
Abstract
Background:
Shoulder dislocation injuries may require prolonged recovery and absence from play, with risks of recurrent instability. The impact of shoulder dislocation on return-to-play (RTP) time and player performance in professional soccer athletes remains poorly defined.
Purpose:
To determine the rate and timing of RTP, risk of recurrence, and player performance after shoulder dislocation in elite professional soccer athletes.
Study Design:
Descriptive Epidemiology Study.
Methods:
Professional soccer athletes who sustained a shoulder dislocation between 2010 and 2024 across the 5 major European soccer leagues with a minimum 1-year follow-up were identified using publicly available records. Injured athletes were matched by position, age, height, season, experience, and preinjury minutes played and compared to uninjured controls. RTP rates, recurrence, field time, and performance up to 4 seasons after injury were assessed.
Results:
A total of 118 soccer athletes with shoulder dislocations were included (38% defenders, 23% attackers, 20% goalkeepers, and 19% midfielders). Mean age at time of injury was 26.2 ± 4.2 years. Overall, 87% returned to the same level within 2 seasons after shoulder dislocation. Injured athletes missed a median of 68 days and 10 games, with goalkeepers missing more days (124 vs 60, P < .001) and games (21 vs 8, P < .001) compared to outfield players. Recurrence occurred in 18% at a mean time of 2.6 ± 2.4 years, with a higher risk in athletes ≤25 years (26% vs 12%, P = .046). By treatment, 59% and 41% underwent operative and nonoperative management, respectively, with similar recurrence rates (17.1% vs 18.8%, P = .823) but longer time to recurrence in the operative group (3.82 ± 2.91 vs 1.41 ± 0.69 years, P = .009). Injured athletes played significantly fewer games, total minutes, and minutes per game during the index season and at 1 and 2 seasons after shoulder injury compared with matched controls. However, performance metrics and RTP rates in all seasons after injury remained comparable to matched controls across all positions and treatment groups.
Conclusion:
Professional soccer athletes returned to play at a high rate and a median of 68 days after shoulder dislocation, with an 18% recurrence rate. Despite reduced field time for up to 2 seasons after injury, overall player performance and RTP were not adversely affected.
Professional soccer imposes considerably high physical demands and frequent player-to-player contact, particularly at the elite level, with great intensity and speed, exposing athletes to a broad spectrum of musculoskeletal injuries. While most soccer-related injuries involve the lower extremities, upper extremity injuries still occur and warrant greater clinical attention due to their potential impact on player availability and performance.7,9,11,14 Among these, anterior glenohumeral or shoulder dislocation is an important pathology in young athletes and may have substantial implications for professional athletes.1,15,16,21 However, shoulder dislocations remain poorly characterized within elite soccer. 21
Shoulder dislocations in soccer can result from several mechanisms that may vary by player position, most commonly from direct contact to the upper extremity or from attempts to catch or brace a fall. 22 Goalkeepers appear particularly vulnerable due to the unique demands of their position, including repetitive overhead reaching, diving movements, forceful landings, and rapid arm transitions, all of which increase their risk of instability events.9,20,22 Shoulder dislocation injuries may require prolonged recovery and absence from play, with risks of recurrent instability, functional impairment, and need for surgical intervention. 16
Previous investigations on shoulder dislocations in soccer have primarily focused on epidemiology and management.7,15,20,21,23 However, there remains a paucity of literature regarding return-to-play (RTP) expectations, recurrence risk, optimal management strategies, and the impact of these injuries on performance across player positions in professional soccer. Knowledge of these metrics can help sports medicine specialists counsel athletes and set appropriate expectations. As such, the purpose of this matched-cohort study was to determine the rate and timing of RTP after shoulder dislocation in elite professional soccer athletes, assess the risk of recurrence after RTP, and evaluate the effect of shoulder dislocation on future field time and performance outcomes. We hypothesized that professional soccer athletes sustaining a shoulder dislocation would demonstrate high RTP rates but experience prolonged absence from play and reduced field time after injury, particularly among goalkeepers.
