
Abstract
Background:
Anterior cruciate ligament (ACL) reconstruction (ACLR) is increasingly performed in children and adolescents, yet mid- to long-term graft ligamentization remains poorly understood.
Purpose:
To characterize the magnetic resonance imaging (MRI) evolution of ACL grafts in pediatric patients between 2 and 5 years postoperatively.
Study Design:
Case series; Level of evidence, 4.
Methods:
The authors included 50 pediatric patients undergoing transphyseal ACLR with a semitendinosus tendon autograft folded in 4 without additional lateral extra-articular tenodesis to evaluate the evolution of ACL graft ligamentization over 5 years using quantitative (signal-to-noise quotient, SNQ) and qualitative (Howell grading) MRI criteria. The SNQ was measured in intra-articular and intra-tibial graft regions. Tibial tunnel widening (TTW) and its relation to graft signal were also assessed. MRI scans were performed at 6, 12, 24, and 60 months postoperatively.
Results:
Sixteen patients completed a 60-month follow-up. The median intra-articular SNQ peaked at 12 months, decreased by 24 months (median, 3), and finally stabilized, with no significant change at 60 months (median, 2.8; P = .999). Similar trends were observed for intra-tibial SNQ with no significant difference between 24 and 60 months (P = .09). SNQ scores were compared using Wilcoxon signed-rank tests. Howell grading improved mainly within the first 24 months and remained stable thereafter, with Grade 1 or 2 in most grafts at final follow-up. TTW peaked at 6 months and gradually decreased.
Conclusion:
ACL graft ligamentization progresses primarily in the late first 2 years, followed by a subsequent plateau up to 5 years postoperatively.
Keywords
Anterior cruciate ligament (ACL) reconstruction (ACLR) in children and adolescents has become an increasingly common surgical intervention, paralleling a rise in ACL injuries within this population.29,36 This growing incidence is largely driven by factors such as heightened exposure in competitive sports, specialization at a young age, and improved recognition and diagnosis.26,29,47
When surgical criteria are met, early reconstruction is recommended. It enables the management of associated injuries, restores joint stability, reduces the risk of complications (eg, progressive meniscal or cartilage damage and early-onset osteoarthritis), and facilitates a return to preinjury levels of physical activity.7,18,25,27,39,50
Surgical techniques have evolved, becoming safer and more effective, even in growing individuals, with low overall rates of adverse outcomes.7,27,45 However, graft rerupture rates remain high in younger populations, where the incidence of reinjury is notably greater than that observed in adults.6,8,40,48,50
After ACLR, the graft goes through a 3-phase process called ligamentization, during which it gradually transforms to resemble a natural ligament: an initial postoperative phase where the graft is devascularized, preceding a remodeling phase (3-6 months) and finally a maturation phase starting around 12 months.3,15
Histological, macroscopic, and imaging evaluations of grafts have revealed the complex nature of their healing and ligamentization processes in animals20,38,46 and humans.38,43 Biological, biophysical, and surgical strategies have been explored to enhance maturation and show potential.30,44,52,55 However, their clinical effectiveness varies, and ongoing research is required to refine indications and optimize outcomes.
Magnetic resonance imaging (MRI) remains the only noninvasive method to monitor this process, which can be assessed by measuring the signal-to-noise quotient (SNQ) of the ACL graft. 31 Elevated SNQ values typically indicate less advanced graft ligamentization, as they reflect increased water content. Additionally, the degree of ligamentization can be assessed using the Howell classification system.23,24
The incorporation of ACL grafts in children appears to be a slow process, with a significant proportion of patients having grafts mature only after 2 years postoperatively.1,5,35,37 Data regarding mid to long-term graft maturation after ACLR remains limited. Concurrently, a shift may occur in postoperative management, with a move away from time-based rehabilitation protocols toward individualized return-to-sport (RTS) strategies. 22
This study is a follow-up to a previously conducted investigation that evaluated patients up to 24 months after surgery. 1 It aims to provide a more comprehensive understanding of graft ligamentization trajectories in pediatric populations by extending the postoperative follow-up period to 5 years. We hypothesized that the MRI signal of the graft evolves slowly in children. To our knowledge, this is the first study to evaluate graft ligamentization with a 5-year follow-up in skeletally immature patients.
