
Abstract
Background:
Adductor injuries are common in professional soccer, leading to prolonged recovery, compromised player performance, high recurrence rates, and variable outcomes despite advancements in injury prevention and management.
Purpose/Hypothesis:
This study aims to assess trends in return-to-play (RTP), reinjury rates, and performance effects in Major League Soccer (MLS) players. It was hypothesized that RTP times and performance metrics after adductor injuries vary by time period (2010-2015 vs 2016-2021) and player position, with changes in injury management influencing outcomes.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Adductor injuries in MLS players (2010-2021) were analyzed November 8, 2024, using the MLS Injury Surveillance database. All recorded injuries were included and cross-referenced with publicly available data. Injuries were compared across 2 time periods (2010-2015 vs 2016-2021). Injured players were matched 1:2 with noninjured controls by position, age, and MLS experience. RTP duration, reinjury rates, and pre- and postinjury performance metrics were evaluated by time period and player position. Independent t tests and chi-square tests were used to assess differences in RTP duration, reinjury rates, and injury rates. Multivariate regression was performed to identify predictors of RTP.
Results:
Between 2010 and 2021, a total of 1706 players with adductor injuries were identified. RTP times increased from 14.4 ± 10.1 days (2010-2015) to 19.7 ± 15.2 days (2016-2021; P = .0475). Multivariate linear regression identified significant predictors of prolonged RTP, including injury type, onset, and field surface. Compared with acute contact injuries, acute noncontact injurieswere associated with a 12.5-day shorter RTP (β = −12.50; P = .010) and chronic injuries with an 18.4-day shorter RTP (β = −18.44; P = .001). Osteitis pubis was associated with a 37.2-day increase in RTP duration compared with nonrupture injuries(β = 37.24; P = .007). Injuries occurring on grass were associated with a 9.6-day shorter RTP than those on artificial turf (β = −9.56; P = .010). Reinjury rates remained stable between the 2 time periods (21.14% vs 23.18%; P = .513). After injury, all player positions experienced declines in games played and minutes logged, with defenders exhibiting the most pronounced reductions.
Conclusion:
Adductor injuries in MLS athletes were associated with increasing RTP durations over time, with notable position-specific performance effects. Acute contact injuries had the longest RTP duration. RTP durations were significantly longer in 2016-2021 compared with 2010-2015, suggesting evolving trends in injury management. These findings underscore the need for individualized rehabilitation strategies tailored to player position and injury characteristics.
Adductor injuries are a significant concern in professional soccer, accounting for a substantial proportion of time-loss injuries in the sport. These injuries, often caused by high-intensity activities such as sprinting, cutting, and kicking, can result in prolonged recovery periods and reduced athletic performance.5,10 In Major League Soccer (MLS), the physical demands of play, combined with a competitive schedule, make the prevention, management, and rehabilitation of adductor injuries a critical area of focus for sports medicine teams.3,28
Despite advancements in training and injury prevention strategies, adductor injuries remain prevalent, with high rates of recurrence reported in elite athletes.21,26 The complex anatomy and biomechanical role of the adductor muscle group in stabilization and force transmission contribute to the challenges of injury prevention and recovery. 1 Furthermore, the variability in injury mechanisms—ranging from acute contact injuries to chronic overuse—complicates the development of standardized treatment protocols.6,17 Evidence suggests that functional asymmetries, insufficient core strength, and inadequate preseason conditioning are critical contributors to adductor injury risk, underscoring the need for targeted prevention strategies.4,29
Return-to-play (RTP) duration, postinjury performance, and reinjury rate are important measures of recovery from an adductor injury in a professional soccer player. 20 Each of these is multifactorial, as RTP duration is affected by the severity of the injury, the position of the athlete, the time in the season, potentially the player’s contract status, and where the team is in the standings. Understanding the factors influencing RTP and postinjury performance is essential for optimizing outcomes in professional soccer players.
This study aims to provide a comprehensive analysis of adductor injuries in MLS athletes over a 10-year period, focusing on injury rates, RTP durations, reinjury rates, and postinjury performance across different playing positions. By comparing 2 time periods, 2010-2015 and 2016-2021, this study also seeks to identify temporal trends in injury management and recovery. Additionally, it evaluates the positional effect of adductor injuries on key performance metrics, contributing to a growing body of evidence aimed at improving rehabilitation strategies and reducing reinjury risk.7,28 We hypothesized that RTP durations and postinjury performance metrics after adductor injuries in MLS players vary by time period and player position, with evolving injury management strategies contributing to changes in outcomes.
Methods
This retrospective cohort study analyzed MLS athletes who sustained adductor injuries between 2010 and 2021. Adductor injuries were defined as those requiring medical intervention and affecting the adductor muscle group, as recorded in the MLS Injury Surveillance database. Injury diagnoses were made by the team physician for each of these players. The study aimed to evaluate injury rates, RTP durations, reinjury rates, and postinjury performance metrics across 2 periods: 2010-2015 and 2016-2021.
