
Abstract
Background:
Anterior cruciate ligament reconstruction (ACLR) using a quadriceps tendon with bone (QTB) autograft has been associated with reduced quadriceps strength at 6 months postoperatively compared to other autograft options. However, limited studies have assessed strength recovery after return to sports after ACLR, particularly involving QTB autografts.
Purpose:
To examine factors influencing quadriceps strength recovery at 6 and 12 months after ACLR using QTB, bone–patellar tendon–bone (BPTB), and hamstring tendon (HT) autografts.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Individuals who underwent primary ACLR using QTB, BPTB, or HT autografts, had a preinjury Tegner activity scale (TAS) score >5, and completed at least 12 months of follow-up were included. Participants were classified into recovery (>90%) and nonrecovery (≤90%) groups based on the limb symmetry index of quadriceps strength compared to the contralateral leg at 6 and 12 months post-ACLR. Variables associated with quadriceps strength recovery at these time points were analyzed.
Results:
A total of 154 participants were included. Multivariable logistic regression showed that use of QTB (OR, 0.11; P < .001) or BPTB (OR, 0.12; P < .001) autografts, meniscal repair (OR, 0.34; P = .013), and lower preinjury TAS score (OR, 1.68; P = .011) were associated with a significantly increased risk of quadriceps strength deficit at 6 months after ACLR. At 12 months after ACLR, lower preinjury TAS score (OR, 1.48; P = .046) and lower Knee injury and Osteoarthritis Outcome Score (KOOS) pain at 3 months (OR, 1.09; P = .002) were associated with a significantly increased risk of quadriceps strength deficit. The receiver operating characteristic curve showed that a KOOS pain value at 3 months after ACLR of 83.1 points was the cutoff for indicating a strength deficit at 12 months (sensitivity, 78.4%; specificity, 59.1%).
Conclusion:
Use of QTB or BPTB autografts, meniscal repair, and lower preinjury TAS score were factors associated with quadriceps strength deficit at 6 months after ACLR. At 12 months, lower preinjury TAS score and lower KOOS pain at 3 months were factors associated with persistent strength deficit.
Keywords
Anterior cruciate ligament (ACL) injuries are among the most common knee injuries, with an annual incidence of 68.6 per 100,000 persons. 35 The standard treatment for ACL injury is arthroscopic ACL reconstruction (ACLR) using anatomic bone tunnels in the femur and tibia, typically using either a hamstring tendon (HT) or bone–patellar tendon–bone (BPTB) autograft. 27 Previous studies have shown that ACLR provides favorable clinical outcomes regardless of graft type.5,12,32 However, each autograft has limitations: BPTB autografts may lead to anterior knee pain and kneeling difficulty,6,28 while HT autografts are associated with a higher risk of graft failure, reinjury, and strength deficits in hip extension and knee flexion.7,16,34
Quadriceps tendon (QT) autografts have recently gained popularity, offering a larger graft diameter and more favorable tensile properties compared to BPTB and HT autografts. 26 Studies have shown that QT or QT with bone (QTB) autografts provide comparable postoperative stability and failure rates to BPTB autografts, while causing less donor site and anterior knee pain during kneeling,18,23,28,33 and offer superior stability, lower failure rates, and better flexor strength recovery than HT autografts.24,30 However, quadriceps strength deficits have been reported more frequently after QT, QTB, and BPTB autografts, and these grafts may require a longer period of functional recovery compared with HT autografts.9,17,20,21 Nevertheless, some patients receiving HT autografts may also experience quadriceps weakness.39,40 Therefore, restoration of quadriceps strength remains an important rehabilitation challenge across all graft types.
Quadriceps strength recovery after ACLR is associated with hop performance,8,10 self-reported knee function,10,19,41 and return to preinjury sports.25,29 Furthermore, lack of quadriceps strength recovery increases the risk of knee osteoarthritis31,38 and second ACL injury. 13 Therefore, graft-related differences in quadriceps strength recovery may influence return-to-sports testing performance and safe resumption of unrestricted activity, highlighting the need to clarify how graft type affects postoperative strength recovery.
