
Abstract
Background:
The impact of lower extremity torsion on the clinical outcomes in patients who have undergone isolated medial patellofemoral ligament reconstruction (MPFLR) with artificial tape and suture anchors remains unclear.
Purpose:
To evaluate the association between lower extremity torsion and clinical outcomes following MPFLR using FiberTape and knotless SwiveLock anchors in patients with recurrent patellar instability.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This study included 96 knees (65 patients) that underwent MPFLR between 2016 and 2023 with femoral torsion (FT) and tibial torsion (TT) as potential predictors of postoperative outcomes. Preoperative and postoperative assessments included radiographic and computed tomography measurements and clinical evaluations using the Knee injury and Osteoarthritis Outcome Score (KOOS).
Results:
Significant improvements were observed in the KOOS subscale scores (pain, symptoms, quality of life, sports, and activities of daily living) 1 year postoperatively. Knees with FT ≤30° showed superior outcomes in symptoms and sports activities compared with those with FT >30°. Multivariate analysis identified increased FT as negatively associated with patients’ scores on the sports subscale of the KOOS questionnaire (β = −0.251, P = .009), whereas higher TT was positively associated with sports scores (β = 0.335, P < .001). Receiver operating characteristic analysis identified an FT threshold of 27° as a predictor of postoperative apprehension and symptoms.
Conclusion:
These findings underscore the detrimental impact of increased FT on MPFLR outcomes, highlighting the necessity for a comprehensive preoperative assessment of lower extremity torsion. Future research should explore the long-term effects and refine surgical protocols to enhance treatment efficacy.
Patellar dislocation is a common knee disorder in adolescents and young adults.16,34 Recurrent patellar instability is a complex condition often managed surgically through medial patellofemoral ligament reconstruction (MPFLR), which restores the primary medial stabilizer of the patella.8,17 Among the various surgical techniques available for MPFLR, the use of artificial tape combined with suture anchors has emerged as a promising option.12,37,38 This approach provides secure fixation and reduces surgical complexity, resulting in favorable clinical outcomes in patients with recurrent patellofemoral dislocation.23,31
Lower extremity torsion, including femoral torsion (FT) and tibial torsion (TT), affects knee biomechanics and patellar tracking.3,7 Increased FT can increase the lateral force vector of the patella, 7 whereas abnormal TT may increase the risk of graft failure or lead to persistent instability, particularly in patients undergoing isolated MPFLR. Several studies have reported good clinical outcomes after derotational osteotomy in cases of substantial rotational abnormalities.11,33 However, the impact of lower extremity torsion on the clinical outcomes in patients who underwent isolated MPFLR with artificial tape and suture anchors remains unclear.
Hence, this study aimed to address this gap by evaluating the clinical outcomes in patients with varying degrees of lower extremity torsion who underwent MPFLR using FiberTape (Arthrex) and knotless anchors. We hypothesized that patients with increased FT and TT levels would have impaired clinical outcomes after MPFLR.
Methods
Ethics Statements
The study procedures were performed in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. All patients provided written informed consent, and the study was approved by the ethics committee of our institution.
Study Design and Population
This retrospective study included 145 knees with lateral patellar instability with or without recurrent dislocation that underwent isolated MPFLR using FiberTape and knotless SwiveLock anchors (Arthrex) between 2016 and 2022. Of the 146 cases initially identified, we excluded 23 patients aged >30 years, 22 patients without computed tomography (CT) data, and 4 patients without Knee injury and Osteoarthritis Outcome Score (KOOS) data. During follow-up, we further excluded 1 patient (bilateral case) who developed a surgical site infection. Ultimately, 65 patients with 96 MPFLRs were included in the study (Figure 1).
