
Abstract
Background:
Techniques incorporating the long head of the biceps tendon (LHBT) into repair of massive irreparable rotator cuff tears (MIRCTs) have been reported to present good clinical outcomes in a short-term follow-up, but there is a lack of studies with longer observation.
Purpose:
To assess clinical and radiologic results of LHBT redirection with margin convergence repair in patients with MIRCTs in a longer follow-up.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients with at least 2 years of follow-up were enrolled in this retrospective study.
Shoulder range of motion, pain per the numeric rating scale, Constant score, and American Shoulder and Elbow Surgeons questionnaire were assessed. True anteroposterior radiographs were assessed regarding acromiohumeral distance and cuff tear arthropathy per Hamada and Favard classifications. Magnetic resonance imaging scans were analyzed regarding fatty infiltration of supraspinatus (SST) and infraspinatus (IST) according to Goutallier classification and LHBT–rotator cuff construct features.
Results:
The study group involved 45 patients (11 female, 34 male) with a mean age of 65 years (range, 50-77) and mean follow-up of 52 months (range, 24-100). One patient was excluded for reverse shoulder arthroplasty. The mean range of motion was 150° of flexion, 148° of abduction, and 35° of external rotation. The mean pain was 1.0. The mean results were 83.9 in American Shoulder and Elbow Surgeons questionnaire and 71.2 in Constant score. The mean acromiohumeral distance was 5.6 mm (range, 2.0-8.7). On radiographs, cuff tear arthropathy was assessed as grade 1 in 23 patients, grade 2 in 14, grade 3 in 3, and grade 4 in 4. Mild glenoid erosion was observed in 9 patients. Among 35 patients, significant fatty infiltration was observed and graded as 3 in 7 patients for SST and 10 patients for IST and graded as 4 in 1 for SST and 2 for IST. The LHBT was presented intra-articularly in 31 of 35 analyzed magnetic resonance imaging scans and as running directly to the greater tuberosity in 10 of 35. The SST was healed proximally to the LHBT in 28 of 35 patients. One complication (2.2%) and 4 (8.9%) clinical failures were observed.
Conclusion:
At follow-up >2 years, LHBT redirection provided excellent pain-free range of movement, even though muscle strength deficit persisted. The rate of complications and clinical failures seems to be lower than for other nonarthroplasty treatment options for MIRCT.
Keywords
Massive irreparable rotator cuff tears (MIRCTs) remain a challenging-to-treat condition that represents up to 20% of all primary rotator cuff (RC) tears. 16 Even though it is technically possible to repair such a lesion intraoperatively, biological factors such as significant muscle atrophy and high-grade fatty infiltration, tendon retraction to the level of the glenoid, or short tendon remnant may impair the healing process and lead to clinical failure. 17 MIRCT, when left untreated, could lead to development of cuff tear arthropathy (CTA) with significant deterioration in the patient's quality of life and, finally, to end-stage arthrosis. 7
There is general agreement that older patients, especially with pseudoparetic shoulder and irreparable subscapularis tear, may be successfully treated with reverse shoulder arthroplasty (RSA). 27 However, there is no consensus on the best treatment option for patients <60 years of age. 26 Classically, physical therapy, arthroscopic debridement with or without long head of the biceps tendon (LHBT) tenotomy/tenodesis, partial RC repair, graft interpositions, tendon transfers, superior capsular reconstruction (SCR), or balloon arthroplasty was proposed for this specific group of patients.3,13,16 Despite their results at short-term follow-up, such as significant improvement in range of motion (ROM) and patient-reported outcome measurements (PROMs), most of these treatments have not passed the test of time from a variety of causes.8,13 As such, the search continues for other options to treat MIRCT, and the last 5 years have brought new techniques, such as bursal acromial resurfacing, biological tuberoplasty, or different ways of incorporating the LHBT tissue into repairs.1,2,6,10,15,18,21,25
The aim of the study was to determine whether LHBT redirection with margin convergence RC repair may provide good clinical and radiologic results in patients with MIRCT in a longer follow-up period.
Methods
In this retrospective analysis of prospectively collected data, patients were assessed who were diagnosed with MIRCT and treated in our institution between 2016 and 2023 with arthroscopic LHBT redirection with margin convergence posterosuperior RC repair, with at least 2 years of follow-up. Inclusion criteria for surgery involved the following: massive posterosuperior RC tear with a high degree of tendon retraction (grade 3 per Patte classification on magnetic resonance imaging [MRI]), preserved LHBT, fatty infiltration grade ≤4 per Goutallier classification, intact or reparable subscapularis tendon, and no signs of significant omarthrosis (stage <2 per Samilson-Prieto classification and CTA grade <4 per Hamada classification). 19 Operations were performed by 2 high-volume shoulder surgeons and 2 fellowship-trained shoulder surgeons.