Quadriceps strength recovery after ACLR with QT autografts remains underinvestigated, particularly beyond 8 months, and long-term outcomes remain controversial. 21 Identifying factors influencing postoperative quadriceps strength recovery in individuals receiving QTB, BPTB, or HT autografts may help guide graft selection and optimize rehabilitation strategies.
Therefore, the purpose of this study was to identify factors affecting quadriceps strength recovery at 6 and 12 months after ACLR with QTB, BPTB, and HT autografts. It was hypothesized that graft type would significantly influence strength recovery at 6 months after ACLR, but not be an independent predictor at 12 months.
Methods
This study was approved by the ethics committee (ID: 2024-004D) and the internal review board of our institution, and informed consent was obtained from all participants. We retrospectively reviewed medical records of individuals who underwent primary ACLR using QTB, BPTB, or HT autografts and visited our outpatient clinic between April 2018 and April 2024. Inclusion criteria were (1) primary ACLR using QTB, BPTB, or HT autografts; and (2) sports participation with Tegner activity scale (TAS) score >5. Exclusion criteria were (1) multiple-ligament reconstruction; (2) prior surgery or other knee injuries in the affected or contralateral knee; (3) additional treatment such as osteotomy, except meniscal repair or meniscectomy; (4) ACLR using single-bundle HT autografts; (5) additional surgery after ACLR; (6) ACL graft rupture or contralateral injury within 12 months post-ACLR; and (7) follow-up duration <12 months or missing measurement data.
Surgical Technique and Rehabilitation
In single-bundle ACLR using QTB autografts, the full-thickness QT was harvested, leaving a capsule with a 15 mm–long, 9 or 10 mm–wide, and 9 mm–deep patellar bone block. The QT length was 50 to 70 mm depending on the patient's height. 15 The tibial tunnel was first made using an ACL tip guide; then, the femoral tunnel was created using a modified transtibial technique with gradual tibial reaming. 36
In ACLR using BPTB autografts, the central third of the patellar tendon and 9 or 10 mm–wide and 15 mm–long bone blocks were obtained from the patella and tibial tubercle. The tibia and femoral tunnel were created using a modified transtibial technique with gradual tibial reaming, in the same fashion as using QTB autografts. 36
In double-bundle ACLR using HT autografts, the transportal double-bundle technique was used. 37 Femoral and tibial tunnels were drilled using drill bits that matched the diameter of grafts in 0.5-mm steps. In each cases, femoral fixation was performed with a titanium button (EndoButton CL; Smith & Nephew), graft ends were sutured with No. 3 Elp sutures (Akiyama) in a Krackow stitch manner, and tibial fixation of the graft was accomplished at 20° of knee flexion through the application of 20 N of initial tension with final fixation via a double-spike plate (Meira) with a 5.5-mm screw.
Graft selection was based on the patient's preference after a detailed explanation of the advantages and disadvantages of each graft by the operating surgeon (Y.H., S.Y., and 5 other senior surgeons). Meniscal repairability was assessed according to standard repair guidelines during ACLR. Simple or bucket-handle tears without degeneration were repaired, while complex or degenerative tears were partially resected.
At 24 hours postoperatively, participants began a rehabilitation program including isometric quadriceps strengthening and straight leg–raising exercises using a knee immobilization brace for 1 week. Patients who underwent only ACLR were permitted to begin partial weightbearing, and knee range of motion exercises were initiated at 1 week postoperatively; full weightbearing was permitted at 5 weeks. Patients who underwent ACLR and meniscal repair were permitted to start partial weightbearing from 3 weeks after surgery, with full weightbearing permitted at 6 weeks. Low-impact activity (including jogging) was allowed at 4 months, and vigorous sports activities were resumed at approximately 8 months.
