
Abstract
Background:
Bariatric surgery (BS) is an increasingly utilized intervention for the treatment of obesity. However, BS is also associated with postoperative nutritional deficiencies that may affect healing rates after orthopaedic procedures.
Purpose:
To compare failure rates and patient-reported outcomes after arthroscopic rotator cuff repair (RCR) between patients with and without a history of BS.
Study Design:
Cohort study; Level of evidence: 3.
Methods:
Patients in a single institution with a history of BS who underwent arthroscopic RCR for full-thickness supraspinatus tears were identified. These patients were matched in a 1:3 ratio by age, sex, and body mass index to patients without a history of BS who underwent arthroscopic RCR. The minimum follow-up was 24 months. The primary outcome was surgical failure. Secondary outcomes assessed included the numeric rating scale (NRS) score for pain, Single Assessment Numeric Evaluation (SANE) score, American Shoulder and Elbow Surgeons (ASES) Shoulder Score, need for manipulation under anesthesia (MUA) or arthroscopic lysis of adhesions (LOA), infection requiring reoperation, and conversion to reverse total shoulder arthroplasty (rTSA).
Results:
A total of 34 arthroscopic patients with a history of BS who underwent RCR were matched to 102 patients without BS. The BS group had significantly higher overall failure rates (20.6% vs 6.9%; P = .044) than patients without BS. The BS group had significantly higher postoperative NRS pain scores (3.9 vs 1.3; P < .001), lower SANE scores (77.7 vs 87.7; P = .041), and lower ASES scores (72.6 vs 90.4; P < .001) at the final follow-up. Rates of revision RCR, reoperation for MUA or LOA, and conversion to rTSA were not statistically significantly different (P > .050 for all). No postoperative infections were reported.
Conclusion:
A history of BS is associated with increased failure rates, worse postoperative pain, and worse patient-reported outcomes after arthroscopic RCR. Patients with a history of BS and those considering BS before arthroscopic RCR should be counseled regarding a possible risk for inferior outcomes after surgery.
Keywords
Obesity remains a major global public health challenge, particularly in the United States, where 78% of adults are estimated to be classified as overweight or obese by the year 2030. 28 It is a component of metabolic syndrome, a cluster of conditions including high blood pressure, hyperglycemia, and hyperlipidemia, which increase the risk for cardiovascular disease and other major medical problems. 27 Bariatric surgery (BS) has proven to be an effective intervention for obesity and other components of metabolic syndrome when traditional weight loss measures have failed, producing sustained weight loss and improvement in overall metabolic profile. 20 However, BS has also been linked to postoperative nutritional deficiencies secondary to malabsorption, including vitamin D, calcium, iron, protein, and vitamin B12, resulting in multiple systemic medical consequences, including anemia, impaired bone metabolism, and an overall catabolic metabolic state.7,8,10,16,17,22,24,26 These nutritional deficiencies have been shown to persist for years after BS in long-term prospective studies. 5
While BS can be effective at achieving sustained weight loss and for reducing obesity-related comorbidities, the effect of BS on orthopaedic procedures remains largely unknown. The vast majority of investigations in the literature have focused on lower extremity arthroplasty and have demonstrated conflicting results regarding the overall effect of BS on postsurgical outcomes.6,15,21 In the upper extremity, multiple investigations have suggested that BS can lead to increased rates of instability and failure after total shoulder arthroplasty.3,19 Furthermore, the nutritional deficiencies produced by BS have the potential to negatively affect tendon healing. 20
Multiple systematic reviews have found that obese individuals undergoing arthroscopic rotator cuff repair (RCR) have higher rates of complications and reoperations compared with the general population.18,23 Obesity-related comorbidities, such as diabetes, also further increase the risk for complications after RCR. 11 It remains unclear whether treating obesity before arthroscopic RCR may improve outcomes, or whether arthroscopic RCR in the setting of BS affects outcomes. The purpose of this study was to compare failure rates and patient-reported outcomes after arthroscopic RCR between patients with and without a previous history of BS. We hypothesized that patients with a history of BS would have greater failure rates and inferior outcome measures after arthroscopic RCR compared to patients without a history of BS.