Surgical Technique
All procedures were performed under general anesthesia without plexus block with the patient in a beach-chair position. All patients had antibiotic prophylaxis at induction (2 g of cephazolin or 600 mg of clindamycin in case of penicillin allergy). Initially, glenohumeral and subacromial inspections were performed with the 30° arthroscope. Where necessary, subscapularis tendon repair was performed at the beginning of the procedure. Then the arthroscope was switched to the lateral portal, and the irreparability of the posterior RC was confirmed after thorough soft tissue releases and tendon remnant mobilization. The greater tuberosity was prepared with a shaver. A free Hi-Fi Suture (Conmed) was used to perform at least 1 or 2 margin convergence sutures between the supraspinatus (SST) and infraspinatus (IST) remnants and 2 consecutive margin convergence sutures between SST, LHBT and IST (Figure 1).

Arthroscopic view from the lateral portal in the beach-chair position. The left shoulder is being operated on. (A) After thorough release, a free Hi-Fi Suture (white) is pierced through the supraspinatus (SST) and infraspinatus (IST) remnants. (B) The second margin convergence suture is pierced through the IST, long head of the biceps tendon (LHBT), and SST using the Rhino Suture Passer (Arthrex). (C) The view of margin convergence of the IST and LHBT after knot tying. HH, humeral head.
Then the triple-loaded titanium anchor Threvo (Conmed) was placed in the center of the greater tuberosity. In the next step, the first lasso-loop was placed in the IST remnant just medial to the most lateral margin convergence suture (Figure 2A). The second lasso-loop was pierced through the SST and LHBT, again medial to the last margin convergence suture (Figure 2B). The third and last lasso-loop was placed around the LHBT only, as close as possible to the entrance to the sulcus (Figure 2C).

Arthroscopic view from the lateral portal in the beach-chair position. The left shoulder is being operated on. (A) The Rhino Suture Passer (Arthrex) is used to place the lasso-loop suture around the infraspinatus (IST) remnant. (B) The second lasso-loop is placed around the supraspinatus (SST) remnant and long head of the biceps tendon (LHBT). (C) The last lasso-loop is placed around the LHBT only, as close as possible to the entrance to the sulcus. GT, prepared greater tuberosity; HH, humeral head.
At the end, each lasso-loop was retrieved with the second free limb from the same-colored pair, and all sutures were tied with 6 or 7 slip knots (Figure 3).

Arthroscopic view from the lateral portal in the beach-chair position. The left shoulder is being operated on. The whole construction, composed of the infraspinatus (IST), long head of the biceps tendon (LHBT), and supraspinatus, is being brought back to the natural insertion at the greater tuberosity. KP, knot pusher.
This technique was previously published in 2018. 12 Acromioplasty was performed only when necessary, and in such cases coracoacromial ligament was not violated to avoid anterosuperior escape.
After surgery, each patient was placed in an internal rotation brace for 6 weeks. Pendulum exercises began on the first postoperative day. After 4 weeks, each patient was recommended to start a supervised physical therapy program with extended passive ROM and active-assisted ROM exercises. Active ROM was allowed after 6 weeks.
Patient Evaluation
Patients with at least 2 years of follow-up were invited to take part in evaluation with consent. During clinical examination on last follow-up, active shoulder ROM was assessed in forward flexion, abduction, and external rotation, and PROMs were determined by the Constant score (CS) and American Shoulder and Elbow Surgeons (ASES) score, as validated for a Polish population. The level of pain was assessed independently on a numeric rating scale from 0 to 10 points. Complications during the follow-up period were also recorded.
Postoperative true anteroposterior radiographs of the operated shoulder performed during the last follow-up visit were analyzed regarding acromiohumeral distance, CTA development according to Hamada classification, and glenoid erosion according to Favard classification. 4 Postoperative MRI scans were performed in 3 planes (coronal, axial, sagittal) and analyzed in terms of fatty infiltration of the SST and IST according to Goutallier classification and LHBT-RC construction features, such as continuity of reconstruction, the course of the LHBT to the anchor at the greater tuberosity, and the distance between the SST remnant and greater tuberosity. Imaging studies were evaluated by an independent fellowship-trained musculoskeletal radiologist (K.J.K.).