Data Collection
The following demographic data were obtained from medical records: age at surgery, sex, body mass index (BMI), preinjury TAS score, time from injury to surgery, graft type (QTB, BPTB, or HT), and meniscal repair. Postoperative knee pain was assessed at 3, 6, and 12 months using the Knee injury and Osteoarthritis Outcome Score (KOOS) pain subscale. Quadriceps strength and donor site morbidity (DSM) scores 1 were collected at 6 and 12 months post-ACLR. At 12 months, participants were evaluated for anterior-posterior stability using side-to-side difference (SSD) in anterior tibial translation measured with a KT-1000 arthrometer (Medmetric) with manual maximum pull (KT measurement), rotational stability according to the pivot-shift test (grade 0, equal; grade 1, glide; grade 2, clunk; and grade 3, gross), and return to sports.
Maximum isometric quadriceps strength was assessed with participants seated at the edge of the treatment table, knees flexed at 90°. 3 A handheld dynamometer (μTas F-1; ANIMA Co) was applied to the anterior aspect of the distal tibia above the talar dome, and participants extended their knees with maximal effort. Isometric strength was recorded in 3 trials, and the limb symmetry index (LSI) was calculated as the mean strength of the operated leg divided by the nonoperated leg multiplied by 100. Quadriceps strength assessments were undertaken by an experienced, qualified physical therapist (N.A., and 2 other physical therapists) in the same private orthopaedic outpatient clinic. Because scar locations differed between graft types, blinding of the assessor was not feasible.
Participants were categorized into good recovery (GR) and poor recovery (PR) groups based on an LSI ≥90% or <90% at 6 and 12 months after surgery. According to Grindem et al, 13 quadriceps LSI <90% is associated with an elevated risk of knee reinjury.
Statistical Analysis
The chi-square or Fisher exact test was used for categorical variables, and the Student t test or Mann-Whitney U test was used for continuous variables. Normal distribution was assessed using the Shapiro-Wilk test for continuous variables. A logistic regression model was used to obtain univariate and multivariate odds ratios with 95% confidence intervals for quadriceps strength recovery. Multivariable logistic analyses were performed to adjust for confounding factors with a P value <.1 in univariate analysis that may influence quadriceps strength recovery. The receiver operating characteristic (ROC) curve for KOOS pain at 3 months after ACLR was generated to identify the cutoff value of KOOS pain as a predictor of quadriceps strength recovery at 12 months. The relationships between KOOS pain at 3 months after ACLR and graft type, preinjury TAS scores, and sex were analyzed using the Kruskal-Wallis test, Spearman rank correlation coefficient, and Mann-Whitney U test, respectively.
Analyses were performed using SPSS statistics 28 (IBM). Statistical significance was set at a P value <.05.
Results
We retrospectively recruited 279 consecutive participants who underwent primary ACLR using QTB, BPTB, or HT autografts. A total of 21 participants with preinjury TAS scores <5, 12 with multiple-ligament reconstruction, 27 with a prior surgery or other knee injuries in the affected or contralateral knee, and 2 who received additional treatment (eg, knee around osteotomy) were excluded. Eighteen who underwent ACLR using single-bundle HT autografts were also excluded. Additionally, 1 participant who underwent further meniscal surgery after ACLR, 5 with ACL graft rupture or contralateral ACL injury (4 with HT autograft and 1 with QTB autograft) within 12 months, and 39 with <12 months of follow-up or missing measurement data were excluded. A total of 154 participants were included in the final analysis (Figure 1).

Flow diagram depicting the patients with anterior cruciate ligament reconstruction (ACLR) included in the present study along with reasons for exclusion at each stage. BPTB, bone–patellar tendon–bone autograft; HT, hamstring tendon autograft; QTB, quadriceps tendon with bone autograft.
