
Abstract
Background:
Depression is prevalent among patients undergoing arthroscopic shoulder procedures and is associated with worse patient-reported outcomes after shoulder stabilization surgery. However, recurrent shoulder instability after stabilization among patients with depression has yet to be investigated.
Hypothesis:
Patients with depression experience higher rates of recurrent shoulder instability and inferior functional outcomes compared with patients without depression.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This single-institution retrospective study (2009-2023) identified 531 patients undergoing primary shoulder stabilization surgery for recurrent shoulder instability. Patients were stratified into 2 cohorts based on depression status. Primary procedures included arthroscopic or open Bankart repair, remplissage, open Latarjet, and open distal tibial allograft. Data from electronic medical records included demographics and clinical outcomes.
Results:
Of 531 patients, 110 (21%) had a preoperative diagnosis of depression. Compared to patients without a diagnosis of depression, depression patients were older (29.9 vs 24.2 years; P < .001), had higher body mass index (28.5 vs 26.6; P = .005), and greater comorbidities (American Society of Anesthesiologists and Charlson Comorbidity Index scores, smoking rates, and rates of comorbid mental health disorders) (all P < .001). The depression cohort had lower range of motion (ROM) in all measures before surgery, and ROM in external rotation remained lower postoperatively (P < .001). Patients with depression had worse postoperative Single Assessment Numeric Evaluation (82 vs 88; P > .04) and American Shoulder and Elbow Surgeons (79 vs 89; P = .02) scores. Lifetime recurrent instability rates were higher in the depression group compared with the nondepression group (23% vs 14%; P = .03), and instability-free survival at 2, 5, and 10 years was lower in patients with depression (P = .02).
Conclusion:
Patients with depression have increased rates of recurrent instability and lower patient-reported outcome scores after shoulder stabilization surgery. Shoulder stabilization surgery is an effective treatment option for patients with depression, but depression evaluation should be considered in the preoperative assessment to aid in patient and physician education on the risks of inferior clinical outcomes.
Mental health disorders, including anxiety and depressive disorders, exhibit a yearly prevalence of approximately 18% and 10%, respectively, among adults. 12 The incidence of mental health disorders in orthopaedics has significantly increased following the COVID-19 pandemic and the enhanced recognition of the biopsychosocial model in managing musculoskeletal injuries.2,9,22 During the height of the pandemic, the age-standardized prevalence of depression was 18.5%, with a notable rise to 21.5% for adults aged 18 to 24. 14 Patients with shoulder instability may exhibit a higher rate of depression, with prevalence rates reported up to 50% in previous studies. 24 The increased prevalence of depression may be related to the pain and disability that accompany shoulder instability, both of which have been linked to worsening of depressive symptoms.3,20
Shoulder stabilization surgery is an effective treatment for patients with shoulder instability. In patients with a history of depression, depressive symptoms show improvement after surgery. 24 Despite the improvements in depressive symptoms, these patients can face inferior functional outcomes, prolonged opioid use, and limited return to sports postoperatively.8,13,24 These challenges may be further exacerbated by the reported heightened pain perception that has been associated with depression.23,25
While depression has been linked with higher rates of surgical failure and revision in shoulder arthroplasty and rotator cuff repair (RCR), the relationship between depression and postoperative instability recurrence remains unquantified after shoulder stabilization surgery.7,15,16 Our current study aims to investigate postoperative functional outcomes and rates of recurrent shoulder instability in patients with depression undergoing shoulder stabilization surgery, compared with those without depression. We hypothesize that patients with depression will exhibit inferior functional outcomes and higher rates of recurrent shoulder instability compared with those without depression after shoulder stabilization surgery.
