
Abstract
Background:
Calcific tendinitis of the shoulder is a common, painful rotator cuff disorder with both nonoperative and operative treatment options. The optimal nonoperative modality remains unclear, and it is not well understood how previous nonoperative treatments influence eventual surgical outcomes.
Purpose/Hypothesis:
The purpose of this study was to compare success rates, defined as avoidance of surgery, among 3 nonoperative treatments for calcific tendinitis: physical therapy (PT), corticosteroid injection (CSI), and ultrasound-guided barbotage (USB). For patients who underwent surgery, outcomes were compared according to previous nonoperative management. It was hypothesized that success rates and postoperative outcomes would not differ significantly between modalities.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective review of patients diagnosed with calcific tendinitis from 2009 to 2023 was performed. Exclusion criteria were lack of radiographic confirmation, <6 months follow-up, or incomplete electronic medical record data. Patients were categorized by attempted nonoperative treatment (none, PT, CSI, USB, multiple) and by final management (nonoperative vs operative). Patient-reported outcomes included the visual analog scale (VAS), Subjective Shoulder Value (SSV), and range of motion (ROM), collected at initial and final presentation. Radiographic findings were extracted from radiology reports. Statistical testing used parametric or nonparametric methods as well as a multivariable Cox proportional hazards model to predict nonoperative failure. Significance was set at P < .05.
Results:
A total of 257 patients (mean age 55 ± 11 years) were analyzed with a mean follow-up of 18 ± 16 months with an overall nonoperative success rate of 63%. Success rates did not differ significantly among PT (59%), CSI (75%), and USB (72%), but patients with multiple tendon involvement or calcifications >3 cm were more likely to fail nonoperative management. Patients completing successful nonoperative management improved in VAS, SSV, and ROM, with no between-group differences. All patients who attempted multiple modalities (18/18; 100%) required surgery (P < .01). Among 121 patients undergoing surgery, final VAS, SSV, and ROM outcomes did not differ based on previous nonoperative management.
Conclusion:
PT, CSI, and USB demonstrate similar rates of avoiding surgery for calcific tendinitis. For patients ultimately requiring surgery, outcomes are not influenced by previous nonoperative management. Surgical intervention may be indicated after failure of a single nonoperative modality.
Calcific tendinitis of the shoulder is a common cause of shoulder pain, accounting for 7% of shoulder pain presentations, and is characterized by deposition of calcium within the tendons of the rotator cuff.4,22 Generally, affected patients are between 30 and 60 years old, 10 and though the etiology of calcium deposition remain unclear, the condition has been linked to diabetes, thyroid disease, and disorders of estrogen metabolism. 12 While calcific tendinitis may be asymptomatic or resolve without intervention, treatment with nonoperative or operative management is an option for painful and debilitating presentations.
First-line treatment for calcific tendinitis generally consists of nonoperative management including physical therapy (PT), corticosteroid injection (CSI), and/or ultrasound-guided barbotage (USB). When symptoms are refractory to nonoperative management, arthroscopic surgery is an option to remove the calcium with or without repair of the rotator cuff tendons. 23 Previous studies have demonstrated excellent outcomes after arthroscopic surgery for calcific tendinitis,3,20 with one study demonstrating an overall 92% success rate at 2-year follow-up. 19
While nonoperative management of calcific tendinitis has also been shown to result in excellent clinical outcomes,1,2 it remains unclear whether a particular nonoperative management modality is superior to others in terms of avoiding arthroscopic surgery. Further, for patients who ultimately require arthroscopic surgery, it remains unknown if choice of previous nonoperative management affects postsurgical outcomes. Therefore, we sought to compare the 3 most common nonoperative management modalities for calcific tendinitis performed at our institution: PT, CSI, and USB. The primary aim was to compare success rates, defined as avoidance of surgical intervention, for each nonoperative management modality. Secondarily, for patients who ultimately underwent surgery, subjective patient-reported outcomes (PROs) and objective clinical outcomes were compared based on the type of previous nonoperative management attempted (PT, CSI, or USB). We hypothesized that there would be no significant differences in success rates among nonoperative management modalities and that patients who underwent surgical intervention would demonstrate similar improvement in clinical outcomes and PROs regardless of previous nonoperative management modality.