The mean age at surgery was 24.8 ± 11.1 years. Among the 154 participants, 59 were male and 95 were female. Graft type distribution included 44 QTB, 41 BPTB, and 69 HT autografts (Table 1). Preinjury TAS scores differed among graft types, with higher scores observed with BPTB autografts than with HT autografts (7.9 ± 1.4 vs 7.0 ± 1.4; P = .001).
Comparison Between the GR and PR Groups at 6 and 12 Months After ACLR a

Values are presented as mean (SD) or n (%). Bold P values indicate statistical significance (P < .05). Dashes indicate not applicable. ACLR, anterior cruciate ligament reconstruction; BMI, body mass index; BPTB, bone–patellar tendon–bone; DSM, donor site morbidity; GR, good recovery; HT, hamstring tendon; KOOS, Knee injury and Osteoarthritis Outcome Score; LSI, limb symmetric index; PR, poor recovery; QTB, quadriceps tendon with bone; SSD, side-to-side difference; TAS, Tegner activity scale.
KT measurement indicates KT-1000 arthrometer with manual maximum pull.
Postoperative Clinical Evaluation
The mean LSI of quadriceps strength increased from 83.5% ± 13.8% (QTB, 77.9% ± 15.0%; BPTB, 80.6% ± 14.8%; HT, 88.8% ± 12.5%) at 6 months after ACLR to 92.6% ± 11.9% (QTB, 91.4% ± 13.5%; BPTB, 92.5% ± 14.7%; HT, 93.3% ± 11.4%) at 12 months (Tables 1 and 2). The mean KOOS pain improved from 86.1 ± 12.3 at 3 months to 89.9 ± 9.4 at 6 months and 93.0 ± 9.5 at 12 months. The mean DSM score decreased from 24.0 ± 17.4 at 6 months to 16.1 ± 17.8 at 12 months. The mean KT measurement SSD at 12 months was 0.6 ± 1.3. The pivot-shift test at 12 months was grade 0 in 83.1%, grade 1 in 15.6%, and grade 2 in 1.3% (Table 1). Return-to-sports rates were 77.3%, 78.0%, and 72.5% for the QTB, BPTB, and HT autografts, respectively (P = .757).
Quadriceps Strength Recovery Between the Graft Types a

Values are presented as mean (SD). BPTB, bone–patellar tendon–bone; HT, hamstring tendon; LSI, limb symmetric index; QTB, quadriceps tendon with bone.
Deficient Quadriceps Muscle Strength 6 Months After ACLR
Of the 154 eligible participants, 49 (31.8%) were in the GR group and 105 (68.2%) in the PR group. In the univariate model, BMI, preinjury TAS score, graft type, and meniscal repair were associated with a significantly increased risk of quadriceps strength deficit at 6 months post-ACLR (Table 1).
Multivariable logistic regression showed that use of QTB (OR, 0.11; 95% CI, 0.03-0.36; P < .001), use of BPTB (OR, 0.12; 95% CI, 0.03-0.38; P < .001), meniscal repair (OR, 0.34; 95% CI, 0.14-0.79; P = .013), and lower preinjury TAS score (OR, 1.68; 95% CI, 1.12-2.51; P = .011) were associated with an increased risk of quadriceps strength deficit at 6 months (Table 3).
Multivariable Logistic Analysis for the Association With Quadriceps Strength Deficit at 6 and 12 Months After ACLR a

Bold P values indicate statistical significance (P < .05). Dashes indicate not applicable. ACLR, anterior cruciate ligament reconstruction; BMI, body mass index; BPTB, bone–patellar tendon–bone; DSM, donor site morbidity; HT, hamstring tendon; KOOS, Knee injury and Osteoarthritis Outcome Score; QTB, quadriceps tendon with bone; Ref, reference; TAS, Tegner activity scale.
Deficient Quadriceps Muscle Strength 12 Months After ACLR
Of the 154 eligible participants, 103 (66.9%) were in the GR group and 51 (33.1%) in the PR group. In the univariate model, preinjury TAS score; KOOS pain values at 3, 6, and 12 months post-ACLR; and DSM scores at 6 and 12 months were associated with quadriceps strength deficit at 12 months (Table 1).