Methods
Patient Population
Patients undergoing shoulder stabilization surgery for recurrent shoulder instability from July 2009 to November 2023 were identified via a databank query of relevant International Classification of Diseases 9th and 10th Revision (ICD-9, ICD-10) codes 718.31 and M25.31 (indicating pathologic and recurrent dislocation of the shoulder) and Current Procedural Terminology (CPT) codes 23455 (open capsulorrhaphy with labral repair, such as Bankart procedure), 29806 (arthroscopic capsulorrhaphy with labral repair, such as Bankart procedure), 23462 (Latarjet procedure), and 29807 (superior labrum anterior and posterior [SLAP] repair). CPT code 29807 was included to capture labral repairs performed for instability, particularly when concurrent SLAP lesions were addressed. Operative reports were reviewed to confirm instability as the indication, and isolated SLAP repairs without instability were excluded. Initial retrospective chart review of all potential patients was performed independently by 2 authors (B.J.B. and C.P.T.), and patients with <6 months of postoperative follow-up and those undergoing revision procedures were excluded from further review.
Operative Technique
Shoulder stabilization procedures were performed by 7 fellowship-trained orthopaedic shoulder surgeons (including G.L.J., R.C.R., J.Y.B., and G.L.C.) at The Ohio State University Wexner Medical Center. The primary procedures included arthroscopic or open Bankart repair (with or without capsulorrhaphy), remplissage, open Latarjet, and open distal tibial allograft. For open procedures, access to the shoulder was gained using the standard deltopectoral approach. The subscapularis muscle was managed via a variety of techniques, including tenotomy, lesser tuberosity osteotomy, peel, or split, and was appropriately repaired before case conclusion. Postoperatively, patients began a structured rehabilitation protocol tailored to their specific procedure. Physical therapy regimens were assigned based on the patient's progression at first follow-up, typically beginning 4 weeks postoperatively. All patients followed a standardized rehabilitation protocol specific to their procedure.
Data Collection
Retrospective review yielded 2 distinct cohorts: patients with a diagnosis of depression before shoulder stabilization surgery (depression cohort) and patients without depression (control cohort). The diagnosis of depression was based on clinical documentation in the medical records, with patients identified as having a diagnosis of major depressive disorder at any time before surgery. This diagnosis was established by the treating clinicians, including psychiatrists, psychologists, and other health care providers, using established diagnostic criteria such as the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Diagnosis was confirmed with antidepressive medication status in the year before surgery. Provider notes from preoperative visits were examined for information related to shoulder instability. Collected data included demographic characteristics, history of previous shoulder dislocations, details of instability symptoms (eg, traumatic vs atraumatic, duration, and direction), and preoperative shoulder function (eg, strength and range of motion [ROM]). Both ROM and strength scores were measured by approximation by each surgeon in clinic, and ROM in external rotation (ER) was measured at 0° of abduction. Operative reports and preoperative anesthesia assessments were also reviewed. Data collected from the operative report included procedures performed, approach (open vs arthroscopic), indications, rotator cuff status, glenoid bone loss, Hill-Sachs lesions, and any bone grafts used. Imaging reports supplemented operative reports for rotator cuff status, glenoid bone loss, and Hill-Sachs lesions if not mentioned. Preoperative anesthesia reports provided American Society of Anesthesiologists (ASA) scores, Charlson Comorbidity Index (CCI) scores, and smoking status. Postoperative data were collected from follow-up progress notes and included postoperative shoulder function (eg, strength and ROM), complications, and any revision surgeries. Follow-up time was based on review of all postoperative progress notes, with the most recent progress notes including strength and ROM findings serving as the final follow-up date. Recurrent shoulder instability was defined as any documented subluxation or recurrent dislocation of the shoulder joint by surgeons or the need for revision surgery due to instability. For patients requiring revision surgery, the relevant operative reports were reviewed to determine indications and procedures performed. Patient-reported outcomes (PROs) (Single Assessment Numeric Evaluation [SANE] score, visual analog scale [VAS] for pain, and American Shoulder and Elbow Surgeons [ASES] score) were collected via phone interview from June 2024 to August 2024. The short, 5-item Shoulder Instability–Return to Sport After Injury (short SIRSI) was used to evaluate psychological readiness to return to sport for patients involved in sports or exercise at the time of shoulder stabilization. 20 Further, we asked patients to select their satisfaction with the outcome of their shoulder stabilization based on 4 response options (“very dissatisfied,”“dissatisfied,”“satisfied,” and “very satisfied”).