Methods
Player Identification and Data Source
A retrospective matched-cohort study was conducted on male professional soccer athletes who sustained a shoulder dislocation between 2010 and 2024 while competing in 1 of the top 5 first-division UEFA leagues: Premier League (England), Bundesliga (Germany), La Liga (Spain), Ligue 1 (France), and Serie A (Italy). Players with any recorded shoulder injury were first identified using a publicly available database (transfermarkt.co.uk), following methods established in prior investigations.6,12,18,19,26 Each reported shoulder injury was then manually reviewed and cross-referenced by 2 independent authors (T.K. and H.H.) to confirm that the diagnosis specifically represented a shoulder dislocation. Verification was performed using various online resources, including transfermarkt.co.uk, uefa.com, fifa.com, official team websites and press releases, media injury reports, personal athlete websites, and professional statistical platforms. Demographic data, injury history and characteristics, and performance metrics were subsequently extracted from the publicly available database. Institutional review board approval was not required for this study.
Inclusion Criteria
Inclusion criteria consisted of players who sustained a shoulder dislocation while actively rostered and playing on a team in 1 of the top 5 European leagues, had participated in at least 1 match prior to injury, and had a minimum 1-year follow-up after the injury. Exclusion criteria included players with an unknown diagnosis or a diagnosis other than shoulder dislocation.
Data Collection
Player demographic and preinjury characteristics collected included age at the time of injury, height, player position (goalkeeper, defender, midfielder, or attacker), team, league, season of injury, total minutes played in season prior to injury, and years of professional experience at the time of injury. Outfield players were defined as those playing in defensive, midfield, or attacking positions. Injury and RTP variables recorded included date of injury, days and games missed, date of RTP, and recurrence of injury. Each player with a shoulder dislocation was evaluated to determine the type of treatment received (surgical management or nonoperative care). Performance metrics extracted included games played, total minutes played, goals scored, assists, clean sheets, goals conceded, and points per game. RTP was defined as return to competition in any of the 5 major UEFA leagues. Players transferred to another team within one of these leagues were included in the RTP cohort, whereas those transferred to lower-tier leagues were excluded from the RTP cohort.
Case-Control Matching
A representative control group of soccer players was identified and matched to injured players in a 1:1 ratio using the nearest-neighbor method. Players with any history of shoulder injury were excluded from the control cohort. Matching variables included player position, height, age (±2 years), season year (±2 seasons), years of player experience (±1 year), and total minutes played in the season prior to injury. A matched-cohort analysis was then conducted to compare performance metrics between injured players and their uninjured matched controls.
Statistical Analyses
Statistical analyses were performed using Stata statistical software, Release 14.1 (StataCorp LLC). Player demographics and injury characteristics were summarized as means with standard deviations or as medians with interquartile ranges for nonnormally distributed variables. Univariate comparisons of continuous variables were performed using 2-tailed Student t tests, with Wilcoxon rank-sum tests applied when normality assumptions were violated. Categorical variables were expressed as frequencies and percentages and compared using Pearson's chi-square or Fisher's exact tests, as appropriate. Comparative analyses of player field time and performance metrics were performed between injured players and their matched controls for the index season and at 1, 2, 3, and 4 years after the index year. Analyses at each time point included all athletes with available follow-up for that season after injury. A subgroup analysis stratified by player position was also performed. Injured players who transferred to leagues outside the 5 major UEFA leagues and were therefore excluded from the RTP cohort were also excluded from the performance analyses. A post hoc analysis of injured players treated operatively versus nonoperatively was also conducted to evaluate differences in RTP rates, field time, performance metrics, and recurrence. Statistical significance was set at P < .05.
Results
Player Demographics and Preinjury Characteristics
A total of 118 professional soccer athletes participating in 1 of the top 5 major European soccer leagues were identified as having sustained a shoulder dislocation injury between 2010 and 2024. The mean age at the time of injury was 26.2 ± 4.2 years (range, 18-37 years), the mean height of injured athletes was 1.83 ± 0.07 m, and the mean number of years of playing experience in a top 5 league was 9.6 ± 4.1 years. Shoulder dislocations most frequently occurred in defenders (n = 45, 38%), followed by attackers (n = 28, 23%), goalkeepers (n = 23, 20%), and midfielders (n = 22, 19%). There were no significant differences in age at the time of injury, height, calendar year of season, years of experience, and total minutes played in the season prior to injury between the injured and control cohorts (P > .05). Demographics and preinjury characteristics for soccer athletes who sustained shoulder dislocations and uninjured controls are presented in Table 1.
Player and Control Demographics and Preinjury Characteristics a

Values are presented as mean ± standard deviation unless otherwise indicated.
