
Abstract
Background:
Achilles tendinopathy is one of the most prevalent lower limb tendinopathies that, while commonly present in physically active people, can affect men and women of all ages and lifestyles. Although this condition can significantly affect patients’ daily lives, not much is known regarding that which contributes to negative influences on patients’ physical activity.
Purpose:
To explore the association between objectively measured physical activity behavior and pain, kinesiophobia, pain catastrophizing, and symptoms of central sensitization in patients with midportion Achilles tendinopathy.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
For 130 adult patients with midportion Achilles tendinopathy (mean age, 47; 55% female), physical activity was measured via wrist-worn actigraphy and assessed as daily step count and active minutes. The latter includes lightly, fairly, and very active minutes, as well as total active minutes. Linear regression analyses explored the relationship between physical activity behavior and pain intensity, pain interference, kinesiophobia, pain catastrophizing, and central sensitization. All analyses were controlled for age and sex.
Results:
A significant association was found between pain intensity and participants’ daily step count scores (regression coefficient, −591; 95% CI, −994 to −187) and very active minutes (regression coefficient, −3.76; 95% CI, −5.86 to −1.67). Pain intensity was not significantly associated with patients’ total, lightly, or fairly active minutes. Similarly, no significant associations were found between physical activity and pain interference, kinesiophobia, pain catastrophizing, and symptoms of central sensitization.
Conclusion:
Only pain intensity of patients with midportion Achilles tendinopathy is significantly associated with their daily steps and time spent being very physically active, as determined via actigraphy.
Achilles tendinopathy is one of the most common lower limb tendinopathies, with an estimated prevalence of 6% in both athletic and nonathletic individuals.32,44 It is considered an overuse injury that mostly occurs in physically active people, though it can affect men and women of all ages and lifestyles.16,32,44 While Achilles tendinopathy initially presents itself as localized tendon pain and stiffness after moments of inactivity, over time, patients will experience pain with walking, thus severely limiting their ability to work or practice their hobbies. 21 As such, it can negatively affect patients’ daily activity behavior, rendering them more inactive over time.9,21
Recently, there has been a growing interest in considering psychological factors, including pain-related cognitions, as contributors negatively influencing patient-reported outcomes in patients with Achilles tendinopathy.20,37,38,41 Kinesiophobia, the fear of pain related to movement, is associated with decreased quality of life and increased disability, pain, and symptom severity in patients with Achilles tendinopathy. 42 Additionally, kinesiophobia is suggested to be a debilitating factor hindering patients with Achilles tendinopathy from becoming or remaining physically active.8,37 This is in line with the role of kinesiophobia as described in the well-known fear-avoidance model for musculoskeletal pain. 43 The fear-avoidance model explains how a maladaptive interpretation of a pain experience can lead to pain catastrophizing (ie, having catastrophic thoughts and feelings regarding pain), which in turn can develop into kinesiophobia and activity avoidance behavior, ultimately leading to disuse, disability, and persistent pain. 43 Similarly, pain catastrophizing, also a key factor in the fear-avoidance model, has been shown to correlate negatively with patients’ self-reported participation, indicating a potential association with their physical activity behavior. 37 Nevertheless, so far, no significant relationship between kinesiophobia or pain catastrophizing and self-reported physical activity scores has been reported in patients with Achilles tendinopathy, though studies assessing the relationship between such pain-related cognitions and objective physical activity levels are lacking.37,42
Furthermore, central sensitization, defined as “an amplification of neural signaling within the central nervous system that elicits pain hypersensitivity,” has been suggested as a relevant factor in some patients with persistent tendinopathy, though the evidence is still conflicting.10,23,27,28,47 While a negative association between central sensitization and physical activity behavior has recently been reported in other patients with musculoskeletal pain, this relationship has not yet been studied in those with Achilles tendinopathy.17,48
Though the negative relationship between physical activity and pain intensity in patients with musculoskeletal pain is generally well-established, strong evidence linking patients’ pain and their daily physical activity behavior seems lacking in patients with Achilles tendinopathy.4,13,18 More so, these findings are often limited by the use of self-reported physical activity measures.9,26 Though the latter are widely used collection tools for physical activity, they also come with limitations, such as recall bias.29,36 So far, only preliminary evidence has been found indicating no association between patients’ pain intensity and their objective physical activity behavior (eg, as assessed via a wearable activity tracker), highlighting the need for further studies to investigate this relationship. 40
Therefore, the aim of this analysis is to explore the associations between objectively measured physical activity behavior and pain, kinesiophobia, pain catastrophizing, and self-reported symptoms of central sensitization in patients with midportion Achilles tendinopathy. We hypothesized that fewer daily steps and time spent being physically active are associated with elevated pain, kinesiophobia, pain catastrophizing, and symptoms of central sensitization.