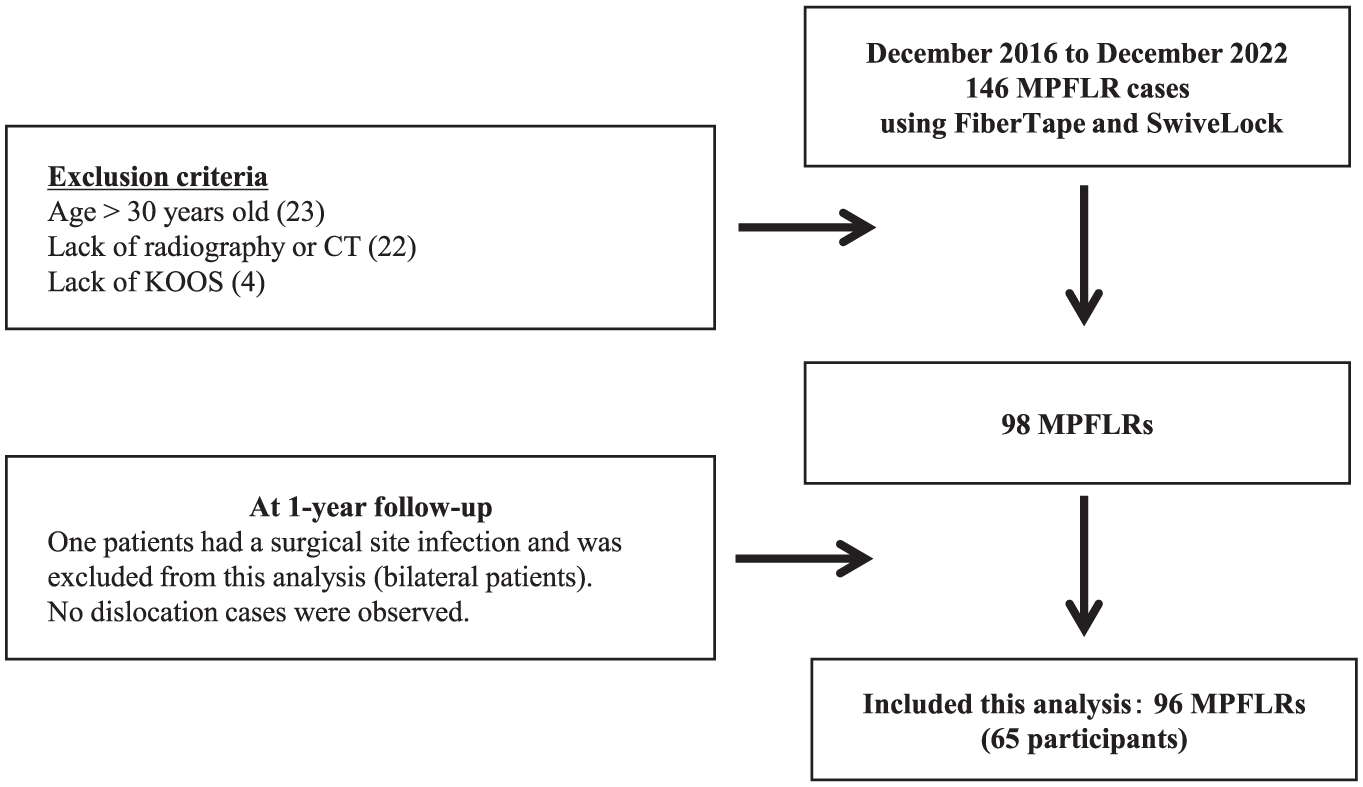
Flowchart of study patients. KOOS, Knee injury and Osteoarthritis Outcome Score; MPFLR, medial patellofemoral ligament reconstruction.
Surgical Management
MPFLR was performed for patients who had experienced at least 2 episodes of recurrent patellar dislocation, confirmed through clinical history, physical examination, and imaging. All patients had previously received nonoperative treatments (eg, physical therapy and bracing) but continued to experience symptoms of instability. Contraindications for this procedure included high-grade trochlear dysplasia (Dejour type D dysplasia), 5 severe patellofemoral osteochondral damage, and skeletal immaturity, which was assessed using plain radiographs by confirming the closure of the distal femoral and proximal tibial growth plates. MPFLR was performed using polyester high-strength suture tape (FiberTape) and knotless anchors (SwiveLock), following previously established methods. 14 The procedure began by performing diagnostic arthroscopy to assess patellar tracking, trochlear and patellar dysplasia, lateral retinacular tightness, and any chondral damage. On the basis of the results of passive patellar tilt and medial patellar glide tests conducted with patients under anesthesia, as well as arthroscopic findings, lateral retinacular release was performed in cases of considerable lateral tightness, defined as irreducible patellar tilt. This was achieved through the anterolateral portal by using scissors to avoid excessive postoperative patellofemoral contact pressure.
