitive training for improving cognitive function in adults with hearing loss. The primary aim of cognitive training is to improve cognitive function, but given the relationship between listening and cognition, this type of training might have consequential benefits for adults with hearing loss. The primary aim of auditory training is to improve auditory skills, but recent evidence suggests there may improvements in cognition (Ferguson & Henshaw, 2015). Here, we are looking at how effective each type of training is on cognition for this population.
When auditory training studies were combined, there were small but significant transfer of learning effects favoring improved working memory and overall cognition. The beneficial effect of auditory training on cognition may be explained by the Ease of Language Understanding model (Rönnberg et al., 2013) within the Scaffolding Theory of Ageing and Cognition (Goh & Park, 2009). The Ease of Language Understanding model suggests that working memory (a primarily frontal function) is a cognitive resource responsible for an individual’s successful use of attention when listening to speech, processing and interpretation of hearing aid signals, and potential hearing impairment impacting their long-term memory (Rönnberg et al., 2013). The Scaffolding Theory of Ageing and Cognition suggests that older adults experience a decline in cortical function as part of normal ageing, and the ageing brain recruits (scaffolds) additional cognitive resources from frontal regions to compensate for functional deficits (Goh & Park, 2009). Older adults with hearing loss may therefore recruit additional (frontal) cognitive resources to compensate for diminished auditory perception and to support their attention and working memory capacity during auditory training. Auditory training may provide a small consequential improvement in working memory and overall cognition, which are trained during tasks that require the concomitant use of auditory perception and cognitive resources by adults with hearing loss.
When separated into individual cognitive domains, which resulted in a small number of studies, auditory training pooled effects reduced to nonsignificance for executive function and attention/processing speed. These nonsignificant effects may be the result of a Type II error, with small to moderate effect sizes reported for individual domains, but only two (or fewer) studies were included in these pooled effects. Nonetheless, home-based computer-delivered auditory training appears to provide a small improvement in cognitive function in adults with hearing loss.
When cognitive training studies were combined, there was a large and statistically significant improvement in overall cognition, driven by both on- and off-task learning. When separated into individual cognitive domains, pooled effects reduced to nonsignificance for executive function, short-term memory, and attention/processing speed. However, there was a high degree of heterogeneity across studies, which was eliminated on removal of Anderson et al (2013b). This raises some important questions about how the training in this study was classified. Anderson et al. (2013b) used a cognitive training program (“Brain Fitness”) that primarily targeted working memory, attention, and executive skills but used auditory stimuli. Interestingly, this auditory–cognitive training approach provided very large improvements in cognitive function, primarily driven by improvements in attention as measured by the Integrated Visual and Auditory Continuous Performance Test. Removing this large effect from the overall pooled effect meant that cognitive training was no longer significantly more effective than auditory training at improving overall cognition. Oba et al. (2013) trained participants using an adapted Visual Digit Span task to improve working memory and reported on-task improvement on the Visual Digit Span task posttraining. Henshaw and Ferguson (2013b) used the working memory platform Cogmed™ and showed statistically significant improvements in performance for trained working memory tasks (on-task). These cognitive training findings are supported by evidence from meta-analyses in healthy older adults (Lampit et al., 2014; Pronk et al., 2011) and in older adults with mild cognitive impairment (Hill et al., 2016) and Parkinson’s disease (Lawrence et al., 2017), which also demonstrate improved performance on on-task (trained) outcomes and off-task outcomes, but only when they are structurally similar to those trained during computer-delivered cognitive training. Older adults with impaired hearing may experience cognitive decline (Jayakody et al., 2017a; Lin et al., 2013), but the ageing brain can maintain neural plasticity (Hill, Kolanowski, & Gill, 2011) and its ability to strengthen and modify neuronal connections (i.e., synaptogenesis) leading to positive changes in response to training. Cognitive training provides a set of tasks that involve repeated use at increasing difficulty, which induces a stimulation-focussed improvement in domains trained during an intervention (Kim & Kim, 2014). Cognitive training interventions for adults with hearing loss are relatively novel, but results from this meta-analysis suggest some therapeutic potential for improving working memory and overall cognition.
Findings from this review suggest both auditory and cognitive training are effective for improving cognition in adults with hearing loss. By design, cognitive training is more targeted and provides a more intensive stimulation of cognitive abilities, whereas auditory training may improve cognition by training auditory perception that also involves the use of cognitive resources. We may therefore expect cognitive training to be more beneficial for improving cognition. As discussed, the large pooled effect of cognitive training in this review was primarily driven by effects reported by Anderson et al. (2013b) who used a training paradigm involving cognitive tasks and auditory stimuli. It is therefore possible that an integrated (cognitive/auditory and auditory) training program may be most beneficial for improving cognition in adults with hearing loss (Ferguson & Henshaw, 2015). It is important to note, however, that the auditory training program (LACE™) developed by Sweetow and Henderson Sabes (2006) adopts a similar structure by involving auditory tasks with a cognitive component. It is therefore somewhat difficult to delineate the classification of auditory training programs that involve cognition with cognitive training programs that involve auditory perception, and the pooled effects reported in this review should be interpreted with this caveat in mind.