Methods
Design and Setting
This study was a retrospective secondary analysis using baseline data from a longitudinal clinical trial that aimed to assess sex differences in treatment outcomes among patients with midportion Achilles tendinopathy. Baseline data for the trial were collected between June 2018 and February 2023 at the University of Delaware, Newark, Delaware, in the United States. The trial protocol was prospectively registered at ClinicalTrials.gov (NCT03523325) and was approved by the institutional review board at the University of Delaware. No changes to the protocol were made following the start of the study.
Participants
All participants included in the longitudinal trial had to be between 18 and 65 years old and diagnosed with midportion Achilles tendinopathy based on clinical diagnostic tests and their self-reported pain and symptoms during activity. 22 Participants were excluded if they had insertional Achilles tendinopathy, history of Achilles tendon rupture, recent steroid injection in the Achilles tendon, or any additional injury that might prevent them from participating in an exercise program. All participants provided written informed consent before study enrollment.
Data Collection
During participants’ initial assessment, demographic data (age, sex, ethnicity, body mass index), symptom duration, and injury location (left, right, or both) were collected. Symptom severity was evaluated using the Victorian Institute of Sport Assessment–Achilles. 34 Additionally, participants were asked whether they identified as being a runner, jumper, or both.
The Patient-Reported Outcomes Measurement Information System–29 (PROMIS-29) was used to evaluate participants’ pain intensity (PROMIS Pain) and pain interference for functioning (PROMIS Interference). 5 The PROMIS Pain measures participants’ pain intensity using an 11-point numeric rating scale ranging from 0 (“No pain”) to 10 (“Worst imaginable pain”). 5 PROMIS Interference is scored using a T-score metric (mean ± SD, 55 ± 10.8), with a higher score representing more pain interference for functioning. 5 Kinesiophobia was assessed using the Tampa Scale for Kinesiophobia (TSK) for which the total score can range from 17 to 68 with higher scores indicating higher levels of kinesiophobia. 12 Pain catastrophizing was evaluated using the Pain Catastrophizing Scale (PCS) with scores ranging from 0 to 52 and higher scores indicating a higher degree of catastrophizing. 39 Self-reported symptoms of central sensitization were collected using the Central Sensitization Inventory (CSI) part A. This questionnaire lists 25 statements on symptoms indicative of central sensitization and results in a total score between 0 and 100. 19
Following the initial assessment, participants were given a Fitbit Inspire activity monitor (Fitbit Inc), a wrist-worn actigraphy device, to assess physical activity behavior. Fitbit activity trackers are known to systematically underestimate step count and activity intensity relative to reference standards. 7 Nonetheless, their performance is generally considered acceptable, 7 and they remain widely used and regarded as reliable tools in clinical research settings.2,3,31,45 Participants were instructed to wear their Fitbit device during waking hours while participating in the 1-year study and to synchronize it with the corresponding app on a daily basis. For this secondary analysis, data from the first 2 weeks following study enrollment were collected. While the Fitbit was being worn, it tracked participants’ steps and active minutes. All collected data via de the Fitbit activity trackers were processed via a device- and company-specific algorithm (Fitbit Inc). Daily Fitbit data were synced and accessed via Fitabase, an independent research data platform (Small Steps Labs, LLC). Using these data, daily step count was calculated as the mean number of steps participants took on a daily basis. Daily active minutes were categorized as lightly active (1.6-2.9 metabolic equivalents of task [METS]), fairly active (3.0-5.9 METS), and very active (≥6.0 METS), as calculated by Fitbit's proprietary algorithm. 1 Additionally, minutes from all categories were summed to calculate total active minutes (≥1.6 METs). Daily active minutes were averaged for each category. Minimum wear time to include Fitbit data in this secondary analysis was determined to be ≥7 days with nonzero step count during the 2-week assessment period. 6 As such, data from patients who consistently performed a minimum number of daily steps (eg, because of severe symptoms) could also be included in the analysis.