The study was carried out in accordance with human rights, and the study protocol was approved by the local bioethics committee of the District Medical Chamber, Białystok, Poland (OIL/K.B.-375/2017). Informed consent was obtained from all participants in the study. No artificial intelligence was used in preparation of the study and this article.
Results
Sixty patients were identified with a follow-up >2 years. From those patients, 15 were lost to follow-up. One patient was excluded for conversion to RSA. The final study group involved 44 patients (11 female, 33 male) with a mean age of 65 years (range, 50-77). The mean time of last follow-up was 52 months (range, 24-100).
Functional Outcome
The mean postoperative ROM was 150° of forward flexion, 148° of abduction, and 35° of external rotation. Mean postoperative pain per the numeric rating scale was 1.0. Seven patients indicated pain as ≥4. The mean ASES score was 83.9 (range, 50-100), and the mean CS was 71.2 (range, 14-98.3). The mean subscores of the CS were as follows: pain, 11.4 out of a maximum 15; activities of daily living, 16.6 out of 20; ROM, 34 out of 40; strength, 9 out of 25 (Figure 4).

Clinical results in American Shoulder and Elbow Surgeons (ASES) questionnaire and Constant score validated for the Polish population. ADL, activities of daily living; ROM, range of motion. [Green bars indicate a total score in presented scale/subcategory, blue bars indicate the mean result of the study group.]
Radiologic Outcome
The mean acromiohumeral distance was 5.6 mm (range, 2.0-8.7 mm). CTA was assessed as grade 1 in 23 patients, grade 2 in 14, grade 3 in 3, and grade 4 in 4. Signs of glenoid erosion were observed in 9 patients (20%) and assessed as grade 1 in 8 patients and grade 2 in 1 patient according to the Favard classification. The 1 patient with grade 2 glenoid erosion had previously been included in the clinical failure group.
From 44 evaluated patients, 35 had postoperative MRI performed at a mean 53 months (range, 24-102 months). Fatty infiltration was described as grade 1 in 7 patients for SST and 9 patients for IST, grade 2 in 20 and 14 patients, grade 3 in 7 and 10 patients, and grade 4 in 1 and 2 patients. The LHBT was present intra-articularly in 31 analyzed MRI scans, but only in 10 cases did the LHBT run directly to the anchor at the greater tuberosity. The mean distance of the SST remnant to the greater tuberosity was measured as 40.2 mm (range, 22-53), but the SST was healed proximally to the LHBT in 28 patients.
Complications and Failures
During the follow-up period, no immediate complications were observed. One patient required revision surgery owing to loosening of the suture anchor used for subscapularis repair 8 months after primary surgery, a factor not directly associated with the LHBT augmentation technique itself. No other complications were observed in a longer follow-up.
Three patients had other trauma events that led to LHBT-RC remnant construction retear within first 2 years after surgery, although no one required revision surgery. All of them accepted their clinical status after a course of physical therapy. Two patients presented a positive Hornblower sign on clinical examination, which was not associated with the surgical technique itself. Finally, only 1 patient needed conversion to RSA.
In total, 1 complication (2.2%) was observed, and 4 cases (8.9%), including the one with RSA, were marked as surgical failure for not achieving pain-free satisfactory ROM after the procedure.
Discussion
The most important finding is that LHBT redirection with margin convergence cuff repair provides good, almost pain-free ROM in the majority of patients treated for MIRCT in a follow-up >2 years. The mean postoperative pain score was 1.0. Functional outcomes were good to excellent, with a mean ASES of 83.9 and mean CS of 71.2. The complication rate was 2.2%, and 4 clinical failures (8.9%) were observed.
It has been widely discussed in the literature that techniques incorporating the LHBT into repair of MIRCT provides significant improvements in ROM and PROMs at 1- and 2-year follow-up, but they are expected to get worse over time.8,13 Hughes et al 13 reported that in a short-term observation most nonarthroplasty treatment options reduced the level of pain postoperatively to a mean 1 or 2 points per the numeric rating scale, although PROMs varied among surgical techniques. Thus, the ASES was reported as between 74 and 80 points for partial repair, 74 and 94 for SCR, 80 and 90 for subacromial spacers, and 70 for tendon transfers. For the CS, it was reported as 64 to 84 points for debridement, 70 to 89 for partial repair, 64 to 84 for SCR, 60 to 76 for subacromial spacers, and 58 to 74 for tendon transfers. Yet, Ji et al 14 showed that techniques incorporating the LHBT into repair of large and massive RC tears provided significant improvement in pain level—from a mean 7.1 preoperatively to 2.0 postoperatively and with ASES scores from 35 to 83 in a follow-up of 2 years. In our study, patients after LHBT redirection with margin convergence RC repair had a mean postoperative pain score of 1.0, with mean functional outcomes of 83.9 for the ASES and 71.2 for the CS. In comparison with the data presented earlier, our study revealed that good and excellent clinical outcomes may be observed after LHBT augmentation even in the case of irreparable RC tears and even in a longer follow-up period of a mean 4 years.