Players with adductor injuries were identified through the MLS Injury Surveillance database, which compiles injury data across all MLS teams. A systematic approach was used November 8, 2024, to extract and analyze player performance data using Microsoft Power Automate. Player-specific identifiers, including age, team affiliation during the injury year, and positional designation, were used as inputs to automate the blinded retrieval of performance metrics. Baseline performance was operationally defined as statistics recorded during the season immediately preceding the injury year, whereas postinjury performance data encompassed all available metrics after the injury event. Data were sourced from the publicly accessible MLS database (MLSsoccer.com/stats). Extracted performance parameters included total games played, average minutes per game and per season, goals scored, assists, shutouts, and goals conceded.
Inclusion criteria required players to have participated in at least 1 full MLS season before their injury and at least 1 full season after their RTP. For reinjury analysis, each player was included only once for their first injury. Noninjured controls were selected from the same database in a 2:1 ratio, matched to injured players by age (±2 years), playing position, years of MLS experience (±1 year), and season (±1 year). This matching ensured balanced cohorts for analysis. The final cohort consisted of 1706 injured players paired with 3412 noninjured controls.
Pre- and postinjury performance metrics were collected by 2 authors (F.H. and C.H.), including games played, minutes played, goals scored, assists, clean sheets, and goals conceded. Metrics were analyzed by player position (forwards, midfielders, defenders, and goalkeepers) to assess position-specific effects of adductor injuries on performance. Player performance outcomes at 1, 2, and 3 seasons postinjury were evaluated relative to baseline metrics collected during the season before the index injury year. RTP was defined as the time (in days) from injury to return to competitive match play. Reinjury was defined as any subsequent adductor injury occurring within 2 years of RTP on the same side of the body (laterality), as recorded in the league’s database. Although specific imaging or diagnostic confirmation of the exact muscle was not available, injuries were considered reinjuries if they involved the same laterality and occurred within the defined timeframe. Injury rate was calculated by dividing the number of players with adductor injuries in a given year by the total number of MLS players that year.
Injury rates, RTP durations, and reinjury rates were compared between the 2 cohorts (2010-2015 vs 2016-2021) using independent t tests for continuous variables and chi-square tests for categorical variables. Comparisons of pre- and postinjury performance metrics between injured players and controls were conducted using independent t tests for normally distributed variables. Continuous variables were expressed as mean ± standard deviation.
A multivariate linear regression model was used to assess the association between RTP duration and independent variables, including player position (forwards, midfielders, defenders, goalkeepers), injury type (nonrupture, ruptured, osteitis pubis), injury onset (acute contact, acute noncontact, chronic), field type (artificial turf, grass), weather conditions (clear/sunny, rainy/cloudy), and injury period (2010-2015 vs 2016-2021).
Nonrupture injuries were defined as avulsion, bursitis, contusion, fatigue, hematoma, general soreness, general tightness, irritation, inflammation, pain, spasm, sprain, strain, swelling, tendinosis, tendinopathy, and tendonitis.
Regression coefficients (β), standard errors, P values, and 95% CIs were reported. Statistical significance was set at P < .05. All analyses were performed using Stata (Release 17, StataCorp).
Results
From 2010 to 2021, 1706 players diagnosed with adductor injuries were identified and paired with 3412 noninjured control subjects for analysis. Athletes injured between 2010 and 2015 (n = 850) had a mean RTP of 14.4 days, whereas those injured between 2016 and 2021 (n = 856) returned after a mean of 19.7 days (P = .0475). The type of playing surface did not significantly affect RTP duration. Athletes injured on grass (n = 1204) had a mean RTP of 15.9 days, whereas those injured on artificial turf (n = 226) had a mean RTP of 20.3 days (P = .2271). No significant difference in RTP times was found based on player position. Midfielders (n = 430) had a mean RTP of 14.9 days, forwards (n = 247) 14.5 days, and defenders (n = 403) 14.9 days (P = .9947). RTP times varied nonsignificantly between competitive settings, with injuries sustained during games or matches (n = 575) resulting in a mean RTP of 17.9 days, compared with 15.6 days for injuries sustained during practice (n = 679; P = .216). Contact-related acute injuries (n = 113) had the longest RTP at 27.6 days, whereas acute noncontact injuries (n = 1665) had a mean RTP of 17.4 days. Chronic or gradual noncontact injuries (n = 758) had the shortest RTP at 14.9 days (P = .0648), demonstrating a trend toward significance.
