
Abstract
Background:
Recurrent anterior shoulder instability rates are high after isolated arthroscopic Bankart repair (ABR), especially among patients with off-track Hill-Sachs lesions (HSLs) and significant glenoid bone loss. However, there are limited data on long-term recurrent anterior shoulder instability rates and patient-reported outcomes (PROs) following isolated ABR among patients with on-track HSLs and <20% glenoid bone loss.
Purpose:
To evaluate long-term clinical outcomes and PROs after isolated ABR for on-track HSLs with <20% glenoid bone loss, a population where isolated ABR remains indicated.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A retrospective review was conducted on patients undergoing isolated ABR for anterior shoulder instability between 2007 and 2018. Exclusion criteria included age <14 or >40 years, glenoid bone loss >20%, off-track HSL, concomitant remplissage, and revision procedures. All patients were contacted to obtain minimum 7-year clinical outcomes, including recurrent anterior shoulder instability and revision stabilization surgery, as well as PRO measures including Western Ontario Shoulder Index (WOSI), pain visual analog scale (pVAS), and Subjective Shoulder Value scores. Variables were compared between recurrent anterior shoulder instability and revision stabilization surgery groups. Significance was set to P < .05.
Results:
Long-term outcomes were obtained from 55 patients (mean age, 22 years; 32% of all eligible patients) at a mean follow-up of 10.4 years. Seventeen (31%) patients sustained ≥1 recurrent anterior shoulder instability event, and 8 (15%) patients underwent revision stabilization surgery. Younger age (P = .002) and collision athletics (P = .02) were associated with sustaining recurrent anterior shoulder instability, whereas distance to dislocation was not associated with recurrent anterior shoulder instability (P = .59). However, near-track HSLs (P = .02) and increased glenoid bone loss (P = .007) were associated with undergoing revision stabilization surgery. For every 1% increase in glenoid bone loss, there were 19% higher odds of undergoing revision stabilization surgery (P = .02). With regard to PROs, 67% of patients achieved the Patient Acceptable Symptom State (PASS) for WOSI and 55% of patients achieved the PASS for pVAS. Patients with recurrent anterior shoulder instability were less likely than those without recurrent instability to achieve the PASS for both WOSI (24% vs 87%; P < .001) and pVAS (29% vs 66%; P = .01).
Conclusion:
Rates of recurrent anterior shoulder instability were high following isolated ABR for on-track HSLs with <20% glenoid bone loss and were associated with inferior PROs at mean 10-year follow-up. Younger age and collision athletics were associated with sustaining recurrent anterior shoulder instability, while increased glenoid bone loss was an independent predictor of undergoing revision stabilization surgery. There remains a clinical need for improved stratification of on-track HSLs to identify patients who may benefit from additional procedures to improve recurrent anterior shoulder instability rates and subjective outcomes at long-term follow-up.
Keywords
Arthroscopic Bankart repair (ABR) is the cornerstone of surgical stabilization for anterior shoulder instability, with the addition of concomitant remplissage or Latarjet indicated in patients with off-track Hill-Sachs lesions (HSLs) or significant glenoid bone loss. 29 Early incorporation of the glenoid track concept, which identified on-track HSLs as low risk for engagement and off-track HSLs as high risk for engagement, simplified the surgical management of anterior shoulder instability; however, subsequent clinical studies demonstrated a persistently high recurrent anterior shoulder instability rate following isolated ABR for on-track HSLs.20,21,25 Such revelations led to the development of concepts such as distance to dislocation (DTD) to improve stratification of HSL engagement risk, surgical decision making, and clinical outcomes.2,14,15
Current literature evaluating long-term clinical outcomes following ABR for anterior shoulder instability is limited. Available evidence indicates rates of recurrent anterior shoulder instability up to 37%; however, it is limited by the inclusion of both on-track and off-track HSLs, significant glenoid bone loss, and heterogeneity in surgical techniques.1,5,12 In addition, studies reporting on long-term patient-reported outcomes (PROs) following ABR for anterior shoulder instability remain limited. 7
The purpose of this study was to evaluate the long-term clinical outcomes following isolated ABR for anterior shoulder instability with on-track HSLs and <20% glenoid bone loss, as well as risk factors for recurrent anterior shoulder instability. The secondary purpose of the study was to evaluate the relationship between recurrent anterior shoulder instability and long-term PROs. We hypothesized (1) that the long-term rate of recurrent anterior shoulder instability would exceed 25% following isolated ABR for on-track HSLs and <20% glenoid bone loss and that younger age and smaller DTD would be associated with recurrent anterior shoulder instability and (2) that recurrent anterior shoulder instability would be associated with inferior PROs at final follow-up.
