
Abstract
Background:
Lateral patellar instability is more common in adolescents and young adults, and morphologic factors contribute to patellar dislocation. However, the relationship between baseline physical activity and morphologic risk factors in this population remains unclear.
Purpose:
To investigate the association between baseline physical activity and morphologic factors in patients with lateral patellar instability.
Study Design:
Cohort study; Level of evidence 3.
Methods:
A total of 111 knees of 75 patients (mean ± SD age, 20.4 ± 10.0 years) undergoing medial patellofemoral ligament reconstruction for lateral patellar instability were retrospectively analyzed. Patients were stratified into the competitive sports (n = 34), recreational sports (n = 18), and nonsports (n = 23) groups based on presymptom activity. Imaging parameters included trochlear depth (TD), Dejour classification and patellar height (Insall-Salvati ratio [ISR]) on preoperative lateral radiographs; congruence angle (CA), sulcus angle (SA), and tilt angle (TA) on Merchant view; and tibial tuberosity−trochlear groove (TT-TG) distance on preoperative computed tomography. To compare morphological parameters among the 3 groups, generalized estimating equations were used to account for within-patient clustering.
Results:
The nonsports group had a significantly higher mean age (P < .01). Bilateral knee surgeries were more frequent in competitive and nonsports groups (P = .04). Mean TD was 1.9 mm (95% CI, 1.4-2.3 mm) in the competitive group, 1.0 mm (0.3-1.6 mm) in the recreational group, and 1.1 mm (0.6-1.6 mm) in the nonsports group; TD was significantly higher in the competitive group than in the other groups (P = .02). Mean CA was 8.4° (7.3°-9.5°), 9.1° (7.8°-10.4°), and 6.8° (5.5°-8.0°), respectively, with a significant difference between the recreational and nonsports groups (P = .03). No group differences were observed for ISR, SA, TA, TT-TG, and Dejour classification.
Conclusion:
Many competitive athletes demonstrated greater TD but nonetheless frequently underwent bilateral surgical procedures. Similarly, nonsports participants also showed a high rate of bilateral procedures, which may reflect more severe trochlear dysplasia rather than activity-related demand alone. These findings highlight the importance of considering both baseline activity level and trochlear morphology when determining surgical indications in young patients with lateral patellar instability.
Keywords
Patellar dislocation and lateral patellar instability are multifactorial conditions influenced by both soft tissue and osseous factors. Morphologic risk factors—including patella alta, trochlear dysplasia, tibial tuberosity lateralization, and ligamentous laxity—contribute to an increased risk of patellar dislocation and instability.2,20 First-time patellar dislocation occurs most frequently in adolescents, with the highest incidence reported among individuals aged 14 to 18 years. 17 Although the underlying reason for this age-specific pattern is unclear, it may reflect higher activity levels and greater exposure to risk in this population. 17
Patellar dislocation can occur during sports participation as well as during activities of daily living, and recurrent instability may lead to chronic knee dysfunction, reduced quality of life, and limitations in sports activity. 18 Numerous studies have identified morphologic abnormalities—such as trochlear dysplasia, patella alta, increased tibial tubercle–trochlear groove distance, and lateral patellar tilt—as key anatomic risk factors for recurrent lateral patellar instability.4,5,10,13,15 However, the baseline physical activity status of patients who ultimately develop symptomatic instability has not been well characterized, and it remains unclear how active these patients were before the onset of symptoms. Understanding presymptom activity level may provide useful clinical context, complementary to established anatomic risk factors, by helping clinicians better interpret functional limitations at presentation and tailor diagnostic and treatment decisions. Specifically, although anatomic abnormalities are recognized contributors to recurrent patellar instability, little is known about the baseline physical activity levels of patients who eventually develop symptomatic instability. Understanding patients’ presymptom activity status may offer additional context when evaluating functional limitations, counseling patients, and selecting appropriate treatment strategies.
The purpose of this study was to investigate the relationship between baseline physical activity status and morphologic risk factors in patients with patellar dislocation and lateral patellar instability. The hypothesis is that patients with more severe trochlear dysplasia would demonstrate lower baseline activity levels and undergo bilateral surgical procedures more frequently.
Methods
Patients
A retrospective analysis was conducted. Between December 2016 and December 2021, 82 consecutive patients underwent isolated medial patellofemoral ligament reconstruction, which was the first-line surgical treatment for patellar instability at our institution during this period. No patient underwent tibial tubercle osteotomy or other additional bony procedure. At our institution, surgical intervention is considered even after a first-time patellar dislocation when clinical instability and predisposing anatomic risk factors are present. The cohort also included patients referred after developing recurrent patellar instability following prior dislocation episodes managed elsewhere. Notably, during the study period, no eligible patients with patellar dislocation were managed nonoperatively. Exclusion criteria were (1) previous surgery on the index knee (n = 1), (2) concomitant anterior cruciate ligament reconstruction (n = 2), (3) congenital or habitual patellar dislocation (n = 3), and (4) patellofemoral osteoarthritis (n = 1). A total of 111 knees from 75 patients (18 male and 57 female; mean ± SD age, 20.4 ± 10.0 years) were included in this study. Of these, 34 patients were in the competitive sports group, 18 in the recreational sports group, and 23 in the nonsports group (Figure 1).