RTP times did not significantly differ based on the game location of the injury. Athletes injured at home (n = 290) had a mean RTP of 18.5 days, whereas those injured away (n = 239) had a mean RTP of 14.3 days (P = .2010). Younger athletes (≤25 years; n = 657) had comparable RTP of 19.0 days compared with older athletes (>25 years; n = 843), who averaged 15.4 days for RTP (P = .1774). The specific in-game time at which the injury occurred did not significantly affect RTP. Injuries occurring within the first 30 minutes (n = 163) had a mean RTP of 18.6 days, compared with 21.3 days for injuries in the second 30 minutes (n = 64) and 16.7 days for injuries occurring in the final 30 minutes (n = 85) of play (P = .9187). The discrepancy in total numbers (n = 1706) reflects incomplete game time data available for certain players, which should be considered as a limitation of this analysis. Weather conditions at the time of injury were not associated with significant differences in RTP times. Injuries sustained in sunny or clear conditions (n = 1249) resulted in a mean RTP of 16.3 days, whereas injuries in rainy or snowy conditions (n = 65) had an RTP of 15.6 days (P = .9079). All the aforementioned data are shown in Table 1.
Return-to-Sport Time in MLS Athletes With Adductor Injuries Between 2010-2021 a
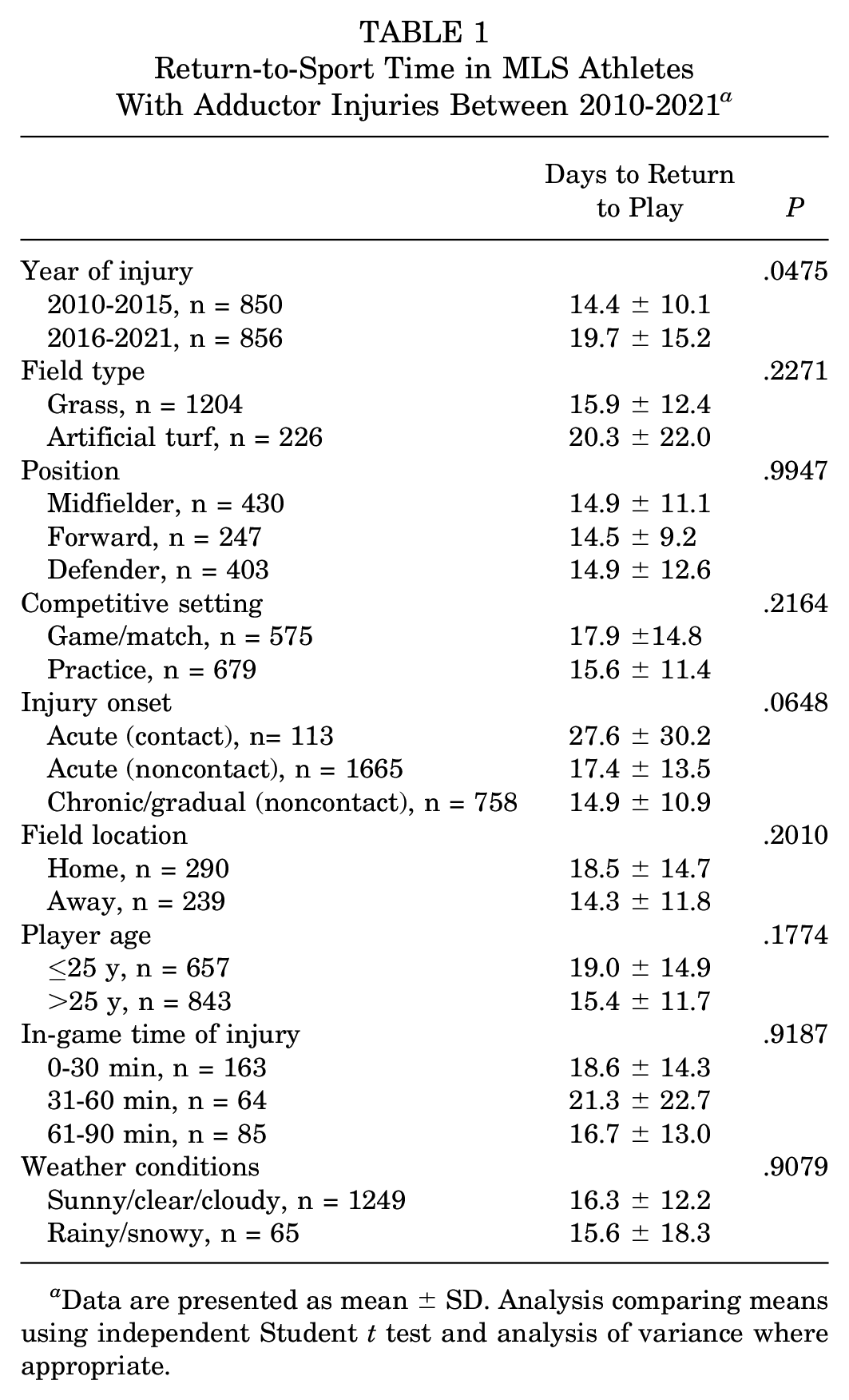
Data are presented as mean ± SD. Analysis comparing means using independent Student t test and analysis of variance where appropriate.