Methods
Study Population
The present study was approved by the institutional review board at the University of Pittsburgh (No. STUDY20030061). All consecutive patients who underwent surgery for shoulder instability from 2007 to 2018 by 5 fellowship-trained academic sports medicine surgeons (B.P.L., M.R., J.D.H., A.L.) were retrospectively reviewed. First, all nonanterior stabilization procedures were excluded. Prior to database formation, all patients who underwent open surgery or who had a history of ipsilateral shoulder surgery, concomitant fracture fixation, concomitant rotator cuff repair, diagnosis of posterior or multidirectional shoulder instability, history of uncontrolled seizures or seizures within the past 2 years, and connective tissue disorders were excluded. Inclusion criteria for the present study included all patients undergoing primary isolated ABR for magnetic resonance imaging (MRI)–confirmed findings of anterior shoulder instability, including Bankart lesions and/or HSLs. All patients who met these inclusion criteria were then screened for additional exclusion criteria including age <14 years or >40 years, glenoid bone loss >20%, off-track HSLs, revision procedures, concomitant remplissage, and <7 years of follow-up.
Variables collected from patient charts included demographics (age, sex, laterality of instability), sport type (contact, collision, and/or overhead athlete), number of preoperative instability episodes, and instability type (glenohumeral dislocation vs subluxation). Among patients who met inclusion criteria, collision sport types included football, hockey, lacrosse, and wrestling, whereas contact sport types included all collision sports plus basketball and soccer. Sports that were considered neither contact nor collision sports included baseball, volleyball, track and field, skiing, and dance. Overhead sport types included football (position specific, such as quarterback), basketball, baseball/softball, volleyball, and tennis/squash. Glenohumeral dislocation was defined as requiring manual shoulder reduction, and glenohumeral subluxation was defined as an instability event that did not require manual shoulder reduction. MRI measurements collected included percentage glenoid bone loss and DTD as outlined below.
All ABR procedures were performed with the patient in the lateral decubitus or beach-chair position, based on surgeon preference, using standard arthroscopic suture anchor techniques with a minimum of 3 suture anchors. Patients underwent a standard postoperative physical therapy protocol including use of a sling for 4 to 6 weeks followed by gradual initiation of range of motion around 4 weeks. Return to sport was guided by criteria-based return-to-sport testing and/or surgeon discretion.
All patients included for analysis were contacted for completion of a questionnaire at minimum 7-year follow-up. Informed consent was obtained prior to questionnaire completion. Patients were assessed for recurrent anterior shoulder instability, defined as sustaining recurrent glenohumeral dislocation and/or subluxation after the index procedure, and revision stabilization surgery for recurrent anterior shoulder instability. Patients were additionally assessed for postoperative PRO measures, including Western Ontario Shoulder Index (WOSI), 13 pain visual analog scale (pVAS), 26 and Subjective Shoulder Value (SSV). 8 WOSI and pVAS scores were reported as both raw value and if the score achieved the Patient Acceptable Symptom State (PASS), which previous literature has identified as ≤480 and ≤1, respectively, following ABR. 16 As there is no reported PASS for SSV, SSV was reported as raw value only. All questionnaires were completed using an institutional electronic data capture database (REDCap; Vanderbilt University). Follow-up length was determined using date of questionnaire completion relative to date of ABR.
Revision stabilization surgery was indicated in patients who presented with recurrent anterior shoulder instability who were treated unsuccessfully with nonoperative management. Indications for revision surgery were determined on a patient-specific basis, based on number of recurrent anterior shoulder instability episodes, risk factors addressable by surgical correction (for example, glenoid bone loss), and patient-specific sport participation and desire to return to sport.
Measurement of Glenoid Bone Loss and DTD
Measurement of percentage glenoid bone loss was performed as previously outlined using T1-weighted MRI sequences. 3 Glenoid bone loss was measured on sagittal MRI using the best-fit circle method on the slice in which the maximal diameter of the glenoid face was visualized. The percentage of glenoid bone loss was calculated as the diameter of maximal anterior glenoid bone loss (d) divided by the diameter of the glenoid using the best-fit circle (D) times 100 and recorded as a percentage from 0 to 100. DTD was calculated as previously described as the glenoid track (0.83D – d) minus the Hill-Sachs interval (HSL width plus width of intact bone bridge between the rotator cuff attachment and the lateral margin of the HSL) and was recorded in millimeters. Based on prior literature, off-track HSLs were defined as DTD ≤0 mm and were excluded from the study, whereas near-track HSLs were defined as 0 mm < DTD ≤ 10 mm. 2 Imaging measurements were performed by 3 reviewers (S.D.) with extensive training in shoulder imaging analysis prior to analysis of our patient cohort. Intraclass correlation coefficients (ICCs) were determined to be good for both glenoid bone loss (ICC, 0.70) and DTD (ICC, 0.71).