Methods
A single-center study enrolled 50 consecutive patients. Approval was obtained from the local ethics committee (RnIPH 2019-56). The inclusion criteria were as follows: age between 6 and 16 years at the time of surgery; symptomatic ACL tear verified by MRI; presence of open growth plates at the time of surgery, confirmed on anteroposterior knee radiographs; and availability at the 60-month follow-up. The exclusion criteria were as follows: history of knee ligament surgery, joint infection, or inflammatory disease, ACL rupture or rerupture occurring during the follow-up period.
Surgical Technique and Postoperative Rehabilitation
The detailed surgical techniques have been published previously. 1 All patients underwent the same surgical procedure, namely a transphyseal ACLR with a quadrupled semitendinosus (ST4) tendon graft and adjustable femoral and tibial cortical fixation buttons. Based on a written protocol, outpatient physical therapy was initiated immediately after surgery. The standardized protocol instructed both patients and physical therapists to follow the same 1-year rehabilitation plan after ACLR. Follow-up consisted of 5 time points: 1 preoperatively and then at 6, 12, 24, and 60 months postoperatively.
Follow-up Planning
The 60-month follow-up was planned after the 24-month assessment as an extension of the original study. Patients were contacted by telephone, with up to 2 attempts, to schedule their final follow-up visit.
MRI and Image Analysis
MRIs were performed on 1.5 T units (Siemens Aera, GE Medical Systems Optima MR360, Toshiba Titan) at 6, 12, 24, and 60 months after ACLR and entailed a minimum of 4 sequences: T1 sagittal, proton density-weighted fat-saturated sagittal, coronal, and axial. MRI criteria validated in previous studies were applied to assess graft remodeling.11,15 MRI signal of the ACL graft and tibial tunnel widening (TTW) were assessed by 2 pediatric radiologists (L.S. and A.L.).
Primary Outcome
The signal intensity of the ACL graft was quantified in its intra-articular (IAG) portion by measuring the SNQ,31,46 calculated as follows through 3 regions of interest:
Secondary Outcomes
The SNQ was also evaluated in the graft's intra-tibial portion (ITG).

Howell intra-articular and intra-tibial grades were assessed and divided into 4 grades.23,24
Grade 1: Complete hyposignal of the ACL graft, equivalent to the posterior cruciate ligament or patellar ligament signal. Grade 2: graft with >50% proton density-weighted fat-saturated hyposignal. Grade 3: graft showing >50% proton density-weighted fat-saturated hypersignal, with portions showing normal ligament appearance. Grade 4: global hypersignal of the ACL graft with no portion of normal signal. Howell grade 1 and an SNQ close to 0 reflect good graft maturation. (Figure 1).

SNQ-IAG measurement at 60-month follow-up on sagittal T2 fat-saturated MRI. Placement of ROIs: 3 ROIs on the intra-articular segment of the ACL (1 proximal, 1 middle, and 1 distal), 1 ROI 2 cm in front of the patellar tendon, and 1 ROI on the PCL. (A) A boy aged 12 years at the time of surgery. SNQ, 1.2; Howell grade 1. (B) A girl aged 15 years at the time of surgery. SNQ, 9.4; Howell grade 3. ACL, anterior cruciate ligament; IAG, intra-articular graft; ROI, region of interest; PCL, posterior cruciate ligament; SNQ, signal-to-noise quotient.
The TTW was calculated with the following formula: 21

The bone tunnel (drilled) cross-sectional area (CSA) was calculated using the diameters of the tunnels according to the operative report. The measured CSA was assessed on oblique MRI slices, with the mean area recorded at the entrance of the tibial tunnel.
