
Abstract
Background:
Bone marrow lesions (BMLs) are associated with knee pain and predict structural changes and joint replacement. Their significance in the context of opening-wedge high tibial osteotomy (OWHTO) is, however, unclear.
Purpose:
To investigate whether preoperative BMLs are associated with cartilage regeneration-like tissue and postoperative patient-reported outcomes after OWHTO and to evaluate how 1-year changes in BMLs (ΔBML) relate to these outcomes.
Study Design:
Cohort study: Level of evidence, 3.
Methods:
In this retrospective study, 138 knees underwent arthroscopy during OWHTO, and 85 knees underwent follow-up arthroscopy. Participants also completed questionnaires and underwent magnetic resonance imaging (MRI). Cartilage status at the medial femoral condyle (MFC) and medial tibial plateau (MTP) was evaluated using the International Cartilage Research Society (ICRS) grading system during initial and follow-up arthroscopies to assess improvement after OWHTO. Postoperative outcomes were assessed using the Knee injury and Osteoarthritis Outcome Score (KOOS). BMLs were scored according to the MRI Osteoarthritis Knee Score, and ΔBML was calculated.
Results:
The preoperative BML score weakly correlated with the initial ICRS grade at the MFC (r = 0.306; P < .001) and MTP (r = 0.353; P < .001). At the MTP, a preoperative smaller BML score was significantly associated with cartilage improvement (P = .030). In addition, preoperative large BML significantly correlated with improvement in ΔBML scores at the MFC (r = 0.643; P < .001) and the MTP (r = 0.757; P < .001). Regression analysis demonstrated that postoperative valgus alignment and low body mass index (BMI) were correlated with cartilage improvement in MFC; in contrast, cartilage improvement in MTP was correlated with low BMI, preoperative higher ICR grade, and a smaller preoperative BML. Also, improvement in BML scores on MTP was correlated with better KOOS symptoms 1 year after high tibial osteotomy (HTO) (P = .045).
Conclusion:
Smaller preoperative BMLs were associated with greater postoperative cartilage improvement in MTP after OWHTO. Furthermore, BML improvement was significantly related to better knee symptoms in short- to midterm patient-reported outcomes after OWHTO.
Keywords
High tibial osteotomy (HTO) is an effective treatment for medial knee osteoarthritis (OA), as it shifts the mechanical axis from the medial to the lateral compartment. 28 Among HTO procedures, opening-wedge HTO (OWHTO) is commonly performed and allows for more accurate correction in coronal planes than closed-wedge HTO.16,27 While relatively good mid- to long-term survival rates have been achieved,2,10,30 patient-reported outcomes (PROs) are not always excellent. 35 Poorer postoperative PROs are associated with inferior cartilage regeneration-like tissue, undercorrection (lower postoperative weightbearing line ratio [WBLR]), and proximal tibial morphology.9,26,38 The association of PROs with preoperative magnetic resonance imaging (MRI) findings, however, remains unclear.
Bone marrow lesions (BMLs) observed on MRI are potential indicators of focal bone fragility in knees with OA. BML histology reflects subchondral bone changes, including microcracks, active bone remodeling, edema, fibrosis, and bleeding. 21 BMLs are associated with knee pain3,19,33,43 and altered bone metabolism,13,29,31 and predict radiographic structural changes5,6 and the eventual need for joint replacement. 36 Therefore, the presence of preoperative BMLs might be considered to predict limited cartilage improvement or inferior postoperative PROs after OWHTO.
This study investigated whether preoperative BMLs are associated with postoperative cartilage regeneration-like tissue and PROs after OWHTO, and evaluated how 1-year changes in BMLs (ΔBML) relate to these outcomes. We hypothesized that patients with large preoperative BMLs would exhibit less cartilage improvement and inferior PROs compared with those without BMLs, and that reducing the BML area would be associated with cartilage regeneration-like tissue filling.
