
Abstract
Empathy is an important competence for communication professionals. This article investigates two aspects of empathy in an educational setting: the validity of self versus other assessments and the manifestation of empathy in communicative behaviors. Communication students were given a mediating role in discussions with two clients and their empathy was measured using self-ratings and client assessments. Videos of highest- and lowest-rated students were analyzed to identify empathy-related behaviors. No correlation was found between self-rated empathy and clients’ assessments. Several verbal and nonverbal behaviors corresponded to empathy: body language, an other-orientation in asking questions, paraphrasing, and a solution orientation.
Keywords
Empathy is considered to be a critical competence for communication professionals (Fuller et al., 2018, 2021). Although it may not be mentioned in listings of specific communication skills taught in academic programs (e.g., Clokie & Fourie, 2016; Ortiz et al., 2016), it underlies the success of many oral and written communication activities. When Coffelt et al. (2019) asked employers about their views on relevant communication skills, their responses boiled down to three generic core competencies: relating, translating, and executing. Both relating (building and maintaining relationships) and translating (listening, bridging, and adapting to audiences) depend strongly on communication professionals’ empathy.
Support for the relevance of empathy in communication practice can be easily found. Analyzing reader feedback on professional documents, De Jong and Lentz (2007) showed that ineffective communication can often be attributed to a lack of empathy. Conversely, Edwards et al. (2016) showed that perspective-taking skills have positive effects on communication satisfaction and the use of integrative strategies, while reducing misunderstandings. Johnson-Eilola and Selber (2013) argued that modern technical communicators should profile themselves as users’ advocates, a role that fully depends on their willingness and ability to see technical products from the perspectives of user groups. Empathy may be even more salient in face-to-face or mediated interactions. Research drew attention to the importance of empathy in customer interactions such as call-center phone calls (C. M. Clark et al., 2013), in rhetorically and emotionally complex situations such as e-complaint refusals (Decock et al., 2020), apologies (Bisel & Messersmith, 2012), and “bad news” conversations (G. L. Bradley & Campbell, 2014), in fostering a healthy workplace atmosphere (Mayfield & Mayfield, 2015; Yue et al., 2020), and in cross-cultural and intercultural encounters (Swartz et al., 2019).
Despite its relevance for the communication profession, empathy has not yet been thoroughly scrutinized in the academic communication literature. This stands in contrast with the health care literature (cf. Howick et al., 2017; Schrooten & De Jong, 2017), in which empathy is generally treated as a crucial, challenging, and multifaceted competence (Pedersen, 2009). Caregivers’ empathy has many personal and situational antecedents, but research suggests that it can be trained and improved (cf. Batt-Rawden et al., 2013; Kataoka et al., 2019; Stepien & Baernstein, 2006). Still, research has also shown that students’ empathy often declines during regular medical programs (Hojat et al., 2009; Nunes et al., 2011), suggesting that empathy, when not given proper attention, may easily be suppressed by other educational or professional demands. In addition, health care researchers proposed several approaches for measuring caregivers’ empathy, including self and other reports using questionnaires (Hojat & LaNoue, 2014; Mercer et al., 2004) and observation (Bylund & Makoul, 2005).
Insights from the health care context cannot be straightforwardly translated to the context of professional communication but may still be used to inspire communication research on empathy. In this article, we analyze how empathy manifests itself in professional communication education in the form of students’ self-ratings and clients’ assessments. We investigated whether students’ own estimations of their empathy competence are in line with independent judgments by others. In addition, we investigated to what extent overall empathy judgments can be attributed to specific communicative behaviors. We conducted our research in a specific higher education setting in which individual students were given a facilitating and mediating role in a discussion with two clients. Our two research questions were as follows:
Research question 1: What is the relationship between communication students’ self-rated empathy competence and independent empathy judgments by clients?
Research question 2: Which behaviors are perceived to signal empathy competence?
Theoretical Background
Conceptualizing Empathy
Considering the many different definitions of empathy (Hall & Schwartz, 2019), we defined empathy as the willingness and ability to understand other persons’ perspectives, beliefs, and emotions and to confirm and express this understanding in communicative behavior. A distinction can be made between cognitive empathy (understanding others’ internal state and perspectives), affective empathy (imagining others’ emotions), and behavioral empathy (expressing cognitive and affective empathy) (M. Clark et al., 2019). Empathy thus involves a mental disposition as well as a capability to express it. As such, it relates to the concept of a you-attitude (Rodman, 2001), which also puts other persons’ feelings and viewpoints first in communicative behavior. Gordon (1988) spoke of creating a state wherein the “other” feels understood, as opposed to a state of feeling defensive.
Various studies elaborated on the listening aspect of empathy. In a scenario-based study, Haas and Arnold (1995) showed that listening is a crucial communication competence in interpersonal interactions. Ramos Salazar (2017) distinguished between content listening (focusing on facts and figures) and people listening (focusing on feelings and emotions), arguing that only the latter relates to compassion. Roebuck et al. (2015) investigated four types of listening behaviors of managers and nonmanagers—empathetic listening, distracted listening, judgment rushing, and conclusion jumping—claiming that the latter three types reflect a view on listening as a waste of time, with many potentially negative consequences. Golen (1990) identified six listening barriers, which can be seen as immediate threats to empathic behavior: being lazy, closed-minded, opiniated, insincere, bored, and inattentive.