Methods
Institutional review board approval was obtained for this retrospective cohort study from the University of Pittsburgh. We reviewed all patients diagnosed with calcific tendinitis and treated by 1 of 3 fellowship-trained orthopaedic sports medicine surgeons (B.P.L, M.R., A.L.) at our academic medical center between 2009 and 2023. Patients were included if they had radiographic confirmation of calcific tendinitis, ≥6 months’ follow-up, and complete demographic, clinical, and outcome data. Patients were excluded if they lacked a formal radiographic diagnosis, had incomplete data, or had <6 months' follow-up.
Demographic variables extracted from the medical record included sex, age at diagnosis, hand dominance, and comorbidities (body mass index, smoking status, diabetes, thyroid disease, vitamin D deficiency). Clinical outcomes included pain, assessed by the visual analog scale (VAS), Subjective Shoulder Value (SSV), and active range of motion (ROM). Forward flexion (FF) and external rotation (ER) were measured in degrees, and internal rotation (IR) was measured as the highest vertebral spinous process reached by the thumb, converted to a 0 to 15 numeric scale (0 = S1; 15 = T4).
All patients underwent standard shoulder radiographs (anteroposterior and lateral views). Images were interpreted by board-certified radiologists, and diagnostic reports were extracted from the electronic medical record. Calcification location was determined on lateral views. Calcification size was measured on anteroposterior views from the most medial to the most lateral aspect of the largest deposit, if multiple were present.
At our institution, no formal protocol exists for operative versus nonoperative management of calcific tendinitis. Shared decision-making was utilized between the treating surgeon and the patient to determine nonoperative management versus operative management. Patients were classified into 1 of 3 final management cohorts:
Nonoperative success: patients who attempted ≥1 nonoperative treatment (PT, CSI, or USB) and avoided surgery
Nonoperative failure: patients who attempted ≥1 nonoperative treatment but ultimately required surgery
Primary surgery: patients who underwent surgery without a trial of nonoperative treatment
Among patients who attempted nonoperative management, treatment modality was further categorized as having attempted PT, CSI, USB, or multiple modalities. We defined success as avoidance of surgery after nonoperative treatment and failure as progression to surgery after nonoperative treatment.
CSI was performed with an 18- or 22-gauge needle, depending on patient characteristics and provider preference. A mixture of 40 to 80 mg of triamcinolone, 2 mL of 1% lidocaine, and 2 mL of 0.25% bupivacaine was injected in the subacromial space of the affected shoulder. USB was performed with an 18- or 22-gauge spinal needle, depending on calcification characteristics and provider preference. The skin and deep tissues were anesthetized with buffered 1% lidocaine. Under ultrasound visualization, the calcification was fenestrated by multiple needle passes, and aspiration was attempted if the deposit appeared liquefied on ultrasound imaging. Corticosteroids were not administered adjunctively during USB attempts. Patients of the PT cohort were referred to therapists of their choosing, and no standardized protocol was prescribed.
For patients undergoing operative treatment, arthroscopic surgery was performed in the beach-chair position. Calcium deposits were completely excised, and tendon integrity was assessed. If excision resulted in a high-grade partial- (>50%) or full-thickness tear, concomitant rotator cuff tendon repair was performed. Postoperative rehabilitation consisted of short-term sling immobilization followed by progressive, supervised ROM and strengthening with a physical therapist.