With the knee positioned at 90° of flexion (figure-4 position), a 2- to 3-cm longitudinal skin incision was made along the medial border of the patella. The medial retinaculum (first layer) was opened, and the FiberTape was passed deep to the first layer. Next, the medial edge of the patella was exposed, and 2 blind tunnels were drilled to accommodate 3.5-mm SwiveLock anchors. These fixation points were positioned proximally near the quadriceps insertion point and distally at the midsection of the medial patellar edge. FiberTape was secured in these tunnels using SwiveLock anchors.
For femoral fixation, a 2.4-mm Kirschner wire was inserted at the Schöttle point through a 1- to 2-cm incision, guided by imaging and a medial patellofemoral ligament (MPFL) guide (JBM0200-01/2; BEAR Medic). 26 After ensuring isometry of the FiberTape and confirming proper patellar tracking through the full range of motion, the FiberTape was anchored to the femur at 90° of knee flexion using a 4.75-mm SwiveLock anchor. The FiberTape was intentionally left slightly looser than the native MPFL to prevent overtensioning upon final fixation. A final arthroscopy was performed to confirm proper patellar tracking after fixation. Postoperative rehabilitation emphasized early range of motion exercises. Muscle activation exercises (eg, patellar setting and straight-leg raises) were initiated promptly. Weightbearing exercises were introduced on the basis of pain tolerance.
Radiographic Measurements
Preoperative radiographic evaluation of the knee was performed. Skilled radiology technicians obtained weightbearing anteroposterior plain and axial radiographs with the knee flexed at 30°. The sulcus and patellar tilt angles were measured on these axial views. 9 The Caton-Deschamps index was calculated from lateral plain radiographs to assess patellar height. 4 These measurements were performed using Picture Archiving and Communication System software (ShadeQuest/ViewR, version 1.24.15; Fujifilm Medical), which allows measurement precision values of 0.01° for angles and 0.01 mm for lengths.
Computed Tomography Measurements
FT and TT were assessed using 2 reference lines for each measurement, as illustrated in Figure 1.15,25 FT was determined as the angle formed between a line passing through the center of the femoral head and neck and a second line tangent to the posterior femoral condyles (Figure 2A). Similarly, TT was measured using the angle between the line tangential to the posterior edge of the tibial plateau and the second line connecting the centers of the medial and lateral malleoli (Figure 2B). Patients were categorized into 2 groups based on the threshold value of 30° (ie, torsion degree <30° and torsion degree ≥30°) for FT and TT based on a prior study. 21 The tibial tubercle–trochlear groove (TT-TG) distance was measured as follows. 24 First, the trochlear groove was identified on axial CT images at the deepest point of the trochlea, and the corresponding center point was marked. Second, in a similar manner, the tibial tubercle was identified on the axial images at the most prominent point of the tibial tuberosity, and its center point was marked. Third, a perpendicular line was drawn from each center point to a reference line along the posterior condyle, and finally, the distance between these 2 perpendicular lines was recorded as the TT-TG distance (Figure 2C). The measurements were performed using ShadeQuest (Fujifilm Medical), and 2 independent observers (K.I. and S.U.) examined the interrater reliability of 40 randomly selected patients.

Measurement of femoral torsion and tibial torsion. (A) Femoral torsion was determined by the angle formed between a line passing through the center of the femoral head and neck and a second line tangent to the posterior femoral condyles. (B) Tibial torsion was measured using the angle between a line tangential to the posterior edge of the tibial plateau and a second line connecting the centers of the medial and lateral malleoli. (C) The tibial tubercle–trochlear groove (TT-TG) distance was measured on axial computed tomography images by marking the center points of the trochlear groove and tibial tubercle, then drawing perpendicular lines to a reference line along the posterior condyles. The distance between these perpendicular lines was recorded as the TT-TG distance.