Previous studies have already established the interobserver reliability of the SNQ, Howell, and TTW.13,14,31,56
Statistical Analysis
This study was conducted under the hypothesis that SNQ would demonstrate a slow progression in the pediatric population. Before database lock and analysis, data quality was rigorously assessed for completeness and consistency. Baseline characteristics were summarized using descriptive statistics, reported as medians for continuous variables and counts for categorical variables. The primary endpoint, SNQ-IAG, was compared between 24 and 60 months using the Wilcoxon signed-rank exact test. Given the limited sample size (n = 16), no longitudinal mixed-model analysis was performed, as a significant decrease in SNQ-IAG between 12 and 24 months had already been established in the previous study. 1 Secondary endpoints, including tibial SNQ-ITG, were analyzed in the same way. Correlations between SNQ-IAG and TTW were assessed using linear regression or Spearman correlation. Ordinal variables, such as Howell scores for both intra-articular and tibial tunnel grafts, were compared between 24 and 60 months using the Wilcoxon signed-rank test for paired ordinal data. Nonparametric comparative analyses were also performed to compare patients included in the 60-month follow-up with those excluded or lost to follow-up. Continuous variables were compared using the Wilcoxon rank-sum test, and categorical variables using the Fisher exact test. All statistical analyses were conducted using RStudio (R Version 4.5.1; R Foundation for Statistical Computing), and P < .05 were considered statistically significant.
Results
Between September 2017 and April 2019, a total of 50 patients (33 boys; 17 girls) underwent transphyseal ACLR. A total of 24 patients were lost to follow-up, and 9 experienced graft rerupture at 6, 20, 42, 44, 48 (n = 2), 59, and 60 (n = 2) months postoperatively (7 boys, 2 girls). One patient sustained a contralateral ACL rupture at 16 months. This left 16 patients with a complete 60-month follow-up (Figure 2).

Patient flowchart. Full follow-up within 60 months included patients who had follow-up at 6, 12, 24, and 60 months postoperatively. ACL, anterior cruciate ligament.
No statistically significant differences were observed between patients with complete follow-up (n = 16) and those lost to follow-up or excluded (n = 34) regarding demographic variables, surgical characteristics (except age at time of surgery), or postoperative MRI SNQ values at 6, 12, and 24 months postoperatively (Table 1). This indicates that the final cohort was representative of the original study population.
Patient Characteristics—Comparison of Baseline and Early Postoperative Characteristics Between Patients With Complete Follow-up and Those Lost to Follow-up or Excluded a

Data are presented as median (IQR). BMI, body mass index; IQR, interquartile range; SNQ IAG, signal-to-noise quotient in intra-articular graft.
At final follow-up, the median age was 17.3 years (IQR, 3.4), and the median imaging follow-up duration was 60 months (IQR, 1.3).
SNQ values decreased significantly from 12 to 24 months after peaking at 12 months (Figure 3).

Evolution of SNQ IAG and ITG over time. SNQ IAG, signal-to-noise quotient of the intra-articular graft; ITG, signal-to-noise quotient of the intra-tibial graft.
At 60 months, the median SNQ-IAG value was 2.8, showing a nonsignificant difference compared with 24 months (3; P≥.999). SNQ-ITG values followed a comparable trend, with no significant change between 24 and 60 months (P = .09) (Table 2).