Multivariable logistic regression showed that lower preinjury TAS score (OR, 1.48; 95% CI, 1.00-2.17; P = .046) and lower KOOS pain at 3 months (OR, 1.09; 95% CI, 1.03-1.15; P = .002) were associated with an increased risk of quadriceps strength deficit at 12 months (Table 3).
The area under the ROC curve for KOOS pain at 3 months post-ACLR, as a predictor of quadriceps strength deficit at 12 months, was 69.6%, and the best cutoff value was 83.1 points (sensitivity, 78.4%; specificity, 59.1%) (Figure 2).
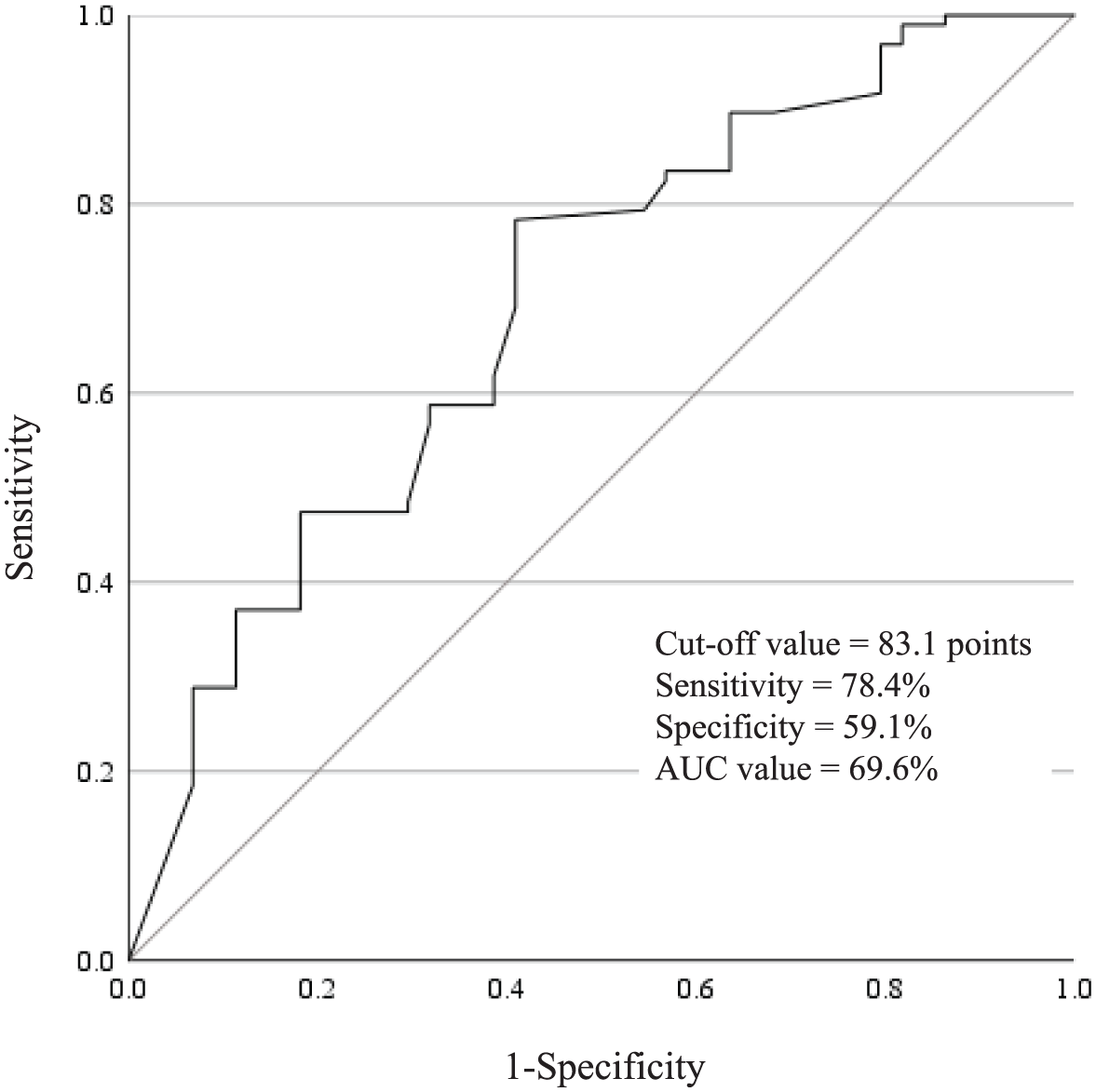
Receiver operating characteristic (ROC) curve of Knee injury and Osteoarthritis Outcome Score (KOOS) pain at 3 months as a predictor of quadriceps strength deficit at 12 months after anterior cruciate ligament reconstruction (ACLR). The area under the curve (AUC) was 69.6%. Based on ROC analysis, a KOOS pain cutoff of 83.1 points at 3 months best indicated quadriceps strength deficit at 12 months post-ACLR.