Methods
Patients
In this retrospective cohort study, 190 consecutive knees underwent OWHTO for medial unicompartmental knee OA by surgeons in our hospital between November 2008 and July 2023. The patients were followed for at least 1 year. When the opening gap was filled with newly formed bone based on imaging (radiograph and tomosynthesis), the implant was removed. In cases with poor new bone formation, implant removal at 1 year was postponed, and these cases were excluded from this study. The inclusion criteria for OWHTO were symptomatic varus radiographic knee OA of Kellgren-Lawrence (KL) grade ≥2 with articular cartilage lesions, and with or without subchondral bone insufficiency fractures of the knee on the medial femoral condyle (MFC) or medial tibial plateau (MTP). Varus alignment was defined as the weightbearing line passing through <40% of the tibial plateau width from the medial edge. Eligibility was determined regardless of patient age or history of partial meniscectomy. The exclusion criteria were active knee infection (n = 0); inflammatory diseases, such as rheumatoid arthritis (n = 0); malignancy (n = 1); no implant removal or second-look arthroscopy (n = 41); no preoperative MRI data (n = 3); and incomplete knee injury and OA outcome scales (Kee injury [KOOS]) data (n = 8). Finally, among 190 consecutive knees that underwent OWHTO, 138 knees with initial arthroscopy during OWHTO, preoperative MRI, and completed questionnaires were enrolled in a cross-sectional statistical analysis of the relationship between preoperative BMLs and postoperative cartilage status and PROs. Additionally, 85 of 138 knees that underwent follow-up arthroscopy and postoperative MRI >1 year after OWHTO were included in a longitudinal statistical analysis of the association between improvements in BMLs, cartilage status, and PROs after OWHTO.
This retrospective observational study design was approved by the ethics committee of our institution (Ref No. 2019-1096). Informed consent was obtained from all patients for treatment and for the use of their clinical data for research and publication.
Surgical Procedure
Before surgery, the target for postoperative lower limb alignment was to position the weightbearing line, approximated by the mechanical axis, to pass through the Fujisawa point, which corresponds to 62.5% of the width of the tibial plateau measured from the medial edge. 7 Digital planning was performed using MediCAD (Hectec GmbH) based on anteroposterior whole-leg radiographs under full weightbearing conditions.
The surgical procedure has been previously described in detail and is briefly summarized here. 38 After arthroscopy, OWHTO was performed using various plates: the Puddu plate (Arthrex), Position HTO plate (Aesculap), and Tris Medial HTO Plate System (OLYMPUS). A longitudinal skin incision was made on the medial aspect of the proximal tibia, and the pes anserinus was identified. The first layer was incised along the superior border of the pes anserinus, and the pes was retracted posteriorly to expose the superficial medial collateral ligament. The osteotomy level was determined by fluoroscopy, and the superficial medial collateral ligament was transected using a chisel and knife. A monoplane or biplane osteotomy was performed, leaving the lateral 10 mm of the tibial head intact as a hinge for the osteotomy. The WBLR was measured from the center of the femoral head to the talus using an alignment rod under fluoroscopic guidance. While the opening gap was determined by the WBLR based on preoperative planning, it was reduced in preoperative planning when the medial proximal tibial angle exceeded 95°. A wedged β-tricalcium phosphate block (HOYA Technosurgical Co, Ltd) was placed posteriorly in the opening gap space, and the proximal tibia was fixed to the plate.
As part of postoperative rehabilitation, patients were allowed partial weightbearing immediately for 3 weeks after surgery, followed by full weightbearing. Range of motion exercises were started the day after surgery. Depending on the level of postoperative pain, patients were allowed to return to their daily activities. Except in cases of nonunion, the implant was removed at 1 year.
