
Abstract
Calcific tendinitis is a common pathology of the rotator cuff. More prevalent in women of middle age, calcific tendinitis is often extremely painful and can cause a significant decrease in patient quality of life. The following case study demonstrates the important role of sonography in diagnosis and treatment of calcific tendinitis.
Introduction
Calcific tendinitis is a common pathology of the rotator cuff, occurring in up to 7.5% of asymptomatic shoulders and in as many as 20% of painful shoulders. 1 The condition is a result of calcium deposition, in the form of hydroxyapatite, within the tendons of the rotator cuff. Patients may present with pain, localized swelling, redness, fever, and decreased range of motion. Although the exact etiology of calcific tendinitis is unknown, the presence of one or more calcium deposits within the tendons of the rotator cuff typically requires immediate treatment for patients in the acute phase of the condition. Accurate diagnosis is difficult based solely on patient presentation and medical history, potentially delaying patient treatment and prolonging patient suffering. 2 This case report demonstrates that sonography can provide quick diagnosis of calcific tendinitis as well as sonographic guidance for percutaneous treatment.
Case Report
A 61-year-old woman presented to an outpatient orthopedic office with acute onset right shoulder pain and a positive drop-arm test. The patient had a history of a right rotator cuff partial tear and right shoulder acromioclavicular (AC) joint osteoarthritis. Conventional radiographs of the right shoulder demonstrated a significant lobular calcification, characteristic of hydroxyapatite deposition, positioned in the subdeltoid bursa superficial to the greater tuberosity (Figure 1). Sonographic imaging showed an echogenic focus with ill-defined borders situated at the insertion point of a thinned supraspinatus tendon (Figure 2). These findings, when combined with patient history, were highly suggestive of ruptured supraspinatus calcific tendinitis with residual extruded defect in the subdeltoid bursa. A steroid injection performed with ultrasound guidance did not alleviate patient symptoms, so an ultrasound-guided barbotage was scheduled.
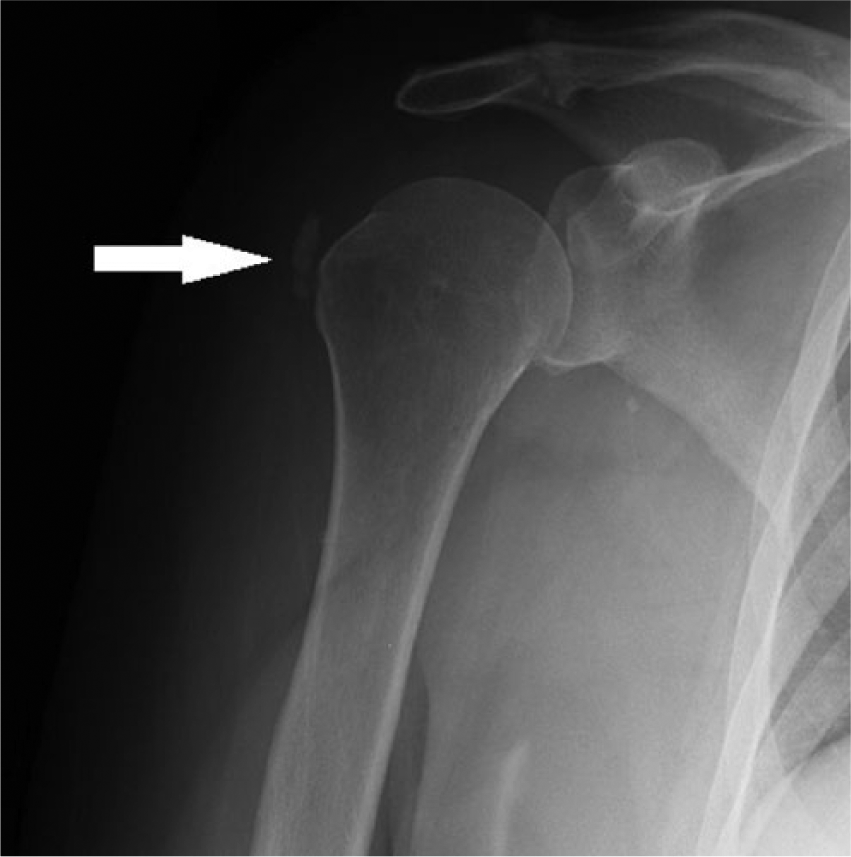
Conventional x-ray shows lobular calcification (arrow) at the right shoulder.