Of the athletes who sustained a shoulder dislocation, 69 (58.5%) underwent primary surgical management, whereas 49 (41.5%) were treated nonoperatively. Goalkeepers were significantly more likely to undergo surgical management (n = 20/23, 87%) compared with outfield players (n = 49/95, 51.6%; P = .002). No other player demographic factors or preinjury characteristics were significantly associated with treatment method (P > .05).
Return to Play
Overall, 87.3% (n = 103/118) of players who sustained a shoulder dislocation returned to play successfully at the same level of competition. Of these, 69.5% (n = 82) returned in the same season of injury, and 84.7% (n = 100) returned within 1 season of injury. Injured athletes missed a median of 68 days (range, 4-222 days) and 10 games (range, 1-41 games). By player position, goalkeepers had a significantly lower rate of RTP in the same index season of injury (n = 11/23, 47.8%) compared with outfield players (n = 71/95, 74.7%; P = .012). Goalkeepers also missed significantly more days (median 124 [IQR, 85-159] vs 60 [IQR, 25-92], z = 4.80, P < .001) and games (median 21 [IQR, 13-30] vs 8 [IQR, 4-13], z = 4.67, P < .001) compared to outfield players. No significant differences were observed in RTP rates by player position at any time point after the index season. Player injury characteristics and RTP outcomes are summarized in Table 2.
Injury Characteristics and Return to Play a
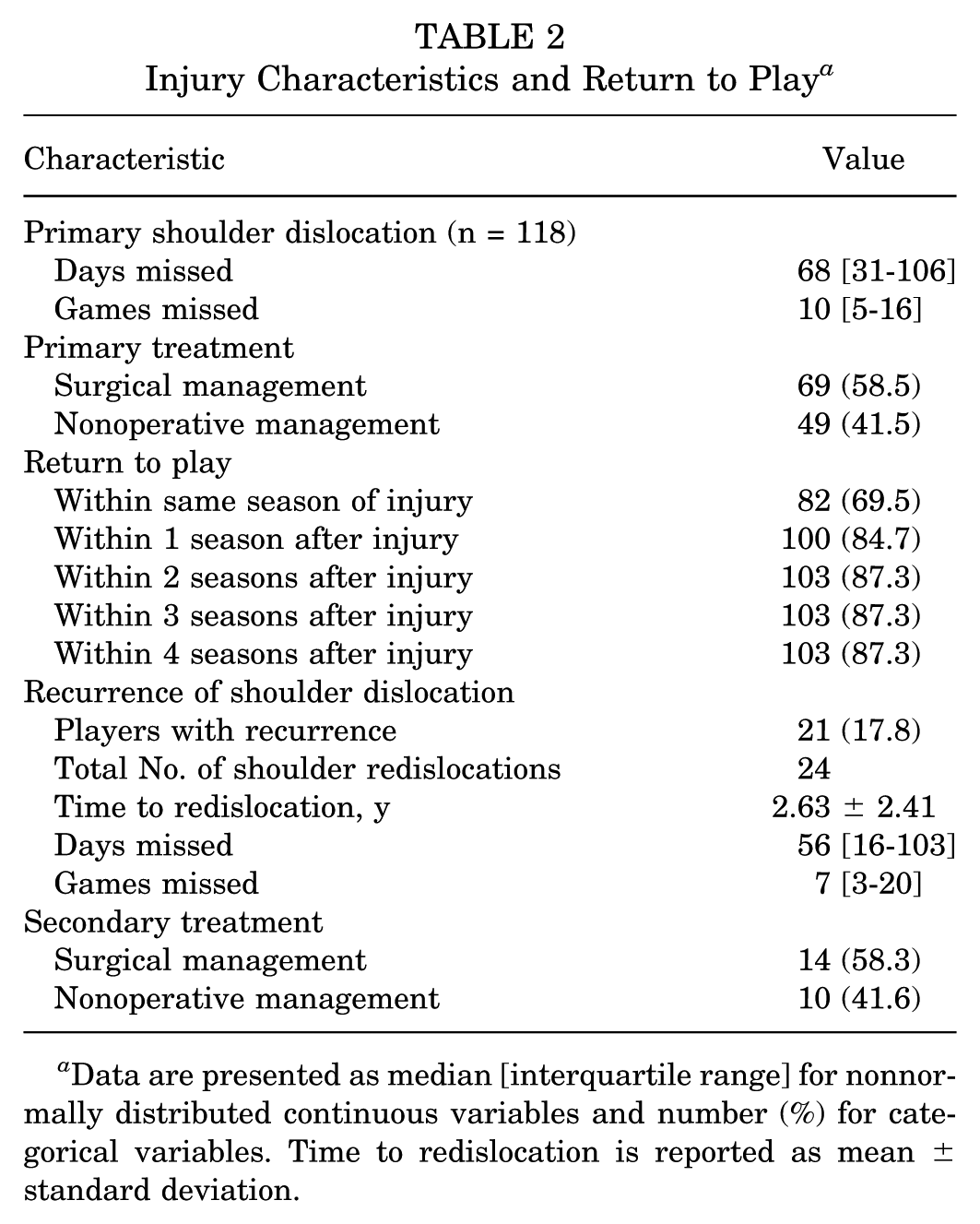
Data are presented as median [interquartile range] for nonnormally distributed continuous variables and number (%) for categorical variables. Time to redislocation is reported as mean ± standard deviation.