Comparisons were made across nonoperative treatment subgroups (PT, CSI, USB, multiple modalities) and final outcome cohorts (nonoperative success, nonoperative failure, primary surgery). Normality was assessed visually with Q-Q plots, and statistical tests included chi-square, Fisher exact, independent t test, analysis of variance, Mann-Whitney U, and Kruskal-Wallis, as appropriate. A multivariable Cox proportional hazards model was utilized to estimate the association between patients’ demographic and calcification characteristics and nonoperative failure. The final multivariable model was validated using the log-likelihood ratio test and Cox-Snell residuals. Any post hoc analyses were performed with Tukey correction. Spearman rank correlation was used to assess the relationship between follow-up time and outcomes. All analyses were performed in R Version 4.5 (R Core Team) with statistical significance defined as P < .05.
Results
Cohort Overview
A total of 359 patients with calcific tendinitis were identified during the study period. After 63 patients were excluded for lack of radiographically confirmed calcific tendinitis, 28 for clinical follow-up <6 months, and 11 for missing SSV data at either the diagnostic visit or the final follow-up, a total of 257 patients were included in the final analysis.
Of the 257 patients, 217 (84%) attempted ≥1 nonoperative treatment modality: 64 received CSI, 74 received PT, 61 received USB, and 18 received multiple modalities. All patients in the CSI group received a single injection. In the USB group, 51 patients (84%) underwent 1 barbotage session and 10 patients (16%) underwent ≥2 sessions.
Of the 217 patients who attempted nonoperative treatment, 136 patients (63%) avoided surgery (nonoperative success) and 81 patients (37%) ultimately required surgery (nonoperative failure) (Figure 1). From the total of 257 patients, 40 (16%) underwent surgery without previous nonoperative treatment (primary surgery). In total, 121 patients (47%) underwent surgery (81 nonoperative failure + 40 primary surgery).

Patient selection flowchart. Initial exclusion criteria included patients without radiographically diagnosed calcific tendinitis (CT), insufficient follow-up time of ≥6 months from diagnosis if treated nonoperatively or from operation date if treated operatively, and missing or incomplete data in the medical record. Patients may have attempted corticosteroid injection (CSI), physical therapy (PT), ultrasound-guided barbotage (USB), multiple nonoperative modalities, or no nonoperative modalities. Patients were categorized based on their final outcome as primary surgery (no nonoperative modality was attempted), nonoperative failure (attempted nonoperative treatment but eventually underwent surgery), or nonoperative success (avoided surgery).
Demographics
Baseline demographics of operative versus nonoperative patients are presented in Table 1. The mean age at diagnosis was 55 ± 11 years. Patients managed nonoperatively were more likely to have involvement of the dominant side (59% vs 44%; P = .04). No other demographic variables differed significantly between operative and nonoperative cohorts (all P > .05). Within the nonoperative management subgroups (PT, CSI, USB, and multiple modalities), no significant demographic differences were identified (Table 2).
Demographic Data, Stratified by Final Management Disposition a

Data are presented as mean ± SD for continuous measures and n (%) for categorical measures. Bold value is significant at P < .05. BMI, body mass index.
Demographic Data, Stratified by Nonoperative Management Attempted a

Data are presented as mean ± SD for continuous measures and n (%) for categorical measures. A total of 217 of the 257 patients in this study attempted some form of nonoperative management. Significance was defined as P < .05. BMI, body mass index.