Statistical Analysis
This study utilized multiple statistical methods for data analysis. Kaplan-Meier survival curves were used to estimate survival probabilities, with a 95% CI to assess failure rates. Failure was defined as any documented subluxation or recurrent dislocation of the shoulder joint by surgeons or the need for revision surgery due to instability. Differences in survival distributions were evaluated using the log-rank test. Continuous variables were assessed for normality using the Shapiro-Wilk test. Normally distributed continuous variables were analyzed using Student t test or analysis of variance, while nonnormally distributed variables were analyzed using the Wilcoxon rank-sum test as appropriate. Ordinal variables were compared using ordinal logistic regression or the Wilcoxon signed-rank test. A significance threshold of P < .05 was applied for all 2-sided tests. Continuous variables were reported as mean ± SD, categorical variables were reported as frequencies (percentage), and ordinal variables were described by their median values. All statistical analyses were conducted using Stata/SE Version 17.0 (StataCorp).
Results
Demographics
Initial databank query identified 1397 patients who underwent shoulder stabilization surgery. Of these, 531 patients met inclusion criteria, and 110 (21%) had a preoperative diagnosis of depression. Patients with depression were on average older at 29.9 ± 10.2 years (vs 24.2 ± 8.8 years; P < .001). Follow-up in our depression cohort varied at 3.3 ± 3.5 years (range, 0.5-15.2 years). Patients with depression had inferior physical health status before surgery as indicated by significantly higher ASA physical classification scores (1.9 vs 1.4; P < .001) and CCI scores (0.3 vs 0.1; P < .001). Depression was also associated with a variety of comorbidities, including higher smoking rates (24% vs 11%; P < .001), higher BMI (28.5 ± 6.3 kg/m2 vs 26.6 ± 5.3 kg/m2; P = .005), and higher rates of comorbid mental health disorders such as anxiety and substance use disorders (71% vs 13%; P < .001) (Table 1).
Comparative Demographics a

Data are presented as n (%) or mean ± SD, unless otherwise indicated. ASA, American Society of Anesthesiologists; BMI, body mass index; CCI, Charlson Comorbidity Index; MHD, mental health disorders.
The groups differed significantly regarding the chronicity of shoulder instability, as patients with depression had a higher preoperative rate of atraumatic shoulder instability (30% vs 18%; P = .02), and these patients tended to have a longer duration of instability symptoms before operative treatment (5.64 years vs 3.77 years; P = .003). In both groups, patients most commonly had shoulder dislocation rather than subluxation, with a similar proportion experiencing dislocation-related instability (depression, 80%; no depression, 75%; P = .25). The direction of instability was anterior for most patients in both groups, and the difference in direction between the 2 groups did not reach statistical significance (P = .17). The percentage of patients with Hill-Sachs lesions was similar between the cohorts (depression, 65%; no depression, 60%; P = .13). However, there was a significantly higher percentage of patients with depression who had glenoid bone loss (45% vs 33%; P = .02). Among those with glenoid bone loss, the amount of bone loss was similar between the 2 groups (depression, 16.39%; no depression, 16.76%; P = .65). The percentage of patients with bipolar bone loss was similar between those with and without depression, as 38 patients (35%) in the depression cohort had bipolar bone lesions, compared with 116 patients (28%) without depression (P = .16) (Table 2).
Nature of Instability and Bone Loss a

Data are presented as n (%) unless otherwise indicated.
Etiology was unknown for some patients. Percentage reflects number of patients with respective etiology divided by number of patients with known etiology based on information from medical records.
Among patients with glenoid bone loss.
The primary indication for surgery in all patients was recurrent shoulder instability. In the depression group, surgical interventions included 69 soft tissue repairs (63%) and 41 bone augmentation procedures (37%). In the nondepression group, treatment consisted of 302 soft tissue repairs (72%) and 119 bone augmentation procedures (28%). The difference in procedure types between the 2 groups did not reach statistical significance (P = .07) (Table 3).
Procedure Type and Tabulation of Procedures Performed a

Data are presented as n (%). DTA, distal tibial allograft.
Soft tissue repair included both arthroscopic and open Bankart repair.
Bone augmentation included both open Latarjet and DTA.