In our study, radiologic parameters such as acromiohumeral distance, healing and retear rates, and osteoarthritis progression were analyzed, which has not been done in other studies.23,24 Data from the literature suggest that utilizing the LHBT in RC repairs in MIRCT leads to a lower retear rate and an improved healing rate.5,24,28 In contrast, our results do not show the same conclusion when healing is defined as a coaptation of the SST to natural insertion at the greater tuberosity. However, in 28 of 35 patients (80%), the SST had healed proximal to the LHBT, which should be considered as healing of the whole construct in this technique (Figure 5).
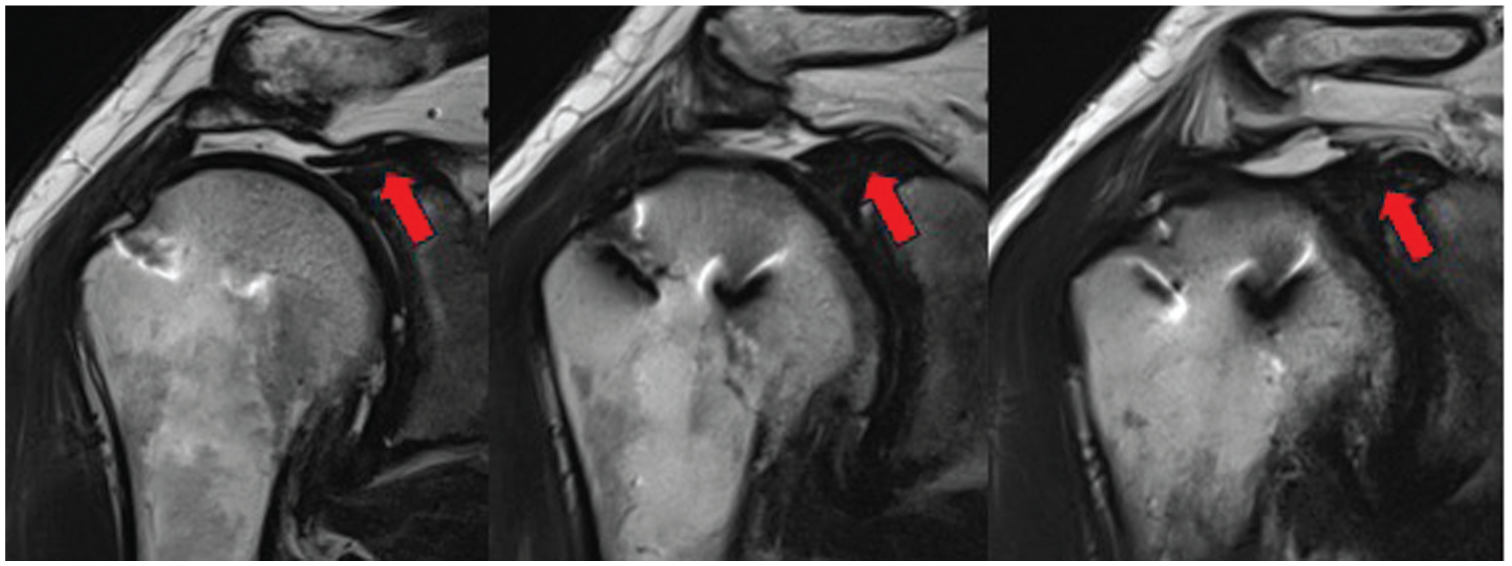
Three slides from T2 coronal magnetic resonance imaging scans of the right shoulder performed 4 years after LHBT redirection illustrate that the supraspinatus remnant healed proximally to the LHBT (red arrows). LHBT, long head of the biceps tendon.