Arthroscopic Evaluation of the Cartilage
Arthroscopy was performed at the time of both OWHTO and implant removal to assess the conditions of the cartilage, meniscus, and cruciate ligaments. The severity of the articular cartilage damage was scored from 0 to 4 according to the International Cartilage Research Society (ICRS) grading system 20 on the MFC, lateral femoral condyle (LFC), MTP, lateral tibial plateau (LTP), trochlea, and patella. The ICRS grades were assigned by consensus of the operating surgeons at the time of the arthroscopy and recorded in the medical record. ICRS grades range from 0 to 4, with higher grades indicating a greater degree of cartilage damage. The summed ICRS grades of the 6 locations were used for statistical analysis as an index of degeneration. We defined cartilage improvement as replacing damaged cartilage with fibrocartilage and an improvement in ICRS grade.
Radiographic Evaluation
Pre- and postoperative radiographic parameters were measured using digital planning software (MediCAD). Postoperative radiographs were evaluated at 1 year after OWHTO. The WBLR, joint line convergence angle, and medial proximal tibial angle (MPTA) were measured using the anteroposterior views of the whole leg under weightbearing conditions. The mechanical axis was defined as the line from the center of the femoral head to the center of the talus on a weightbearing radiograph. The WBLR was defined as the percentage of the tibial plateau width at which the mechanical axis passed relative to the medial edge. 12 The MPTA was defined as the medial angle formed between the mechanical tibial axis and a line tangential to the joint surface of the proximal tibial plateau. The posterior tibial slope (PTS) was measured in lateral knee radiographs. 8 The KL grade and all radiographic parameters were independently assessed by 2 orthopaedic surgeons (K.K. and T.T.) to evaluate interrater reliability, and repeated measurements were performed to assess intrarater reliability. High intra- and interrater reliability of alignment measurements using mediCAD software has been reported. 34
Evaluation of BMLs on MRI
Pre- and postoperative MRI data were used. A postoperative MRI was obtained after implant removal at 1 year after OWHTO. BMLs were defined as areas of low signal intensity on T1-weighted images and high signal intensity on Short T1 Inversion Recovery sequences on MRI. BMLs were assessed on a 4-point scale according to the MRI Osteoarthritis Knee Score system. 13 Each region was scored as follows: 0, none; 1, <33%; 2, 33%–66%; and 3, >66% of the affected region. Evaluations were conducted in 6 regions: 3 on the MFC (trochlear, central, and posterior) and 3 in the medial tibial regions (anterior, central, and posterior) (Figure 1). The total MFC score ranged from 0 to 9 points, and the total MTP score was calculated similarly. The sum of the MFC and MTP scores represented the overall medial BML burden. Patients with a total BML score of 0 were classified as the non-BML group, while those with scores ranging from 1 to 9 were classified as the BML group. BML scoring was performed by a single orthopaedic surgeon (K.K. and T.T.); therefore, interrater reliability was not assessed. A change in the BML score from the pre- to postoperative evaluation was defined as the ΔBML score (preoperative BML score – postoperative score). A ΔBML score of ≥1 point was considered to indicate BML improvement after OWHTO.

Changes in lower limb alignment, BMLs, and arthroscopic findings before and after OWHTO.