Functional Outcomes and PROs
Patients with a preoperative diagnosis of depression demonstrated significantly lower baseline ROM for forward elevation (145°± 34° vs 157°± 27°; P < .001), IR (T12 vs T11; P = .003), and ER (60°± 17° vs 64°± 15°; P = .05) compared with those without depression. Both groups showed improvements in forward elevation ROM postoperatively, and measurements at final follow-up were comparable (163°± 19° vs 165°± 18°; P = .13). However, patients with depression had diminished postoperative ER ROM, with significantly lower final measurements compared with those without depression (57°± 17° vs 63°± 14°; P < .001). Mean postoperative ROM for IR showed no improvement and remained lower among patients with depression (T12 vs T11), but the difference between the groups was not found to be statistically significant (P = .06) (Table 4). On average, all patients had 5/5 strength in all measures pre- and postoperatively.
Comparative Functional Outcomes of Range of Motion a
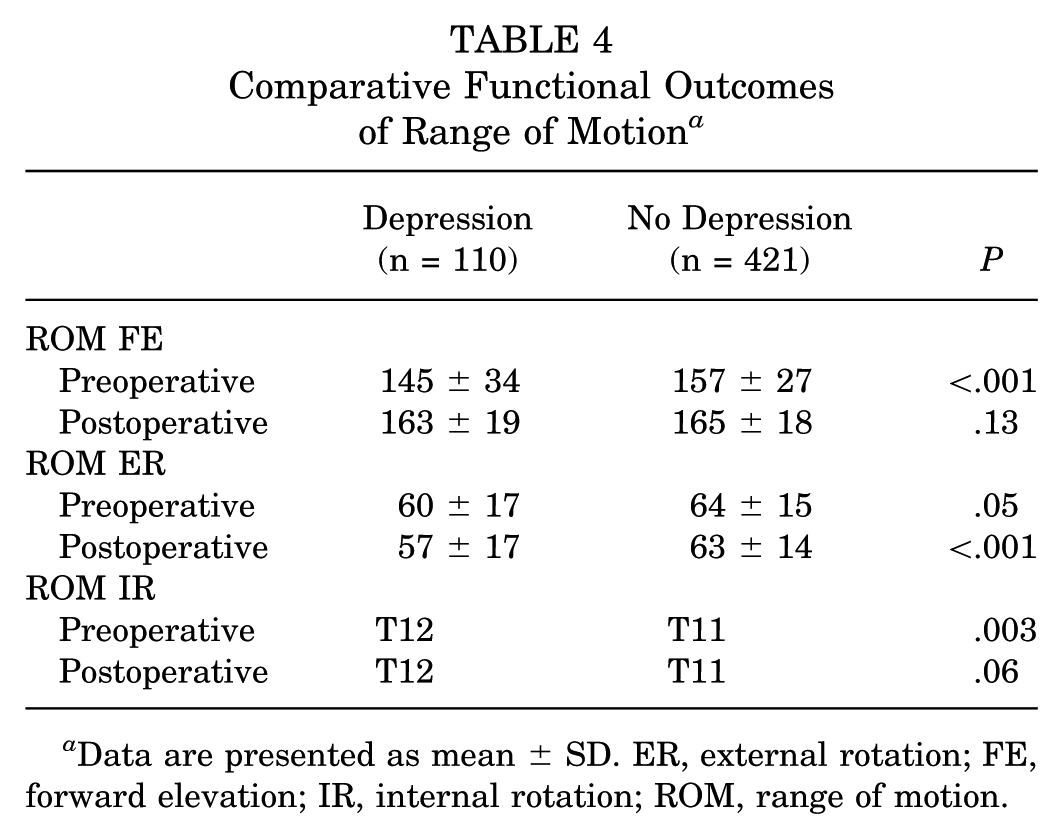
Data are presented as mean ± SD. ER, external rotation; FE, forward elevation; IR, internal rotation; ROM, range of motion.