All study data were collected, managed, and de-identified using REDCap electronic data capture tools hosted at the University of Delaware.14,15
Statistical Analysis
First, the normality of all relevant variables was checked. Second, a sensitivity analysis was completed to compare characteristics between participants achieving minimum Fitbit wear time and those who did not using Mann-Whitney U tests and chi-square tests. Next, associations between physical activity behavior and pain intensity, pain interference, kinesiophobia, pain catastrophizing, and symptoms of central sensitization were analyzed using linear regression models. For each physical activity measure, 5 regression models were constructed with either the PROMIS Pain, PROMIS Interference, TSK, PCS, or CSI as independent variables. All regression models were controlled for participants’ age and sex. For all analyses, the significance level was set to .05. Statistical analysis was performed in R Studio Version 2024.09.0+375 (R Version 4.2.2). 30
Results
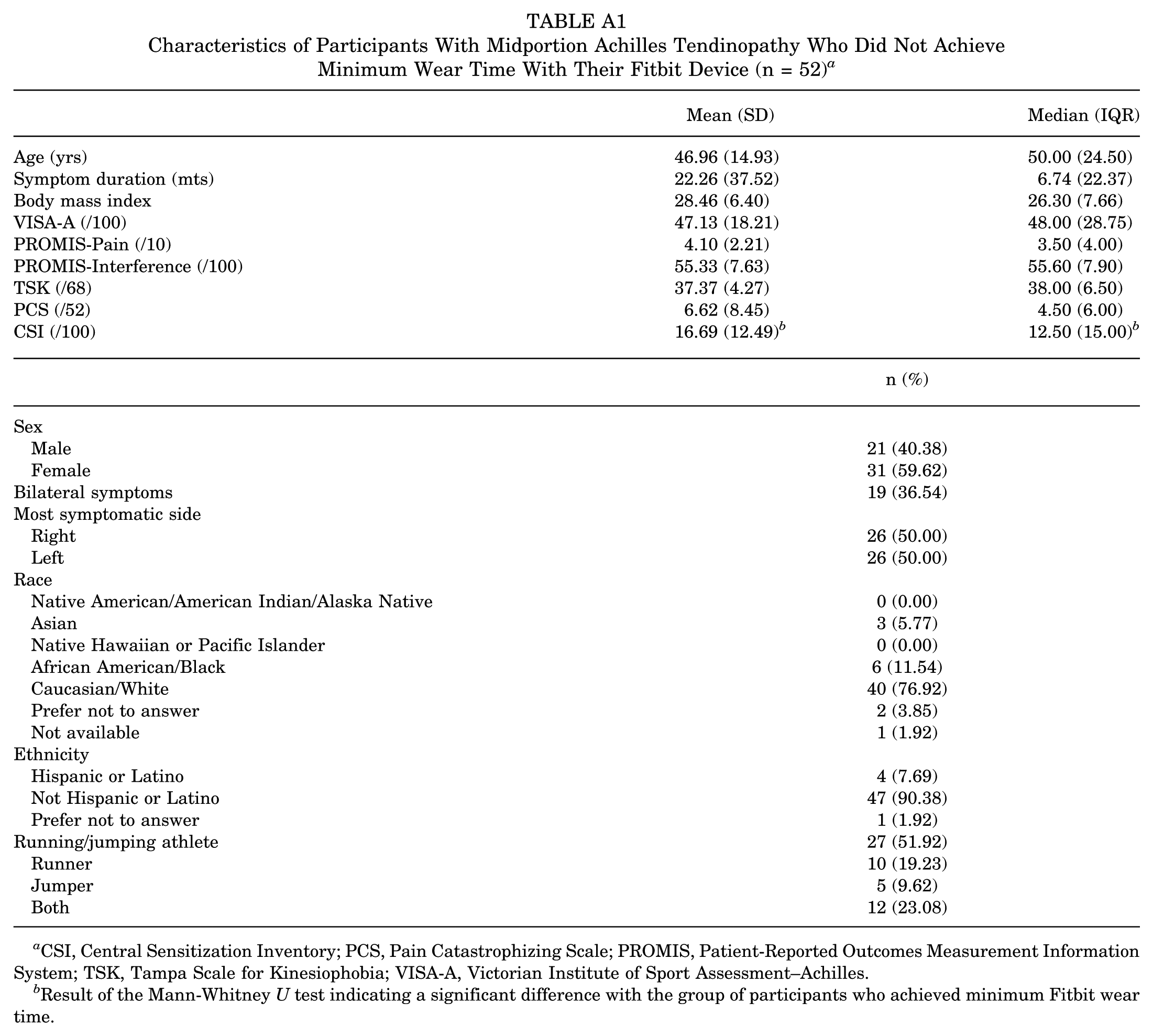
Of the 182 participants in the original longitudinal trial, 130 achieved the minimum wear time with their Fitbit device and were included in this secondary analysis (Figure 1). Demographics, injury characteristics, and initial measures of physical activity behavior, pain intensity, pain interference, kinesiophobia, pain catastrophizing, and symptoms of central sensitization of the 130 included participants are reported in Table 1. Notably, 88% of included participants wore the Fitbit device for 12 days or more, showing