Moreover, Lädermann et al 17 postulated that complete closure of the defect in MIRCT is less important than restoration of a stable fulcrum for normal shoulder kinematics, which likely explains the good clinical results of LHBT redirection with margin convergence repair with a fair MRI presentation. Another important issue in patients with MIRCT, which was additionally analyzed, is the development of CTA. Its progression is associated with impaired shoulder function and limited quality of life. Moreover, continuous glenoid wear and progressive glenohumeral joint deformity can affect the result of the RSA as an ultimate treatment option. 7 In this study, we found that patients treated with LHBT redirection did not have significant glenoid wear and bone loss at a mean follow-up of 53 months. Any signs of glenoid erosion were presented in 9 of 44 patients, but only in 1 case was it graded >1 according to the Favard classification. Moreover, follow-up radiographs revealed significant CTA, graded 3 and 4 according to the Hamada classification, in 7 of 44 patients at least 2 years after LHBT redirection. Finally, in the study group, only 1 patient required revision to RSA for a nonfunctional RC and CTA development at 35 months from initial surgery.
In summary, an LHBT redirection was performed without cutting its labral attachment and by suturing the IST and SST remnants to the proximal part of LHBT with a margin convergence technique. The whole construct was then anchored to the greater tuberosity using lasso-loop sutures with threads from a triple-loaded titanium suture anchor. This way, not only were the great mechanical properties of the LHBT as SCR utilized, but a new motor unit was also created by connecting the SST and IST muscle bellies with greater tuberosity through the LHBT. 9 Thus, we believe that the presented technique is a dynamic mechanobiological reinforcement, which differentiates it from other mechanical or biological solutions presented in the literature.1,5,11 Moreover, from the very beginning, only 1 triple-loaded titanium suture anchor positioned in the center of the greater tuberosity was used, and the construction was fixed with the arm in 30° of abduction. It was recently shown that fixation in this way is the most effective in reducing posteroanterior humeral head translation. 22 As only 1 suture anchor and a single, locally available autograft are used for the whole construction, the technique seems to be the most cost-effective when compared with other techniques in the literature.20,28 Furthermore, it is readily reproducible and easy to revise, and it does not exhaust other treatment options.
There are also some disadvantages of this technique. Even though it meets high patient satisfaction and yields good clinical results, significant muscle strength deficits persist, as reflected in the CS. In addition, the redirection of the LHBT at the greater tuberosity and the margin convergence among IST, LHBT, and SST results in both muscle bellies having 1 point of fixation at the humeral head, which can lead to limited external rotation restoration in position I. Interestingly, external rotation limitation in position II was not an issue, and only 2 patients presented a positive Hornblower sign. This finding can indicate the high importance of proper teres minor function for LHBT redirection with margin convergence RC repair.
Our study also has some limitations. The most important drawback is that it was a retrospective analysis with no control group. Additionally, from the 60 patients who underwent surgery, 45 responded positively to our invitation, with 25% lost to follow-up. Consequently, the final study group was small. Another limitation is that only postoperative results from the last follow-up were included without a comparison with preoperative data. Finally, while clinical examination, PROMs, and radiographic analysis were performed for all 44 patients in the study group, just 35 had follow-up MRI scans.
To our knowledge, there is a limited number of studies presenting >2 years of clinical and radiologic results of utilizing LHBT tissue in the treatment of MIRCT. It has been widely discussed in the literature that techniques incorporating LHBT into repair of MIRCT provide significant improvements in ROM and PROMs at 1- and 2-year follow-up, but these are expected to worsen over time.8,13 Our study shows good and excellent clinical results at longer term. The mean follow-up for our study group was >4 years, with the greatest being as long as 9 years. From those, 26 patients presented follow-up >4 years, including 15 exceeding 6 years. During observation, only 2 of 45 patients required revision surgery, but it should be noted that 1 of them had it performed because of complications not associated with the LHBT redirection technique itself. The overall complication rate in this study was 2.2% and the clinical failure rate was 8.9%. This technique seems to be superior to a “gold standard” nonarthroplasty treatment option for MIRCT, specifically partial RC repair, which has a reported failure rate as high as 14%. 16 Furthermore, until now the lowest rate of complications has been reported for SCR (5%) and arthroscopic debridement (6%), whereas tendon transfer and graft interposition techniques have a >20% rate of complications. 16 The current study and past ones thus outline the complexity and difficulty of treating patients with MIRCT.
Conclusion
In follow-up >2 years, LHBT redirection with margin convergence RC repair provides excellent, pain-free range of movement, even though muscle strength deficit persists. The rate of complications and clinical failures seems to be lower than for other nonarthroplasty treatment options available for MIRCTs.
Footnotes
Final revision submitted January 6, 2026; accepted February 16, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the local bioethics committee of the District Medical Chamber, Białystok, Poland (OIL/K.B.-375/2017).
Data Availability Statement
All data available upon request from the corresponding author.