Patients in the depression cohort had inferior scores on self-reported questionnaires used to assess shoulder function. Patients with depression reported similar levels of return to sport after shoulder stabilization surgery when compared with those without depression as assessed by the short SIRSI form (60.9 ± 33.1 vs 73.2 ± 24.2; P = .24). In terms of subjective shoulder function, patients in the depression cohort had significantly lower SANE scores (82.1 ± 15.8 vs 87.8 ± 12.1; P = .04) and ASES (78.8 ± 19.8 vs 88.6 ± 12.5; P = .02) forms. Last, patients with depression reported similar VAS pain scale scores after surgery when compared with those without depression (2.2 ± 2.5 vs 1.4 ± 1.8; P = .21) (Table 5). While not statistically significant, we did find that a higher proportion of patients with depression reported being “very dissatisfied” (5.4% vs 1.8%) and “dissatisfied” (5.4% vs 2.7%) with their shoulder stabilization surgery (P = .41). Furthermore, more patients without depression reported being “very satisfied” (69.6% vs 56.8%) with the outcomes of their shoulder surgery (Table 6).
Comparative Patient-Reported Outcomes a

Data are presented as mean ± SD. ASES, American Shoulder and Elbow Surgeons; SANE, Single Assessment Numeric Evaluation; Short SIRSI, short, 5-item Shoulder Instability–Return to Sport After Injury; VAS, visual analog scale for pain.
Comparative Patient Satisfaction by Patient Type a

Data are presented as n (%). P = .41. Of depression patients, 37 were available for phone interview with satisfaction survey. Of patients without depression, 112 were available for phone interview with satisfaction survey. Percentages reflect these denominators.
Recurrent Instability and Survival Analysis
Recurrent instability rates were higher in the depression group compared with the nondepression group (23% vs 14%; P = .03). Depression was also associated with lower recurrence-free survival at 2 years (82% vs 90%), 5 years (62% vs 80%), and 10 years (52% vs 62%) (P = .02) (Figure 1). Patients who underwent bony augmentation had significantly lower rates of recurrence, regardless of depression status (11% vs 18%; P = .04). Reoperation rates did not differ significantly between groups. Overall, 66 patients (12%) underwent revision surgery after the index shoulder stabilization, with recurrent shoulder instability being the most common indication for revision in both groups (depression, n = 10/18 [56%]; no depression, n = 28/48 [58%]). Among patients with depression, 18 (16%) underwent revision surgery at a mean of 2.3 years postoperatively, compared with 48 patients (11%) without depression, who underwent revision surgery at a mean of 3.7 years following index shoulder stabilization. While the difference in revision rates between the 2 cohorts was not statistically significant (P = .33), the earlier time to revision in the depression group was statistically significant (P = .03).

Kaplan-Meier curve for instability recurrence–free survival by patient type.
Discussion
Patients with a preoperative diagnosis of depression experienced inferior outcomes after shoulder stabilization surgery, including higher rates of recurrent shoulder instability, lower postoperative ROM, and poorer PROs (SANE and ASES scores). These findings support our hypothesis that depression negatively affects both patient-reported and functional outcomes after surgery. Previous literature is limited to a single study 24 that reported outcomes after shoulder stabilization surgery in a relatively small cohort of patients with and without depression. Our current study includes the largest sample size to date of patients with depression undergoing shoulder stabilization and provides a comprehensive analysis of the differences in outcomes between these groups.
In our study, a medical history of depression was found in 21% of the patients. This aligns with other studies reporting similarly high rates of depression in patients undergoing various upper-extremity procedures, although methodological differences limit direct comparison. Weekes et al 24 reported 51% of patients undergoing shoulder stabilization surgery had clinical depression as assessed by the Quick Inventory of Depressive Symptomatology–Self Report (QIDS-SR) preoperatively. Furthermore, Cho et al 4 reported the prevalence of depression among patients undergoing RCR to range from 12.8% and 26.2% using the Hospital Anxiety and Depression Scale (HADS). Quantification of depressive symptoms in both studies was performed prospectively, allowing the potential effect of the upper-extremity injury on depressive symptoms to be considered. In contrast, Freshman et al 7 reported that 14.6% of patients undergoing arthroscopic RCR had a diagnosis of depression within the 1-year preoperative period based on ICD-10 codes. The high prevalence of depression among patients in our study may reflect the use of lifetime depression diagnoses rather than restricting it to a narrower preoperative time frame, although diagnosis was confirmed with antidepressant medication status in the year before surgery. The prevalence of depressive symptoms at the time of surgery may still be underestimated in our study, as the pain and functional limitations associated with shoulder instability likely exacerbate preexisting depression. Regardless of methodological differences, the prevalence of depression among patients with shoulder instability is well above that of adults in the United States, which raises concern.