good participant adherence. Characteristics of the 52 excluded participants are detailed in Appendix Table A1. However, as they did not wear their Fitbit for a sufficient amount of time, no data were available regarding their physical activity measures. Only for the CSI scores was a small significant difference (P = .048) found between included participants and those excluded due to not achieving minimum wear time, with the latter reporting lower CSI scores.
Study flowchart.
Characteristics of Participants With Midportion Achilles Tendinopathy Achieving Minimum Wear Time With Their Fitbit Device (N = 130) a
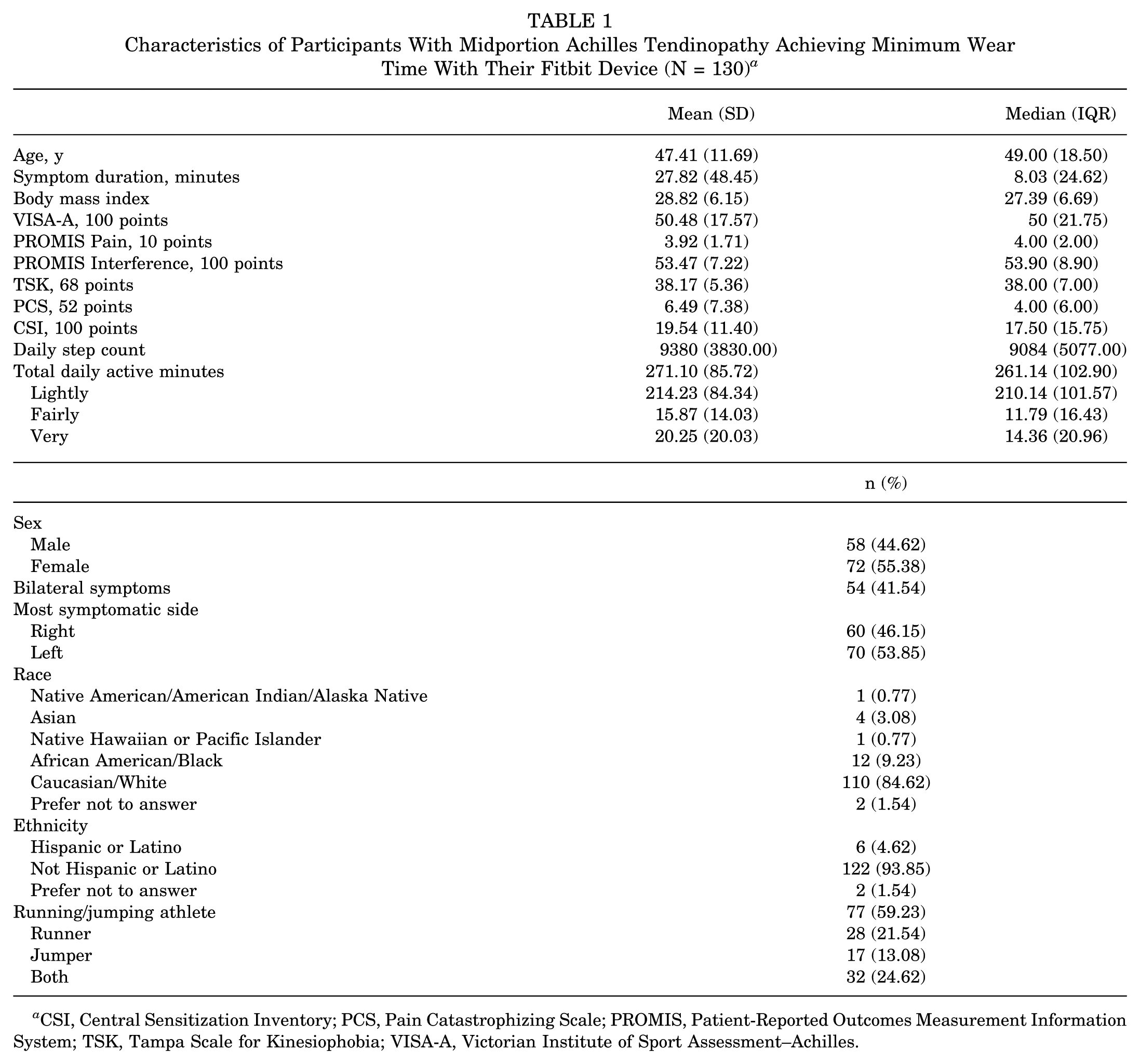
CSI, Central Sensitization Inventory; PCS, Pain Catastrophizing Scale; PROMIS, Patient-Reported Outcomes Measurement Information System; TSK, Tampa Scale for Kinesiophobia; VISA-A, Victorian Institute of Sport Assessment–Achilles.
Results of the linear regression models evaluating the relationship between daily step count and pain intensity, pain interference, kinesiophobia, pain catastrophizing, and symptoms of central sensitization are reported in Table 2. Only PROMIS Pain was shown to have a significant association with participants’ daily step count with an estimate of −591 (95% CI, −994 to −187). These findings indicate that for every additional point reported on the PROMIS Pain scale, participants took a mean 591 steps less on a daily basis.
Results of Linear Regression Models Evaluating the Relationships Between Daily Step Count With Pain Intensity, Pain Interference, Kinesiophobia, Pain Catastrophizing, and Symptoms of Central Sensitization (N = 130) a