CONSORT (Consolidated Standards of Reporting Trials) diagram of patient inclusion in the study. MPFL, medial patellofemoral ligament.
Procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. All patients provided written informed consent, and the study was conducted with approval from our institution's ethics committee.
Clinical Assessments
From medical records, age, sex, body mass index, laterality of knee joint, and Tegner activity score prior to symptom onset were collected. The interval from symptom onset to data collection had a median of 6 months (range, 0-74 months). Activity level was assessed based on patients’ self-reported physical activity prior to the initial patellar dislocation, using the Tegner activity scale as a reference. Patients were categorized into 3 groups according to their typical sports participation before the first dislocation: (1) competitive sports, defined as participation in organized competitive events or official matches; (2) recreational sports, defined as participation in noncompetitive sports activities or regular school physical education classes; and (3) nonsports, defined as no engagement in sports activities (Figure 1). Preinjury Tegner scores were obtained retrospectively from each patient based on his or her activity status before the initial patellar dislocation.
Image Evaluation
Predisposing morphologic factors were quantitatively assessed using preoperative radiographs and computed tomography (CT) scans. The following radiologic parameters were measured: (1) Insall-Salvati ratio (ISR) for patella alta11,19 (Figure 2); (2) trochlear depth (TD) for trochlear dysplasia 8 (Figure 2); (3) congruence angle (CA) on Merchant view for lateral displacement of the patella 8 (Figure 3); (4) sulcus angle (SA) on Merchant view for trochlear groove depth 14 (Figure 3); (5) tilt angle (TA) on Merchant view for lateral tilt of the patella relative to the femoral condyles 3 (Figure 3); and (6) tibial tuberosity–trochlear groove (TT-TG) distance on superimposed CT images for lateral malposition of the tibial tuberosity 8 (Figure 4). In addition, trochlear dysplasia was classified according to the Dejour classification using true lateral radiographs, based on the presence of the crossing sign, supratrochlear spur, and double contour sign.6,7 All radiologic assessments were performed on a digital radiography system.

Measurement of the Insall-Salvati ratio (ISR) and trochlear depth (TD). The ISR was calculated as the ratio of the patellar tendon length (LT), measured from the inferior pole of the patella to its tibial insertion, to patellar length (LP), measured along its greatest diagonal (from the superior to the inferior pole). TD was defined as the distance from the trochlear floor (B) to the most anterior condylar contour line (A), measured along a line subtended 15° distal from the perpendicular intersecting the tangent of the posterior femoral cortex and the most proximal portion of the posterior femoral condyles.