Statistical Analysis
All data were analyzed using IBM SPSS Statistics (Version 29). Descriptive statistics are reported for all demographic variables, imaging measurements, PROs (including raw values and percentage of patients who achieved PASS), and clinical outcomes across the total cohort meeting inclusion criteria. Differences in demographic variables, imaging measurements, and postoperative PROs were compared between groups with and without recurrent anterior shoulder instability, as well as with and without revision stabilization surgery. Univariate analysis was performed using independent t test or Mann-Whitney U test for parametric and nonparametric data, respectively, and chi-square test for dichotomous variables. Multivariate logistic regression was then performed to evaluate factors independently associated with higher odds of sustaining recurrent anterior shoulder instability or undergoing revision stabilization surgery and included all variables with P < .10 on univariate analysis. Finally, subgroup analysis of patients with subcritical glenoid bone loss <13.5% was performed to identify rates of recurrent anterior shoulder instability, revision stabilization surgery, and postoperative PROs among this subgroup population. 22 Significance for all tests was set to P < .05.
Post hoc power analysis was conducted based on the observed means and standard deviations of WOSI and pVAS scores between patients who sustained recurrent anterior shoulder instability and patients who did not sustain recurrent anterior shoulder instability. With an alpha level of .05, analysis yielded a power of 97% and 89%, respectively, to detect the observed between-group differences.
Results
Total Cohort
A total 55 patients (mean ± SD age, 22 ± 8 years); female, n = 20 [36%]) met all inclusion criteria (32% of all eligible patients) (Figure 1). The total cohort included 35 (64%) contact athletes, of which 26 (47%) patients were collision athletes, and 20 (36%) overhead athletes. A total of 33 (60%) patients sustained multiple preoperative anterior shoulder instability episodes, and 28 (51%) patients sustained ≥1 glenohumeral dislocation event. Mean percentage glenoid bone loss and DTD were 3.5% and 15.4 mm, respectively, and 11 (20%) patients had near-track HSLs (Table 1).