All models are controlled for age and sex. CSI, Central Sensitization Inventory; PCS, Pain Catastrophizing Scale; PROMIS, Patient-Reported Outcomes Measurement Information System; TSK, Tampa Scale for Kinesiophobia. Values with asterisks indicate statistical significance at **P≤ .01 or ***P≤ .001.
Details on the regression models focused on the relationships between daily active minutes and pain intensity, pain interference, kinesiophobia, pain catastrophizing, and symptoms of central sensitization can be found in Table 3. The PROMIS Pain was significantly associated with participants’ very active minutes (regression coefficient, −3.76; 95% CI, −5.86 to −1.67]). Specifically, for every point participants reported higher on the PROMIS Pain scale, they spent 3.76 minutes less per day being very active. Analysis showed no other significant relationships between daily activity minutes and pain intensity, pain interference, kinesiophobia, pain catastrophizing, and symptoms of central sensitization.
Results of Linear Regression Models Evaluating the Relationships Between Daily Active Minutes With Pain Intensity, Pain Interference, Kinesiophobia, Pain Catastrophizing, and Symptoms of Central Sensitization (N = 130) a

All models are controlled for age and sex. CSI, Central Sensitization Inventory; PCS, Pain Catastrophizing Scale; PROMIS, Patient-Reported Outcomes Measurement Information System; TSK, Tampa Scale for Kinesiophobia. Values with asterisks indicate statistical significance at *P < .05; **P≤ .01; or ***P≤ .001.