Clinical Data Collection
The preoperative demographic characteristics of the patients at the time of surgery, including age, sex, and body mass index (BMI), were retrospectively collected from the medical records. We assessed the range of motion before and 1 year after surgery. The active patellar subluxation (APS) test was conducted to evaluate lateral patellar instability. 10 For this test, the patient was positioned in the supine position with the knee initially held in full extension. The examiner manually applied a lateral translational force to the patella using their thumb. While maintaining this lateral force, the patient was instructed to actively flex the knee to 90° and then extend it back to full extension. During this subluxation maneuver, the examiner carefully observed for any signs of apprehension or an extension lag sign. Subsequently, the reduction maneuver was performed. With the patient starting again from full knee extension, the examiner applied a medial translational force to the patella using their index finger. Then, the patient was asked to actively flex the knee to 90° and subsequently extend it back to full extension. The examiner observed whether the patient could freely flex and extend the knee without showing signs of apprehension. The test was considered positive for lateral patellar instability if the patient exhibited an inability to fully extend the knee or expressed apprehension during the subluxation maneuver, while demonstrating no apprehension and smooth knee motion during the reduction maneuver. Furthermore, preoperative and postoperative patient-reported outcomes a year after surgery were evaluated using the KOOS, which includes 5 subscales: pain, symptoms, quality of life (QOL), sports activities, and activities of daily living (ADL).2,22 In patients with bilateral MPFLR, KOOS scores were obtained separately for each knee; thus, clinical outcome measures were analyzed on a per-knee basis.
Statistical Analysis
Continuous variables are presented as mean ± standard deviation and categorical variables as count and percentage. Data distribution was assessed using the Shapiro-Wilk test. For normally distributed variables, the paired t test was used for preoperative versus postoperative comparisons, and the unpaired t test was used for between-group comparisons. For nonnormally distributed variables, the Wilcoxon signed-rank test and Mann-Whitney U tests were used, respectively.
Multivariate linear regression analysis was conducted to identify independent factors associated with KOOS scores. The dependent variables included postoperative KOOS subscale scores (pain, symptoms, ADL, sports, and QOL), whereas the independent variables included age, sex, BMI, sulcus angle, tilt angle, TT, FT, TT-TG distance, and bilaterality (unilateral vs bilateral cases). Regression results are expressed as β coefficients, P values, and 95% confidence intervals. Statistical significance was set at P < .05. Finally, a receiver operating characteristic (ROC) analysis was performed to estimate the predictive cutoff level of FT for postoperative apprehension or APS. The false-positive ratio was plotted against 1 true-positive fraction, and the cutoff point was defined as the point of the maximum slope (ie, the nearest point to the true positive). The area under the curve was calculated to assess the validity of the ROC analysis.
The intraclass correlation coefficients (2,1; 2-way random-effects model, single measures, absolute agreement) were 0.821 (95% CI, 0.539-0.818; P < .001) and 0.793 (95% CI, 0.492-0.700; P < .001) for FT and TT, respectively. All analyses were performed using a commercial statistical package (SPSS, version 29.0; IBM), and statistical significance was set at P < .05.
Results
Patients’ mean age was 15.6 ± 2.8 years, and 66.7% of patients were female. The mean BMI was 24.6 ± 4.9 kg/m2, with 43 patients undergoing surgery on the right knee. In total, 74 patients (77%) underwent lateral retinacular release in addition to MPFLR.
Radiographic parameters showed a mean Caton-Deschamps index of 1.3°± 0.8°, a sulcus angle of 141.9°± 7.4°, and a tilt angle of 20.7°± 10.0°. CT measurements showed a mean FT of 22.3°± 9.9°, TT of 21.4°± 8.1°, and TT-TG distance of 20.7 ± 2.9 mm (Table 1). Significant improvements were observed across all KOOS domains following MPFLR. Postoperatively, the mean KOOS scores for pain, symptoms, ADL, sports, and QOL were significantly higher than the preoperative values (all P < .001) (Table 2). At the 1-year follow-up, there were no repeat dislocations.