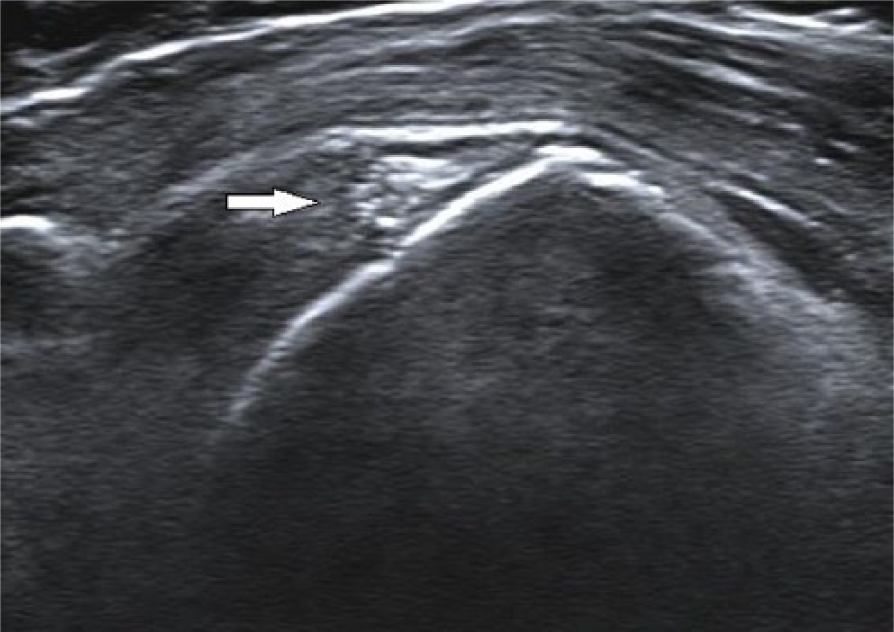
Ultrasound image of patient’s right shoulder showing echogenic calcification with poorly defined borders.
Approximately 1 week after initial presentation of symptoms, the patient underwent an ultrasound-guided barbotage of the right shoulder. Ultrasound-guided percutaneous treatment (UGPT), or barbotage, is an outpatient procedure that involves insertion of two or three needles into the area of rotator cuff calcification for the purpose of dissolving and aspirating the calcific deposit. The procedure was performed on a Siemens Acuson S2000 ultrasound system with an 18L6 HD transducer. During the procedure, a 21-gauge 1.5-inch needle was inserted into the residual calcification in the right supraspinatus tendon. Although no calcific material was able to be aspirated, a solution of anesthetic and steroid was injected into the affected area and the needle was removed. Postprocedure radiographs demonstrated that the treated calcium deposit was nearly absent. The patient tolerated the procedure without complication and was sent home. At the time of 1-month follow-up, the patient had regained full range of motion in the right arm.