Discussion
This secondary analysis explored the relationship between physical activity behavior and pain, kinesiophobia, pain catastrophizing, and self-reported symptoms of central sensitization in patients with midportion Achilles tendinopathy, with the hypothesis that daily steps and active minutes would be negatively associated with these factors. Our analysis showed that only patients’ self-reported pain intensity was negatively associated with their daily steps and minutes being very physically active. No significant associations between physical activity behavior and pain interference, kinesiophobia, pain catastrophizing, and symptoms of central sensitization were found.
Our findings show that patients with Achilles tendinopathy who experience more intense pain, also take significantly fewer steps on a daily basis than those who reported less intense pain. This is a significant finding, as to the best of our knowledge, this is the first study to directly investigate and report a negative relationship between daily step count and pain intensity in patients with midportion Achilles tendinopathy. Particularly, this negative association suggests that patients might cope with increased pain intensity by decreasing their daily load on their Achilles tendon via limiting their steps. More so, our findings suggest that patients primarily adjust their walking behavior rather than any other physical activities, as no significant association was found between pain intensity and total active minutes. However, when analyzing the various levels of intensity for daily active minutes, our analysis showed that fewer very active minutes were associated with higher pain intensity. These findings indicate that high pain intensity, due to Achilles tendinopathy, limits patients from being very physically active (ie, ≥6.0 METS). However, no significant relationship was found between pain intensity and lightly or fairly active minutes. As such, these findings partly agree with those from an exploratory study evaluating daily pain and physical activity patterns using wearable inertial measurement units in people with Achilles tendinopathy. 40 Specifically, the latter study's preliminary findings suggest that patients who are more physically active did not necessarily report more or less pain than those less active. Nevertheless, it should be noted that we collected patients’ mean pain intensity, while the authors of the exploratory study asked patients to rate their worst pain intensity. This discrepancy may explain our significant finding regarding very active minutes: rather than altering their activities because of intense pain flare-ups, patients might only do so whenever they experience higher pain intensity overall. Specifically, only the most strenuous activities were being limited from their daily lives. This might also explain the lack of significant association between physical activity behavior and pain interference, as those strenuous activities might not be part of their day-to-day activities, which were being questioned in the PROMIS Interference item. Nevertheless, our findings indicate that patients with increased pain intensity significantly limited their daily steps and very active minutes, suggesting a considerable impact on their daily physical activity behavior.
The results of this secondary analysis indicate that pain-related cognitions do not significantly influence daily step count or time spent engaging in physical activity, as measured by actigraphy, in patients with midportion Achilles tendinopathy. In light of the low mean PCS score observed in our sample (ie, 6.49/52), the lack of association between pain catastrophizing and physical activity behavior is unsurprising. Additionally, our findings on kinesiophobia are consistent with a previous study that reported no association between kinesiophobia and self-reported physical activity levels. 9 However, our results seemingly contrast those from a recent study investigating psychological factors in patients with Achilles or patellar tendinopathy. 37 That study identified significant associations between patients' sports participation and both pain catastrophizing and kinesiophobia, suggesting that maladaptive pain-related cognitions may limit engagement in sports activities. 37 This discrepancy in findings may be explained by differences in participant characteristics; while the previous study exclusively included (recreational) athletes, a substantial proportion of our participants (40.30%) did not refer to themselves as a runner (21.71%), jumper (13.18%), or both (24.81%). 37 Thus, 40% of our study sample may not regularly participate in sports activities that strenuously load the Achilles tendon. Despite this, our findings from a general sample of patients with midportion Achilles tendinopathy suggest that these patients can remain physically active regardless of maladaptive pain beliefs. Nevertheless, given the growing importance of the role of psychosocial factors in the management of Achilles tendinopathy, future research should consider employing qualitative methods to explore the most relevant psychological themes in this patient population and investigate their potential influence on patients’ daily physical activity behavior.11,20,41
Next, our analysis revealed that self-reported symptoms of central sensitization were not significantly associated with physical activity behavior in patients with midportion Achilles tendinopathy. Although the presence of central sensitization has been identified in a subset of patients with chronic Achilles tendinopathy in previous studies, the evidence remains conflicting and inconclusive.10,27,46 In our study, the mean CSI score was 19.54, which is well below the clinical cutoff commonly used to aid the classification of central sensitization–related pain (40/100). 24 As such, this finding further supports the notion that central sensitization may not be predominantly present in patients with midportion Achilles tendinopathy. In contrast, in other musculoskeletal pain populations, such as patients with low back pain, central sensitization has been established as a clinically relevant factor in specific subgroups, with significant negative associations reported between central sensitization and physical activity levels.25,48 The lack of a similar association in our study suggests that central sensitization is unlikely to be a driving factor for the impact of midportion Achilles tendinopathy on patients’ day-to-day (physical) activities. Nevertheless, given the considerable variability in the presence of central sensitization among patients with Achilles tendinopathy, further research is still warranted to continue exploring its role in specific subgroups.