Methods
After study approval from our institutional review board, a retrospective review was conducted to identify patients with a history of BS who underwent primary arthroscopic RCR by 4 fellowship-trained shoulder and sports medicine surgeons (J.D.H., M.R., A.L., B.P.L.) at a single institution between March 2013 and June 2022. Inclusion criteria consisted of (1) a full-thickness supraspinatus tear and (2) a minimum postoperative follow-up RCR. Exclusion criteria consisted of (1) revision procedures, (2) open procedures, (3) use of biological or bioinductive augments, and (3) patients requiring concomitant subscapularis tendon repairs. The primary outcome was surgical failure, defined as a symptomatic retear confirmed on magnetic resonance imaging (MRI) and/or the need for revision RCR. The decision for performing a postoperative MRI study was made at the discretion of the treating surgeon. Secondary outcomes assessed included numeric rating scale (NRS) score for pain, Single Assessment Numeric Evaluation (SANE) score, American Shoulder and Elbow Surgeons (ASES) Shoulder Score, need for reoperation for arthroscopic lysis of adhesions (LOA) or manipulation under anesthesia (MUA), postoperative infection, and conversion to reverse total shoulder arthroplasty (rTSA).
The electronic medical record (EMR) was reviewed to confirm a history of BS before the performance of the arthroscopic RCR procedure, confirm the patient's past medical history, determine the tear size (assessed under direct arthroscopic visualization), and determine the Goutallier cuff atrophy grade (from the MRI radiology report). 25 Operative reports were reviewed to determine surgical repair construct (single- vs double-row repair), number of anchors, and concomitant procedures including formal acromioplasty and biceps tenodesis.
Eligible patients who underwent BS were contacted via telephone and email addresses were obtained from the electronic medical record and provided with a link to an electronic survey to obtain current demographic and clinical evaluation. Financial compensation was provided for completion of the survey through internal institutional funding. All survey responses were collected using REDCap (Research Electronic Data Capture; Vanderbilt University, Nashville, Tennessee), a HIPAA (Health Insurance Portability and Accountability Act)–compliant survey and data storage application. Patients who completed the survey were then matched in a 1:3 ratio by age (within 5 years), sex, and body mass index (BMI) (within 3 kg/m2) to patients in the no BS control group. Control participants were reviewed for match eligibility in consecutive order based on most recent surgical date.
A total of 712 RCR cases were retrieved from the initial query. After chart review, 74 patients were identified as having a history of BS performed before their arthroscopic RCR procedure. A total of 34 patients with a history of BS (24 female, 10 male; mean age, 56.4 ± 8.5 years; mean BMI, 33.5 ± 7.2 kg/m2) completed the electronic survey and met inclusion criteria. Of the cases excluded, 2 were open procedures, 5 utilized biological augmentation, 3 required subscapularis repairs, and 30 were unable to be reached for follow-up or declined to complete the survey. Techniques of BS procedures performed in descending frequency included Roux-en-Y (n = 17), adjustable gastric banding (n = 4), and sleeve gastrectomy (n = 1). Twelve patients were unable to recall the details of their bariatric surgical procedure, and no further information on the surgical technique was available in the EMR. The mean time from BS to arthroscopic RCR was 11.1 ± 7.2 years. The BS cohort was matched to 102 patients without a history of BS who underwent arthroscopic RCR (72 female, 30 male; mean age, 57.0 ± 8.1 years; mean BMI, 32.9 ± 7.0 kg/m2).