Calcification Characteristics
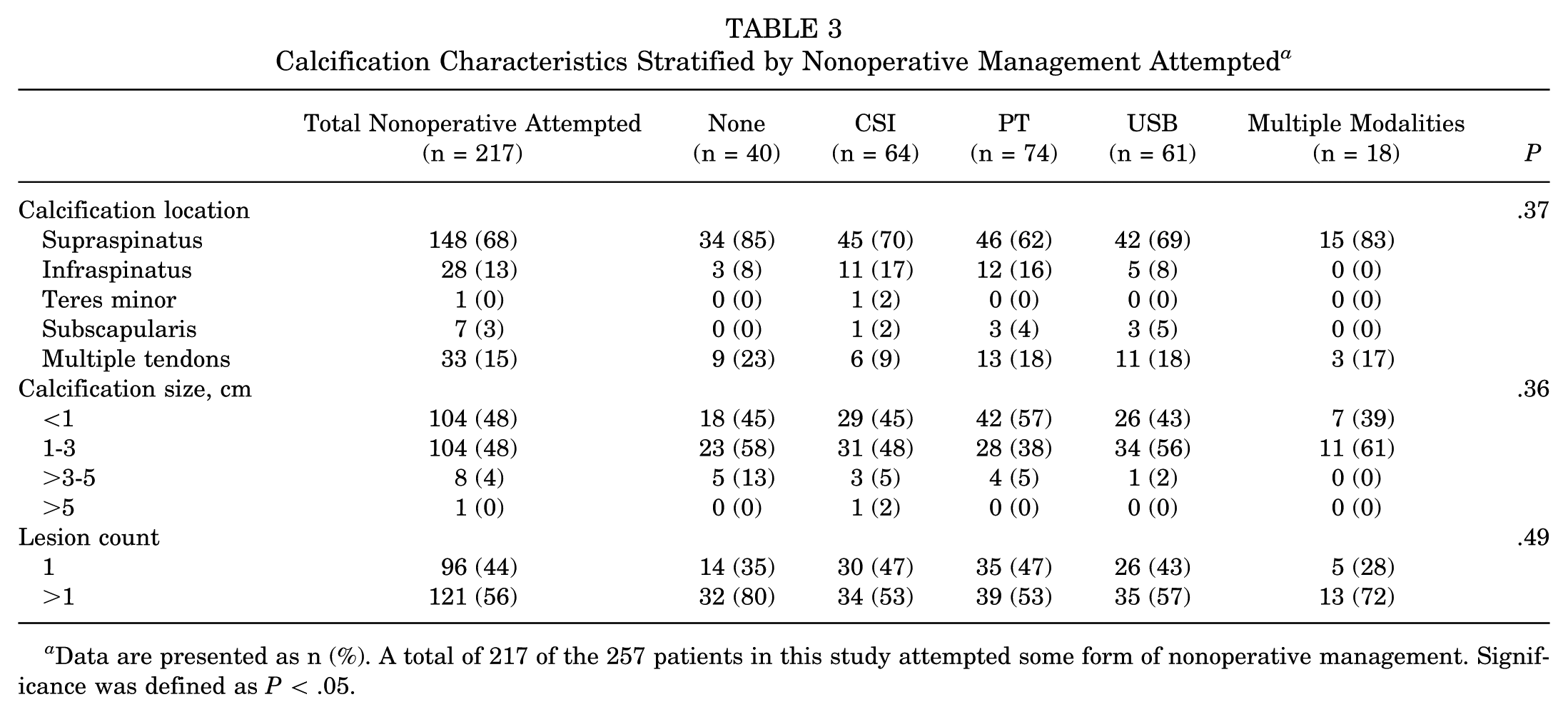
No significant differences in calcification location, size, or count were observed among the nonoperative treatment subgroups (PT, CSI, USB, and multiple) (all P > .05) (Table 3). When stratified by ultimate outcome (nonoperative success vs nonoperative failure vs primary surgery), Fisher exact test showed significant variation in calcification location (P = .03), size (P = .02), and count (P < .01) (Table 4). However, none of the post hoc pairwise comparisons remained significant after Tukey correction for multiple testing.
Relative Success Rates in Avoiding Surgery, Stratified by Nonoperative Treatment Modality Attempted a
Data are presented as n unless otherwise indicated. Bold value indicates significance at P < .05. CSI, corticosteroid injection; PT, physical therapy; USB, ultrasound-guided barbotage.