SNQ Values at 24 and 60 Months of Follow-up a
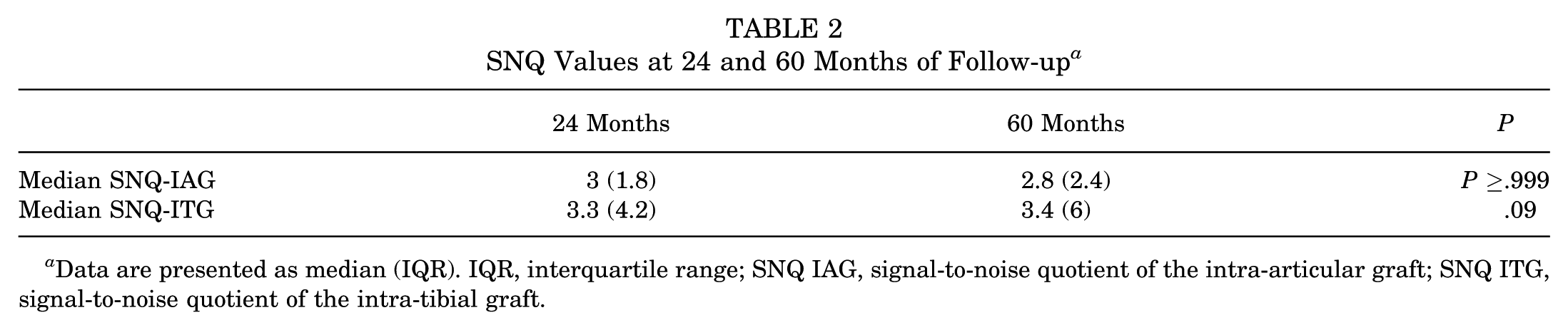
Data are presented as median (IQR). IQR, interquartile range; SNQ IAG, signal-to-noise quotient of the intra-articular graft; SNQ ITG, signal-to-noise quotient of the intra-tibial graft.
The Howell grades improved mainly between 12 and 24 months, with most grafts moving toward lower grades, but showed no statistically significant change between 24 and 60 months (P = .18 and .79, for IAG and ITG, respectively). At 60 months, most grafts reached grade 1 or 2, although a slight increase in grade 3 was observed, with Grade 1 remaining predominant (Figure 4).

Evolution of the Howell scale IAG & ITG over time. IAG, intra-articular graft; ITG, intra-tibial graft.
Tibial cross-sectional area increased by 71.4% at 6 months, gradually narrowing to 67.8% of the original drilled area at 60 months. Correlation analyses revealed no significant association between SNQ-IAG and TTW at any postoperative time point.
Discussion
Both intra-articular and intra-tibial SNQ values remained globally stable between 24 and 60 months postoperatively, following an initial significant decrease observed between 12 and 24 months, after peaking at 12 months. 1 This stabilization suggests that graft signal intensity reaches a plateau rather than continuing to decline. Howell grading followed a similar pattern, with most grafts improving between 12 and 24 months and then remaining stable up to 5 years. However, a slight increase in grade 3 cases was observed at the final evaluation. This evolution mirrors that observed in adult studies, in which grafts exhibit an early peak in signal intensity around 6 months, followed by progressive normalization and stabilization as ligamentization progresses.2,56
A key observation is that the peak in signal intensity, corresponding to the early phase of graft remodeling, occurs later in pediatric patients than in adults, reflecting a slower ligamentization process.2,5,56 Several factors may contribute to this delayed maturation. The intra-articular cytokine environment,9,42 age-related variations in tendon microstructure, 4 and differences in physical activity modalities between children and adults 50 have all been proposed to influence graft remodeling dynamics. No significant association was observed between residual laxity and graft maturation.1,34
Tibial tunnel widening, which peaked around 6 months postoperatively and then gradually decreased, showed no clear relationship with ligamentization. This aligns with Biset et al, 10 who reported no correlation between tibial tunnel enlargement and graft maturation after short semitendinosus tendon autograft reconstruction, and with Liu et al, 32 who described early tunnel expansion followed by stabilization over time, without any link to clinical outcomes or graft appearance. Conversely, Zhang et al 54 identified a potential association between graft maturation and the femoral tunnel aperture radius, suggesting that specific anatomical characteristics may influence the biological healing process.
The minor shift in Howell grade distribution does not necessarily indicate graft deterioration but may reflect physiological remodeling variability. This interpretation is supported by Pauvert et al, 37 who demonstrated that MRI appearances of normal ACLs in adolescents can show significant heterogeneity in both signal intensity and qualitative grading. Persistent graft hypersignal in adults has also been described years after ACLR. 19 Scheffler et al 41 reported that, while the mechanical properties of grafts decrease during ligamentization, they may never fully return to normal levels.