Measurement of the sulcus angle (SA), congruence angle (CA), and tilt angle (TA). The SA was defined as the angle formed by lines connecting the highest points of the medial and lateral femoral condyles to the deepest point of the trochlear sulcus (AOB). The CA was defined as the angle between the line bisecting the SA and the line connecting the sulcus apex to the central ridge of the patella (COD). The TA was defined as the angle between the line connecting the anterior edges of the femoral condyles and the line spanning the maximal width of the patella (E).

Measurement of the tibial tuberosity–trochlear groove (TT-TG) distance using superimposed femoral and tibial computed tomography images. The TT-TG distance was defined as the separation between 2 parallel lines (yellow): one passing through the center of the tibial tuberosity and the other through the base of the trochlear groove (green), both perpendicular to the posterior condylar line (red).
Statistical Analysis
Patients were compared among 3 groups (competitive sports, recreational sports, and nonsports). Demographic variables compared using 1-way analysis of variance and chi-square test. In the analysis of morphological parameters, because some patients contributed bilateral measurements, within-patient correlation was addressed by clustering at the patient level. Continuous outcomes were analyzed using generalized estimating equations with a Gaussian distribution and an exchangeable correlation structure. Overall group effects were assessed using Wald chi-square tests, with pairwise comparisons conducted using Wald tests based on robust standard errors. For the categorical outcome (Dejour classification), multinomial logistic regression with cluster-robust standard errors was used. Overall and pairwise group differences were evaluated using Wald tests. The Holm step-down procedure was applied to adjust for multiple comparisons. All tests were 2-sided, with statistical significance set at P < .05.
Intraclass Correlation Coefficients
All bone morphology measurements were performed by knee surgeons with >10 years of clinical experience. For interobserver reliability, 2 surgeons (Y.K. and E.S.) independently performed blinded measurements at separate time points. For intraobserver reliability, 1 surgeon (Y.K.) performed duplicate measurements at separate time points.
Results
Demographic characteristics for the 3 groups are presented in Table 1. The mean age of the nonsports group was significantly greater (P < .01), and the proportion of male patients was significantly higher in the competitive sports group (P < .01). Bilateral knee surgery was required significantly more often in the competitive and nonsports groups (P = .04).
Patient Characteristics According to Baseline Level of Activity a

Data are presented as n or mean ± SD, unless otherwise indicated. BMI, body mass index; F, female; M, male.
Bone morphology measurements (mean ± 95% CI) for the 3 groups are presented in Figures 5 to 11. For TD, the estimated mean (95% CI) was 1.9 (1.4-2.3) mm in the competitive group, 1.0 (0.3-1.6) mm in the recreational group, and 1.1 (0.6-1.6) mm in the nonsports group. The competitive group demonstrated significantly higher values compared with both the recreational and the nonsports groups (P = .02) (Figure 6). For CA, the estimated mean (95% CI) was 8.4° (7.3°-9.5°) in the competitive group, 9.1° (7.8°-10.4°) in the recreational group, and 6.8° (5.5°-8.0°) in the nonsports group, with a significant difference between the recreational and the nonsports groups (P = .03) (Figure 7). No significant differences were observed in ISR, SA, TA, TT-TG, or Dejour classification among the groups. Intraclass correlation coefficients ranged from 0.79 to 0.92 for interobserver reliability and from 0.84 to 0.96 for intraobserver reliability.

Insall-Salvati ratio. No significant differences were observed among the competitive, recreational, and nonsports groups.