Other studies elaborated on the expression of empathy. In a series of studies on the effects of motivating language, Mayfield and Mayfield showed that empathetic language—expressing appreciation and showing genuine interest—is an important aspect of leadership communication, with positive effects on employees’ work attendance (2009), decision making (2015), and perceptions of the creative environment (2017). Yue et al. (2020) also found positive effects on organizational identification, mediated by a perceived positive emotional culture.
Based on interviews with seasoned communication professionals, Fuller et al. (2021) developed an empathy framework, underlining its complexity and multifaceted nature. At the core of the competence, many specific types of knowledge, attitudes, and skills can be found. The actual empathic behavior, however, is also affected by auxiliary factors such as personal characteristics, characteristics of the communication partner(s), and organizational context. Empathy manifests itself in five types of behavior:
- Appraising context: Forming an understanding of the situation of others.
- Facilitating environment: Creating a setting in which others can safely express their thoughts and feelings.
- Collecting data: Being keen on verbal and nonverbal cues that express engagement, concerns, emotions, etc.
- Interpreting signals: Making sense of others’ cues, without bias or prior assumptions.
- Clarifying understanding: Expressing understanding and rapport.
In all, empathy appears to be a comprehensive competence, comprising both an internal state—the knowledge, attitude, and skills needed to empathize with others—and an ability to express this internal state to others. In interactions, a reciprocal relationship may be assumed between the internal state and the expression of empathy: Feeling empathy can be helpful for expressing it, while expressing empathy contributes to an atmosphere in which the other is more willing to disclose thoughts and feelings.
Measuring Empathy
Most studies on professional empathy rely on people’s self-assessment. In their review of earlier research, Hall and Schwartz (2019) found that 80% of the studies used self-reports; other, less current, approaches are observation (Bylund & Makoul, 2005), ratings by others (e.g., Schrooten & De Jong, 2017), physiological measurements, and tests.
Despite their popularity, there are various potential flaws associated with people’s self-reports on empathy. First, self-assessments may be biased by social desirability. People may be inclined to give themselves inflated scores just because they think that being empathic is to be preferred. Second, it might be hard for people to assess their own level of empathy, which depends on critical self-reflection as well as knowledge of the complexities of being empathic. In line with the Dunning-Kruger effect (Dunning, 2011), it is imaginable that a U-shaped or inverted curve emerges, with people who do not care about empathy overestimating their level of empathy and people who care a lot about empathy underestimating it. Third, self-assessments are limited to empathy as a mental disposition and, at best, intentions to express it, but cannot incorporate how other people experience someone’s level of empathy. In a health care setting, Silvester et al. (2007), for instance, found that patients and caregivers did not always agree on which types of behaviors contributed to experiencing empathy. And fourth, self-assessments are often generic, excluding the influence of contextual factors in specific situations. The latter two objections refer to an implicit assumption of self-reports: they conceptualize empathy as a personal quality instead of a relational construct (Sulzer et al., 2016).
In their reviews of research comparing self-ratings of empathy with ratings by others, Davis et al. (2006) and Sanchez et al. (2019) conclude that the findings thus far are inconsistent but generally unfavorable for self-reports. Investigating the factorial validity of an adapted version of the Jefferson Scale of Empathy to measure law students’ levels of empathy, Spivak et al. (2018) showed that caution is needed when applying insights from health care research to other contexts. In an organizational communication context, Park and Raile (2010) found that employees’ self-ratings of their perspective-taking abilities did not correlate with those of colleagues and with colleagues’ communication satisfaction. Discrepancies between employees’ own and colleagues’ ratings of their perspective-taking abilities were negatively related to colleagues’ communication satisfaction, suggesting that self-reflection on empathy must be a part of the overall empathy concept. In a health care context, Schrooten and De Jong (2017) reported similar findings.
In our study, we further explore the validity of self-rated empathy, by comparing students’ own scores not only with the scores given by their interaction partners, but also with those resulting from independent examinations of their observable behaviors.
Empathy and Communicative Behaviors
Although it seems unrealistic to capture all aspects of expressed empathy in intersubjectively observable behaviors, several studies suggest that manifestations of empathy may be observed by identifying verbal and nonverbal behaviors demonstrating rapport and understanding. In the context of medical consults, for instance, Bylund and Makoul (2005) distinguished “empathic opportunities”—moments when patients explicitly or implicitly refer to emotional, personal, or family concerns. Caregivers’ responses to such opportunities can be rated on a scale ranging from denying (low empathy) to sharing feelings or experience (high empathy). This approach seems especially useful for the specialized and scripted genre of doctor-patient consults, in which empathic opportunities might be relatively easy to identify. Still, this approach could also be useful in grading empathy in communication interactions.