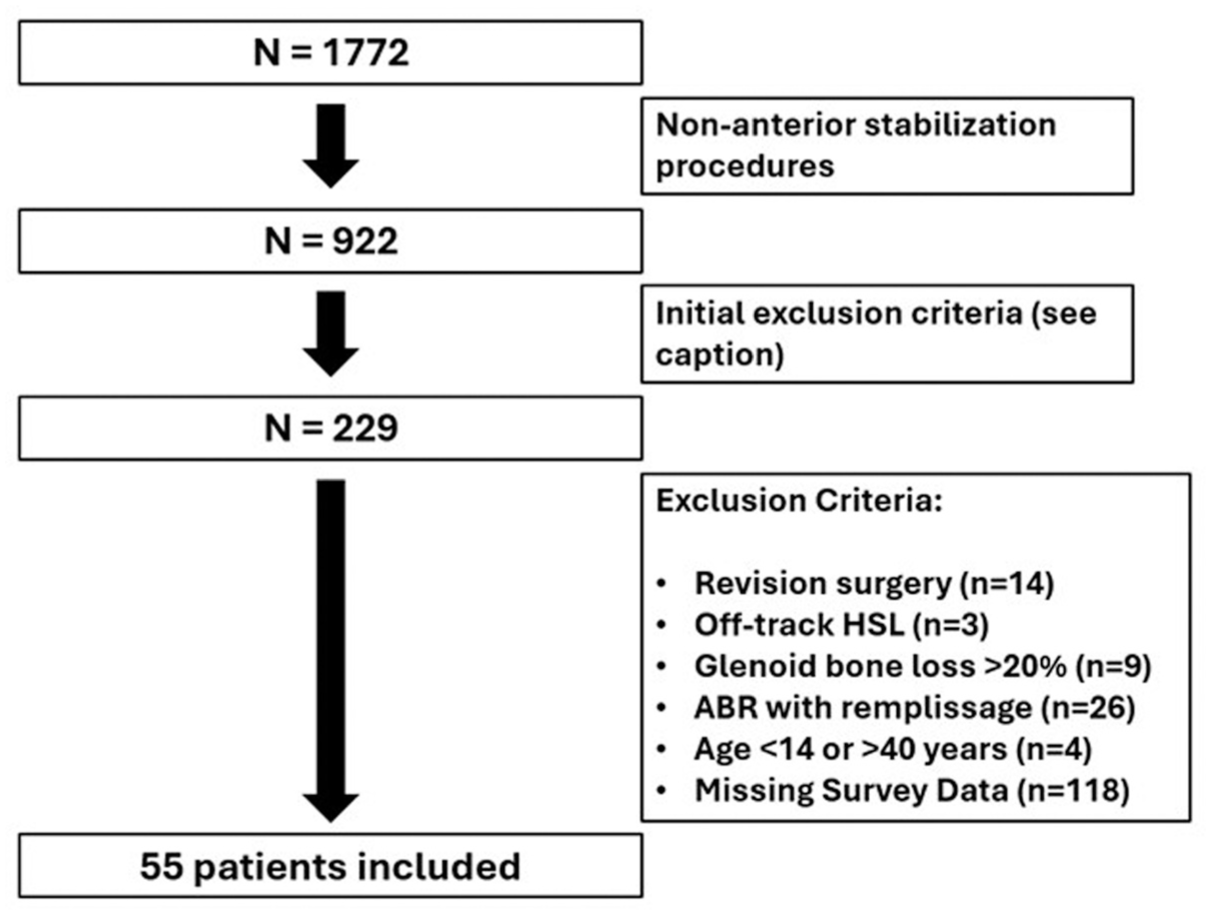
Flowchart of inclusion and exclusion criteria. All patients who underwent surgical stabilization of shoulder instability were retrospectively reviewed. First, all non-anterior shoulder stabilization procedures were excluded. Exclusion criteria then included all patients who underwent open surgery, had history of ipsilateral shoulder surgery, concomitant fracture fixation, concomitant rotator cuff repair, diagnosis of posterior or multidirectional shoulder instability, history of uncontrolled seizures or seizures within the last 2 years, and connective tissue disorders. After identifying all patients who underwent primary isolated ABR, additional exclusion criteria for the present study were applied and included revision surgery, off-track HSL, glenoid bone loss > 20%, concomitant remplissage, age < 14 years or > 40 years, and less than 7 years of follow-up. ABR, arthroscopic Bankart repair; HSL, Hill-Sachs lesion.
Demographic and Surgical Characteristics for Patients Undergoing Isolated Arthroscopic Bankart Repair for On-Track Hill Sachs Lesions a
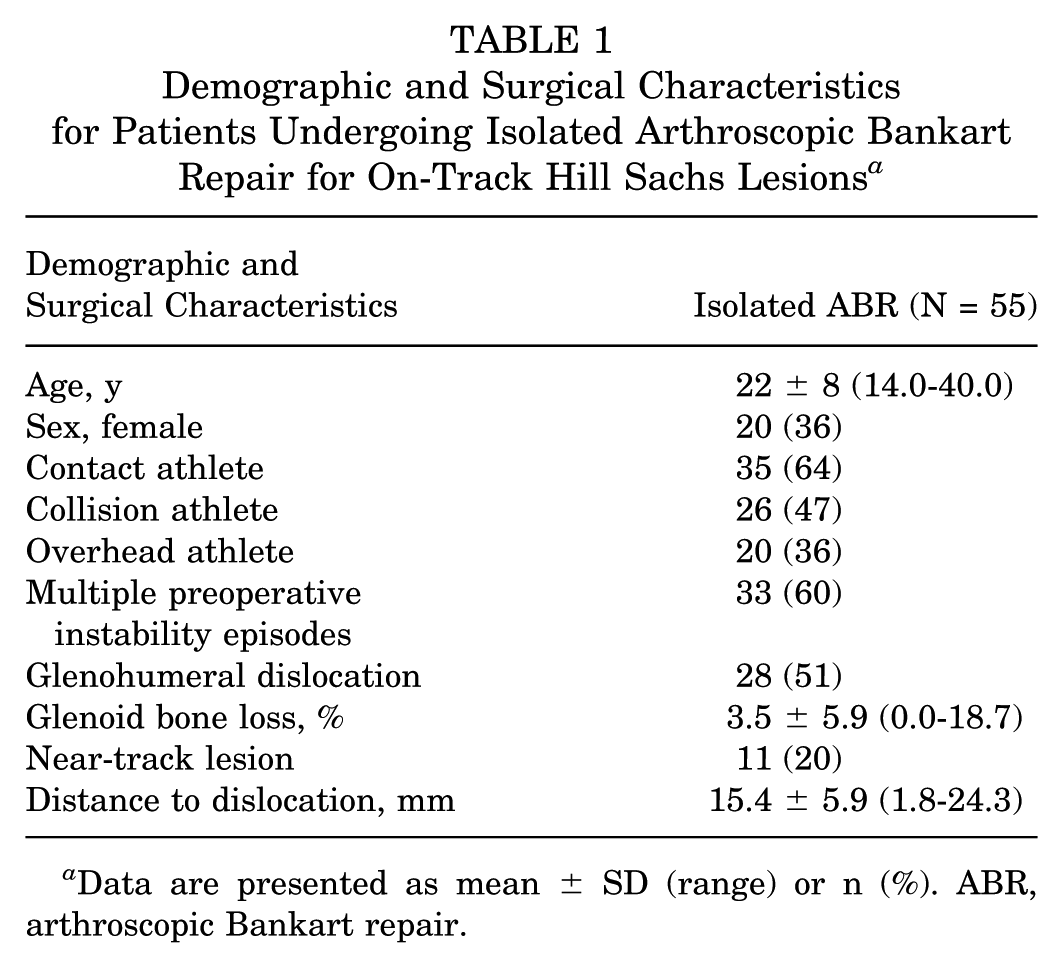
Data are presented as mean ± SD (range) or n (%). ABR, arthroscopic Bankart repair.
All patients who underwent surgical stabilization of shoulder instability were retrospectively reviewed. First, all nonanterior shoulder stabilization procedures were excluded. Exclusion criteria then included all patients who underwent open surgery or those with a history of ipsilateral shoulder surgery, concomitant fracture fixation, concomitant rotator cuff repair, diagnosis of posterior or multidirectional shoulder instability, history of uncontrolled seizures or seizures within the past 2 years, and connective tissue disorders. After identifying all patients who underwent primary isolated ABR, additional exclusion criteria for the present study were applied and included revision surgery, off-track HSL, glenoid bone loss >20%, concomitant remplissage, age <14 years or >40 years, and <7 years of follow-up.