Statistical Analysis
Quantitative data are expressed as the mean ± standard deviation. The chi-square test was used to evaluate differences in categorical variables, and the Mann-Whitney U test was used to evaluate differences in continuous variables between the non-BML and BML groups. The Spearman rank correlation test was performed to investigate the correlation between the preoperative BML score and the preoperative ICRS grade, preoperative BML scores on the MFC and MTP, ΔBML, and postoperative radiographic parameters. To investigate factors associated with cartilage improvement, logistic regression analysis was performed with cartilage improvement as the dependent variable and age, sex, preoperative body mass index (BMI), postoperative radiographic parameters, preoperative ICRS score, and BML as independent variables. To investigate factors related to the postoperative KOOS subscales, multiple linear regression analyses were performed with KOOS subscales as dependent variables and age, sex, preoperative BMI, postoperative radiographic parameters, preoperative ICRS score, and BML as independent variables. To analyze factors related to cartilage improvement, logistic regression analysis was performed with cartilage improvement as the dependent variable and age, sex, preoperative BMI, postoperative radiographic parameters, preoperative ICRS score, and ΔBML as the independent variables. To investigate factors related to postoperative KOOS subscales, multiple linear regression analyses were performed with KOOS subscales as dependent variables and age, sex, preoperative BMI, postoperative radiographic parameters, preoperative ICRS score, and ΔBML as independent variables. Data input and analysis were performed using SPSS software Version 29 (SPSS Inc). Statistical significance was set at P < .05. The post-hoc power of relationships between preoperative BMLs and cartilage improvement on MTP and between cartilage improvement and KOOS symptoms were 0.998 and 0.861, respectively. All statistical analyses were performed with SPSS (Version 29; SPSS, Inc)
Results
Patient Characteristics
The mean patient age at the time of OWHTO was 57.9 ± 6.9 years (range, 33-78 years), and the mean follow-up period was 4.2 ± 2.9 years (range, 1.2-15.3 years) (Table 1). No significant differences were observed between the BML and non-BML groups in age, sex, BMI, opening distance, or follow-up period for either the MFC or MTP. Mean preoperative BML scores were 1.2 ± 2 for the MFC and 1.5 ± 2 for the MTP. Of 138 knees, BMLs were detected in the MFC in 65 knees (47.1%) and in the MTP in 80 knees (58%). Arthroscopy revealed cartilage improvement after OWHTO in the MFC in 54 knees (39.1%) and in the MTP in 38 knees (27.5%).
Patient Characteristics a

Data are presented as mean ± SD or n (%). BMI, body mass index; BML, bone marrow lesion; ICRS, International Cartilage Repair Society; LFC, lateral femoral condyle; LTP, lateral tibial plateau; MFC, medial femoral condyle; MTP, medial tibial plateau; Preop, preoperative.
Radiographic data are shown in Table 2. The preoperative hip-knee-ankle angle (HKAA), WBLR, and MPTA all showed significant changes postoperatively (P < .001; P < .001; and P < .001, respectively). The intrarater reliability of the KL grade, HKAA, WBLR, and MPTA was 0.92 (95% CI, 0.88-0.94), 0.94 (95% CI, 0.91-0.96), 0.97 (95% CI, 0.96-0.98), and 0.97 (95% CI, 0.95-0.98), respectively. The interrater reliability of those parameters was 0.90 (95% CI, 0.84-0.94), 0.93 (95% CI, 0.82-0.99), 0.97 (95% CI, 0.95-0.98), and 0.93 (95% CI, 0.90-0.96), respectively.
Radiographic Parameters a
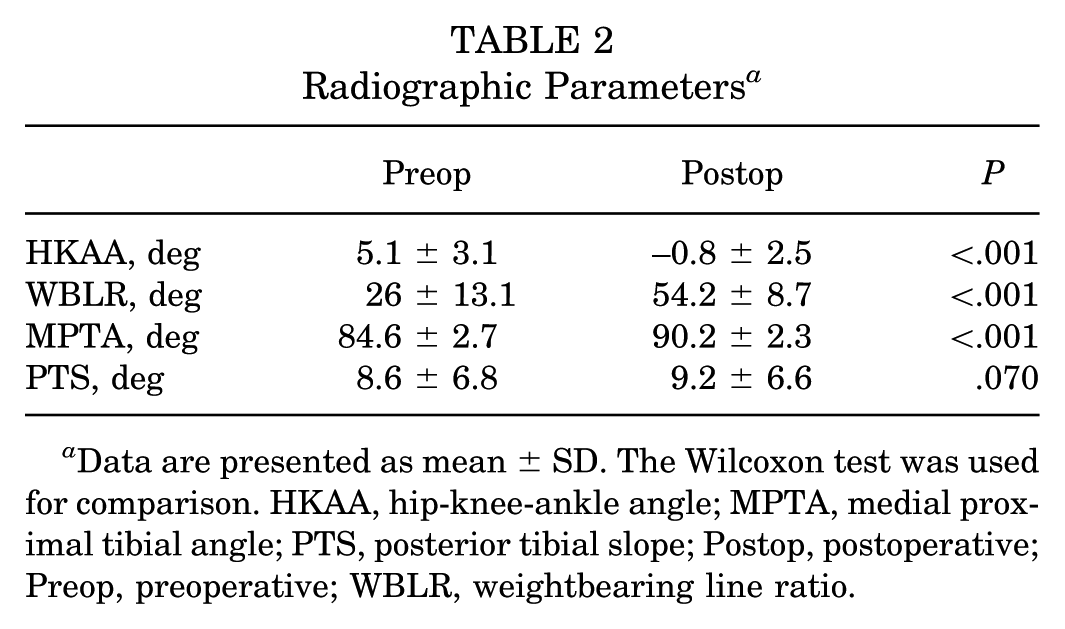
Data are presented as mean ± SD. The Wilcoxon test was used for comparison. HKAA, hip-knee-ankle angle; MPTA, medial proximal tibial angle; PTS, posterior tibial slope; Postop, postoperative; Preop, preoperative; WBLR, weightbearing line ratio.