In a variety of vocational contexts outside professional communication, specific behaviors have been identified that might enact empathic communication. Håkansson and Montgomery (2003) posited that expressing empathy may involve showing understanding and concern, dealing with emotions, and exploring or emphasizing similarity. This relates to specific communicative behaviors like verbal articulations of understanding, questioning tactics to reveal underlying emotions, and the use of specific gestures and other nonverbal cues or mimicry (Barger & Grandey, 2006; Bodie, 2011; Chu et al., 2014; M. Clark et al., 2019; Dowell & Berman, 2013; Shapiro & Gottman, 2004). It is our purpose in this article to further explore specific empathy-expressing behaviors in professional communication contexts. However, it must be stressed that the relation between communicative behaviors and perceived empathy is not necessarily straightforward. The effects of specific communicative behaviors might depend on their dosage and specific execution. For instance, sharing feelings or experiences may come across as empathic, but when it is done too much or in the wrong way it could also have the opposite effect.
Method
We investigated empathy in an educational setting with advanced communication students. The students individually played a facilitating and mediating role in a discussion with two clients (played by professional actors). Prior to the interactions, students completed a self-assessment questionnaire. Immediately after their interactions, their empathy was assessed by both clients. To answer the first research question, we compared the empathy scores of students and clients. To answer the second research question, we inductively analyzed and compared a selection of the highest- and lowest-ranking interactions, in search of specific behaviors that may have contributed to or detracted from the clients’ empathy perceptions. This study was approved by the Ethics Committee of the University of Twente. Below, we will give a more detailed overview of the research.
Data Collection
We collected the data for our study during a program-required two-day workshop on intercultural communication, scheduled in the fourth (final) year of a Bachelor of Communication program. A few days before the workshop, students were asked to complete a self-assessment empathy questionnaire online. The questionnaire was introduced as part of ongoing research, aiming at “get[ting] an idea of how you assess your own interpersonal skills at the end of your fourth year.” Students were offered an opt in or opt out, as required by the school’s ethical standards. The first day of the workshop consisted of theoretical and practical training on intercultural communication without specific attention to empathy. On the second day, students were randomly assigned to participate in a professional communication simulation using professional actors as clients. Two different cases were used in which the students had to play a facilitating and mediating role in a discussion between two clients who differed in national backgrounds, interests, and perspectives.
Students were given basic case information before the interaction. They were instructed to respond to the clients as if the situation were a real professional event. They received feedback about their performance after the sessions. The clients were portrayed by four trained role-play actors, who were assigned to either of the two cases. The actors had contributed to earlier versions of the workshop and felt comfortable with the case roles and the educational context. All actors were given detailed background information about their roles and were briefed about how to use the empathy-assessment questionnaire.
The interactions took place in a university classroom. Students entered the room in groups of four or five; the two clients were already seated. The entire session lasted 45-60 minutes, with the facilitating and mediating role alternating between students. Every student was responsible for 10 minutes of a session. Immediately after these 10 minutes, both clients independently rated their experiences with the student on paper, which on average took 2-4 minutes. Once the rating was complete, another student would resume. At the end of the session, the clients had a 30-60-minute break. They were instructed not to talk about the session with each other or with students during their breaks. Their assessment forms were collected by the first researcher at the end of the day. The interactions were video recorded with permission of all students and clients.
Participants
The participants were bachelor-level students in their final semester of a professional communication program. We focused on students from one particular study phase in order to minimize the influence of differences in general communication knowledge, skills, and experience. We chose for fourth-year students, because they were as close as possible to becoming communication practitioners and could be expected to have an end-of-program level of empathy. The participants were just a few months away from entering the professional field, had all followed the same educational program for four years, and had completed a required 6-month internship, gaining professional work experience. Our study was conducted just before the start of their individual graduation assignments. Of the 87 students enrolled in the course, 80 fully completed the self-assessment questionnaire and gave their consent to participate; 7 opted out. All 80 participants were included in our analysis for the first research question (comparing self-assessments and client assessments of empathy). Because of technical failure of a microphone during the recordings, six of the 80 videos were deemed incomplete for third party evaluation, resulting in 74 assessable video recordings that were considered for the second research question (comparing participants with high and low empathy scores in search of empathy-supporting communicative behaviors).
The participants ranged in age between 19 and 31 years (mean age = 22.5, SD = 2.15); 74% of the participants identified themselves as female and 26% as male. Participants’ nationalities differed: Most were Dutch or German (both 33%), followed by East European (16%), Asian (9%), North American (5%), Middle American (4%), and South European (1%). Participants were equitably divided between the two case groups based on age, gender, and nationality.
Instruments
As this study assessed empathy from two viewpoints, two instruments were used to assess the participants’ empathy: a self-assessment scale and a client scale. As we are unaware of measures specifically created for processional communication contexts, we chose and gently amended already validated scales widely used in the medical field, which seemed to connect well to our research goals and the interactions under study.