Patients’ Demographic Data and Radiographic Parameters a
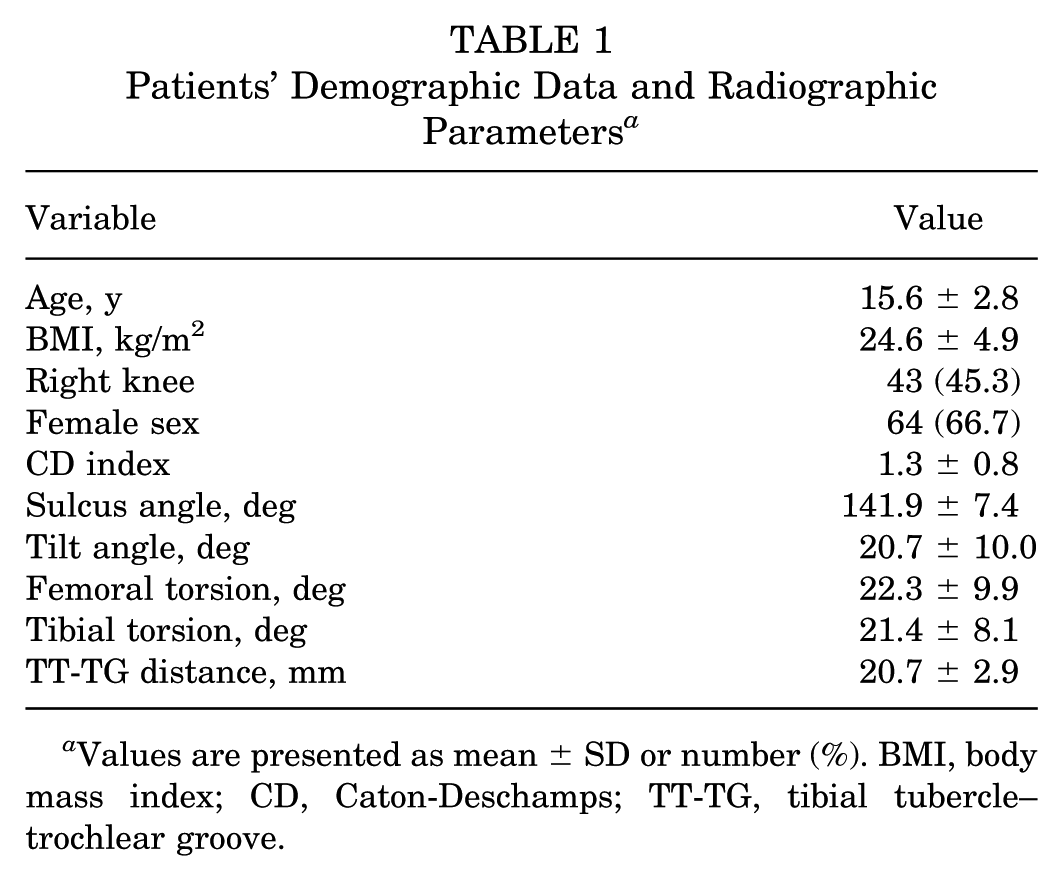
Values are presented as mean ± SD or number (%). BMI, body mass index; CD, Caton-Deschamps; TT-TG, tibial tubercle–trochlear groove.