Recurrence of Shoulder Dislocations
Among all injured players, 17.8% (n = 21/118) sustained a secondary shoulder dislocation at a mean interval of 2.63 ± 2.41 years from the index injury (range, 0.30-10.24 years) (Table 2). Three players experienced a third dislocation event. Following the secondary injury, athletes missed a median of 56 days (range, 3-225 days) and 7 games (range, 0-44 games), with no significant difference compared with days or games missed after the primary injury. Of the 24 recurrent events, 14 (58.3%) were managed surgically and 10 (41.6%) nonoperatively. Players who sustained their primary dislocation at ≤25 years of age had a significantly higher recurrence rate than those >25 years (26% vs 12%, P = .046). Recurrence rates did not significantly differ by player position (P = .103).
Player Field Time and Performance
Overall Cohort
In the overall cohort, players with shoulder dislocations demonstrated significantly reduced field time compared with matched controls across multiple seasons (Figure 1). During the index season, injured players played fewer games (25.7 ± 11.9 vs 33.1 ± 11.8, P < .001), total minutes (1831 ± 1008 vs 2624 ± 1173, P < .001), and minutes per game (69.8 ± 17.4 vs 77.4 ± 15.2, P < .001). In the first season after injury, players played fewer games (26.6 ± 13.2 vs 32.8 ± 11.7, P < .001), total minutes (1900 ± 1176 vs 2608 ± 1087, P < .001), and minutes per game (69.4 ± 18.9 vs 77.5 ± 15.3, P = .001). Similarly, players played fewer games (26.3 ± 13.3 vs 30.9 ± 11.5, P = .016), total minutes (1812 ± 1175 vs 2382 ± 1094, P = .001), and minutes per game (64.2 ± 22.5 vs 76.1 ± 16.2, P < .001) in the second season after injury, as well as fewer total minutes (1716 ± 1252 vs 2242 ± 1268, P = .018) in the third season after injury.
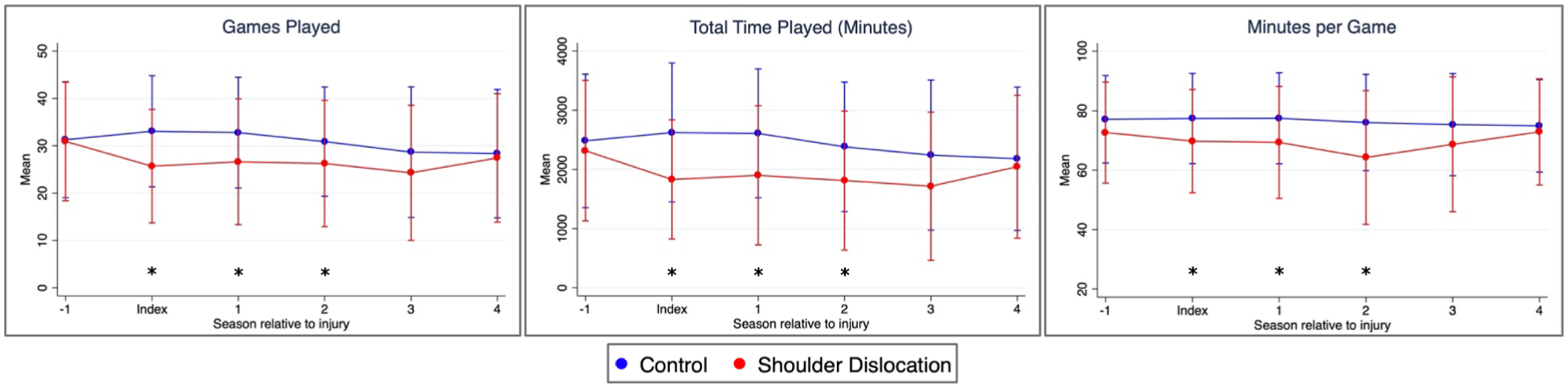
Overall player field time. *P < .05.