For participants’ self-assessment of empathy, we used the Questionnaire of Cognitive and Affective Empathy (QCAE) (Reniers et al., 2011). This is a 31-item questionnaire with 4-point Likert scales (1 = strongly disagree, 4 = strongly agree) measuring five subdimensions: perspective taking (10 items; e.g., “I am good at predicting what someone will do”), online simulation (9 items; e.g., “I always try to consider the other fellow’s feelings before I do something”), emotion contagion (4 items; e.g., “People I am with have a strong influence on my mood”), proximal responsivity (4 items; e.g., “I often get emotionally involved with my friends” problems), and peripheral responsivity (4 items; e.g., “I often get deeply involved with the feelings of a character in a film, play or novel”). The first two subdimensions are meant to measure cognitive empathy, and the last three measures focus on affective empathy. In our study, we used three empathy measures: cognitive empathy (19 items, Cronbach’s alpha = .79), affective empathy (12 items, Cronbach’s alpha = .72), and overall empathy (31 items, Cronbach’s alpha = .77).
For clients’ empathy assessments, we used a condensed scale based on the Consultation and Relational Empathy (CARE) instrument (Mercer et al., 2004). Although the CARE instrument was developed for health care settings, most items apply to the communicative setting of our study. Our modifications were to change the text “doctor” to “student” and omitted questions that were better suited to a consultation in a health care setting (4, 8, 9, and 10). Clients had to assess how good a participant was at (1) making them feel at ease; (2) listening to them; (3) asking questions to clarify their story; (4) understanding their perspective; (5) reading their mood, emotions, and nonverbal cues; and (6) showing concern about them. All items were measured on 5-point scales (1 = poor, 5 = excellent). We assessed the scale reliability separately for different cases and clients. The Cronbach’s alphas ranged from .92 to .95.
Data Analysis
To answer the first research question, we computed correlations between participants’ self-rated empathy scores and the scores provided by the two clients. We started with participants’ overall empathy self-assessment, and then zoomed in on the cognitive and affective empathy subdimensions. For clients’ empathy assessments, we computed composite client scores for all participants. As the clients represented two different positions in the conversations, we assumed that their assessments might differ. The composite scores thus were the average of two assessments from different angles. When combining the two client scores, we took into account that the four clients might differ in their scoring styles. We therefore standardized the clients’ scores into Z-scores and averaged these into single composite scores.
To answer the second research question, we selected 16 video recordings—eight with the lowest and eight with the highest mean empathy scores given by the two clients. Because of problems with a microphone, five of the originally selected videos had to be replaced. The first author tracked the talking time of the participants in all 16 sessions. In addition, two independent coders were hired to review and code the video-taped interactions, without being informed about the participants’ empathy scores. Prior to their task, the coders were trained in using the coding scheme to ensure similar interpretation of concepts.
The coding scheme consisted of an overall measure of the participants’ observed empathy (on a 4-point scale; 1 = poor, 4 = excellent) and a scoring sheet aimed at identifying specific communicative behaviors. The overall measure was used to verify the clients’ composite score per participant. The two coders reached a high degree of reliability in their overall measures (Cronbach’s alpha = .92). The scoring sheet focused on specific verbal cues (question form, paraphrasing, solution orientation, judgment, and emotion identification) as well as nonverbal behaviors (eye contact, posture, and facial expressions), which are all assumed to be measurable components of empathy in the literature (Bodie, 2011; Chu et al., 2014, Clark et al., 2019; Dowell & Berman, 2013; Shapiro & Gottman, 2004).
Results
Comparing Self-Assessments and Client Scores
We used correlation analysis to answer the first research question, about the relationship between students’ self-ratings of their empathy and the experience of the two clients. No significant correlation was found between participants’ self-assessment of their overall empathy competence and the clients’ composite scores (r = –.06, p = .583). Similar results were found regarding participants’ self-assessments of cognitive empathy (r = –.10, p = .362) and affective empathy (r = .02, p = .855). These findings suggest that participants’ own estimations of their level of empathy had no predictive value for their performance in the two clients’ perspectives. To give more detailed insights, Figure 1 provides a scatterplot of participants’ self-assessments of their overall empathy competence and the clients’ composite scores. Although there were some remarkable cases of participants estimating their level of empathy too high or too low, our data do not support general assumptions of a U-shaped or inverted curve.