Association Between KOOS Pain at 3 Months After ACLR and Graft Types, Preinjury TAS Scores, and Sex
At 3 months, KOOS pain values for the QTB, BPTB, and HT autografts were 87.4 ± 10.1, 88.0 ± 13.1, and 83.7 ± 14.6, respectively, demonstrating no significant differences among the graft types. No significant correlation was observed between 3-month postoperative KOOS pain and preinjury TAS scores (r = 0.131; P = .120). Additionally, no significant sex-based differences were found in KOOS pain at 3 months (86.9 ± 9.1 for male vs 85.5 ± 14.2 for female; P = .750).
Discussion
The most important finding of this study was that use of QTB and BPTB autografts was associated with quadriceps strength deficit at 6 months after ACLR, but not at 12 months, and that early postoperative KOOS pain values and lower preinjury activity level were associated with quadriceps strength deficit at 12 months. In the present study, graft type significantly influenced quadriceps strength recovery at 6 months after ACLR, but it was not identified as an independent predictor at 12 months, in support of the first hypothesis.
This is consistent with previous studies reporting significant differences in early quadriceps recovery after QT versus HT autografts.9,17,20,21 Specifically, Johnston et al 21 conducted a systematic review and meta-analysis of quadriceps strength recovery after ACLR using QT autografts and found that between 5 and 8 months postoperatively, strength was not significantly different compared to that after use of BPTB autografts but was reduced after use of HT autografts. The present findings align with those results, suggesting that graft type is an important factor influencing quadriceps strength recovery at 6 months post-ACLR. In a prospective cohort study, Ebert et al 9 reported that quadriceps strength deficit was greater in the QT group than in the HT group and persisted for 12 months. In the present study, graft type was not independently associated with an increased risk of quadriceps strength deficit at 12 months post-ACLR. This may be due to participants in the present study being younger and more physically active than those in the study by Ebert et al. 9
Several studies have reported that meniscal injury, repair, or excision was not associated with a significantly increased risk of quadriceps strength deficit at 12 months after ACLR.14,40 This finding was consistent with the present study at 12 months. However, meniscal repair was associated with quadriceps strength deficit at 6 months post-ACLR. Fan et al 11 conducted a systematic review and meta-analysis of weightbearing rehabilitation protocol after ACLR and found that delayed weightbearing rehabilitation slows recovery of quadriceps strength in the early postoperative period compared with accelerated weightbearing. These results suggest that delayed weightbearing due to meniscal repair may contribute to the strength deficit in the early postoperative period.