Comparison of Preoperative and Postoperative Outcomes a
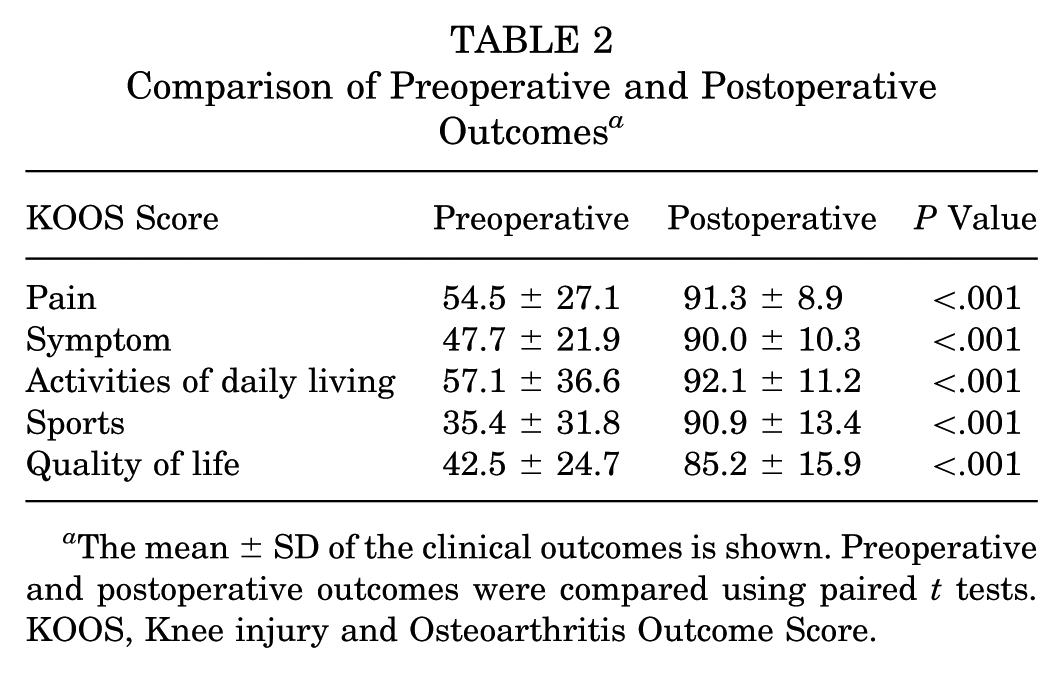
The mean ± SD of the clinical outcomes is shown. Preoperative and postoperative outcomes were compared using paired t tests. KOOS, Knee injury and Osteoarthritis Outcome Score.
The number of MPFLRs with FT ≤30° was 70 (73%). The mean follow-up durations were 2.4 ± 1.6 years and 3.0 ± 1.3 years in knees with FT ≤30° and FT >30°, respectively. Knees with FT ≤30° demonstrated significantly better postoperative KOOS symptom (P = .006) and sports scores (P < .001) than those with FT >30°. There were no significant differences between the groups in terms of postoperative apprehension or APS (P > .05) (Table 3). Similarly, the number of MPFLRs with TT ≤30° was 85 (89%). The mean follow-up durations were 2.6 ± 1.5 years and 2.8 ± 2.1 years in knees with TT ≤30° and TT >30°, respectively. Preoperative and postoperative KOOS scores did not show significant differences between the groups. There were no cases of postoperative apprehension or APS in the TT >30° group (Table 4).
Comparison of Patients Based on Degrees of Femoral Torsion a

Values are presented as mean ± SD or number (%) unless otherwise indicated. Measurements between the 2 groups were compared using the Mann-Whitney U test. APS, active patellar subluxation; BMI, body mass index; CD index, Caton-Deschamps index; FT, femoral torsion; KOOS, Knee injury and Osteoarthritis Outcome Score; TT-TG, tibial tubercle–trochlear groove.
Comparison of Patients Based on Degrees of Tibial Torsion a

Values are presented as mean ± SD or number (%) unless otherwise indicated. Measurements between the 2 groups were compared using the Mann-Whitney U test. APS, active patellar subluxation; BMI, body mass index; CD index, Caton-Deschamps index; KOOS, Knee injury and Osteoarthritis Outcome Score; TT, tibial torsion; TT-TG, tibial tubercle–trochlear groove.
Multivariate analysis identified age, sex, and torsional parameters as significant predictors of postoperative KOOS outcomes. Increased TT was positively associated with higher KOOS sports scores (β = 0.335, P < .001), whereas higher FT was negatively correlated with the same domain (β = −0.251, P = .009). Female sex was an independent predictor of better KOOS ADL scores (β = 0.504, P = .039) (Table 5). ROC analysis indicated that the cutoff value for postoperative knee symptoms was 27.1° for the FT (area under the curve, 0.846; P < .001) (Figure 3).