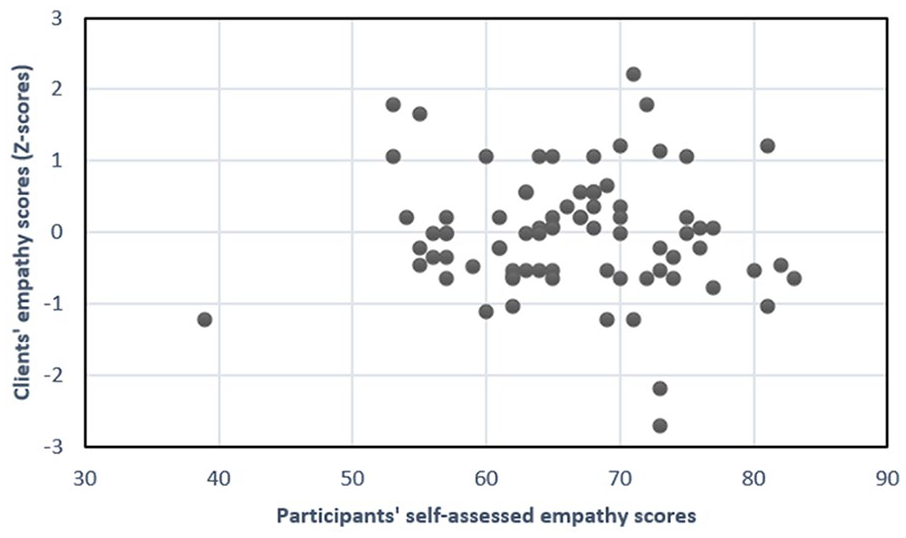
Scatterplot of Participants’ Self-Assessed Empathy and Clients’ Composite Empathy Scores.
Relating Empathy to Specific Communicative Behaviors
The second research question, examining the relation between empathy as experienced by the clients and participants’ specific communicative behaviors, was investigated with an in-depth analysis of a subset of videos of participants’ interactions. A detailed comparison was made of the videos of eight participants with the highest empathy scores and those of eight participants with the lowest empathy scores, according to the clients. Because of problems with one of the microphones, five of the originally selected participants had to be replaced with others. Table 1 gives an overview of the participants included in this analysis, with their empathy score given by the clients, their empathy score given by the independent observers, and the percentage of talking time during their session.
Overview of Participants Included in the Analysis of Communicative Behaviors.
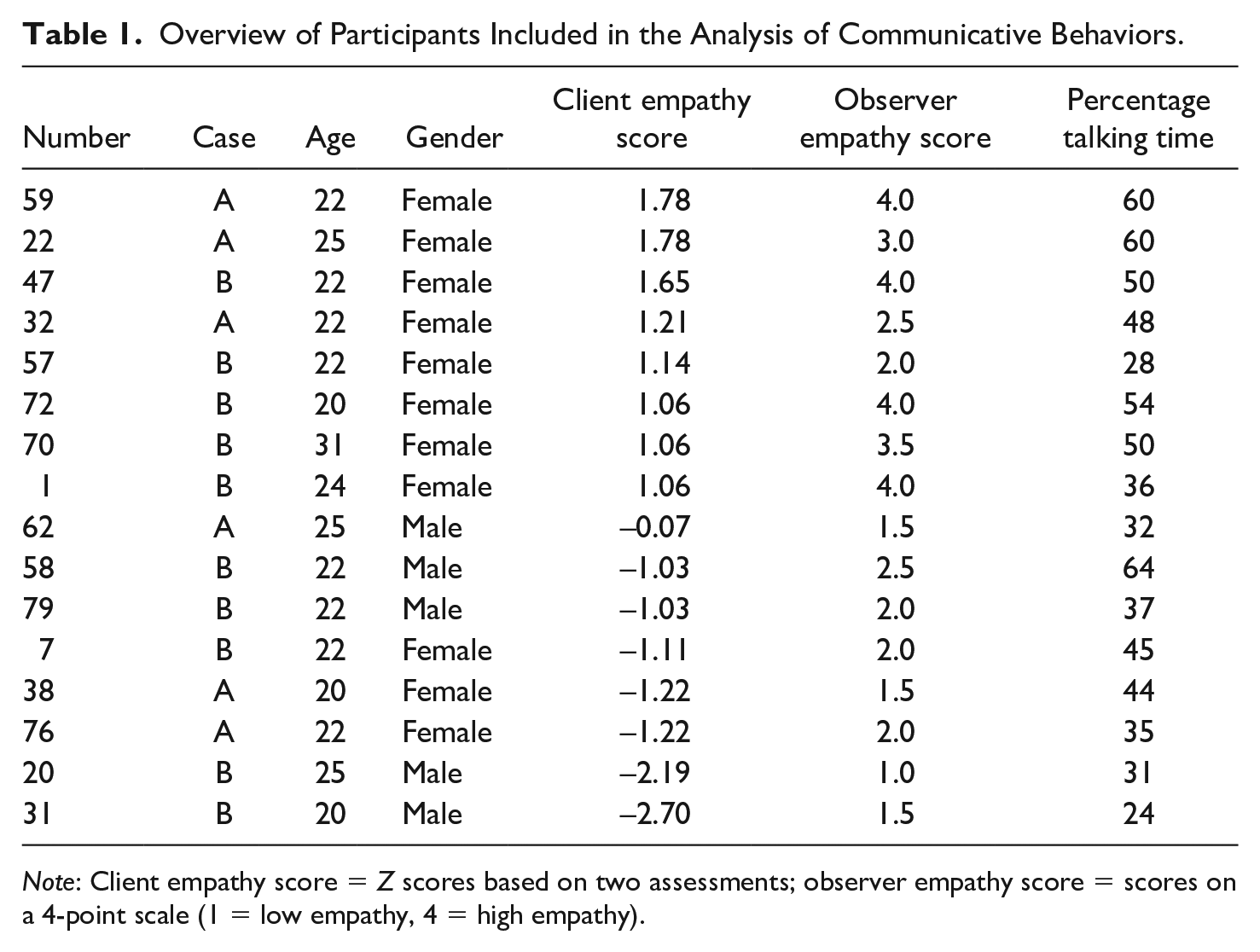
Note: Client empathy score = Z scores based on two assessments; observer empathy score = scores on a 4-point scale (1 = low empathy, 4 = high empathy).