There were insufficient studies to explore factors (e.g., intervention length, adherence to training) that may account for the large degree of heterogeneity within the overall effect of cognitive training on cognition. Furthermore, by combining all study outcome measures for a given cognitive domain for input into the meta-analysis, the benefits of training shown by individual study outcome measures may be lost. For example, Ferguson et al. (2014) showed auditory training-related improvements for divided attention that employed executive control processes, but not for single attention that does not. Removal of Oba et al.’s (2013) participants with cochlear implants or Henshaw and Ferguson’s (2013b) participants with hearing aids had no significant impact on the pooled effect, but removing Anderson et al.’s (2013b) large effect sizes reduced heterogeneity to nonsignificance and the effect to small (remaining significant). The large effects reported by Anderson et al. (2013b) may be the consequence of their integrated intervention (as noted earlier) combined with their longer training schedule of 40 hr (5 sessions × 8 weeks), compared with the other studies involving between 3.5 and 10 hr of training. Shorter and fewer training sessions have been argued to provide optimal conditions to elicit improvement following auditory training (Molloy, Moore, Sohoglu, & Amitay, 2012) and cognitive training (Lampit et al., 2014). Conversely, findings from this review suggest that a longer cognitive training intervention (several weekly 1-hr sessions over multiple months) may be more beneficial for improving cognitive function in adults with hearing loss. It is also important to note that Anderson et al. (2013b) supported large neuropsychological improvements in cognition with improvements in objective measures of neural timing, which provides evidence of neural plasticity in the ageing brain in response to training. There is, however, a limitation to this interpretation of the results. The subset of participants reported by the author’s other study (Anderson et al., 2013a) did not demonstrate improved cognition following the same training parameters, and this variability in results led to a decrease in certainty in the evidence for cognitive training.
The overall certainty of evidence in support for auditory training and cognitive training improving overall cognition was “low” and “very low,” respectively (Schünemann et al., 2017). Certainty in evidence was most frequently downgraded due to methodological bias within studies, variability between study designs and interventions, heterogeneity within pooled effect estimates, and the small number of published studies available for inclusion in this review. Nonetheless, three included studies were rigorous RCTs (Ferguson et al., 2014; Henshaw & Ferguson, 2013b; Saunders et al., 2016). We recommend future researchers follow these examples by conducting high-quality RCTs in accordance with the Consolidated Standards of Reporting Trials guidelines for nonpharmacological interventions (Schulz, Altman, & Moher, 2010) and have sample sizes that are sufficient to provide adequate statistical power for reliable interpretation of results.
Participant adherence to a home-based intervention with limited supervision is of paramount importance when determining the efficacy of a novel therapeutic technique. Among studies in this review, more than 80% of participants adhered to full training schedules, but most trials did not report factors that contributed to adherence (or nonadherence) during interventions. Participants are more likely to adhere to a home-based intervention if there is regular participant–investigator contact, they are intrinsically motivated and engaged in training activities, they believe cognitive function/intelligence is malleable, and when they report belief in the efficacy of the training program to improve their hearing ability or cognitive function (Ferguson & Henshaw, 2015; Henshaw, Mccormack, & Ferguson, 2015a; Jaeggi, Buschkuehl, Shah, & Jonides, 2014; Sweetow & Henderson Sabes, 2010). Although adherence was high among studies in this review, real-world evidence shows that less than 30% of patients complete auditory training when recommended by an audiologist (Sweetow & Henderson Sabes, 2010). Future studies need to report and explore factors that contribute to adherence to ensure home-based interventions are designed to maintain adherence to training schedules and consequently increase our understanding of the efficacy of auditory and cognitive training interventions.
There are several limitations to this review. Only nine studies met inclusion criteria, five auditory training and four cognitive training, and several individual domain pooled effects were supported only by one or two studies. There was, however, no significant heterogeneity within the overall effect for auditory training, providing initial confidence in the current estimate of auditory training improving cognition in adults with hearing loss. Sensitivity analyses also showed that the overall pooled effect for cognitive training improving cognition remained robust and statistically significant following removal of methodologically heterogeneous studies. With these considerations in mind, however, we recommend findings from this review to be regarded as preliminary evidence, and a follow-up meta-analysis should be conducted as more trials become available. This review also included repeated measures designs, reducing certainty in the evidence. Any future meta-analysis should attempt to include only well-designed RCTs to provide Class I evidence in support of (or to potentially refute) the therapeutic potential of auditory training and cognitive training for improving cognition in adults with hearing loss.