Trochlear depth. The competitive group demonstrated significantly higher values compared with both the recreational and nonsports groups (p = .02).
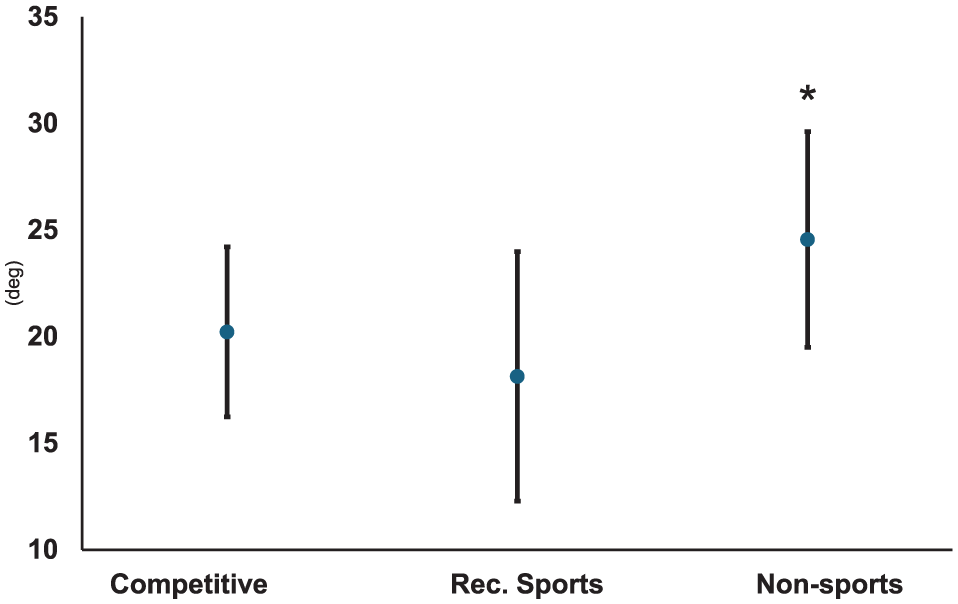
Congruence angle. The nonsports group demonstrated significantly higher values than the competitive and recreational groups (p = .03).

Sulcus angle. No significant differences were observed among the competitive, recreational, and nonsports groups.

Tilt angle. No significant differences were observed among the competitive, recreational, and nonsports groups.

Tibial tuberosity–trochlear groove distance. No significant differences were observed among the competitive, recreational, and nonsports groups.