The two independent observers confirmed the overall empathy assessments by the two clients, with a high correlation (r = .82, p < .001) and a significant difference in observer scores between participants in the high-empathy (M = 33.8) and low-empathy (M = 17.5) groups (Mann-Whitney U test, U = 3.00, p < .005). Like the clients’ scores, the observers’ scores did not correlate with participants’ self-assessments (r = –.22, p = .422). No significant difference was found regarding the percentage of talking time. Participants in the high-empathy group tended to talk more than participants in the low-empathy group (48% vs. 39% on average), but this difference was not significant (Mann-Whitney U test, U = 17.00, p = .13).
Below, our qualitative comparisons will be described. References to individual videos are indicated with participant number (P + number).
Eye contact
Although the literature suggests that the amount of eye contact influences people’s empathy perceptions (Dowell & Berman, 2013), we did not find a relationship between eye contact and perceived empathy in this study. Observations did not indicate noteworthy variations between the participants in the type or duration of eye contact with clients. All participants generally maintained eye contact most of the time, generally with the client who was speaking. In few cases did a participant look away while thinking or speaking, but this did not differ between the high-empathy and the low-empathy groups. Only in one case did observers note a significant variance in eye contact, stating that the participant’s face rarely moved and that he had an almost “Spock-like” gaze (P31). But overall, no differences could be found.
Posture, gestures, and body movement
There were some differences in body movements between participants from the high-empathy and the low-empathy group. Participants with low empathy scores often touched their face or fidgeted with an object (pen, fingernails) and did not often mirror the nonverbal expressions of their clients. They were often noted as sitting either overly formally and stiff or overly informally and nonchalant. Their hand movements were often noted as being “fast and choppy” (P38), using pointed fingers or even making “stop” hand signals (P20) or they rarely used their hands at all (P31). These observations contrasted with those of participants with high empathy scores, who were characterized as sitting relaxed and calmly: they more likely nodded their heads when listening to a speaker, often made synchronous hand movements, with open palmed gestures, and kept their hands still when not speaking.
Verbal behaviors
Although there were no significant differences in percentages of talking time, the talking time was spent in noticeably different ways in the high-empathy versus low-empathy groups. Participants with high empathy scores were more inclined to summarize, reframe, and formulate questions that honored both clients’ perspectives. Participants with low empathy scores focused more strongly on strictly guiding the process, sharing information, and offering advice or judgments.
Question form and intention
Participants in both groups used open and closed questions during the interactions. There was not a noticeable difference in the amount or type of questions between the groups. However, the content requested with the questions appeared to be quite different. Participants with high empathy scores asked for elaboration, for the clients’ opinions, what their needs were, and how they came to feel the way they did. In contrast, students with low empathy scores often asked the clients to provide more data or facts, to confirm opinions and judgments, or to build evidence for process solutions.
Paraphrasing
Attempts to paraphrase during the interactions, to demonstrate an understanding of the clients’ perspective, happened in many forms. The way in which information was paraphrased differed between the two groups. Participants with low empathy scores paraphrased by either repeating verbatim what was said or summarizing facts and actions. Some of the participants with high empathy scores paraphrased and additionally asked for confirmation if their understanding was correct. They also paraphrased more often from the first person, for example: “I heard you say that . . . ” (P22), “Before we move forward, I want to take a moment to see if I understand correctly . . . ” (P70), or “So I think what I am hearing from you guys . . . ” (P72). Participants with high empathy scores often used paraphrasing to emphasize aspects of the case where clients had shared goals (P59) or to indicate similarities in perspective (P1). These strategies were absent among the participants with low empathy scores.
Solution orientation
Participants with high empathy scores often presented their solutions as questions, used “we” phrases, or combined solutions with a suggestion or possibility, for example: “Maybe we can help . . . ” (P72) or “Maybe we can think about” (P70). Participants with low empathy scores, on the other hand, used more directive “I” phrases, for example: “I suggest that you . . . ” (P79) or “I think you should . . . ” (P76). There was also a difference in the participants’ sense of responsibility. Participants with high empathy scores made statements reflecting an inclusive responsibility, such as “We’re looking for an easy fix that doesn’t exist, but we will find a solution (P1); participants with low empathy scores placed themselves outside of responsibility, for example: “I suggest you find a different solution to that” (P79).