Ueda et al 40 reported that preinjury sport level was a factor associated with quadriceps strength deficit 12 months after ACLR using an HT autograft. In the present study evaluating ACLR using QTB, BPTB, and HT autografts, lower preinjury TAS scores were associated with a significantly increased risk of quadriceps strength deficit at both 6 and 12 months after ACLR. These findings suggested that, regardless of graft type, lower preinjury activity levels are associated with a reduced potential for quadriceps strength recovery after ACLR. Therefore, rehabilitation programs tailored to preinjury activity level may be needed to optimize quadriceps recovery after ACLR.
Previous studies have suggested that knee pain may delay muscle strength recovery after ACLR.14,39 In the present study, KOOS pain at 3 months post-ACLR was associated with quadriceps strength deficit at 12 months. Additionally, among participants with strength deficits at 12 months, KOOS pain at 3 months was 79.7 ± 15.7, which was lower than the Patient Acceptable Symptom State threshold of 80.56 points, 4 the absolute score at which patients consider their condition satisfactory. Additionally, the 3-month KOOS did not differ significantly among graft types and was not significantly associated with preinjury activity level or sex. These findings suggest that early postoperative pain may influence subsequent quadriceps strength recovery independent of graft type, preinjury activity level, or sex. The cutoff value for KOOS pain at 3 months post-ACLR determined in the present study was 83.1 points. Therefore, if KOOS pain does not exceed 83 points at 3 months, clinicians should consider intensifying rehabilitation to ensure the quadriceps strength index surpasses 90% by 12 months post-ACLR. There are several potential contributors to knee pain after ACLR, including DSM, sex, age, and preoperative pain.28,32 In the present study, no statistically significant differences were found in the rate of meniscal repair, graft type, or DSM at 12 months post-ACLR. The precise cause of knee pain after ACLR remains unclear. Future studies are needed to further elucidate its underlying mechanisms.
Limitations
There were some limitations to this study. First, this study included a relatively limited number of patients compared with the total number of patients in whom ACLR was performed during the study period. In addition, some data loss and follow-up attrition occurred, and the relatively low events-per-variable values in our multivariate models may limit the stability of the regression estimates. Therefore, the results of the multivariate analysis should be interpreted with caution. Second, variables related to postoperative quadriceps strength recovery, such as preoperative quadriceps strength and cartilage injury, were not assessed. However, most factors identified in previous studies were included. Third, the follow-up period was relatively short. Therefore, surveillance for graft rerupture and contralateral ACL injury may have been insufficient, and longer-term follow-up is required to more accurately evaluate these outcomes. Nonetheless, 1 year of postoperative muscle strength is a reasonable endpoint, considering the timeline for return to sports. 22 Fourth, strength was assessed using isometric testing; isokinetic measures may have provided more robust evaluations. However, prior studies have demonstrated that isometric quadriceps strength testing performed at 90° of knee flexion provides valid and reliable measurements and represents a reasonable alternative to isokinetic assessment.2,3 Fifth, the sensitivity and specificity of KOOS pain at 3 months on ROC analysis were modest. This may be due to the multifactorial nature of postoperative strength recovery, including influences from age, sex, graft type, pain, and rehabilitation. Sixth, this study was retrospective in design and graft selection was not randomized, which may have introduced selection bias. Indeed, preinjury activity level differed among graft types. Although preinjury TAS scores were included as a covariate in the multivariate analysis, residual confounding cannot be completely excluded. Seventh, the surgical technique differed between the graft types, including the number of bundles, femoral tunnel drilling, and graft diameter. Finally, the varied location of scars between the 3 autografts made blinding of the physical therapist who performed the assessments difficult. Despite these limitations, this study offers valuable insights for designing more effective rehabilitation programs after ACLR.
Conclusion
Use of QTB or BPTB autografts, meniscal repair, and lower preinjury TAS scores were associated with quadriceps strength deficit at 6 months after ACLR. At 12 months, lower preinjury TAS scores and lower KOOS pain values at 3 months were associated with quadriceps strength deficit.
Footnotes
Final revision submitted February 7, 2026; accepted February 13, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Kishima Medical Corporation (ID: 2024-004D).