Calcification Characteristics Stratified by Nonoperative Management Attempted a

Data are presented as n (%). A total of 217 of the 257 patients in this study attempted some form of nonoperative management. Significance was defined as P < .05.
Calcification Characteristics Stratified by Nonoperative or Operative Management a

Data are presented as n (%). Bold values indicate significance at P < .05.
Success of Nonoperative Treatment
Among patients attempting nonoperative treatment (n = 217), there was no significant difference in success rates among PT (59%), CSI (75%), and USB (72%). Pairwise comparisons with absolute risk differences and 95% CIs are shown in Appendix Table A1. Patients who attempted multiple modalities were significantly more likely to undergo surgery compared with those who attempted a single modality (P < .01) (Table 5).
In a multivariable Cox proportional hazards model (Table 6), calcific tendinitis involving multiple tendons (hazard ratio [HR], 2.32; P = .03) and calcifications >3 cm in size (HR, 2.15; P = .04) were significant predictors for failure of nonoperative treatment. Neither modality of nonoperative treatment nor multiple USB attempts were significant predictors of failure of nonoperative treatment after adjustment for demographic and calcification characteristics.
Predictive Factors for Nonoperative Failure Based on Multivariable Cox Proportional Hazards Modeling a

Utilization of >1 nonoperative treatment modality perfectly predicted nonoperative failure and was therefore excluded from the model. Bold values indicate significance at P < .05. CSI, corticosteroid injection; PT, physical therapy; USB, ultrasound-guided barbotage.
Clinical Outcomes
Across all cohorts (primary surgery, nonoperative failure, and nonoperative success), all patients experienced significant improvement between diagnosis and final follow-up in VAS (–5.5 ± 3.2; P < .01), SSV (+26.3 ± 31.0; P < .01), and forward flexion (+16.5°± 44.8°; P < .01). Across all cohorts, there was no significant improvement in external rotation (+1.1°± 25°; P = .67) or internal rotation (+0.3 ± 4.7 vertebral levels; P = .50). At time of diagnosis, the nonoperative success cohort had significantly lower forward flexion (124°± 56°) than the primary surgery cohort (150°± 37°) and the nonoperative failure cohort (150°± 37°) (P < .01), as well as significantly lower external rotation (43°± 25°) compared with the primary surgery cohort (54°± 19°) and the nonoperative failure cohort (56°± 22°) (P < .01). However, by final follow-up, there were no significant differences in VAS, SSV, or ROM between the primary surgery, nonoperative failure, and nonoperative success cohorts (all P > .05) (Table 7).
Pre- and Postoperative Patient-Reported Outcomes and Range of Motion Values for All Cohorts a

Data are presented as mean ± SD. Bold values indicate significance at P < .05. Primary surgery: patients who attempted no nonoperative treatment modalities and proceeded directly to surgery. Nonoperative failure: patients who attempted nonoperative treatment but eventually underwent surgery. Nonoperative success: patients who attempted nonoperative treatment and did not undergo surgery. SSV, Subjective Shoulder Value; VAS, visual analog scale.
Within the nonoperative success cohort, there were no significant differences in VAS, SSV, or ROM across the PT, CSI, and USB subgroups at either baseline or follow-up (all P > .05) (Table 8). Within the nonoperative failure cohort, there were no significant differences in VAS, SSV, or ROM across the PT, CSI, USB, and multiple modality subgroups at either baseline or follow-up (all P > .05) (Table 9).