Discussion
Main Findings and Implications
In this mixed-method study, we investigated advanced communication students’ empathy competence in an educational setting. Two research questions were addressed. First, we investigated the congruence between students’ self-assessments of their empathy competence and the assessments by others (the clients involved in the discussions and, in a subsample, two independent observers). Our results suggest that students are not able to estimate their level of empathy as experienced by others. This finding casts further doubt on the validity of self-assessments of empathy, corroborating earlier research in medical settings (Davis et al., 2006; Sanchez et al., 2019; Silvester et al., 2007; Sulzer et al., 2016).
The difference between self and other assessments may be partly ascribed to the role of personal bias. Earlier theories already pointed out that people have a tendency to overestimate their personal abilities and virtues. For instance, according to the third-person effect (Corbu et al., 2020; Davison, 1983), people expect effects of media or fake news to be larger on others than on themselves; in attribution theory, the notion of self-serving bias suggests that people tend to attribute positive events to themselves and negative events to circumstances (G. W. Bradley, 1978; Zhang et al., 2018). In line with such forms of bias, it seems plausible that students might overestimate their level of empathy.
However, there were also students who seemed to underestimate their level of empathy. Three other factors might lay a role here. The first involves students’ conceptualization of empathy. Although we did not find overall evidence for a U-shaped or inverted relation between self-assessment and performance, which could indicate a Dunning-Kruger effect (Dunning, 2011) in the area of empathy, it is still imaginable that for individual students a different understanding of showing empathy affected their answers to the self-assessment questions, with low-empathy students conceptualizing it as a relatively limited and easy activity and high-empathy students realizing the complexity and the comprehensive nature of empathizing. The second involves the relation between empathy as an internal state and empathy as behavior. Self-assessment questionnaires focus predominantly on people’s willingness and perceived ability to empathize with others, without the behavioral aspect of showing empathy. Assessments by others must rely on the way empathy is shown through the use of verbal and nonverbal behaviors. Discrepancies between the two might reflect differences in skills to show empathy during interactions. Schrooten and De Jong (2017) drew attention to these two perspectives on empathy: (1) behavior first: via behavioral tips and tricks that may not reflect empathy as a disposition (e.g., Bonvicini et al., 2009; Bylund & Makoul, 2005; Coulehan et al., 2001; Harres, 1998), and (2) disposition first: via dispositional empathy (involving knowledge, attitude, and skills) that may not always lead to the expression of empathy in behaviors. The third factor involves the distinction between empathy as a more or less generic and personal disposition and empathy as a relational construct (Sulzer et al., 2016). Self-reported questionnaires focus on empathy as personal quality, whereas assessments by clients and observers reflect the way empathy manifests itself in the interactions between student and clients.
Discussions about the validity of self-assessments of empathy therefore should move from straightforwardly questioning their validity to acknowledging their limitations (as well as the limitations of other types of assessments) and evaluating how combinations of self and other assessments can contribute to an optimal diagnosis of students’ empathy competencies.
The discrepancies between students’ own empathy scores and the observations by clients and observers call for a comprehensive approach to teaching empathy in communication programs, encompassing and connecting the disposition-first and behavior-first perspectives. Students must be aware of the importance and the breadth of empathy, develop a willingness to empathize in professional encounters, and hone their ability to listen and “read” the views, understandings, interests, concerns, and feelings of others. They must also be able to reflect on their own communicative behavior and the way it may affect the impression they make on others and others’ willingness to disclose or cooperate. Fuller et al.’s (2021) framework may be a good starting point for developing empathy education. In addition, being aware of specific dos and don’ts in verbal and nonverbal behaviors will further facilitate students’ ability to express their empathy in professional interactions.
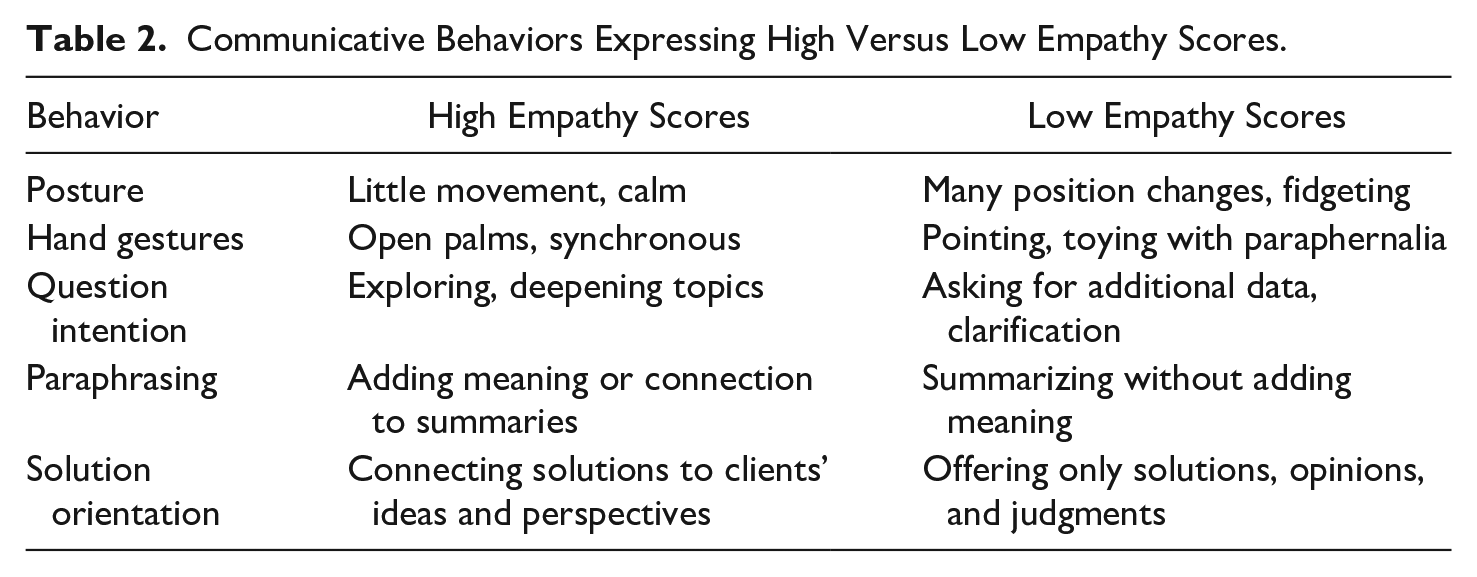