Goalkeepers
Goalkeepers comprised 23 players (20%) with a mean age of 27.8 ± 4.2 years. Goalkeepers who sustained shoulder dislocations demonstrated significantly fewer games played during the index season (22.0 ± 16.7 vs 36.2 ± 9.5, P < .001) and the first season after injury (21.4 ± 15.1 vs 36.2 ± 12.1, P = .002). They also recorded fewer total minutes played in both the index season (1897 ± 1363 vs 3263 ± 1104, P < .001) and the first postinjury season (1969 ± 1519 vs 3257 ± 863, P = .002). Minutes per game were lower for injured goalkeepers during the index season (86.3 ± 6.3 vs 89.8 ± 1.2, P = .012). No differences in field time metrics were found at any other time point. Although injured goalkeepers registered fewer clean sheets across multiple seasons, this difference did not reach statistical significance. No significant differences were observed between injured and control goalkeepers in goals conceded per game or points per game across any season. Field time and performance metrics for injured and control goalkeepers are presented in Figure 2.

Goalkeeper field time and performance metrics. *P < .05.
Outfield Players: Defenders, Midfielders, and Attackers
Among the 95 outfield players, 45 (38%) were defenders, 22 (19%) were midfielders, and 28 (24%) were attackers. Outfield players with shoulder dislocations demonstrated significantly fewer games played, total minutes, and minutes per game compared with matched controls during the index season and across multiple following seasons (P < .05) (Figure 3). Defenders demonstrated significantly fewer games played and total minutes during the index season (P < .01), as well as reduced minutes per game during the index season and at 1 and 2 seasons after RTP (P < .05). Midfielders played significantly fewer games, total minutes, and minutes per game 1 year after injury (P < .01) and fewer total minutes and minutes per game 2 seasons after injury (P < .01). Attackers played significantly fewer total minutes and minutes per game 2 seasons after injury (P < .05).

Outfield players’ field time. *P < .05.
Injured outfield players demonstrated similar performance metrics compared with matched controls (Figure 4), except for recording more assists per game 2 seasons after RTP (0.16 ± 0.23 vs 0.10 ± 0.09, P = .031). No defenders demonstrated any significant difference in points, goals, or assists per game as compared with control athletes at any time point. Injured midfielders recorded higher points per game 2 seasons after RTP (1.88 ± 0.37 vs 1.44 ± 0.51, P = .010), while injured attackers recorded more assists per game 2 seasons after RTP (0.28 ± 0.26 vs 0.15 ± 0.07, P = .038).

Outfield players’ performance metrics. *P < .05.
Post Hoc Analysis: RTP, Performance, and Recurrence by Injury Management
Players who underwent surgical management missed significantly more days (median 94 [IQR, 71-129] vs 25 [IQR, 19-41], z = 8.12, P < .001) and games (median 15 [IQR, 10-24] vs 5 [IQR, 3-7], z = 7.29, P < .001) compared with those treated nonoperatively. Surgically managed players also had a significantly lower rate of RTP in the same season (69.5%) compared with players treated nonoperatively (83.3%, P = .007), although there was no significant difference in RTP at 1, 2, 3, and 4 seasons after injury.
Field time and player performance metrics were similar between athletes treated surgically and nonoperatively as well as in subgroup analysis based on player position, except for nonoperative outfield players having higher assists per game at 4 seasons after injury (0.17 ± 0.18 vs 0.06 ± 0.07, P = .013) and higher points per game during the index season (1.60 ± 0.41 vs 1.37 ± 0.54, P = .021).
The recurrence rate was similar between players treated surgically (n = 12/70, 17.1%) and nonoperatively (n = 9/48, 18.8%; P = .823). However, the time to redislocation was significantly greater in athletes managed surgically (3.82 ± 2.91 years) than in those managed nonoperatively (1.41 ± 0.69, P = .009). The revision rate in surgically managed athletes was 14.3% (n = 10/70), and 8.3% (n = 4/48) of athletes initially treated nonoperatively ultimately underwent surgery. Of the 3 athletes who sustained 3 dislocation events, 2 initially underwent nonoperative treatment for both the primary and secondary dislocations, with 1 receiving surgery and the other continuing nonoperative care after the tertiary event. The third athlete underwent primary operative treatment, nonoperative treatment for the secondary dislocation, and revision surgery following the tertiary event.