Results of analysis of injury rate and reinjury rate are shown in Table 2. A nonsignificant reduction in injury rates was observed between the 2 periods, with a rate of 18.0% in the 2010-2015 cohort and 15.18% in the 2016-2021 cohort (P = .165). A significant increase in RTP duration was observed over time, with athletes injured in the 2010-2015 cohort having a mean RTP of 13.98 ± 36.92 days, compared with 19.98 ± 44.53 days in the 2016-2021 cohort (P = .012).
Details Comparing 2010-2015 to 2016-2021 a

Data are presented as mean ± SD unless otherwise noted. RTP, return to play.
Reinjury rates were similar across the 2 periods, with a rate of 21.14% in the 2010-2015 cohort and 23.18% in the 2016-2021 cohort (P = .513). Additionally, time to RTP after a second injury trended longer in the 2016-2021 cohort (16.34 ± 27.53 days) compared with the 2010-2015 cohort (12.18 ± 24.17 days), although this difference did not reach statistical significance (P = .084). These findings suggest that although there had been a modest decline in overall injury rates, athletes in the more recent cohort took longer to return to play after their injuries, with no significant changes observed in reinjury rates over time.
Statistically significant predictors of RTP duration included injury type, injury onset, and field type. Compared with players who had nonruptured injuries, players diagnosed with osteitis pubis had significantly longer RTP durations (β = 37.24; 95% CI, 9.97 to 64.51; P = .007). Injury onsetalso influenced RTP, with acute noncontact injuries associated with a 12.50-day shorter RTP (β = −12.50; 95% CI, −21.95 to −3.04; P = .010), and chronic injuries with an 18.44-day shorter RTP (β = −18.44; 95% CI, −28.32 to −8.56; P = .001), both relative to acute contact injuries. Players injured on grass returned to play significantly faster than those injured on artificial turf (β = −9.56; 95% CI, −16.85 to −2.28; P = .010).
Other variables, including player position (midfielders: β = 3.10, P = .391; defenders: β = 2.23, P = .539; goalkeepers: β = −3.95, P = .497), weather conditions (β = 0.48, P = .882), age (β = −0.16, P = .577), and injury period (2016-2021 vs 2010-2015: β = 0.42; 95% CI, −5.70 to 4.86; P = .875) were not statistically significant predictors of RTP, as shown in Table 3.
Multivariate Analysis on Factors Affecting Return to Play a

Ref, reference group in multivariate model.
Nonrupture includes avulsion, bursitis, contusion, fatigue, hematoma, general soreness, general tightness, irritation, inflammation, pain, spasm, sprain, strain, swelling, tendinosis, tendinopathy, tendonitis.
Forwards who sustained adductor injuries showed minimal effect on games played and other performance metrics over the observed periods. No significant differences were found in games played per season between injured and control groups in the index year, 1 year postinjury (P = .918), and 3 years postinjury (P = .657). However, 2 years postinjury, forwards with adductor injuries played fewer games than controls (−2.63 ± 7.99 vs −0.44 ± 7.59; P = .028), indicating a possible delayed effect of adductor injuries on participation. Minutes played, goals per season, and assists per season showed no significant differences between injured forwards and controls, shown in Table 4.