Discussion
A basic understanding of shoulder anatomy is essential for accurate sonographic imaging. The shoulder is a ball-and-socket joint, known as the glenohumeral joint, formed by the junction of the humeral head and a shallow socket of the scapula. However, the humeral head does not fit perfectly within the socket, thereby depending on the rotator cuff, a collective of muscles and tendons surrounding the shoulder joint, for added stability. Situated anteriorly to posteriorly, the subscapularis, supraspinatus, infraspinatus, and teres minor muscles, along with their respective tendons, form a cuff, or covering, over the humeral head, securing it to the scapula (Figure 3).3,4
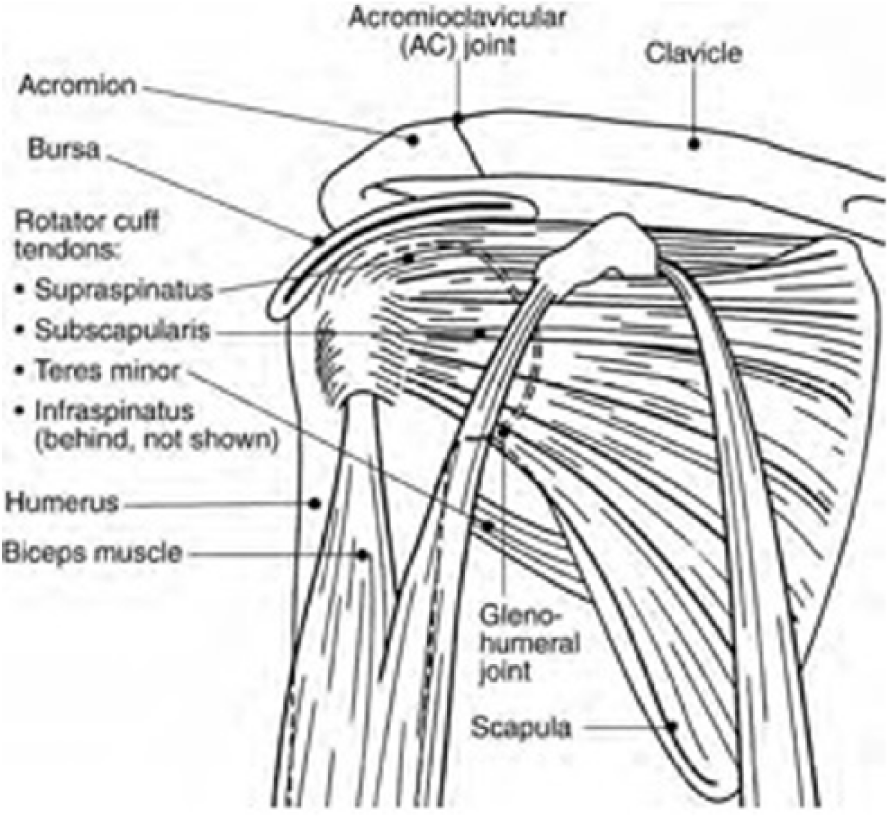
Structure of the shoulder. 5
The subscapularis muscle is large and triangle shaped. Its thick fibers originate beneath the scapula and insert onto the lesser tuberosity of the humerus via the subscapularis tendon. The supraspinatus muscle originates in the supraspinatus fossa of the scapula, passes underneath the acromion, a bony process of the scapula that articulates with the collarbone, and inserts onto the greater tuberosity of the humerus in the form of the supraspinatus tendon. This tendon is the most commonly torn tendon of the rotator cuff and a common site for calcific deposits to form.3,4 The infraspinatus muscle lies inferiorly to the scapular spine within the infraspinatus fossa and terminates in a wide tendon that inserts onto the greater tuberosity of the humerus, just inferior to the supraspinatus tendon. The smallest muscle of the rotator cuff is the teres minor muscle. Thin and laterally positioned, it originates at the axillary border of the scapula and attaches via the teres minor tendon onto the posterior greater tuberosity of the humerus. Along with providing stability, these muscles are used to perform a variety of shoulder movements, including flexion, abduction, and internal and external rotation. In addition to the components of the rotator cuff, there are several bursae in the shoulder region. The subacromial-subdeltoid bursa is the largest in the body and is the shoulder bursa of greatest clinical significance. 4 This bursa provides assistance to the rotator cuff in motion, particularly overhead movement. 4
Frequent, repetitive shoulder motion, enabled by rotator cuff muscles and tendons, makes rotator cuff lesions the most common soft-tissue ailment of the shoulder, followed by rotator cuff tears and calcific tendinitis. 6 Calcific tendinitis, also known as calcific tendinopathy, occurs in up to 7.5% of asymptomatic shoulders and in as many as 20% of painful shoulders.7,8 Caucasian women of middle age (30–50 years) are most often affected.1,7-10 The condition is characterized by painful, calcific deposits within the rotator cuff tendons, often at the insertion point of the supraspinatus tendon.2,4,7,9 Despite their typical location within the tendons of the rotator cuff, calcifications are not typically associated with rotator cuff tears.10,11 Calcific tendinopathy causes chronic pain, which is relative to adjacent tissue inflammation resulting from constant irritation during movement caused by the calcification.2,7 This pain is confined to the affected shoulder and often exacerbated at night. 7 Those affected may also experience tenderness, isolated swelling, redness, and decreased range of motion.9,12