The mean follow-up length for the total cohort was 10.4 ± 2.6 years (Table 2). A total of 17 (31%) patients sustained recurrent anterior shoulder instability after isolated ABR, of which 8 (15%) patients underwent revision surgery. The mean time to recurrent anterior shoulder instability was 2.6 ± 2.5 years (range, 0.7-8.2 years). The mean WOSI, pVAS, and SSV scores at final follow-up were 395.1, 2.1, and 79, respectively. A total of 37 (67%) patients achieved PASS for WOSI, and 30 (55%) patients achieved PASS for pVAS (Table 2).
Clinical and Patient-Reported Outcomes for Patients Undergoing Isolated Arthroscopic Bankart Repair for On-Track Hill Sachs Lesions a

Data are presented as mean ± SD or n (%). ABR, arthroscopic Bankart repair; PASS, Patient Acceptable Symptom State; postop, postoperative; pVAS, pain visual analog scale; SSV, Subjective Shoulder Value; WOSI, Western Ontario Shoulder Index.
Recurrent Anterior Shoulder Instability
Patients who sustained recurrent anterior shoulder instability were more likely to be younger (18 vs 24 years old; P = .002) and collision athletes compared with noncollision athletes (71% vs 37%; P = .02). There were no significant differences between patients who sustained recurrent anterior shoulder instability versus no recurrent anterior shoulder instability with regard to glenoid bone loss (5.8% vs 2.5%; P = .06), frequency of near-track HSLs (29% vs 16%; P = .24), or DTD (14.7 vs 15.7 mm; P = .59) (Table 3). Multivariate regression analysis identified younger age as a significant predictor of recurrent anterior shoulder instability (odds ratio [OR], 0.81; 95% CI, 0.66-0.99; P = .046) (Appendix Table A1). For each additional year of age starting at age 14 years, the odds of recurrent anterior shoulder instability decreased by 19%.