Pre- and Postoperative Patient-Reported Outcomes and Range of Motion Values for Patients of the Nonoperative Success Cohort, Stratified by Modality of Nonoperative Management a
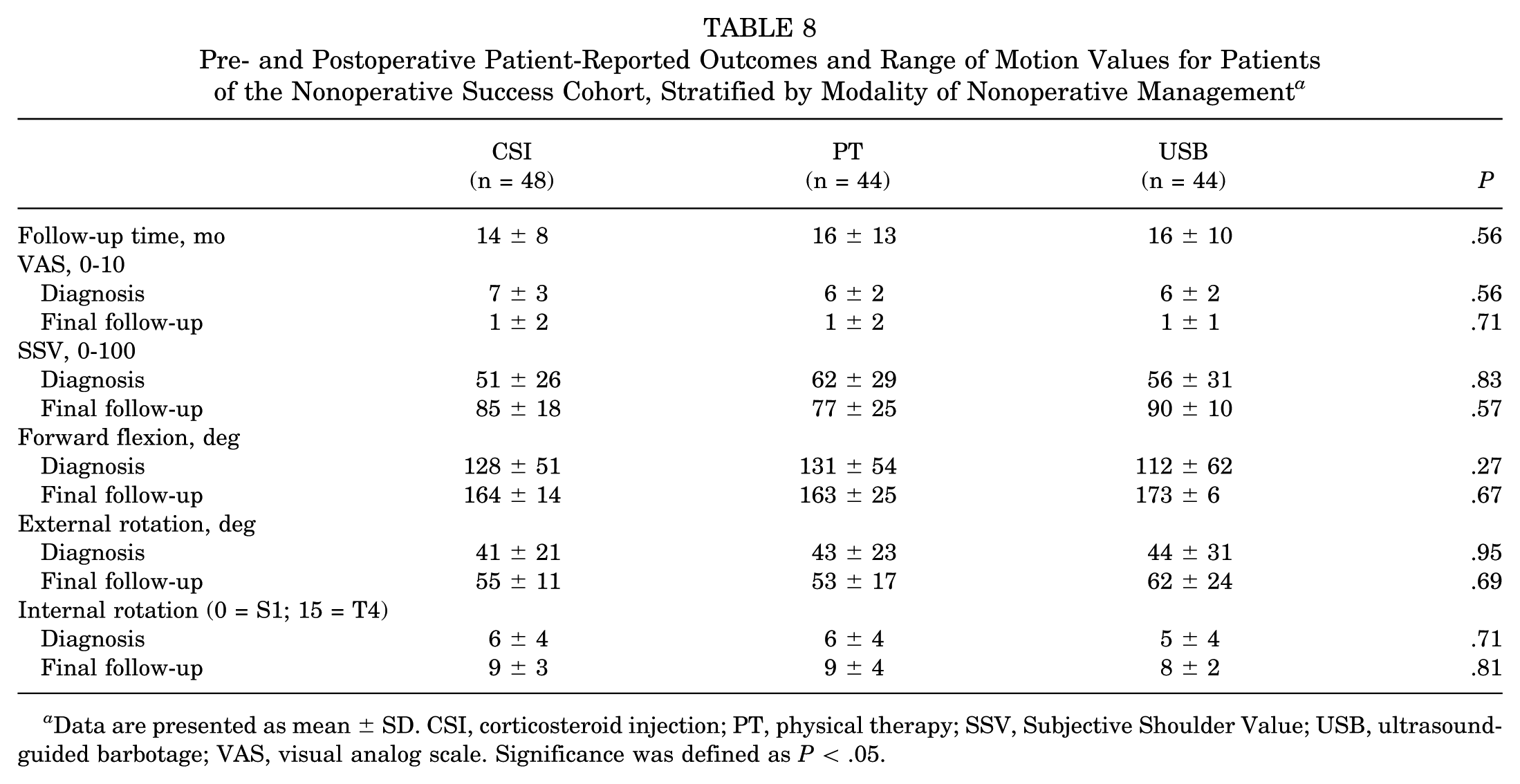
Data are presented as mean ± SD. CSI, corticosteroid injection; PT, physical therapy; SSV, Subjective Shoulder Value; USB, ultrasound-guided barbotage; VAS, visual analog scale. Significance was defined as P < .05.