Discussion
The present matched-cohort study evaluated RTP rates, recurrence, and player performance outcomes in 118 elite European professional soccer athletes who sustained a shoulder dislocation. The principal finding was that 87% of players returned to the same level of play within 2 seasons following a shoulder dislocation, missing a median of 68 days and 10 games. The recurrence rate was 18%, with a mean time to recurrence of 2.6 years. Overall, injured athletes demonstrated reduced field time during the index season and at 1 and 2 seasons after injury compared with matched controls; however, performance metrics following RTP were similar between groups across all player positions. Although surgically managed athletes missed more days and games and had a lower RTP rate during the index season compared with those treated nonoperatively, subsequent RTP rates and performance metrics at all later time points, as well as recurrence rates, did not differ significantly between treatment groups. To our knowledge, this is the first study to perform a matched-cohort analysis of player performance following shoulder dislocation in professional elite soccer athletes.
Shoulder injuries in soccer have a low reported incidence of 2% to 4.4%,10,17,20 yet the impact of shoulder dislocations remains clinically important. A UEFA injury surveillance study found that 28% of shoulder injuries in professional players were severe—defined as absence from training and match play over 28 days. 10 In the present study, more than 75% of players missed over 28 days, which highlights both the severity of these injuries and that the effect of shoulder dislocations on time to RTP may be greater than previously described. Prior investigations have also demonstrated an elevated risk of upper extremity injuries among goalkeepers compared with outfield players, likely reflecting the position-specific demands of repetitive overhead reaching, rapid arm transitions, diving, and forceful landings.9,13,20 Terra et al 25 reported that the most common mechanisms of dislocation in goalkeepers were abduction, external rotation, and extension. Nonetheless, outfield players account for most dislocations (77%) in our cohort, underscoring that shoulder dislocations remain a meaningful concern across all positions. Although not classified as a collision sport, soccer is considered a contact sport because the rules permit frequent physical interactions such as tackles, shoulder-to-shoulder challenges, and aerial duels, which create regular opportunities for high-speed player-to-player contact when contesting possession and defending. Consequently, a substantial proportion of soccer injuries result from a direct or incidental impact. In a systematic video analysis of 37 shoulder dislocations, Schneider et al 22 identified the 2 primary injury mechanisms as direct contact to the upper extremity by an opponent (60%) and attempting to catch a fall with an outstretched arm (38%).
Our study demonstrated a high RTP rate of 87% among soccer athletes sustaining a shoulder dislocation, indicating that most players achieve functional recovery and return to their preinjury level within 2 seasons of injury. Despite missing a median of 68 days and 10 games following shoulder dislocation, nearly 70% of players were able to RTP within the same index season of injury, suggesting that shoulder dislocation injuries are not necessarily season-ending. The likelihood of returning to play during the same season depends on several factors, including the timing of the injury within the season, whether surgical management is required, and the player's position. Surgically managed athletes had a significantly lower RTP rate in the index season and missed more days and games than those treated nonoperatively. This is expected as structured postoperative rehabilitation is required to restore functional stability and minimize the risk of recurrence. In a retrospective case series of 22 professional soccer athletes undergoing surgical stabilization for anterior shoulder instability, the median time to RTP was 77 days, 15 which was similar to our cohort, where surgically managed athletes returned at a median of 94 days. Moreover, compared with outfield players, goalkeepers exhibited a lower RTP rate within the index season and required a significantly longer recovery, missing a median of 124 days and 21 games. This likely reflects goalkeepers’ reliance on upper extremity function, as they must be able to reach overhead, make rapid multidirectional movements, and dive and land safely. These demands place greater stress on the shoulder and require restoring range of motion, strength, and proprioception before safely returning to competition, thus requiring more time before RTP. 20 Goalkeepers were also significantly more likely to undergo surgical management, further contributing to their prolonged recovery.