Results of Multivariate Analysis of the Factors Associated With Postoperative Outcomes a
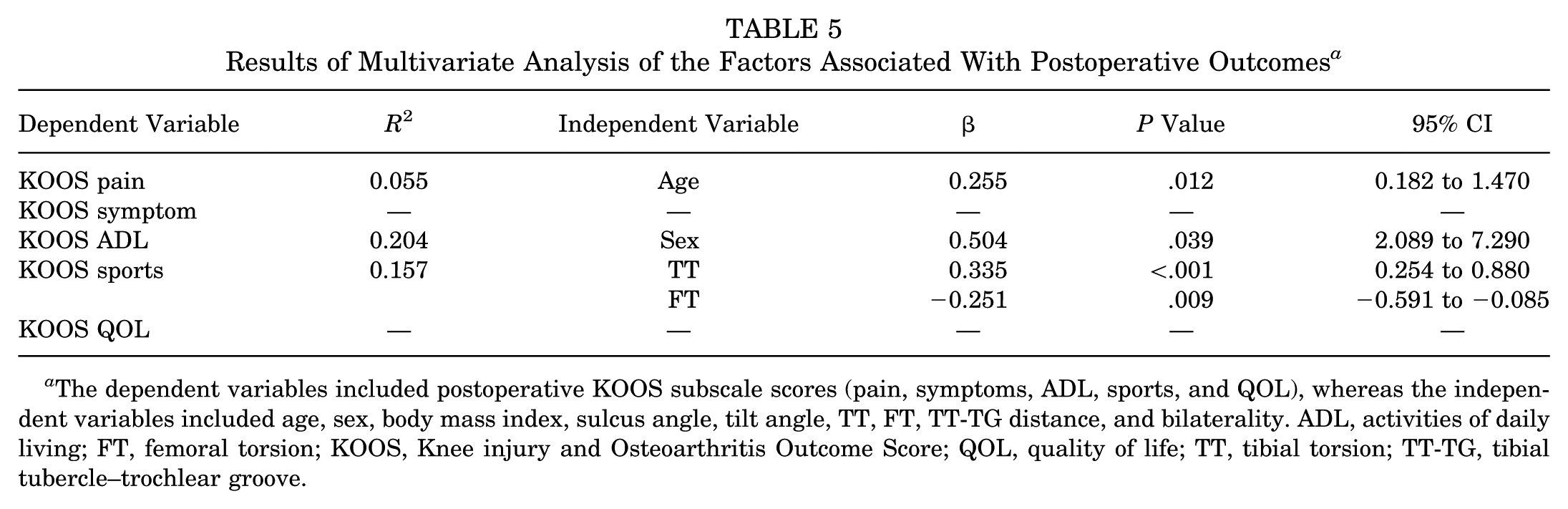
The dependent variables included postoperative KOOS subscale scores (pain, symptoms, ADL, sports, and QOL), whereas the independent variables included age, sex, body mass index, sulcus angle, tilt angle, TT, FT, TT-TG distance, and bilaterality. ADL, activities of daily living; FT, femoral torsion; KOOS, Knee injury and Osteoarthritis Outcome Score; QOL, quality of life; TT, tibial torsion; TT-TG, tibial tubercle–trochlear groove.

Receiver operating characteristic curve for determining the threshold value of femoral torsion for postoperative apprehension and APS. APS, active patella subluxation; AUC, area under the curve; FPF, false-positive fraction; TPF, true-positive fraction.
Discussion
The most important finding of the present study was that increased FT was associated with inferior clinical outcomes after isolated MPFLR using FiberTape and SwiveLock; however, patella alta, femoral trochlear dysplasia, increased TT-TG distance, and TT were not associated with inferior outcomes. To achieve optimal clinical outcomes in patients undergoing MPFLR for patellar instability, correction of severe femoral extremity malrotation may need to be considered.
Numerous studies have underscored the critical role of lower extremity torsion in recurrent patellofemoral instability.1,15,16,20,32 Increased FT and TT cause increasing MPFL strain along with lateral patellofemoral contact pressure. 30 Increased FT has been identified as a significant risk factor, with a threshold of ≥20° being particularly relevant in patients with intact medial patellofemoral ligaments. 13 However, few studies have investigated the association between lower extremity torsion and clinical outcomes after MPFLR.