Forward Metrics Compared With 1 Year Before Index Year a
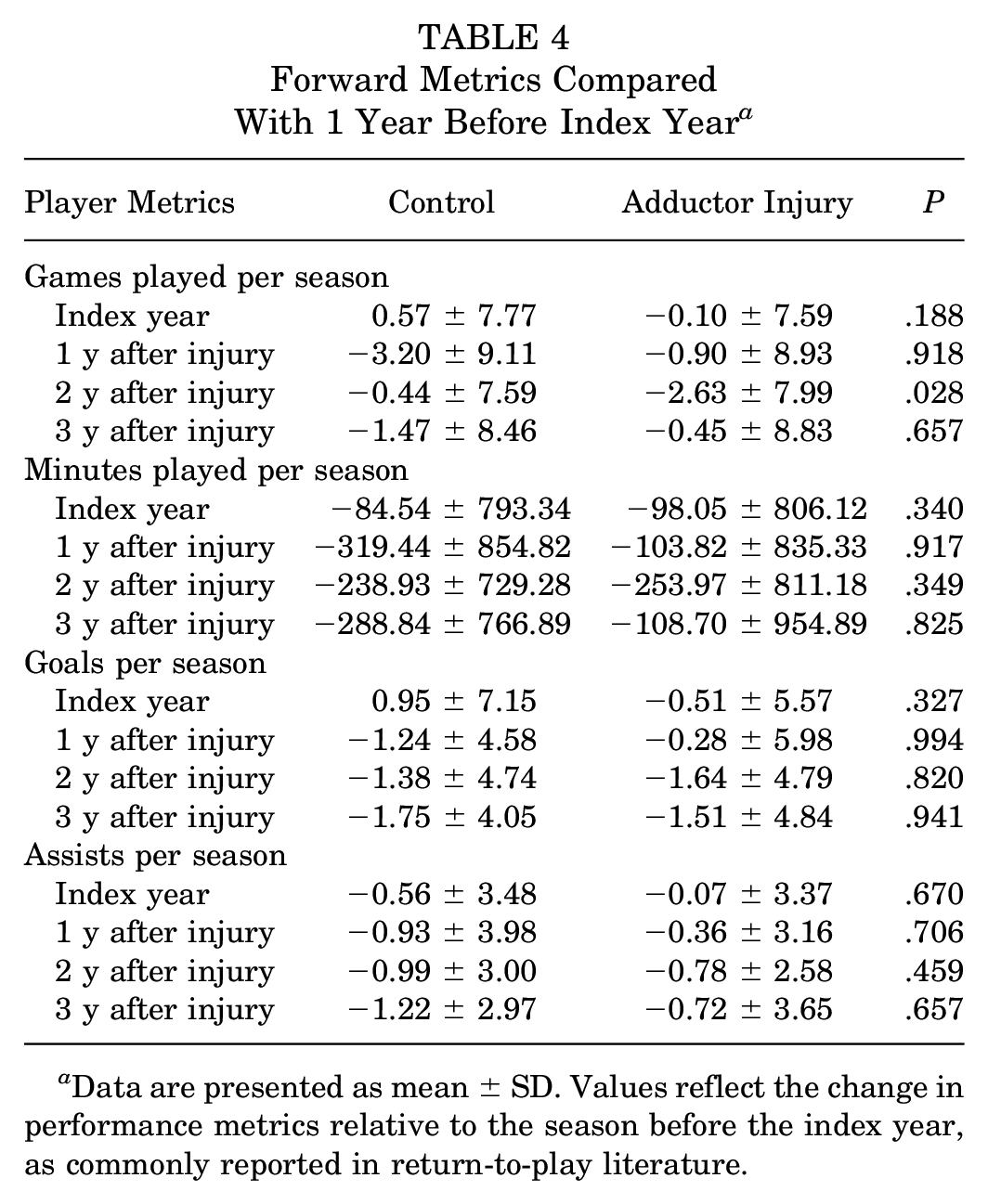
Data are presented as mean ± SD. Values reflect the change in performance metrics relative to the season before the index year, as commonly reported in return-to-play literature.
Midfielders exhibited a notable reduction in games played after adductor injuries. Injured midfielders played significantly fewer games 1 year postinjury (−2.35 ± 8.81) compared with controls (0.36 ± 8.23; P = .004). This trend continued into the second year postinjury, although not reaching statistical significance (P = .063). Minutes played per season for midfielders were significantly reduced in the index year (P = .049), 1 year postinjury (P= .002), and 2 years postinjury (P = .037) compared with controls, reflecting a sustained decrease in game involvement. Additionally, midfielders scored fewer goals in the first (P = .044) and second years postinjury (P = .031) and recorded fewer assists 2 years (P = .044) and 3 years postinjury (P = .039); further details are shown in Table 5.
Midfielder Metrics Compared with 1 Year Before Index Year a

Data are presented as mean ± SD. Values reflect the change in performance metrics relative to the season before the index year, as commonly reported in return-to-play literature. Boldface indicates statistical significance.
Defenders experienced the most pronounced reductions in performance after adductor injuries. Games played per season were significantly lower for injured defenders compared with controls in the index year (−0.60 ± 7.99 vs 1.21 ± 7.74; P = .015), 1 year postinjury (−2.58 ± 8.51 vs 0.98 ± 8.29; P = .001), and 2 years postinjury (−2.37 ± 8.87 vs 0.37 ± 8.56; P = .003). Similarly, injured defenders logged significantly fewer minutes than controls in the index year (−53.33 ± 770.28 vs 111.13 ± 739.33; P = .003), 1 year postinjury (−246.74 ± 781.97 vs 66.5 ± 797.77; P = .001), and 2 years postinjury (−254.01 ± 806.55 vs 3.16 ± 792.29; P = .001). Goals per season were notably lower for injured defenders 1 year postinjury (−0.22 ± 1.04 vs 0.07 ± 1.24; P = .013), although differences in subsequent years were not statistically significant. Assists per season were also significantly reduced in the index year for injured defenders (−0.18 ± 1.69 vs 0.22 ± 1.98; P = .048), as shown in Table 6.
Defender Metrics Compared with 1 Year Before Index Year a

Data are presented as mean ± SD. Values reflect the change in performance metrics relative to the season before the index year, as commonly reported in return-to-play literature. Boldface indicates statistical significance.