All patients in both treatment groups underwent arthroscopic RCR in the beach-chair position. Repair technique, implant selection, and utilization of concomitant procedures were at the discretion of the treating surgeon and based on the pathology identified at the time of surgery. All patients underwent postoperative rehabilitation under a standard institutional postoperative protocol. Patients were immobilized for 6 weeks postoperatively, with passive range of motion exercises beginning at 2 weeks after surgery. Active range of motion activities were initiated at 6 weeks after surgery with the guidance of physical therapy. Clearance for full functional activity was typically granted at 6 months postoperatively, depending on clinical course.
For statistical analysis, continuous variables were assessed using the Student t test for parametric data and Mann-Whitney U test to make comparisons between groups and between pre-and postoperative values. Chi-square and Fisher exact tests were used for categorical variables. The Shapiro-Wilk test for normality was used to assess the distribution of continuous data. Significance was set at a P value <.05. Power analysis was not performed given the low prevalence of eligible patients and novelty of the study. The proportion of patients who met or exceeded the Patient Acceptable Symptom State (PASS) for arthroscopic RCR was determined for each patient-reported outcome score using previously published anchor-based reference threshold values for the NRS (1.7), SANE (71.0), and ASES (78.0) scores. 12 Statistical analysis was performed using Stata (Version 18; Stata Corp).
Results
No significant differences were present in patient characteristics at baseline, including involvement of the dominant side, diagnosis of diabetes, and smoking status (Table 1). The mean rotator cuff tear size and median Goutallier rotator cuff atrophy grade did not significantly differ between groups (Table 2). There was no significant difference in the utilization rate of biceps tenodesis (P = .328) and acromioplasty (P = .808) performed, or the use of double- versus single-row repair constructs (P = .674). No bicep tenotomies were performed. The median anchor size was 4.75 mm for the medial and lateral rows in both cohorts.
Patient Characteristics a
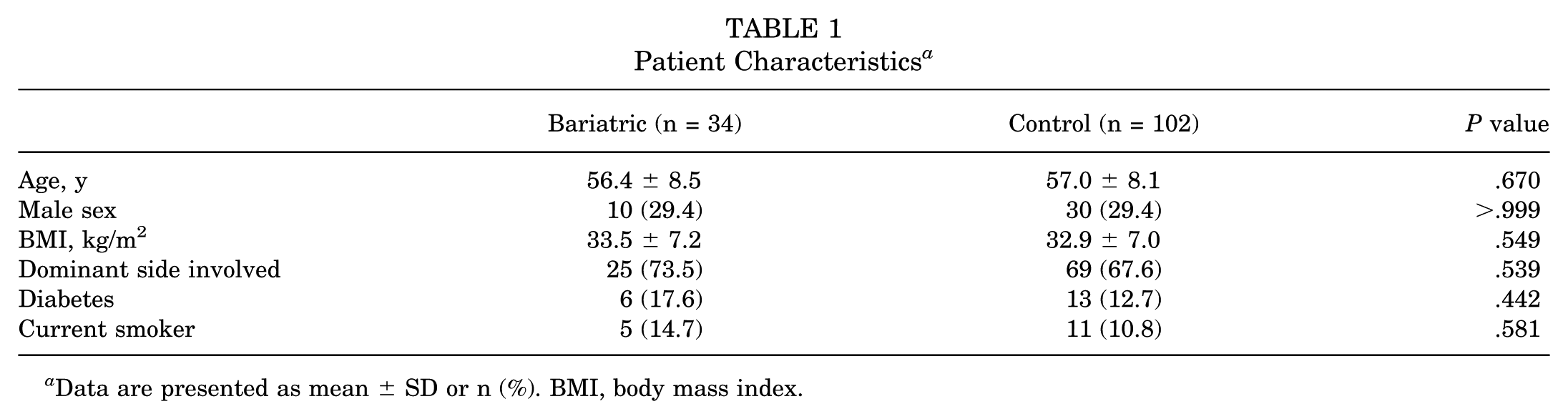
Data are presented as mean ± SD or n (%). BMI, body mass index.