Pre- and Postoperative Patient-Reported Outcomes and Range of Motion Values for Patients of the Nonoperative Failure Cohort, Stratified by Initial Nonoperative Management Attempted a

Data are presented as mean ± SD. CSI, corticosteroid injection; PT, physical therapy; SSV, Subjective Shoulder Value; USB, ultrasound-guided barbotage; VAS, visual analog scale. Significance was defined as P < .05.
Variable Follow-up Time
We accounted for variable follow-up time in a ranked correlation analysis. Spearman rank correlation coefficient was not statistically significant for any variable (VAS: ρ = 0.02, P = .41; SSV: ρ = 0.07, P = .22; FF: ρ = −0.25, P = .13; ER: ρ = −0.06, P = .21; IR: ρ = −0.01, P = .33), indicating that follow-up time was not significantly associated with any outcome in the available data.
Post Hoc Power Analysis
A post hoc power analysis showed that the power of detecting a significant difference in the reported success rate of avoiding surgery, if a difference in success rate exists, is 51% when comparing PT versus CSI, 7% when comparing CSI versus USB, and 35% when comparing PT versus USB.
Discussion
The most important finding of this study was that the overall success rate of nonoperative management for calcific tendinitis was 63%, with no significant differences among patients treated with PT, CSI, or USB. Patients of the nonoperative success cohort demonstrated significant improvements in PROs and ROM, and no single nonoperative treatment modality appeared superior. Furthermore, we found larger calcification size (>3 cm) and involvement of multiple tendons were found to be significant predictors of nonoperative failure. Among those patients of the nonoperative failure cohort, outcomes improved substantially regardless of the previous nonoperative modality attempted. A subset of patients elected to undergo surgery without a trial of nonoperative treatment. These patients were clinically similar to those who attempted nonoperative management, and their surgical outcomes were comparable with patients who failed nonoperative management. For patients with severe symptoms, reluctance to delay definitive intervention, or risk factors for nonoperative failure (eg, calcium deposits >3 cm or multiple tendon involvement), 11 primary surgery may represent a reasonable option.
An unexpected observation was that all patients who underwent multiple nonoperative management modalities ultimately proceeded to surgery. This pattern may reflect more refractory disease, although these patients did not differ in baseline pain or calcification characteristics compared with other nonoperative treatment modality groups. These findings suggest that switching between multiple nonoperative strategies may not provide additional benefit once an initial approach has failed. Rather, failure of an initial modality should prompt consideration of surgical intervention, as repeated trials of alternative therapies risk prolonging pain, delaying functional recovery, and postponing the definitive benefit that surgery can provide. Clinicians should therefore weigh the opportunity cost of extended nonoperative management against the potential advantages of earlier surgical treatment.
Our findings align with previous studies demonstrating favorable outcomes after nonoperative care for calcific tendinitis,6,16,24 though no consensus exists regarding the optimal modality or combination of modalities. 14 Much of the extant literature on nonoperative management of calcific tendinitis is of poor quality and high risk of bias, complicating definitive recommendations. 21 USB has recently received increased attention and has shown efficacy compared with extracorporeal shockwave therapy (ESWT) in meta-analysis,13,23 although we did not include ESWT in the present study. Some reports suggest USB may yield superior outcomes compared with PT and/or CSI,2,17 a finding not reproduced here. Conversely, de Witte et al 8 reported that concurrent administration of CSI with USB did not improve outcomes in a 5-year randomized trial. In contrast, patients in the present study underwent single modality sequentially rather than concomitantly.
Other nonoperative strategies, including nonsteroidal anti-inflammatory drugs and ROM exercises, have also demonstrated benefit in pain and functional scores. 6 Additionally, spontaneous recovery through resorption of calcium deposits has been described, potentially explaining similar improvements across groups in the current study. 7 Moosmayer et al 15 further supported this natural history, reporting equivalent outcomes between sham treatment and USB, with or without CSI. Taken together, these findings suggest that the natural course of calcific tendinitis plays a substantial role in patient recovery and that the specific choice of nonoperative modality may be less critical than previously thought. From a clinical perspective, these findings highlight the importance of setting appropriate expectations during shared decision-making and considering early transition to surgery when prolonged nonoperative management delays relief without altering eventual outcomes.