Regarding postoperative complications, we found patients with depression to have lower rates of instability-free survival after shoulder stabilization surgery. Despite increased rates of recurrent shoulder instability in patients with depression, both cohorts had similar rates of revision after primary stabilization. Similarly, Freshman et al 7 report higher rates of postoperative complications after arthroscopic RCR among patients with a preoperative diagnosis of a mental health disorder. While our study focused on recurrent shoulder instability as a complication of interest, our results agree with those reported previously regarding arthroscopic RCR. Notably, they did report an increased rate of revision arthroscopic RCR and conversion to shoulder arthroplasty. These differences could arise from the fact that the incidence of failed RCR is high among all patients and commonly warrants revision or conversion to shoulder arthroplasty. In contrast, revision after shoulder stabilization is less common, and our sample size may not be adequately sized to detect any differences.17,26
Furthermore, depression may affect the interpretation of instability sensations, and these patients may be more apt to report subluxations after surgery. Not all instability events are considered equal, and surgeons may view mild or infrequent episodes as manageable without surgery, especially in patients with lower functional demands or limited interest in revision. These patient- and surgeon-related factors likely also contribute to the observed discrepancy between recurrence and revision rates.
In our study, patients with a preoperative diagnosis of depression had worse preoperative shoulder function in all measures of ROM. Postoperatively, ER ROM remained significantly lower among patients with depression when compared with those without depression. Improvements in shoulder function were limited to forward elevation ROM in our cohort, and patients in the depression cohort experienced decreased mean ER ROM after surgery. No previous studies have compared pre- and postoperative ROM measurements between patients with depression and those without. Our results are partially explained by the fact that most shoulder stabilization surgeries in our study included capsulorrhaphy, or tightening of the joint capsule, which may limit range of motion in ER. Given that the primary measure of success is shoulder stability, surgeons are often willing to sacrifice postoperative ROM to gain stability of the shoulder. 11 Patients with depression may have been disproportionately affected by this, as patients with mood disorders have been shown to have significantly lower rates of compliance with physical therapy after other shoulder procedures, such as shoulder arthroplasty. 6
PROs and satisfaction are important metrics when evaluating the success of elective surgical procedures. Weekes et al 24 reported patients with clinical depression having inferior preoperative shoulder function based on the Western Ontario Shoulder Instability Index (WOSI) questionnaire. 24 Both groups showed improvements in WOSI scores 1 year postoperatively, but patients in the clinical depression group continued to have worse WOSI scores than those without depression after shoulder stabilization surgery. Similarly, a meta-analysis by Davey et al 5 found that patients with preexisting mood disorders had significantly lower ASES and Simple Shoulder Test scores after arthroscopic RCR and were more likely to experience postoperative pain. Our findings align with these trends, as patients in the depression cohort demonstrated significantly lower ASES and SANE scores after shoulder stabilization. Although patients with depression reported higher mean levels of postoperative shoulder pain, the results were not statistically significant in our study. This difference may stem from the acute and traumatic nature of most shoulder instability cases compared with the chronicity of rotator cuff tears. Evidence from Nichols et al 19 supports this hypothesis, showing that psychological factors more strongly influence symptomatology in patients with atraumatic, chronic shoulder instability. Given that most patients in our cohort underwent surgery for traumatic shoulder instability, the effect of depression on postoperative pain may be less pronounced than in chronic shoulder conditions. Furthermore, pain and depression are often comorbid conditions with a bidirectional relationship. As shoulder stabilization surgery has been shown to significantly decrease depressive symptomatology, this may improve pain in this cohort after surgery. 24
We used the short SIRSI score to compare the psychological readiness to return to play after surgery. Previous studies have analyzed psychological factors that affect return to sport after shoulder stabilization surgery. A recent systematic review by Gibbs et al 8 found that psychological factors were cited by the majority of patients who failed to return to sport, with the most common factor being fear of reinjury. Although patients with depression in our cohort did report lower short SIRSI scores on average, the difference between cohorts was not statistically significant. Hence, other psychological factors such as fear of reinjury or kinesiophobia may have a more pronounced effect on return to play when compared with depression.