Goalkeepers demonstrated a temporary reduction in performance metrics after adductor injuries. Injured goalkeepers played significantly fewer games 1 year postinjury (−4.18 ± 7.19) compared with controls (0.56 ± 10.24; P = .033). Minutes played per season were also significantly lower for injured goalkeepers at one year (−383.18 ± 660.07) than controls (48.50 ± 923.57; P = .031). Injured goalkeepers recorded fewer clean sheets 1 year postinjury (−2.59 ± 3.59) compared with controls (−0.53 ± 3.81; P= .044), suggesting a short-term effect on defensive performance. However, no statistically significant differences were observed between groups in games played, clean sheets, or goals conceded in the index year or in subsequent years, as shown in Table 7.
Goalkeeper Metrics Compared with 1 Year Before Index Year a
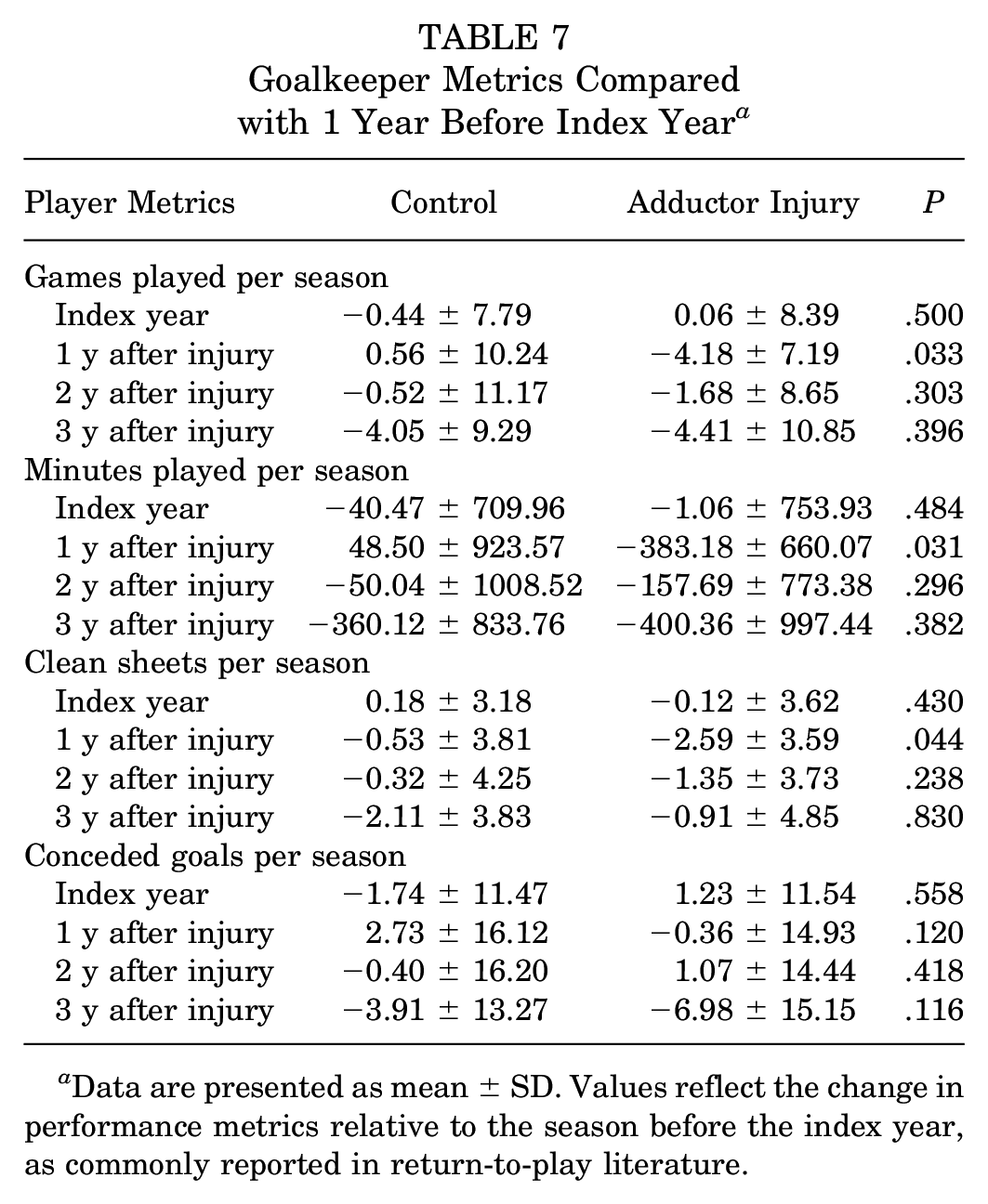
Data are presented as mean ± SD. Values reflect the change in performance metrics relative to the season before the index year, as commonly reported in return-to-play literature.