In recent years, much attention has been paid to the factors associated with failure of nonoperative management. Larger calcification size and multiple calcium deposits have been reported as predicting failure of nonoperative management, in line with our findings in the present study.9,11 Surgeons should consider the initial size and distribution of calcium deposits within the rotator cuff when deciding operative versus nonoperative management with patients.
This study serves to enhance understanding of the influence different nonoperative treatment modalities have on outcomes after surgery. Our data suggest that surgical improvements in pain, PROs, and ROM occur regardless of the nonoperative modality tried beforehand, supporting previous evidence that arthroscopic management is effective in patients with persistent symptoms.11,18,25 The degree of postoperative improvement therefore appears independent of previous nonoperative treatment pathway. Further, the present study supports current literature demonstrating equivalent outcomes between nonoperative and operative management. 5
Limitations
There are several limitations to this study. First, given the retrospective, single-institution nature of this study, it is subject to selection bias and may limit its generalizability. However, demographic analysis was undertaken to help eliminate major demographic factors influencing the results. Treatment selection was based on shared decision-making between patients and providers, and unmeasured factors such as patient preference and provider practice patterns may have influenced treatment allocation in ways that cannot be fully captured through statistical adjustment. Second, although follow-up time was not significantly associated with postoperative VAS, SSV, FF, ER, or IR among patients with available data, bias due to differential loss to follow-up remains a possibility. Baseline characteristics were compared between patients with shorter and longer follow-up, and no significant differences were observed. Third, the lack of a standardized PT protocol limits reproducibility and internal validity, though it may enhance external validity by reflecting real-world heterogeneity in PT practice. Finally, this study had a relatively small number of patients in each treatment group and could be underpowered to detect differences among the cohorts. Our post hoc power analysis demonstrated inadequate statistical power to detect a significant difference in the reported success rates of avoiding surgery between modalities. Consequently, with an acceptable level of statistical power typically defined as 80% or higher, the findings are at risk of a type 2 error. Nonetheless, this cohort represents a 14-year period at a tertiary institution among 3 high-volume fellowship-trained surgeons. Further investigation with greater numbers of patients, randomization of patients to nonoperative treatments, and longer follow-up is warranted.
Conclusion
PT, CSI, and USB demonstrate similar rates of avoiding surgery for calcific tendinitis. For patients ultimately requiring surgery, outcomes are not influenced by previous nonoperative management. Surgical intervention may be indicated after failure of a single nonoperative modality.
Footnotes
Appendix
Pairwise Comparisons of the Success Rates of Avoiding Surgery for the Nonoperative Treatment Modalities (n = 217) a

| Comparison | Success Rate | Absolute Difference | P |
|---|---|---|---|
| CSI vs PT | 75 vs 59 | 16 (1 to 30) | .11 |
| CSI vs USB | 75 vs 72 | 3 (–12 to 18) | .35 |
| CSI vs multiple | 75 vs 0 | 75 (56 to 84) |
|
| PT vs USB | 59 vs 72 | 13 (–28 to 36) | .14 |
| PT vs multiple | 59 vs 0 | 59 (40 to 70) |
|
| USB vs multiple | 72 vs 0 | 72 (53 to 82) |
|
Data are presented as percentages or percentage (95% CI). Bold values indicate significance at P < .05.
Final revision submitted January 25, 2026; accepted March 5, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.P.L. reports education payments from Mid-Atlantic Surgical Systems. A.L. reports consulting fees from Arthrex, Tornier, and Stryker.
Ethical approval for this retrospective study was obtained from the University of Pittsburgh institutional review board (No. STUDY20030061).