Despite these differences within the index season, no significant differences in RTP rates were observed across player positions or treatment groups at 1, 2, 3, and 4 seasons after injury. In the overall cohort, injured athletes demonstrated reduced field time in the index season and during the 2 seasons following injury compared with matched controls, reflected by fewer games played and reduced total minutes and minutes per game. However, once athletes returned to play, performance metrics were generally comparable between injured and control players across all positions. These findings suggest that while shoulder dislocations result in meaningful time missed and reduced participation during the index and subsequent seasons, they do not appear to adversely influence on-field performance once athletes return to competition.
The recurrence rate of shoulder dislocations in soccer athletes was 18%, which was lower than previously reported rates of 24% and 35% in German and Brazilian professional athletes, respectively.20,23 This discrepancy may reflect methodological differences, as the present study relied on a game-availability dataset that may not include redislocations occurring during the offseason or not resulting in missed playing time. Cohort composition also varied; prior studies included more homogeneous cohorts and included second- and third-division athletes as well. Notably, within our cohort, younger age was associated with increased risk, with athletes 25 years or younger demonstrating a higher recurrence rate of 26%. Recurrence rates were similar between athletes managed surgically and nonoperatively; however, the timing of recurrence differed with mean intervals of 3.8 years and 1.4 years, respectively. This may suggest that surgical stabilization can provide greater durability, potentially delaying recurrence even if the risk is not eliminated. It is important to note that the revision rate was 14%, whereas 8.3% of those treated nonoperatively ultimately underwent surgery. Thus, the decision to pursue early surgical stabilization should carefully balance the potential benefits against the risk of subsequent procedures.
In our study, 60% of soccer athletes underwent primary surgical intervention, encompassing nearly all goalkeepers (87%) and approximately half of outfield players (52%). This reflects important positional differences in treatment decision-making. As goalkeepers depend heavily on full, reliable shoulder function, persistent instability or limitations may have greater implications for performance and career, likely prompting surgical intervention. Several studies have evaluated surgical outcomes in this population. Terra et al 25 reported on 12 Brazilian professional goalkeepers who underwent arthroscopic capsulolabral repair, demonstrating excellent or good Rowe scores in 80% of acute cases and 57.2% of recurrent cases at a mean follow-up of 3.8 years. Similarly, Castagna et al 4 assessed 9 elite Italian goalkeepers who underwent surgery (8 arthroscopic capsuloplasties and 1 open Latarjet) for isolated anterior instability. The authors noted a 90% subjective return to the same level of play and mean times of return to training and full sport of 105 and 150 days, respectively, although 4 goalkeepers reported residual symptoms of apprehension or pain postoperatively. 4 Broader outcomes across player positions were examined by Alentorn-Geli et al, 3 who evaluated 57 Spanish competitive soccer athletes undergoing arthroscopic capsulolabral repair. At a minimum 5-year follow-up, the authors reported an 86% RTP rate, with 73% returning to the same preinjury level and 11% sustaining traumatic redislocations. 3 Reasons for not returning to play were personal and not related to shoulder function. 3 Clinical outcomes were excellent, with median Rowe and shortened Disabilities of the Arm, Shoulder and Hand scores of 80 and 2.3, respectively. 3 Open bone-block procedures also demonstrate favorable results in select high-demand outfield athletes. Stirma et al 24 evaluated 10 professional Brazilian players treated with the open Latarjet procedure for recurrent anterior instability. At a mean follow-up of 3.4 years, all athletes returned to play (100%) at a mean of 94 days, with restoration of range of motion, no complications, and no recurrent instability. 24 These studies suggest that both arthroscopic stabilization and the Latarjet procedure provide high RTP rates and improved outcomes in appropriately selected soccer athletes.
Nonoperative management remains an important first-line approach prior to surgical intervention and is generally indicated for first-time anterior dislocations in low-risk athletes without substantial bony defects. Conti et al 5 evaluated conservatively treating 20 in-season competitive outfield players with a first-time anterior glenohumeral dislocation, using a dynamic shoulder brace and a structured 40-day rehabilitation program. All players underwent magnetic resonance imaging and computed tomography to exclude rotator cuff pathology and glenoid bone loss exceeding 25%. 5 The authors reported that all players returned to training at approximately 40 days, with 90% reporting no pain, discomfort, or instability symptoms. 5 Conservative management failed in 2 athletes, with both subsequently undergoing a Latarjet procedure: 1 with a bony Bankart lesion involving 23% of the glenoid had a traumatic recurrence at 50 days postinjury, and 1 with a large capsular rent had an early subluxation episode at 45 days postinjury. 5 These findings suggest that structured conservative management may permit in-season return in carefully selected athletes.