Comparison of Demographics and Surgical Characteristics Between Patients With and Without Recurrent Anterior Shoulder Instability a
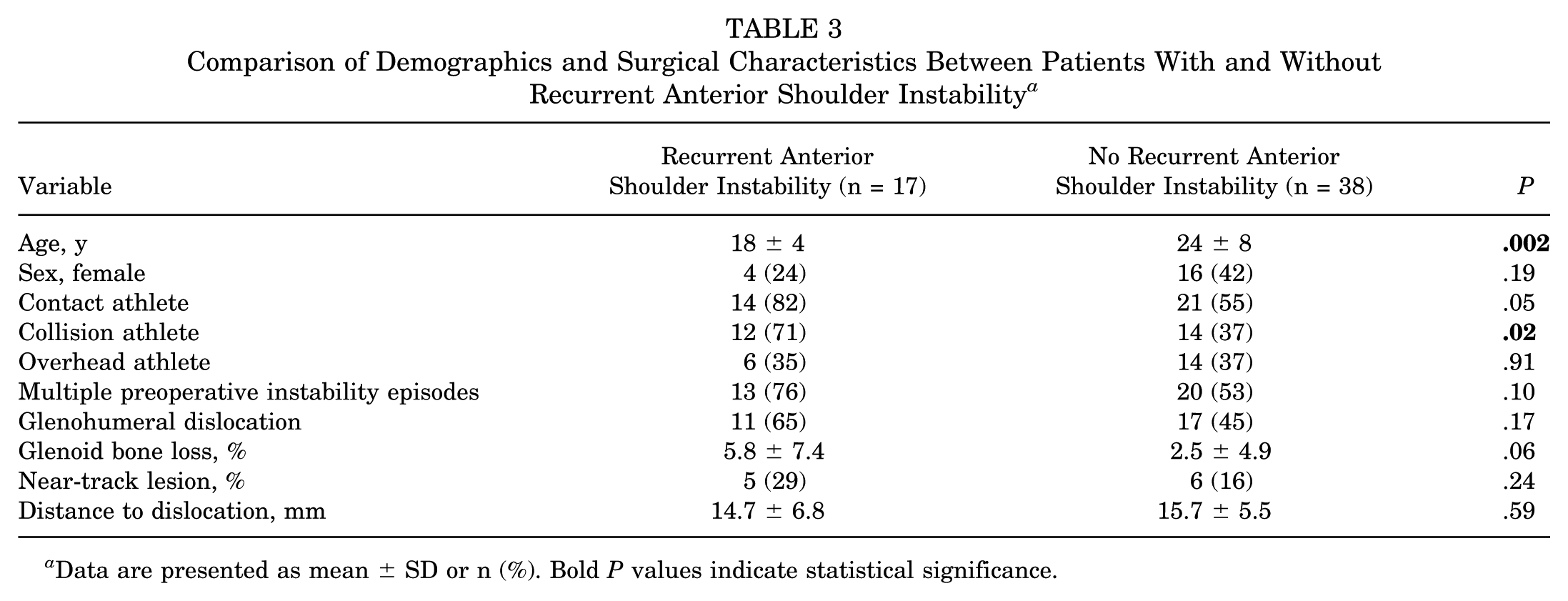
Data are presented as mean ± SD or n (%). Bold P values indicate statistical significance.
Mean WOSI (752.8 vs 235.1; P < .001) and pVAS (4.2 vs 1.2; P < .001) scores were significantly higher (worse) in patients who sustained recurrent anterior shoulder instability compared with patients who did not sustain recurrent anterior shoulder instability, and SSV (64 vs 86; P < .001) was significantly lower (worse) in patients who sustained recurrent anterior shoulder instability compared to patients who did not sustain recurrent anterior shoulder instability. Additionally, the percentage of patients who achieved PASS for WOSI (24% vs 87%; P < .001) and pVAS (29% vs 66%; P = .01) was significantly lower in patients who sustained recurrent anterior shoulder instability compared with patients who did not sustain recurrent anterior shoulder instability (Table 4).
Comparison of Patient-Reported Outcomes Between Patients With and Without Recurrent Anterior Shoulder Instability a

Data are presented as mean ± SD or n (%). Bold P values indicate statistical significance. PASS, Patient Acceptable Symptom State; postop, postoperative; pVAS, pain visual analog scale; SSV, Subjective Shoulder Value; WOSI, Western Ontario Shoulder Index.
Revision Stabilization Surgery
Patients who underwent revision stabilization surgery for recurrent anterior shoulder instability were more likely to have increased glenoid bone loss (10.2% vs 2.3%; P = .007) and higher frequency of near-track HSLs (50% vs 15%; P = .02). No other preoperative variables were found to be significantly different between patients who underwent revision stabilization surgery compared with patients who did not undergo revision stabilization surgery (Table 5). Multivariate regression analysis identified increased glenoid bone loss as a significant predictor of undergoing revision stabilization surgery (OR, 1.19; 95% CI, 1.03-1.38; P = .02) (Appendix Table A2). For each 1% increase in glenoid bone loss preoperatively, the odds of revision stabilization surgery increased by 19%.