Discussion
This study provides a comprehensive analysis of adductor injuries in MLS athletes over a 10-year period, focusing on injury rates, RTP times, reinjury rates, and postinjury performance across different playing positions. Key findings from this study include a significant increase in mean RTP durations from 14.4 days (2010-2015) to 19.7 days (2016-2021; P = .0475), while reinjury rates remained statistically unchanged (21.14% vs 23.18%; P = .513). Multivariate analysis identified osteitis pubis (P = .007), acute noncontact onset (P = .010), chronic onset (P = .001), and grass surface (P = .010) as significant predictors of RTP duration. Position-specific performance outcomes showed that defenders and midfielders had the most sustained postinjury declines in games played and minutes logged, with defenders showing significant reductions up to 2 years postinjury (eg, games played difference 1 year postinjury: −2.58 ± 8.51 vs 0.98 ± 8.29; P = .001) and midfielders demonstrating significant reductions in goals (P = .044) and assists (P = .039) over multiple seasons. The findings highlight significant temporal trends in RTP durations, variability in performance effects by position, and the multifaceted nature of recovery after adductor injuries.
Return-to-Play Durations and Injury Trends
The significant increase in RTP durations from 2010-2015 (14.4 days) to 2016-2021 (19.7 days; P = .0475) may reflect evolving trends in injury management, rehabilitation protocols, or more conservative return-to-sport strategies in recent years. 5 This trend aligns with recent literature emphasizing the importance of comprehensive recovery to reduce reinjury risk in elite athletes.18,22,26 The reduction in overall injury rates, from 18.0% to 15.18%, was not statistically significant but may suggest potential advancements in injury prevention strategies, including prehabilitation and load management practices.10,12,20 Serner etal 20 reported a 1-year reinjury rate after return to sport after adductor injuries; however, we expanded the timeframe to 2 years in this study to capture as many reinjury cases as possible and provide a more comprehensive analysis.
The multivariate analysis identified significant predictors of RTP duration, highlighting the effect of injury type, onset, and playing surface on recovery times. Osteitis pubis was associated with the longest RTP duration (P = .007), a finding consistent with previous research demonstrating prolonged rehabilitation in athletes with groin-related pathologies.9,10,13 Injury onsetalso influenced RTP, with acute noncontact (P = .010) and chronic injuries (P = .001) resulting in significantly shorter RTP times compared with acute contact injuries, aligning with studies emphasizing the role of injury mechanism in recovery trajectories.3,18,19 Additionally, players injured on grass fields returned to play faster than those on artificial turf (P = .010), supporting evidence that playing surface can affect rehabilitation and injury outcomes.1,8 These findings suggest that injury mechanism and surface conditions may play a crucial role in rehabilitation timelines, emphasizing the need for tailored recovery protocols based on injury characteristics.
Reinjury Rates and Chronicity
Reinjury rates remained stable across the 2 cohorts (21.14% vs 23.18%; P = .513), underscoring the persistent challenge of preventing recurrent adductor injuries. 3 Acute contact injuries exhibited the longest RTP times (27.6 days), compared with acute noncontact and chronic injuries, potentially indicating greater severity or complexity of recovery for these injuries. This aligns with previous findings indicating that contact injuries are associated with more extensive tissue damage.16,27,28 Furthermore, the contribution of chronic injuries to reinjury risk underscores the importance of addressing underlying biomechanical and tissue-related factors during rehabilitation.11,13
Performance Effects by Position
The positional analysis revealed marked variability in postinjury performance effects. Defenders exhibited the most pronounced reductions in games played and minutes logged, with significant differences observed 1 and 2 years postinjury compared with controls. These findings are consistent with the high physical demands placed on defenders, particularly in terms of sprinting and directional changes, which heavily engage the adductor muscle group.24,28,29 In contrast, forwards and goalkeepers demonstrated less pronounced performance declines, likely reflecting differences in position-specific activity profiles.1,7
For midfielders, significant reductions in goals and assists in the first and second years postinjury highlight the potential for adductor injuries to affect technical performance metrics. This finding suggests that midfielders, who often rely on explosive lateral movements, change of direction, and endurance, may experience prolonged deficits in these domains despite returning to play.2,8,17
Comparison to Established Literature
The observed increase in RTP durations from 2010-2015 to 2016-2021, along with the stable reinjury rates, is consistent with trends reported in previous studies on muscle injuries in professional football. Ekstrand etal 5 noted similar findings, attributing longer RTP times to the adoption of more conservative rehabilitation approaches and the emphasis on reducing reinjury risk through comprehensive recovery strategies. Additionally, the variability in performance effects across player positions aligns with Verrall and colleagues’ 16 observations that defenders are disproportionately affected due to the high physical demands of sprinting and lateral movements, which heavily engage the adductor muscle group.21,26 The persistent challenge of reinjury prevention despite advancements in injury management highlights the complex interplay of biomechanical, physiological, and sport-specific factors, as emphasized by Weir etal 27 in their review of lower limb injuries. 9 These findings underscore the need for tailored, position-specific rehabilitation protocols to address the unique demands of professional soccer players.