Overall, the management of shoulder instability in soccer athletes should be individualized, considering player position, timing within the season, degree of instability, presence of bony defects, and career implications. While surgical stabilization can offer reliable outcomes, particularly in goalkeepers and recurrent cases, nonoperative treatment may enable selected outfield athletes to complete the season safely. In fact, our study found that field time and performance metrics were comparable between athletes treated surgically and those managed nonoperatively, both in the overall cohort and across player positions. The present study is limited by the lack of detailed surgical reports; however, the literature underscores the importance of tailoring treatment strategies to the specific demands, risk profiles, and competitive circumstances of each athlete.
Prevention strategies have been used to reduce the risk and severity of upper extremity injuries among soccer athletes. In 2016, Ejnisman et al 8 developed a dedicated shoulder injury prevention program for soccer, named FIFA 11+ Shoulder (FIFA 11+S), designed to improve core stability, neuromuscular control, local muscular endurance, eccentric rotator strength, and agility. The FIFA 11+S program consists of 3 progressive phases: (1) a general warm-up; (2) exercises to develop strength and balance of the shoulder, elbow, wrist, and finger muscles; and (3) exercises for core stability and muscle control. 8 The FIFA 11+S takes 20 to 25 minutes to complete and is recommended to be practiced 3 times per week. 8 Al Attar et al 2 sought to assess the effectiveness of the FIFA 11+S program and conducted a single-blinded randomized control trial of 726 goalkeepers who were randomized to either the FIFA 11+S group (n = 360) performing the program before all training sessions for 1 season (6 months) or a control group continuing their usual warm-up routine. The authors demonstrated that implementing the FIFA 11+S program reduced upper extremity injury incidence among goalkeepers by approximately 68%, including reductions in contact, noncontact, initial, recurrent, and overuse injuries, as well as injuries of minor and moderate severity. 2 Given the demonstrated efficacy of the FIFA 11+S for upper extremity injury reduction, we recommend expanding its use beyond goalkeepers and incorporating it into training warm-ups for all soccer athletes, including outfield players.
Our study has several limitations inherent to retrospective, database-driven designs. First, injury identification relies on a publicly available online database, and despite methods to cross-reference and verify injuries, the lack of access to official medical records introduces potential selection and misclassification bias. Excluding shoulder injuries without sufficient diagnostic detail may have omitted true dislocations or subluxations, and incomplete reporting on treatment methods raises a small risk of misclassifying surgically treated athletes as nonoperative. Second, detailed information on injury severity, imaging findings (eg, labral pathologies, glenoid bony defects, Hill-Sachs lesions), surgical techniques (open vs arthroscopic, with or without the use of bone augmentation), and rehabilitation protocols was not available, limiting assessment of factors that could influence outcomes. Third, recurrence and RTP estimates may be affected by injuries occurring outside official league and match availability records, as well as by players retiring or transferring outside the top 5 leagues. Additionally, any study involving professional athletes carries an inherent risk of bias, as these individuals are financially and personally motivated to return to play and are thus unlikely to be directly generalizable to the greater population of nonathletes or lower-level athletes. Contract structures in European soccer leagues often include guaranteed contracts with defined durations, which may also influence RTP decisions. Despite these limitations, our matched-cohort study provides objective, systematically derived data on RTP, recurrence, field time, and performance using one of the largest publicly trackable cohorts of elite soccer athletes with shoulder dislocations, providing sports medicine specialists with valuable evidence in an area of elite soccer injury management that remains understudied.
Conclusion
RTP following shoulder dislocations in elite professional soccer athletes was high, with 87% returning to the same level within 2 seasons. Injured athletes missed a median of 68 days and 10 games. The recurrence rate was 18%, occurring at a mean of 2.6 years. Although field time was reduced during the index season and the 2 seasons after RTP, player performance remained comparable to that of matched controls across all positions. Surgically treated players missed more time initially, but long-term RTP rates, performance outcomes, and recurrence were similar to those treated nonoperatively. Future studies are warranted to better identify factors influencing RTP and recurrence and to optimize treatment and rehabilitation strategies for elite soccer players.
Footnotes
Final revision submitted March 9, 2026; accepted March 20, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: X.L. is a paid consultant and receives royalties from FH Orthopaedics.
Ethical approval was not sought for the present study.