Cuff Tear Features and Surgical Variables a
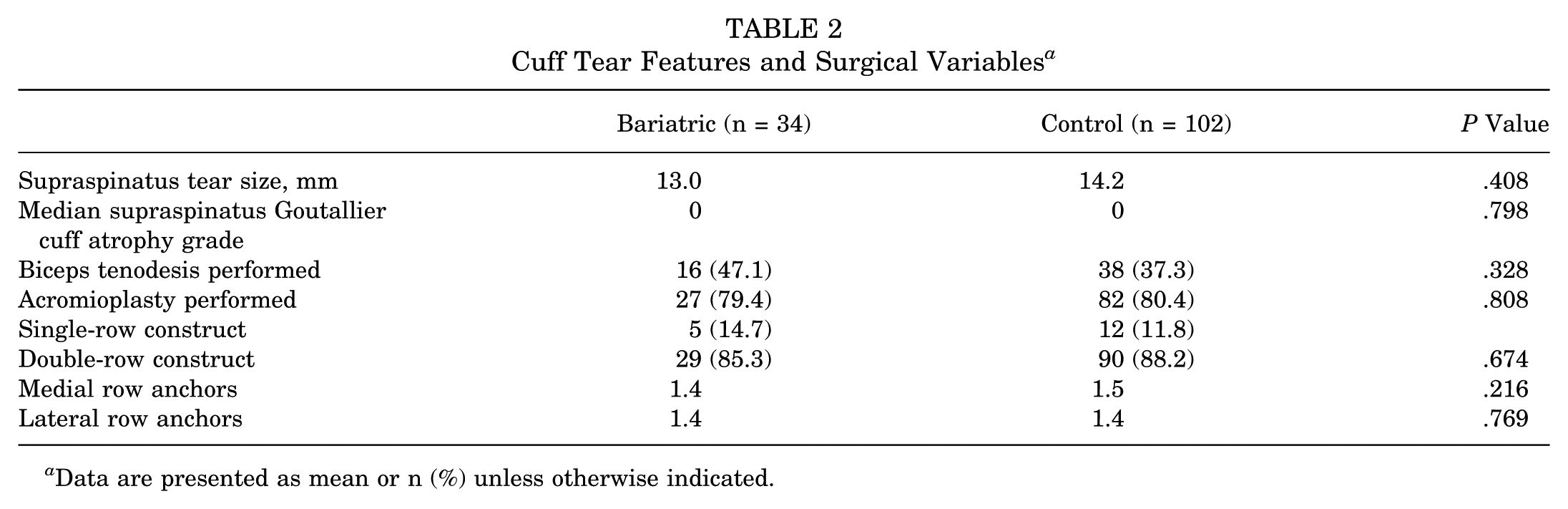
Data are presented as mean or n (%) unless otherwise indicated.
The mean follow-up was significantly different between the groups (52.7 months in the BS group, 72.3 months in the no BS group; P < .001). Table 3 lists primary and secondary outcome measures at the final follow-up. The BS group had significantly higher overall failure rates than patients without a history of BS (20.6% vs 6.9%; P = .044). The need for revision RCR (P = .267), MUA (P = .680), and conversion to rTSA (P = .154) rates did not reach significance between the groups. No postoperative infections were reported in either group.