This brings us to the second research question, focusing on communicative behaviors that differentiate between students with high and low empathy scores. By zooming in on specific verbal and nonverbal behaviors, we developed a tentative listing of empathy-related behaviors that can be trained in communication programs. Table 2 gives an overview of these behaviors. Nonverbal behaviors seemed to be largely unconscious, requiring thorough personal training. In various disciplines, general frameworks are available for the training of nonverbal communication skills, both in face-to-face encounters (Hellmann et al., 2020; Lorié et al, 2017; Peterson, 2005) and in online communication (Darics, 2020; Sharma & Vyas, 2022). Differences in verbal behaviors generally went beyond the presence or absence of the generic categories of asking open questions, paraphrasing, and working toward solutions. Instead, differences were found in the way students executed them. Showing genuine interest, building rapport, expressing uncertainty, and maintaining a dialogue appeared to be the distinctive features.
Communicative Behaviors Expressing High Versus Low Empathy Scores.
Limitations and Suggestions for Future Research
The study reported in this article is a first attempt to make sense of empathy in the educational practice of academic communication programs. Although empathy appears to be a central competence for communication professionals, the research attention to teaching empathy to communication students is as yet very limited. Given the current state the art, we did not have empathy scales at our disposal that are validated for communication contexts. Future research should work on developing and validating self and other assessment scales for measuring empathy.
Another limitation that should be kept in mind is the very specific context in which data were gathered. The students in our study were placed in a facilitating and mediating role between two clients. Their individual sessions lasted about 10 minutes. Although our sessions appeared to differentiate in students’ empathy level, it is imaginable that different contexts and longer individual session would lead to somewhat different results. Other context could involve using cases with less complexity, for instance focusing on the interaction with just one conversation partner, or could extend to written (cf. De Jong & Lentz, 2007) or online (Darics, 2020; Sharma & Vyas, 2022) communication. Future research could further investigate how empathy-related competencies manifest themselves in various contexts.
Another interesting alley for future research would further zoom in on the relation between students’ self-assessed empathy and their empathy performance. In our study, we only measured students’ general self-assessments of empathy. In follow-up research, it would be interesting to see how such general self-assessments relate to students’ own evaluations of their performance during the interactions and to compare students’ own evaluations to the client assessments. Instead of solely focusing on last-year students, future research might also compare the development of (self- and other-assessed) empathy over time in communication programs. Furthermore, future research could focus on a refinement, extension, and quantitative assessment of the empathy-related behaviors identified in this study, and on the separate and combined effects of disposition-first and behavior-first empathy education in communication programs.
Pedagogical Implications
Throughout our research, it has been challenging to find indications that empathy competence receives much attention in professional communication programs. With this study, we hope that educators make a step toward designing curricula to include honing and measuring the development of empathy competence. Communication curricula should focus more strongly on the systematic development of empathy competence among students. This involves knowledge about the importance of empathy in various communicative settings as well as the development of attitudes and training of skills. Our experiences in this study show that working with professional actors who are specifically trained to play certain roles and to assess students’ performance can work well in academic programs. Other options include role-reversal, discourse analysis, and the use of narratives. For students’ self-assessments and other-assessments, the two scales used in this study may be a good starting point.
Conclusion
In contrast to the context of medical programs, the attention to empathy in the academic literature on communication programs is still very limited. Because empathy must be considered as important to communication professionals as it is to health care professionals, we described a first attempt to investigate empathy among communication students. Our findings suggest that self and other assessments of empathy must be seen as different and possibly complementary measures. Furthermore, we showed that several verbal and nonverbal communicative behaviors may impede or enhance the empathy perceptions others have.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was made possible with the financial support of the Netherlands Organization for Scientific Research, Doctoral Grant for Teachers, under Grant #023.005.094.