Previous studies have demonstrated that increased FT amplifies the lateral force vector acting on the patella, potentially leading to persistent instability or graft failure.9,15,25 Qiao et al 19 reported that patients with FT >30° showed inferior scores on clinical outcome measures such as Tegner, Kujala, International Knee Documentation Committee, Lysholm, and KOOS scales after combined MPFLR and tibial tubercle transfer. Deng et al 6 reported that MPFLR alone may be inadequate for patients with increased FT and suggested combining MPFLR with femoral transverse osteotomy, which showed promising results. Similarly, Zhang et al 33 reported that patients with FT >30° had inferior postoperative clinical outcomes, including greater patellar laxity, a higher rate of residual J-sign, and lower patient-reported outcome scales after combined MPFLR and tibial tubercle transfer. Although our study analyzed isolated MPFLR using FiberTape, the results support those of previous studies.
Studies investigating the effect of TT after MPFLR are limited.18,19 Qiao et al 20 reported that patients with TT >30° showed inferior scores on clinical outcome measures such as Tegner, Kujala, International Knee Documentation Committee, Lysholm, and KOOS scales after MPFLR. 27 However, Zhang et al 35 reported that there were no significant differences in postoperative Kujala scores between patients with different external TT (>30° vs <30°). In the present study, increased TT did not negatively affect postoperative outcomes and was positively associated with higher KOOS sports scores in multivariate analysis. This difference may be due to the severity of TT. In the study by Qiao et al,19,20 the mean TT was higher than that in our study. Nonetheless, further research is required to explore the underlying mechanisms and validate these findings in larger cohorts.
Femoral trochlear dysplasia, TT-TG distance, and patellar height were not significantly associated with postoperative outcomes, which is consistent with the findings by Zhang et al. 36 However, these anatomic factors have been linked to poor patellofemoral stability in previous studies.37,38 This discrepancy may be attributed to the small sample size of the present study, which could have limited our ability to detect subtle effects. Moreover, patients in this cohort demonstrated mild lateral patellar shift and femoral trochlear dysplasia compared with those in previous studies.37,38 These findings highlight the multifactorial nature of patellofemoral instability and suggest that the presence of anatomic risk factors alone may not necessarily predict poor outcomes following isolated MPFLR. Further studies with larger cohorts and longer follow-up are warranted to clarify these associations.
Limitations
This study has some limitations. First, the retrospective nature of the study and small sample size may have introduced selection bias and yielded insufficient power to detect differences. Second, the accuracy of TT-TG distance measurements can vary depending on the imaging modality and patient positioning. Although CT is considered a reliable method for assessing the TT-TG distance, small differences in axial plane selection and patient positioning may affect accuracy.6,28,29 Third, the interpretation of lower limb torsion in relation to clinical outcomes remains unclear. The lack of preoperative sports performance data makes it difficult to directly assess how FT and TT affect postoperative improvement. Moreover, the threshold for “abnormal” TT has been variably defined in the literature. Fourth, clinical outcomes were analyzed on a per-knee basis, including bilateral cases. Consequently, patients with bilateral involvement were counted twice, which may have introduced bias in the interpretation of patient-reported outcomes. Finally, long-term follow-up data were lacking, and future studies should aim to evaluate the durability of the outcomes beyond the 2-year postoperative period. Our findings suggest that preoperative evaluation of FT and TT should be included in the decision-making process, particularly in cases of increased FT, where additional interventions (eg, derotational osteotomy) may be necessary.
Conclusion
This study highlights the potential influence of FT on postoperative outcomes following isolated MPFLR using FiberTape. While the procedure restored patellofemoral stability and yielded satisfactory patient-reported outcomes, increased FT showed an association with less favorable results in the sports subscale of the KOOS questionnaire. However, the absence of preoperative and postoperative sports performance data limited our ability to draw conclusions. Nevertheless, these findings underscore the importance of considering preoperative rotational alignment for patients undergoing MPFLR and highlight the need for future prospective studies to guide individualized treatment strategies.
Footnotes
Final revision submitted November 8, 2025; accepted November 9, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.