Overall, the results of this secondary analysis mainly provide insight into the (lack of) relationship between physical activity, pain, and pain-related cognitions in patients with midportion Achilles tendinopathy. First, these findings suggest that patients' negative beliefs about pain do not necessarily hinder them from maintaining an active lifestyle. More so, they can carefully motivate health care providers to consider implementing active rehabilitation programs to encourage physical activity in patients, even if they exhibit kinesiophobia or pain catastrophizing. Furthermore, our findings can push health care providers to be more aware of (adjusted) physical activity behaviors in patients with midportion Achilles tendinopathy who report high levels of pain intensity. Specifically, incorporating a focus on daily steps in treatment programs may help these patients gradually increase their daily load, as they likely reduced their step count over the course of their condition. Similarly, since these patients may have decreased their participation in highly strenuous activities, physical therapists should ensure a safe and progressively structured reintroduction of such activities as part of their rehabilitation plan. 35 Future longitudinal and interventional studies are therefore needed to validate the clinical relevance of these observations and determine how the relationship between pain-related factors and activity behavior evolves throughout active rehabilitation programs.
Study Strengths
The first major strength of this secondary analysis is that it uses data from a longitudinal cohort including both athletic and nonathletic patients with midportion Achilles tendinopathy, thus providing a representative sample for the larger population with this condition. Second, physical activity behavior was assessed objectively using a wrist-worn actigraphy device, eliminating any recall bias patients might have using self-reported measures. Additionally, to our knowledge, this is the first study to use objective physical activity measures to examine their associations with pain, pain-related cognitions, and symptoms of central sensitization in patients with Achilles tendinopathy.
Limitations
Despite its strengths, this secondary analysis also has some limitations. First, we assessed patients’ pain intensity using a self-reported measure, which can be subject to recall bias. 5 More so, recall-based pain assessment captures only 1 dimension of pain in patients with Achilles tendinopathy. Given the complex nature of pain in these patients, this approach provides only a limited perspective of their pain. 33 Further research should explore the broader spectrum of pain (eg, movement-related pain, pain on palpation) and its relationship with patients’ physical activity behavior. Additionally, as the current analyses are based on cross-sectional data, no conclusions on the long-term impact of pain, pain-related cognitions, and self-reported symptoms of central sensitization can be made. Therefore, further longitudinal research is warranted to better understand the complex interplay between such psychological factors, central sensitization, and physical activity in patients with midportion Achilles tendinopathy. Third, we applied a minimal wear time criterion of ≥7 days with nonzero step count during the 2-week assessment period. Although this procedure is in line with previous studies, it inherently includes a risk of missing activity data. However, participant adherence in our sample was high as 88% of included participants wore the Fitbit device for 12 days or more, thus reducing the likelihood that missing data substantially influenced the activity estimates. Last, these findings are specific to the Fitbit Inspire and its proprietary, nontransparent algorithms, limiting generalizability to other wearable activity trackers. Future research should promote collaboration with manufacturers, adoption of open-source algorithms, and population-specific calibration to enhance the validity and reproducibility of wearable-derived physical activity measures.