Comparison of Demographics and Surgical Characteristics Between Patients With and Without Revision Surgery a

Data are presented as mean ± SD or n (%). Bold P values indicate statistical significance. HSL, Hill Sachs lesion.
Mean WOSI (712.9 vs 341.0; P = .01) and pVAS (4.3 vs 1.8; P = .015) scores were significantly higher in patients who underwent revision stabilization surgery compared with patients who did not undergo revision stabilization surgery, whereas SSV (66 vs 81; P = .024) was significantly lower in patients who underwent revision stabilization surgery compared with patients who did not undergo revision stabilization surgery. Additionally, the percentage of patients who achieved PASS for WOSI (25% vs 74%; P = .006) was significantly lower in patients who underwent revision stabilization surgery compared with patients who did not undergo revision stabilization surgery (Table 6).
Comparison of Patient-Reported Outcomes Between Patients With and Without Revision Surgery a

Data are presented as mean ± SD or n (%). Bold P values indicate statistical significance. PASS, Patient Acceptable Symptom State; postop, postoperative; pVAS, pain visual analog scale; SSV, Subjective Shoulder Value; WOSI, Western Ontario Shoulder Index.
Subgroup Analysis of Subcritical Glenoid Bone Loss
Among the 55 included patients in the present study, 48 (87%) patients had subcritical glenoid bone loss <13.5%. Among the 48 patients with subcritical glenoid bone loss, 13 (27%) patients sustained recurrent anterior shoulder instability and 5 (10%) patients underwent revision stabilization surgery. The mean WOSI, SSV, and pVAS for this subgroup was 371.8 ± 367.8, 80 ± 18, and 2.0 ± 2.4, respectively. Additionally, the percentage of patients who achieved PASS for WOSI (23% vs 86%; P < .001) and pVAS (23% vs 66%; P = .008) was significantly lower in patients who sustained recurrent anterior shoulder instability compared with patients who did not sustain recurrent anterior shoulder instability. Finally, among this subgroup population, glenoid bone loss was not found to statistically differ between patients who sustained recurrent anterior shoulder instability compared with patients who did not sustain recurrent anterior shoulder instability (2.5% vs 1.3%; P = .64).
Discussion
The most important finding of the present study was the 31% rate of recurrent anterior shoulder instability after isolated ABR for on-track HSLs with glenoid bone loss <20% at mean follow-up of 10.4 years. An important secondary finding of the study was the inferior PROs associated with sustaining recurrent anterior shoulder instability and undergoing revision stabilization surgery at long-term follow-up. The results of this study highlight the necessity for improved stratification of high-risk on-track HSLs to prevent long-term recurrent anterior shoulder instability, revision stabilization surgery, and inferior subjective outcomes.
Several prior studies have reported on long-term clinical outcomes after isolated ABR, with reported rates of recurrent anterior shoulder instability up to 37%.1,5,12,17 However, these studies often include patients with off-track HSLs, significant glenoid bone loss >20%, or heterogeneity in surgical techniques.1,12,17,27 Therefore, the findings of these studies may not pertain to the current landscape of anterior shoulder instability surgery, as off-track HSLs are often considered an indication for concomitant remplissage,9,18,19 whereas glenoid bone loss >20% is often an indication for concomitant Latarjet.6,10,11 Literature evaluating long-term clinical outcomes after isolated ABR for on-track HSLs and glenoid bone loss <20%, a population where isolated ABR without remplissage is often indicated, remains sparse. Available literature evaluating long-term outcomes of isolated ABR in this population suggests recurrent anterior shoulder instability rates of 20% to 30%, which aligns with the recurrent anterior shoulder instability rate reported in the present study.7,28 In addition, irrespective of inclusion criteria, several studies have reported on inferior PROs at long-term follow-up among patients who sustain recurrent anterior shoulder instability, compared with patients who do not sustain recurrent anterior shoulder instability.4,7,12 This aligns with the findings of the present study, which identified a nearly 3 times lower rate of achieving PASS for WOSI and pVAS in patients who sustained recurrent anterior shoulder instability or underwent revision stabilization surgery.