Recommendations for Future Research
Future studies should explore the potential of auditory training combined with cognitive training for improving cognition in adults with hearing loss. Work by Anderson et al. provides promising evidence in support of using an integrated cognitive training program (e.g., Brain Fitness) that requires the use of cognitive abilities and auditory perception to complete training activities (Anderson et al., 2013a, 2013b). With the increasing ageing population, clinical trials need to examine whether an integrated auditory–cognitive training paradigm has the potential to simultaneously improve or potentially halt neural degeneration associated with hearing loss and cognitive decline among older adults.
All auditory training studies, excluding one (Sweetow & Henderson Sabes, 2006), that met inclusion criteria for Henshaw and Ferguson’s (2013b) original review were excluded from this review for not including a measure of cognitive function. There is increasing evidence showing adults with better hearing demonstrate better cognitive function across all domains (Taljaard et al., 2016), and findings from this review suggest auditory and cognitive training may improve cognition in adults with hearing loss. Future studies need to include cognitive outcomes while consulting compendiums of neuropsychological tests for thorough descriptions and recommendations for the use of cognitive measures with older adults (Lezak, Howieson, & Loring, 2004; Strauss et al., 2006). More than half of the studies included in this review did not assess or report a measure of baseline cognitive status (e.g., Montreal Cognitive Assessment, Wechsler Adult Intelligence Scale battery). As part of normal ageing, older adults may experience mild cognitive decline which will impact their performance during auditory and cognitive training. Future studies need to include baseline measures of cognitive status to identify participants with or without mild cognitive impairment and whether to include or exclude participants following predefined selection criteria. It will also be useful to explore the potential of these interventions among older adults with hearing loss and with different subtypes (e.g., amnestic vs. nonamnestic) and varying degrees (e.g., mild to dementia) of cognitive decline. The beneficial effects of cognitive training may be artificially limited in older adults with normal cognitive function who experience a ceiling effect during training (i.e., no improvement beyond normal cognition), whereas individuals with cognitive deficits have the capacity to improve in response to training.
We also recommend including outcomes that assess real-world benefits and explicit examination of the long-term efficacy of auditory and cognitive training. More research is also needed to determine whether auditory and cognitive training have the potential to elicit a transfer (learning) effect which benefits older adults in their daily life. Many older adults with hearing loss and cognitive decline experience difficulties completing daily activities and are less likely to socialize (Behera et al., 2016; Mick, Kawachi, & Lin, 2014; Saito et al., 2010). Including measures of instrumental activities of daily living (Jekel et al., 2015), social isolation (Mick et al., 2014), and frailty (Morris, Howard, & Steel, 2016) will determine if these home-based interventions provide practical improvement in the daily life of older adults with hearing loss. Although not a focus of this review, only three studies reported longer term follow-up data (Henshaw & Ferguson, 2013b; Oba et al., 2013; Saunders et al., 2016). Future studies need to include follow-up assessments (e.g., 12 months) to determine the long-term efficacy of auditory and cognitive training for cognition.
Conclusion
The current study is the first systematic review and meta-analysis to provide pooled effect estimates of auditory training and cognitive training for cognition in adults with hearing loss. Nine studies met inclusion criteria, and these preliminary results suggest that home-based auditory training and cognitive training may improve cognition. More high-quality RCTs with long-term follow-up assessments are needed to determine whether auditory, cognitive, or a combined auditory–cognitive intervention is most efficacious for improving cognitive function in adults with hearing loss.
Supplemental Material
Supplemental material for Auditory and Cognitive Training for Cognition in Adults With Hearing Loss: A Systematic Review and Meta-Analysis
Supplemental material for Auditory and Cognitive Training for Cognition in Adults With Hearing Loss: A Systematic Review and Meta-Analysis by Blake J. Lawrence, Dona M. P. Jayakody, Helen Henshaw, Melanie A. Ferguson, Robert H. Eikelboom, Andrea M. Loftus and Peter L. Friedland in Trends in Hearing
Footnotes
Author Contributions
B. J. L. was responsible for conception, design, and execution of the project; conducted article screening, data extraction, bias assessment, and statistical analysis; and wrote the first draft of the article. D. M. P. J. assisted with article screening and provided expert review and critique of important intellectual content. H. H., M. A. F., R. H. E., A. M. L., and P. L. F. provided expert review and critique of important intellectual content.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: B. J. L., D. M. P. J., R. H. E., and P. L. F. are supported by the Ear Science Institute Australia. The contribution by A. M. L. was supported by Curtin University, and the contributions by H. H. and M. A. F. were supported by the National Institute for Health Research. The views expressed are those of the authors and not necessarily those of the Ear Science Institute Australia, Curtin University, the National Health Service, the National Institute for Health Research, or the Department of Health and Social Care.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.