Beyond conventional PRO measures, we also asked patients, “How satisfied are you with the results of your surgery?” to assess patient satisfaction. We found a higher percentage of patients without depression to report being “very satisfied” with the outcome of the operation. To our knowledge, this is the first study to investigate the effect of depression on patient satisfaction after shoulder stabilization surgery. Previous studies have analyzed the association of improvements in preoperative mental health status with improved patient satisfaction after RCR. Utilizing a novel 4-question patient satisfaction questionnaire, Moore et al 18 found that significantly more patients who reported improvements in emotional mental status before RCR achieved satisfaction after surgery. The lower rates of patient satisfaction for patients with depression in our study are similar to those previously reported for RCR patients. This suggests that interventions aimed at improving mental health status in patients with depression before arthroscopic shoulder surgery may lead to improvements in patient satisfaction.
While the correlation between depression and inferior PROs after shoulder surgery has been identified, the potential mediators of this correlation have yet to be fully elucidated. Expectations before shoulder stabilization surgery can influence patients' subjective assessment of a successful operation. These expectations may differ between surgeons and patients, with the latter more reluctant to sacrifice shoulder function at the cost of shoulder stability. Furthermore, patients with higher levels of pain and disability before surgery often have higher expectations for pain relief than other patients. 11 Previous research suggests that depression correlates with worse subjective measures of pain, disability, and quality of life before shoulder surgery. 4 While the retrospective design of our study did not allow for subjective assessment of patients before surgery, we report similar findings, as patients with depression in our cohort had inferior preoperative shoulder function. Given worse preoperative shoulder function, patients with depression may have a unique set of expectations. Identification of patients with depression, thorough assessment of their expectations, and adequate patient education before shoulder stabilization surgery could improve their subjective assessment of postoperative shoulder function. This is supported by previous studies on elective surgery that report better subjective postoperative outcomes in patients who were better educated about the planned procedure. 10
Limitations
While this study addresses a critical gap in literature, it has several limitations. Baseline demographic differences may confound the ability to isolate depression as an independent risk factor for poorer functional outcomes. Additionally, the use of data from a single institution limits the generalizability of our findings. The retrospective design further restricted our capacity to assess depressive symptoms at the time of surgery and identify patients with depression related to the underlying orthopaedic condition using validated tools such as the HADS or QIDS-SR. Although these tools have been employed in previous research, clinical diagnosis of depression has been shown to have greater predictive value than questionnaire-based assessments in evaluating its relationship with medical conditions. 1 Despite the association between depression and inferior postoperative outcomes, most patients achieved shoulder stability, confirming the utility of shoulder stabilization surgery in this subset of patients. Importantly, patients with depression in our study did not receive standardized psychological support as part of their perioperative care. While some patients may have independently sought treatment for depression, coordinated mental health interventions were not integrated into the surgical management process. The role of patient expectations in influencing outcomes after other arthroscopic shoulder procedures warrants further investigation in the realm of shoulder instability.
Conclusion
Patients with depression had increased rates of recurrent instability and lower PRO scores after shoulder stabilization surgery. Shoulder stabilization surgery is an effective treatment option for patients with depression, but depression evaluation should be considered in the preoperative assessment to aid in patient and physician education on the risks of inferior clinical outcomes.
Footnotes
Final revision submitted June 15, 2025; accepted July 8, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: G.L.J. has received honoraria from the Musculoskeletal Transplant Foundation. R.C.R. has received nonconsulting fees from Arthrex. J.Y.B. has received consulting fees from Stryker Corp and Arthrex. G.L.C. has received research funding from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The Ohio State Biomedical Sciences institutional review board (Approval #2024H0084).