An important finding of the present study was that increased glenoid bone loss was associated with higher risk of undergoing revision stabilization surgery at long-term follow-up after isolated ABR for on-track HSLs with glenoid bone loss <20%. Specifically, there was a 19% higher risk of undergoing revision stabilization surgery identified with every 1% increase in glenoid bone loss. Historically, glenoid bone loss 20% to 25% has been considered the threshold for “critical” bone loss, and therefore has served as a surgical threshold for augmenting the glenoid with procedures such as Latarjet.10,11 However, recent literature has challenged this 20% glenoid bone loss threshold, suggesting increased rates of recurrent anterior shoulder instability with glenoid bone loss as low as 13.5%.22-24 The findings of our study appear to support these lower thresholds for critical glenoid bone loss, as increased glenoid bone loss remained an independent predictor of need for revision stabilization surgery after isolated ABR in patients with glenoid bone loss within the current threshold of <20%. However, among the 48 patients in the present study with glenoid bone loss <13.5%, 13 patients sustained recurrent anterior shoulder instability (27% recurrence rate), indicating that long-term rates of recurrent anterior shoulder instability remain high even in the setting of subcritical glenoid bone loss.
The present study also identified a higher incidence of near-track HSLs, defined as DTD ≤10 mm, among patients who underwent revision stabilization surgery. Measurement of DTD has gained significant traction in recent years as a risk factor for recurrent anterior shoulder instability after isolated ABR in short-term outcome studies, with the addition of remplissage reducing recurrent anterior shoulder instability rates in patients with near-track HSLs.2,14,15,30 In the present study, of the 11 patients with near-track HSLs included in the analysis, 5 patients sustained recurrent anterior shoulder instability and 4 patients underwent revision stabilization surgery at minimum 7-year follow-up. Therefore, our findings support this literature suggesting isolated ABR may be insufficient treatment for near-track HSLs due to increased long-term rates of revision stabilization surgery. While mean DTD was not found to differ between patients who underwent revision stabilization surgery versus not, the higher incidence of near-track HSLs in the revision stabilization surgery cohort highlights the importance of consideration of DTD in preoperative planning to prevent inferior long-term clinical outcomes and PROs after ABR.
Limitations
There are several limitations to the present study. First, among patients who met inclusion criteria, the follow-up rate at minimum 7 years postoperatively was 32%, which places the findings at risk of selection bias. Second, given the retrospective nature of the study, we were unable to compare postoperative PROs with preoperative values to identify true change in PROs following isolated ABR and therefore were only able to identify differences in postoperative values. Nonetheless, a significant deterioration in PROs at long-term follow-up was found among patients who sustained recurrent anterior shoulder instability or underwent revision stabilization surgery, which is clinically important with respect to understanding how subjective outcomes may be influenced by recurrent anterior shoulder instability or revision stabilization surgery. Third, the inclusion of 5 surgeons over 11 years introduces inherent variability in surgical technique and postoperative protocols. However, all included patients underwent isolated ABR with a minimum of 3 anchors, in line with current surgical techniques. Finally, data regarding return to sport or play, as well as activity level after surgery, were out of scope of the study.
Conclusion
Rates of recurrent anterior shoulder instability were high following isolated ABR for on-track HSLs with <20% glenoid bone loss and were associated with inferior PROs at mean 10-year follow-up. Younger age and collision athletics were associated with sustaining recurrent anterior shoulder instability, while increased glenoid bone loss was an independent predictor of undergoing revision stabilization surgery. There remains a clinical need for improved stratification of on-track HSLs to identify patients who may benefit from additional procedures to improve recurrent anterior shoulder instability rates and subjective outcomes at long-term follow-up.
Footnotes
Appendix
Binary Logistic Regression for Revision Surgery After Isolated Arthroscopic Bankart Repair for On-Track Hill-Sachs Lesions a

| Binary Logistic Regression for Revision Surgery | ||
|---|---|---|
| Variable | Odds Ratio (95% CI) | P |
| Glenoid bone loss, % | 1.19 (1.03-1.38) |
|
Bold P value indicates statistical significance. Nagelkerke R2 = 0.297.
Final revision submitted January 26, 2026; accepted February 2, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.P.L. reports education payments from Mid-Atlantic Surgical Systems. J.D.H. is a member of the editorial board of Knee Surgery, Sports Traumatology, and Arthroscopy and Annals of Joint and is a consultant for Smith & Nephew. A.L. reports consulting fees from Arthrex, Tornier, and Stryker. A.J.P. is a member of the editorial board of BMC Musculoskeletal Disorders. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this retrospective study was obtained from the University of Pittsburgh institutional review board (No. STUDY20030061).