Dejour classification. No significant differences were observed among the competitive, recreational, and nonsports groups.
Discussion
In this study, the competitive sports group exhibited significantly greater TD than the recreational and nonsports groups. Notably, many competitive athletes underwent bilateral knee surgery at a young age. In contrast, CA was significantly greater in the nonsports group compared with the competitive and recreational groups. These findings indicate an association between higher levels of physical activity and the severity of morphological parameters within our cohort.
Trochlear dysplasia is a primary anatomic risk factor for lateral patellar dislocation and instability in skeletally immature patients when defined as TD <3 mm on magnetic resonance imaging (MRI). 1 Chen et al 3 reported that sulcus depth measured by CT, the most frequently identified anatomic risk factor, demonstrated the strongest diagnostic performance among trochlear morphological parameters and the closest association with recurrent patellar dislocation. Kwon et al 12 investigated patellofemoral morphological features on MRI using machine learning and identified patellar tilt and reduced TD as the strongest predictors of patellar dislocation. Therefore, shallow TD remains a critical diagnostic factor and guides treatment planning, particularly regarding surgical intervention.
Importantly, the observed differences in TD were small, and all patients demonstrated trochlear dysplasia. Therefore, these findings should not be interpreted as indicating that individuals with shallower trochlea are incapable of participating in competitive or recreational sports activities, as many patients with trochlear dysplasia were still able to participate in competitive or recreational sports. However, dynamic MRI analyses of patellar tracking during quadriceps loading have demonstrated that a shallow trochlea is associated with greater lateral patellar tilt and displacement, reflecting diminished bony constraint. 9 Consequently, in patients with trochlear dysplasia, the extensor mechanism may be mechanically disadvantaged, which could influence movement efficiency, particularly during high-demand athletic activities. Previous studies have shown that greater severity of trochlear dysplasia is associated with altered lower-extremity biomechanics during sport-related tasks, including changes in landing mechanics and joint kinematics, suggesting differences in how athletic tasks are performed rather than absolute limitations in physical capability. 16
Conversely, it is also possible that individuals with lower physical activity levels may self-limit participation due to apprehension or fear of instability, rather than biomechanical insufficiency alone. Lifestyle factors and activity modification may therefore influence the observed relationship between trochlear morphology and physical activity. In addition, the distribution of the Dejour classification may be related to differences in physical activity status. Although no statistically significant differences were observed among the groups, Dejour type A tended to be more frequent in the competitive sports group and less frequent in the recreational and nonsports groups. This finding suggests that, although trochlear dysplasia was present across all groups, competitive athletes more commonly exhibited a morphologically less complex form of dysplasia. Notably, despite lower activity levels, patients in the nonsports group more frequently required bilateral surgical intervention. This may reflect a higher prevalence of more severe or morphologically complex trochlear dysplasia in this group, rather than activity-related mechanical demand alone. Thus, the need for bilateral stabilization in nonathletes may be driven by underlying anatomic severity rather than functional loading. Such qualitative differences in trochlear morphology, in combination with modest variations in TD, may influence tolerance to higher functional demands rather than determine physical activity participation.
From a clinical perspective, the modest differences in TD observed in this study are unlikely to independently alter surgical decision-making. Rather, TD should be considered alongside functional demand, symptom severity, and other anatomic risk factors. The higher frequency of bilateral surgical procedures observed in competitive athletes may reflect greater functional requirements rather than trochlear morphology alone.
Limitations
This study has several limitations. First, the groups differed significantly in age, sex distribution, and likely skeletal maturity; the competitive sports group tended to be younger and predominantly male, whereas the nonsports group tended to be older and predominantly female. These differences may confound the observed associations and should be considered when interpreting the findings. Second, this study did not distinguish between patients with first-time and recurrent patellar instability. Its retrospective design also limited the establishment of clear and definitive diagnostic criteria. Although recorded diagnoses were assumed accurate, this assumption introduces potential bias. Differentiating first-time dislocation from recurrent patellar instability is often challenging, as patients who report “instability” may in fact be experiencing repeated episodes of dislocation or subluxation. Furthermore, because our institution primarily receives referred patients, initial symptom onset and early clinical history in some cases occurred prior to presentation at our hospital. Accordingly, certain historical information may have been based on prior records and patient recall rather than contemporaneous documentation at symptom onset. This may introduce recall or information bias and should be considered when interpreting the findings. Third, the study compared imaging findings with patients’ self-reported sports participation but did not assess objective measures of physical function or sports performance. A further limitation is the use of the ISR to evaluate patellar height. Although ISR is a widely used method in patellar instability research and is minimally affected by knee flexion when images are obtained at ≥30° of flexion, it can still be influenced by patellar tendon length. Moreover, multiple methods exist for assessing patellar height, each with its own advantages and limitations, and no single technique is universally superior. 19 These factors may have introduced measurement bias, and future studies incorporating multiple patellar height indices may provide a more comprehensive assessment. Fourth, this study included only patients who underwent surgery performed at our hospital. Because our institution functions primarily as a referral center, all patients evaluated for patellar instability during the study period underwent surgical treatment. Patients treated nonoperatively at other institutions were not captured in this cohort. Therefore, external validity was not assessed, and the findings may not be generalizable to all populations or clinical settings. Finally, although clustering methods were used to account for within-patient correlation, the inclusion of both unilateral and bilateral cases may represent a structural limitation inherent to the study design.
Conclusion
A significant association was observed between baseline activity status and TD. Competitive athletes demonstrated modestly greater TD compared with recreational sports and nonsports participants, while all patients exhibited trochlear dysplasia. Patients without sports participation were generally older, had shallower TD, greater CA, and more frequently required bilateral surgical intervention. In contrast, competitive athletes demonstrated greater TD; however, they commonly underwent bilateral procedures. Taken together, these findings suggest that higher baseline activity levels, even in the presence of relatively greater TD, may be associated with substantial functional demands that can necessitate bilateral surgical intervention. This relationship should be interpreted in the context of patient age, activity level, and overall clinical presentation when considering management strategies.
Footnotes
Final revision submitted February 18, 2026; accepted February 23, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.