Optimization of graft healing remains an area of active investigation. Adjunct procedures, such as lateral extra-articular tenodesis (LET), have gained renewed interest, particularly for their role in reducing graft failure. In contrast, their effects on graft maturation remain less well studied. Current indications for combining LET with primary ACLR in the pediatric population include recurvatum >10°, generalized hyperlaxity, a grade 2 or 3 pivot shift, participation in pivoting, collision, or contact sports, and cases involving poor neuromuscular control or limited rehabilitation capacity. 7 Evidence suggests that additional LET may reduce the risk of graft rerupture. Wilson et al 49 observed a reduced rerupture risk in pediatric populations after the addition of LET. Similarly, Carrozzo et al 12 found that combined ACLR + LET in pediatric patients resulted in a low graft failure rate, comparable to outcomes observed in adults. With respect to graft maturation, Cavaignac et al 14 showed that at 1 year postoperatively, MRI appearance indicated better graft incorporation and maturation with combined ACLR + LET. However, a recent systematic review and meta-analysis indicates that adding LET to ACLR does not significantly improve graft maturation. 17 Whether surgical strategies such as LET could influence both graft maturation and subsequent failure risk simultaneously remains an area requiring further investigation, as several studies have reported a correlation between an elevated SNQ and an increased retear risk.33,51,53 In our study, we did not directly assess this relationship, and no patient underwent an associated LET.
Given the slow graft maturation observed in our cohort, it is reasonable to question whether current postoperative RTS guidelines should be reconsidered or adapted. Greenberg et al 22 emphasized that existing clearance protocols and RTS algorithms lack precision because they often rely heavily on nonmodifiable risk factors and proposed a novel algorithm, the ACL-RRP, as a more individualized approach. Incorporating artificial intelligence into such tools may enhance their accuracy and clinical relevance.
Prolonged restriction of sports participation for several years after surgery appears unrealistic in pediatric and adolescent populations, who require regular physical activity for optimal cardiovascular, musculoskeletal, cognitive, and psychosocial development. The issue may not be solely about timing but also about the quality and individualization of postoperative rehabilitation. Beyond an initial period of sport cessation, tailored, long-term rehabilitation strategies adapted to each child's functional recovery and risk profile may represent a more relevant approach. Additionally, for inclined patients, redirecting toward lower-risk sports may be a pragmatic strategy to maintain physical activity while minimizing re-injury risk.
Although MRI may assist in RTS decision-making, no radiological scoring system has yet proven accurate enough to guide these decisions independently. 16 Overall, these findings underline the dynamic nature of graft healing in pediatric patients and reinforce the notion that complete normalization on MRI may not occur even several years after surgery. Furthermore, they highlight the limitations of using MRI as a standalone marker of biological maturity, particularly in young athletes, where baseline variability is high, warranting further investigation into their correlation with functional outcomes and mechanical stability.
This study presents multiple strengths. It is, to our knowledge, the first to provide a 5-year MRI-based follow-up of ACL graft maturation in skeletally immature patients. The standardized imaging protocol and consistent surgical and rehabilitation approaches enhance the internal validity of the results. Some limitations must be acknowledged. The study was single-centered, lacked a control group, and included a small final sample (n = 16) without previous power analysis. To address potential bias, we took methodological steps to assess the representativeness of our final cohort. The absence of patient-reported outcome measures and objective laxity measurements represents a limitation of this study. It would have been interesting to include SNQ measurements obtained at the time point immediately preceding rerupture. This would have allowed us to explore whether elevated SNQ values could serve as an early indicator of graft vulnerability and help identify patients at higher risk of failure. This could be considered in future prospective studies evaluating the predictive value of MRI markers for graft rerupture in pediatric populations.
Conclusion
Graft signal intensity improves mainly within the first 2 years after ACLR, followed by stabilization up to 60 months, suggesting that pediatric ACL grafts follow a delayed but ultimately stable maturation pattern, supporting the need for individualized postoperative and RTS strategies in this population.
Footnotes
Final revision submitted March 29, 2026; accepted April 4, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: F.A. is a consultant with Orthofix and Zimmer Biomet.
Ethical approval for this study was obtained from the Toulouse University Hospital local ethics committee (RnIPH 2019-56).