Postoperative Outcomes at Final Follow-up
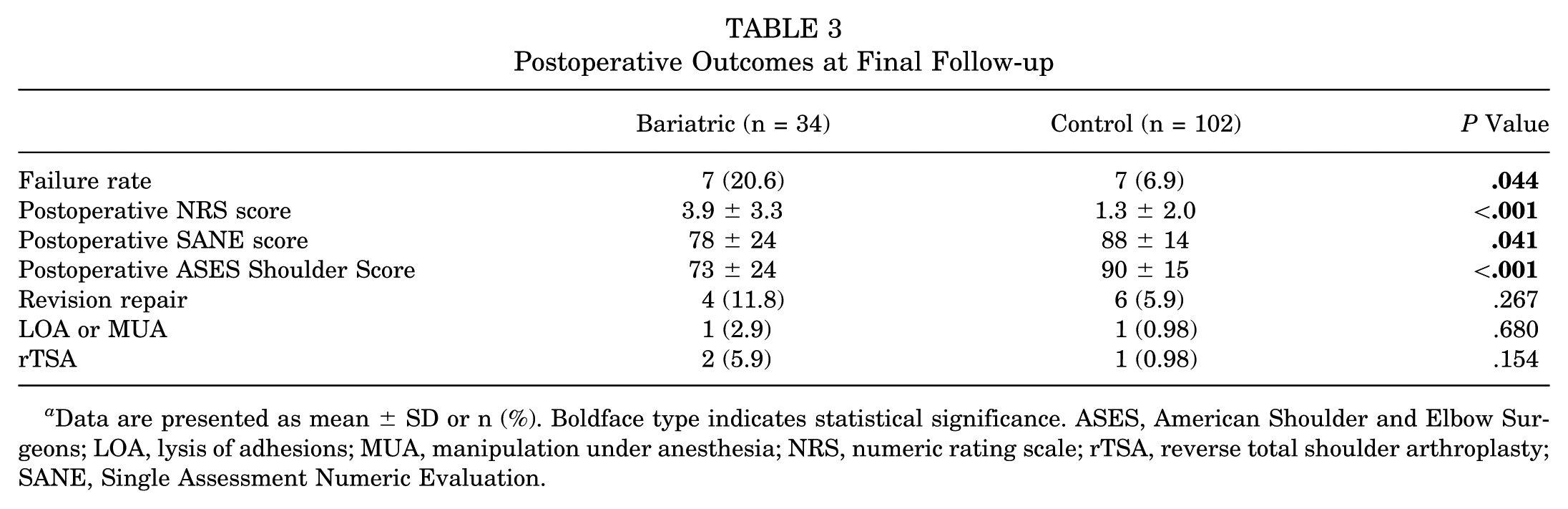
Data are presented as mean ± SD or n (%). Boldface type indicates statistical significance. ASES, American Shoulder and Elbow Surgeons; LOA, lysis of adhesions; MUA, manipulation under anesthesia; NRS, numeric rating scale; rTSA, reverse total shoulder arthroplasty; SANE, Single Assessment Numeric Evaluation.
The BS group had significant differences in subjective outcome measures with higher postoperative NRS (3.9 vs 1.3; P < .010), lower SANE (77.7 vs 87.73; P = .041), and lower ASES (72.60 vs 90.43; P < .001) scores at the final follow-up. For the BS cohort, the PASS was met in 12 (35.3%) patients for the NRS score, 24 (70.6%) for the SANE score, and 15 (44.1%) for the ASES score at the final follow-up. In the matched control cohort, the PASS was met in 68 (66.7%) patients for the NRS score, 85 (83.3%) for the SANE score, and 78 (76.5%) for the ASES score.
Discussion
This study demonstrated that patients with a history of BS had significantly higher surgical failure rates (defined as symptomatic retear and/or reoperation) and inferior patient-reported subjective outcome measures after arthroscopic RCR than patients without a history of BS. The BS cohort also had a decreased proportion of patients achieving the PASS for subjective outcome measures, including NRS, SANE, and ASES scores.
Risk factors for failure of arthroscopic RCR have been extensively researched in the orthopaedic literature. Screening metrics such as the Rotator Cuff Healing Index (RoHI) score have been introduced as tools to help identify patients who may be at high risk for RCR failure. 14 A history of BS may represent an underappreciated risk factor for RCR failure and should be considered when indicating patients for arthroscopic RCR. Surgeons may want to counsel patients who undergo BS of the increased risk of surgical repair failure and inferior outcomes during the informed consent process.