Implications for Rehabilitation and Load Management
Recent anatomic studies have redefined the structural relationships of the adductor muscles and pubic ligaments, particularly with the identification of the pyramidal–anterior pubic ligament–adductor longus complex and the presence of conjoint tendons between the adductor brevis, adductor longus, and gracilis. These insights suggest that injury severity may be influenced by the specific ligamentous attachments involved, with disruptions to the inferior pubic ligament potentially leading to prolonged recovery and increased reinjury risk.14,15 Given the stabilizing role of these structures, rehabilitation strategies should consider not only muscle strengthening but also targeted approaches addressing the ligamentous contributions to adductor function. Acknowledging these anatomic complexities may help refine interpretations of injury severity, optimize RTP timelines, and reduce reinjury rates in professional soccer players.
The observed increases in RTP durations suggest that extended recovery times may not fully mitigate performance declines, particularly in physically demanding positions such as defenders and midfielders. These findings highlight the importance of individualized rehabilitation protocols tailored to position-specific demands.21,22 Integrating strength, endurance, and proprioception training into rehabilitation may help optimize recovery and reduce reinjury risks.6,9,19 The findings underscore the need for targeted rehabilitation strategies tailored to position-specific demands and injury characteristics. Continued emphasis on prevention, individualized recovery protocols,4,12,18 and reinjury mitigation strategies will be essential in optimizing outcomes for elite soccer players.23,25
Limitations
This study has several limitations that should be considered when interpreting the findings. First, the retrospective design inherently relies on the accuracy and completeness of the MLS Injury Surveillance database, which may introduce reporting bias. Another limitation of this study is the incomplete game time data for certain players, which may have affected the analysis of injury timing and its effect on RTP outcomes, potentially introducing bias or reducing the generalizability of the findings. Injuries that were minor or did not require medical intervention may have been underreported, potentially skewing the injury rates and performance metrics.
Another limitation of this study is the lack of access to biomechanical or imaging data, such as magnetic resonance imaging–based grading of injuries, which could provide greater insight into injury severity and structural damage. Due to the lack of imaging or specific diagnostic data, we were unable to confirm whether reinjuries involved the same adductor muscle. Reinjury designation was based on laterality and timing, which may have included new injuries to different muscles within the adductor group.Additionally, the absence of player-reported outcomes limits our ability to assess subjective functional recovery. Furthermore, potential survivor bias must be considered, as our analysis of postinjury performance metrics excludes players who were unable to achieve RTP, potentially underestimating the long-term effect of more severe adductor injuries.
Although RTP duration provides an objective metric, it does not capture the full scope of recovery or readiness for high-level competition. The study grouped adductor injuries into broad categories (acute contact, acute noncontact, and chronic), which may oversimplify the diverse mechanisms and severities of these injuries. More granular categorization based on specific anatomic or functional deficits might yield a deeper understanding of their effect on performance. The use of noninjured controls matched by position, age, and experience helps mitigate confounding factors, but we did not account for other variables such as training load, fitness level, and team-specific medical practices. These factors could influence both injury risk and recovery outcomes, leading to unmeasured confounding.
Importantly, RTP decisions were made by individual team physicians, and RTP criteria likely varied across teams and over time. The heterogeneity in rehabilitation protocols and medical oversight across MLS franchises further limits the ability to draw uniform conclusions about recovery timelines and reinjury risk.
Last, this study focused solely on MLS players, limiting the generalizability of findings to other populations, such as amateur players or athletes in different sports. Differences in playing conditions, medical resources, and rehabilitation protocols across leagues may result in varying outcomes. Future studies addressing these limitations by incorporating prospective designs, biomechanical data, and subjective recovery metrics could enhance the understanding of adductor injury mechanisms, improve prevention strategies, and optimize rehabilitation protocols.
Conclusion
Our study demonstrates that adductor injuries in MLS athletes were associated with increasing RTP durations over time, with notable position-specific performance effects. Acute contact injuries had the longest RTP duration. RTP durations were significantly longer in 2016-2021 compared with 2010-2015, suggesting evolving trends in injury management. These findings underscore the need for individualized rehabilitation strategies tailored to player position and injury characteristics.
Footnotes
Final revision submitted April 7, 2025; accepted April 25, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.F. has received consulting fees from Stryker. K.B. has received consulting fees from Xiros Inc, DePuy Synthes Products, and Medical Device Business Services; hospitality payments from Arthrex Inc and International Life Sciences; and support for education from Medinc of Texas. K.M. has received consulting fees from Arthrex and Anika Therapeutics, Inc. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.