Future Directions
Based on these findings, future research should explore how pain, pain-related cognitions, and symptoms of central sensitization relate to changes in daily activity behavior over time in patients with midportion Achilles tendinopathy, ideally through longitudinal and interventional designs. Given the multidimensional nature of pain, incorporating a broader range of pain outcomes (eg, movement-evoked pain) would allow for a more comprehensive examination of how different pain domains relate to patients’ daily activities. In addition, qualitative studies could help identify the psychosocial themes most relevant to patients’ day-to-day activity patterns and provide deeper insight into the lived experience of Achilles tendinopathy. Overall, while this study offers preliminary insight into these relationships, its findings provide several important directions for future research.
Conclusion
Pain intensity of patients with midportion Achilles tendinopathy is significantly associated with daily steps and time spent being very physically active, as determined via actigraphy. More specifically, this finding indicates that patients who experience higher levels of pain intensity also report lower levels of daily physical activity. In contrast, pain interference, pain-related cognitions, and self-reported symptoms of central sensitization are not significantly associated with physical activity behavior.
Footnotes
Appendix
Characteristics of Participants With Midportion Achilles Tendinopathy Who Did Not Achieve Minimum Wear Time With Their Fitbit Device (n = 52) a
| Mean (SD) | Median (IQR) | |
|---|---|---|
| Age (yrs) | 46.96 (14.93) | 50.00 (24.50) |
| Symptom duration (mts) | 22.26 (37.52) | 6.74 (22.37) |
| Body mass index | 28.46 (6.40) | 26.30 (7.66) |
| VISA-A (/100) | 47.13 (18.21) | 48.00 (28.75) |
| PROMIS-Pain (/10) | 4.10 (2.21) | 3.50 (4.00) |
| PROMIS-Interference (/100) | 55.33 (7.63) | 55.60 (7.90) |
| TSK (/68) | 37.37 (4.27) | 38.00 (6.50) |
| PCS (/52) | 6.62 (8.45) | 4.50 (6.00) |
| CSI (/100) | 16.69 (12.49) b | 12.50 (15.00) b |
| n (%) | ||
| Sex | ||
| Male | 21 (40.38) | |
| Female | 31 (59.62) | |
| Bilateral symptoms | 19 (36.54) | |
| Most symptomatic side | ||
| Right | 26 (50.00) | |
| Left | 26 (50.00) | |
| Race | ||
| Native American/American Indian/Alaska Native | 0 (0.00) | |
| Asian | 3 (5.77) | |
| Native Hawaiian or Pacific Islander | 0 (0.00) | |
| African American/Black | 6 (11.54) | |
| Caucasian/White | 40 (76.92) | |
| Prefer not to answer | 2 (3.85) | |
| Not available | 1 (1.92) | |
| Ethnicity | ||
| Hispanic or Latino | 4 (7.69) | |
| Not Hispanic or Latino | 47 (90.38) | |
| Prefer not to answer | 1 (1.92) | |
| Running/jumping athlete | 27 (51.92) | |
| Runner | 10 (19.23) | |
| Jumper | 5 (9.62) | |
| Both | 12 (23.08) | |
CSI, Central Sensitization Inventory; PCS, Pain Catastrophizing Scale; PROMIS, Patient-Reported Outcomes Measurement Information System; TSK, Tampa Scale for Kinesiophobia; VISA-A, Victorian Institute of Sport Assessment–Achilles.
Result of the Mann-Whitney U test indicating a significant difference with the group of participants who achieved minimum Fitbit wear time.
Final revision submitted February 5, 2026; accepted February 10, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: This article was funded in whole or in part by the NIH. It is subject to the NIH Public Access Policy. Through acceptance of this federal funding, NIH has been given a right to make this manuscript publicly available in PubMed Central upon the official date of publication, as defined by NIH. Research reported in this publication was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases and Eunice Kennedy Shriver National Institute of Child Health and Human Development of the NIH under award Nos. R01-AR072034 and T32HD007490. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the institutional review board at the University of Delaware #1090153.