The exact etiology of calcific tendinopathy is unknown, although a number of theories exist. Natural degenerative changes, resulting from vascular ischemia or repeated trauma, have been suggested to lead to calcium deposition.7,9,12 Genetic predisposition may also be a contributing factor, as there are indications of hereditary susceptibility as well as links between endocrine disorders such as diabetes and calcification development.9,12,13 The prevailing theory suggests that calcific tendinopathy is a reactive process, during which calcifications actively develop and often spontaneously resolve.7-9,14 Calcific deposition is likely due to a decrease in local oxygen concentration, although the precise causative mechanism is, as yet, unclear.7-9,14 Proponents of this theory describe three basic phases that make up the calcifying process. During the first, or precalcific, phase, the involved tendon undergoes fibrocartilaginous metaplasia, becoming less flexible. There are typically no symptoms associated with this stage. 10 In the calcific phase, calcium crystals are deposited and combine to form focal calcifications of considerable size. At this time, the affected individual will possibly experience subacute pain that is exacerbated at night. 10 The latter part of the calcific phase, known as the resorptive phase, is most painful.1,8 The calcium deposit exudes a thick, pasty material that is under pressure. The body’s inflammatory and immune responses are activated and pain can be intense, resulting in significantly decreased range of motion. Finally, during the postcalcific phase, the body attempts to heal the affected tendon. 9
Patients presenting with shoulder pain have historically been initially evaluated with x-rays, followed by more specialized imaging modalities such as computed tomography, contrast arthrography, and magnetic resonance imaging, which is often considered the gold standard for musculoskeletal imaging.3,6 Sonography, however, provides many advantages over these traditional methods of imaging and is quickly becoming the imaging modality of choice for initial imaging of shoulder pathology. Sonography provides substantive diagnostic information without radiation and is noninvasive, is relatively inexpensive, and allows for real-time evaluation of affected areas.3,6,10 In addition, with a sensitivity of more than 90%, sonography is much more capable than physical examination or radiography of evaluating subtle changes in soft-tissue and joint pathology. 4
The shoulder joint, in particular, is favorable to scanning by sonography. Common rotator cuff pathology seen with sonography includes tears, tendinitis, impingement, and calcification. 4 Bony landmarks such as the bicipital groove, which is a sulcus separating the greater and lesser tubercles of the humeral head; the lateral termination of the clavicle; and the acromion are particularly useful to the sonographer. 4 The coracoid process, an anterior hook-like projection of the superior scapula, is also a helpful bony landmark. 4 A high-frequency linear transducer is preferred for scanning the rotator cuff. Such a transducer provides better near-field resolution and a broad superficial field of view and allows use of tissue harmonics, which has a positive effect on image contrast and noise reduction. 3
Sonographic imaging of the shoulder occurs with the patient seated and the affected arm initially resting palm up on the patient’s thigh. 3 The examination begins with an assessment of the biceps tendon, which serves as a landmark by dividing the subscapularis tendon from the supraspinatus tendon. 3 In the transverse plane, the biceps tendon appears as a hyperechoic oval. 3 In the sagittal plane, the biceps tendon appears as a collection of echogenic, parallel lines. 3 Once the biceps tendon has been identified, the tendons comprising the rotator cuff are assessed in both the transverse and sagittal planes.