Obesity is a frequently cited risk factor for complications after arthroscopic RCR, although the literature is less clear regarding subjective and functional outcome measures. Sandler et al 23 performed a systematic review of 118,133 patients and found increased overall complication and reoperation rates in obese individuals undergoing arthroscopic RCR, but no significant difference in pain, ASES score, or range of motion. Another recent systematic review by Ma et al 18 found that obesity increased complication rates and resulted in inferior pain and functional scores. Obesity-related comorbidities further increase the risk for complications, with a systematic review by Hong et al 11 reporting that patients with diabetes had an overall 2.25-fold higher risk of radiographic retear after RCR.
With nearly 42% of all American adults currently classified as obese and >$300 billion estimated to be spent annually on obesity-related health care expenses, BS has emerged as an increasingly popular option for achieving sustained weight loss. 13 Rates of BS have been reported as high as 80 surgeries per 100,000 adults, making it important to understand the effect that these procedures can have on the outcomes of common orthopaedic interventions. 2 Metabolic studies have demonstrated that BS can result in malabsorption of iron, calcium, vitamin D, folate, vitamin B12, and zinc. 20 While long-term prospective studies in the literature are limited, there is evidence that deficiencies in bone metabolism persist more than a decade after BS. 5 There is limited evidence on nutritional supplementation after BS and no consensus on supplementation recommendations postoperatively, but studies suggest that metabolic deficiencies persist despite attempts at supplementation.4,17 These nutritional deficiencies negatively affect bone health and may affect the overall tendon-bone healing environment after arthroscopic RCR, which could be a contributing process to the increased failure rate in the BS cohort found in the present study.
There are several limitations of the present study. This study is limited given the constraints of a retrospective study. There was substantial loss to follow-up as only 34 of the 74 (45.9%) patients identified with a history of BS were able to be contacted to complete the electronic survey. History of BS was self-reported, and limited information was available regarding the details of the bariatric procedure. BS can be achieved through multiple surgical techniques, including Roux-en-Y, sleeve gastrectomy, adjustable gastric banding, and biliopancreatic diversion. These procedures have been shown to have variation in the magnitude of weight loss achieved, effect on metabolic comorbidities, and complication profile.1,9 Furthermore, nutritional values including albumin and vitamin D levels were not available to assess these potential baseline differences. Our cohort size was not sufficient to stratify by procedure type with adequate power, although previous large database investigations that stratified by BS technique for other orthopaedic procedures found no difference in outcomes. 19 Furthermore, there were wide differences in length of time between the patients’ BS and arthroscopic RCR, leaving potential for differences in overall nutritional state. Albumin levels and other nutritional laboratory studies were not routinely obtained as part of the preoperative workup for arthroscopic RCR at our institution and were not available for analysis; therefore, stratification of or controlling for nutritional status was not possible in this retrospective study. While many components of the RoHI score were recorded as part of this study, bone mineral density testing and level of work activity were not available for the majority of patients.
Conclusion
A history of BS is associated with increased failure rates, worse postoperative pain, and worse patient-reported outcomes after arthroscopic RCR. Patients with a history of BS and those considering BS before arthroscopic RCR should be counseled regarding a possible risk for inferior outcomes after surgery.
Footnotes
Final revision submitted March 15, 2026; accepted April 10, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.P.L. reports educational payments from Mid-Atlantic Surgical Systems. J.D.H. reports being part of the editorial board of Knee Surgery, Sports Traumatology, Arthroscopy (KSSTA) and Annals of Joint, and receiving consulting fees from Smith and Nephew. A.L. reports receiving consulting or advisory fees from Arthrex, Stryker, and Tornier; and being a board member of restor3d. V.M. reports receiving education fees from Smith & Nephew, Arthrex, DePuy Synthes, and Conmed; receiving consulting fees from Smith & Nephew and Newclip; receiving royalties from Springer; being a shareholder for Ostesys; being a co-developer of an iPad app (serial No. 61/566,761); being deputy editor-in-chief of Knee Surgery, Sports Traumatology, Arthroscopy (KSSTA); and having grant support from the NIH and Department of Defense. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Pittsburgh Institutional Review Board (STUDY23060003).