The subscapularis tendon is imaged both with the patient’s arm in a neutral position and during external rotation. With the transducer positioned in the transverse plane, the subscapularis tendon is seen in its long axis as a convex band of mid-level echoes situated posteriorly to the subdeltoid fat and superiorly to the humeral head.3,4 With the transducer positioned in the sagittal plane, the subscapularis tendon appears as an echogenic oval. 3 Assessment of the supraspinatus tendon is limited by the overlying acromion process.3,4 Therefore, optimal views are obtained with the patient’s affected arm extended posteriorly, elbow flexed, and the palmar surface of the hand facing outward.3,4 The subscapularis tendon is seen as a convex, homogeneous layer with the transducer in the transverse plane. In a sagittal plane, this tendon is visualized as a beak-shaped band of echogenic layers. 4 The infraspinatus and teres minor tendons are most often imaged with the hand of the affected arm resting on the patient’s thigh.3,4 Using a posterior approach, both the infraspinatus and teres minor tendons have a fibrous appearance in the sagittal plane, although the infraspinatus appears beak shaped whereas the teres minor appears more trapezoidal. Both appear as a convex band of echogenic layers in the transverse plane. Visualization of the teres minor is confirmation that the infraspinatus tendon has been visualized in its entirety. 3
Calcific tendinitis has been reported to be the most commonly diagnosed subacromial pathology discovered with sonography. 2 Calcifications most often appear as a hyperechoic area within a specific rotator cuff tendon and will have definite posterior shadowing.4,7 However, calcification appearance may vary, with these variations having a strong correlation with patient presentation as well as important implications for treatment. According to Fabbro et al., 10 calcific deposits of the rotator cuff may be identified as belonging to one of three categories (Figure 4). Type 1 calcifications are solid and hyperechoic with clearly defined borders and a distinct posterior shadow.4,10 Patients with type 1 calcifications are often mildly symptomatic or have no symptoms at all. 10 Treatment is often unnecessary for these patients. Type 2 calcifications are also solid, well-circumscribed, and hyperechoic but have little posterior shadowing.4,10 Type 3 calcifications are semiliquid. 10 As such, these calcifications are predominantly hyperechoic but appear heterogeneous and lack clear borders or posterior shadowing.4,10 Type 2 and 3 calcifications are associated with highly symptomatic patients in acute pain for whom expeditious treatment is indicated. 10
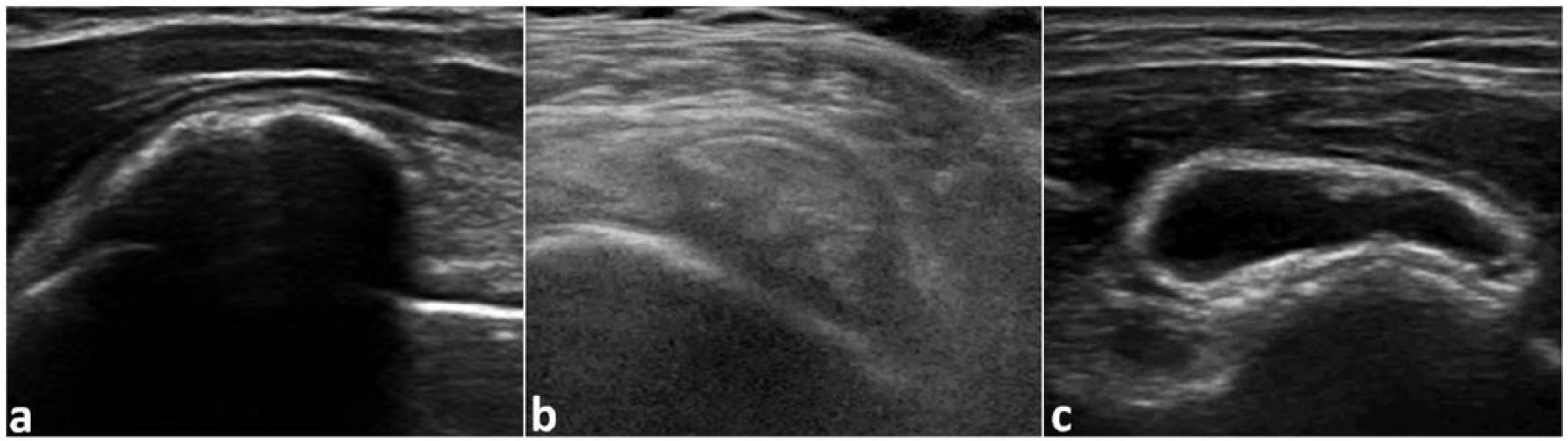
Examples of type 1 (a), type 2 (b), and type 3 (c) calcifications. 15
Other studies have categorized rotator cuff calcifications more specifically by their shape as seen with sonography.9,11 Chiou et al. 11 described the calcifications as arc shaped, fragmented, cystic, or nodular. The arc-shaped, fragmented, and nodular calcifications all appear hyperechoic, although the arc-shaped calcification is the only one determined to consistently have obvious posterior shadowing. 10 The cystic calcification is described as having a clearly defined, echogenic wall that surrounds an area of faint internal echoes or layering debris. 10 Distinction among calcifications can also be made according to vascularity, making power and color Doppler useful components of the sonographic examination.4,11 Non-arc-shaped calcifications demonstrate a higher degree of vascularity when assessed with color Doppler. 11 Nodular calcifications are particularly hypervascular. 11 Increased vascularity has been found highly indicative of a calcification in the resorptive phase, which corresponds to a period of intense symptoms for the affected individual.1,11
Patients with calcific tendinitis benefit from a high-resolution sonogram that can detect microscopic calcifications as well as identify the exact tendon that contains the calcification.6,9 Sonographic imaging also provides information about the size and shape of the calcification as well as the condition of the affected tendon(s).2,7 However, there are a few limitations to the diagnostic capability of sonographic imaging in cases of calcific tendinitis. Sonographic detection of calcifications can be limited by calcification location. In particular, the acromion acts to restrict the available window for imaging those calcifications situated medially to this bony process. 14 In addition, although sonography can provide basic information about a calcification in readiness for intervention, it is not well suited for predicting calcification consistency, which is an important factor for clinicians when determining the most appropriate modality for calcification removal. 14 Calcifications with a liquid-like consistency are well disposed to removal via UGPT, whereas viscous calcifications may require more invasive measures of removal. 14 Despite such limitations, sonographic imaging does provide detailed information about the characteristics of a calcification, which can guide a patient’s treatment plan.
A variety of treatment options are available to the patient with calcific tendinitis. Conservative treatments include oral anti-inflammatories, steroid injections, and physical therapy; all of these can alleviate acute symptoms but do not eliminate the calcific deposit.1,12,14 Other, more invasive, treatments are needed about 15% of the time. 13 Whereas calcification shape and consistency are important factors for determining the most appropriate modality for removing the calcium deposit, there are significant limitations to the majority of available invasive treatment methods. 14 Shockwave therapy can provide favorable outcomes for many patients, but success rates are highly variable, ranging from approximately 50% to 90%.1,10 In addition, shockwave therapy often requires multiple treatments to achieve the desired result and can be painful, particularly when performed during a patient’s episode of acute pain.1,10 Fluoroscopy-guided interventions have been performed since the 1970s but lack accuracy in locating the calcification and expose the patient to unwanted radiation.1,10 Arthroscopic surgery is virtually 100% successful but can require a hospital stay.1,8,10,14
Ultrasound-guided percutaneous treatment, or barbotage, has been performed since 1995 and is rapidly becoming the treatment of choice for calcific tendinitis of the rotator cuff.10,13 This treatment option is most useful when attempting to remove type 2 or type 3 calcifications. 10 Ultrasound-guided percutaneous treatment is minimally invasive and relatively inexpensive. In addition, UGPT does not expose the patient to unwanted radiation and is quick to perform, lasting as little as 20 minutes.7,8 Ultrasound-guided percutaneous treatment is also extremely accurate. Real-time imaging allows for active visualization of the targeted calcification as well as the needle being used for the procedure, meaning that there is a much smaller chance of injury to adjacent structures and fewer associated complications.1,4,7 The patient is afforded almost immediate pain relief and, more often than not, long-term results. 8
Ultrasound-guided percutaneous treatment is performed using a high-frequency linear transducer. The patient is positioned supine or semisupine with the affected arm fully extended and slightly rotated either internally or externally based on calcification location.8,10 After the patient’s skin is disinfected, a sterile drape is put into place and the physician injects a local anesthetic into the patient’s shoulder.7,8,10 With a sonographer on hand to operate the ultrasound equipment, the physician then locates the targeted calcification and, using real-time imaging, inserts two or three needles into the calcification (Figure 5).1,7,8,10 One needle is used to inject a dissolving solution, either saline or anesthetic, directly into the calcification. Using warm saline as a dissolving solution has been found to reduce the amount of time needed to perform the procedure by facilitating calcification dissolution and decreases the chance of postprocedure bursitis.1,10 Injection of the dissolving solution prompts the calcification to degrade, producing a chalky, toothpaste-like waste, which is drained using the other needle(s).8,10
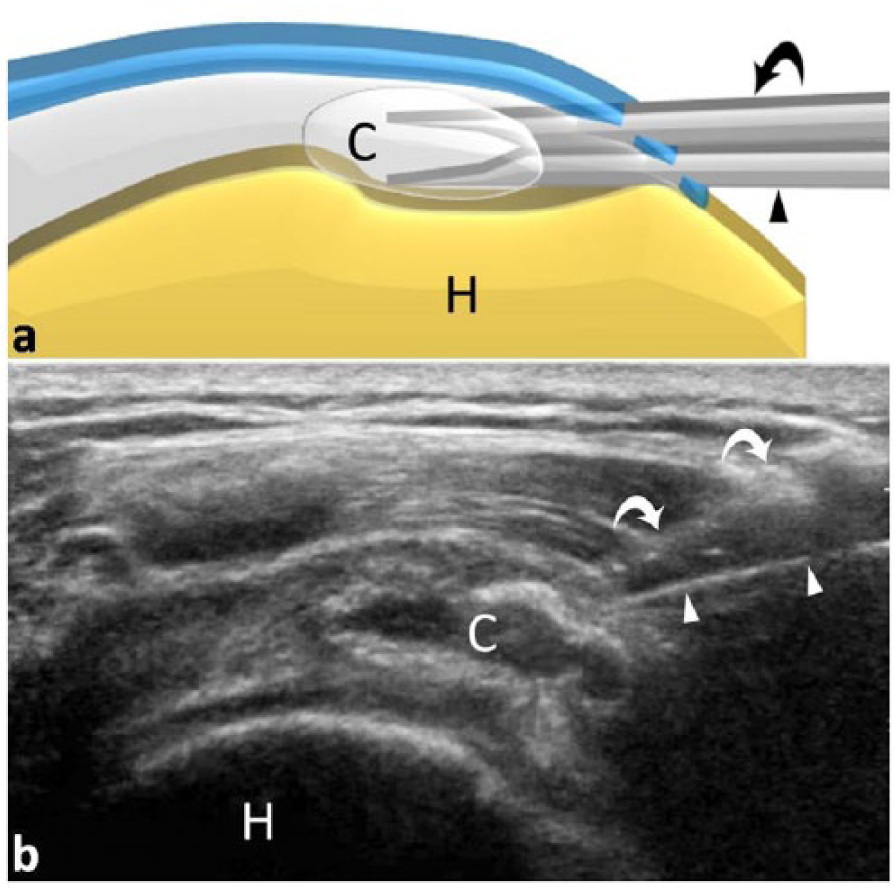
Depiction of two-needle (arrowheads and curved arrows) ultrasound-guided percutaneous treatment to treat rotator cuff calcification (C); humerus (H). 15
These steps are repeated multiple times, until the calcification is completely dissolved or reduced to its smallest possible size. All but one needle is then removed. The remaining needle is repositioned to allow for a steroid injection into the surrounding bursa.7,8,10 This is intended to prevent bursitis from developing postprocedure, which is a complication that occurs in up to 14% of patients. 10 Once the final needle has been removed and hemostasis is achieved, the patient is allowed to leave with few, if any, postprocedural restrictions on activity. The majority of patients with calcific tendinitis treated with UGPT and individualized physical therapy demonstrate significant, often immediate, pain relief as well as improved activities of daily living, strength, and range of motion. 7 Patients typically experience progressive improvements in these areas for up to 1 month postprocedure. 7 In addition, patients treated with UGPT report markedly improved 10-year outcomes when compared to patients not treated or treated with alternate therapies. 8
Conclusion
Sonography is increasingly being used to diagnose disorders of the rotator cuff such as calcific tendinopathy. The many benefits of using sonographic imaging for diagnosis of calcific tendinopathy, particularly its precision and lack of radiation, also make sonography a useful tool for treatment. In addition to these advantages, the components of the shoulder joint are superficial, meaning that the area is easily and safely accessible for interventions performed with ultrasound guidance. Therefore, ultrasound-guided percutaneous treatment, or barbotage, is especially well suited to treatment of calcific tendinopathy. As demonstrated by this case study, UGPT is a quick, elective method for the treatment of calcific tendinopathy.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.