Association Between Preoperative BMLs and Cartilage Improvement and PROs
The preoperative BML score correlated with the initial ICRS grade of the MFC (r = 0.306; P < .001) and MTP (r = 0.353; P < .001). Furthermore, preoperative BML scores of the MFC correlated significantly with those of the MTP (r = 0.382; P < .001). No correlation was detected between the preoperative BML score and BMI, preoperative HKAA, WBLR, MPTA, or PTS in either the MFC or MTP.
In the MFC, the preoperative BML score was not related to cartilage improvement, whereas the postoperative WBLR showed a weak association (P = .020) (Table 3). In contrast, in the MTP, the preoperative lower BML score and higher ICRS grade were weakly associated with cartilage improvement 1 year after OWHTO (P = .030 and P < .001) (Table 3). Furthermore, BMI and ICRS grade at the time of OWHTO were also associated with cartilage improvement in the MTP (P = .041 and P < .001, respectively). No significant difference in the KOOS scores was detected between the BML and non-BML groups (Table 4).
Factors Related to Cartilage Improvement a

The analysis was performed using logistic regression analysis. BMI, body mass index; BML, bone marrow lesion; ICRS, International Cartilage Repair Society; MFC, medial femoral condyle; MTP, medial tibial plateau; MPTA, medial proximal tibial angle; OR, odds ratio; Postop, postoperative; Preop, preoperative; PTS, posterior tibial slope; WBLR, weightbearing line ratio.
Postoperative KOOS Scores a

The Mann-Whitney U test was used for comparison. Data are presented as mean ± SD.
ADL, activities of daily living; BML, bone marrow lesion; KOOS, Knee injury and Osteoarthritis Outcome Score; MFC, medial femoral condyle; MTP, medial tibial plateau; QoL, quality of life.
Association Between BML Change and Cartilage Improvement and PROs
Postoperative BML scores in the MFC and MTP were significantly reduced to 0.8 ± 1.2 and 0.9 ± 1.1, respectively, compared with preoperative values (P = .039 and P < .001, respectively). In addition, the BML score improved in the MFC in 23 of 138 knees (27%) and in the MTP in 34 of 138 knees (40%). The ΔBML scores for the MFC and MTP were 0.3 ± 1.8 and 0.7 ± 1.6, respectively, and were significantly correlated (P = .001) (Figure 2A). In addition, the preoperative BML scores and ΔBML scores in the MFC (Figure 2B) and MTP (Figure 2C) were significantly correlated (P < .001 and P < .001, respectively). Furthermore, the postoperative WBLR correlated significantly with the ΔBML score in the MTP (P = .036) (Figure 2D). Regarding the postoperative PROs, linear regression analysis showed that improvement in the BML score in the MTP significantly correlated with KOOS symptoms (P = .045) (Table 5).

Scatterplots of ΔBML scores.
Factors Related to Postop PROs a
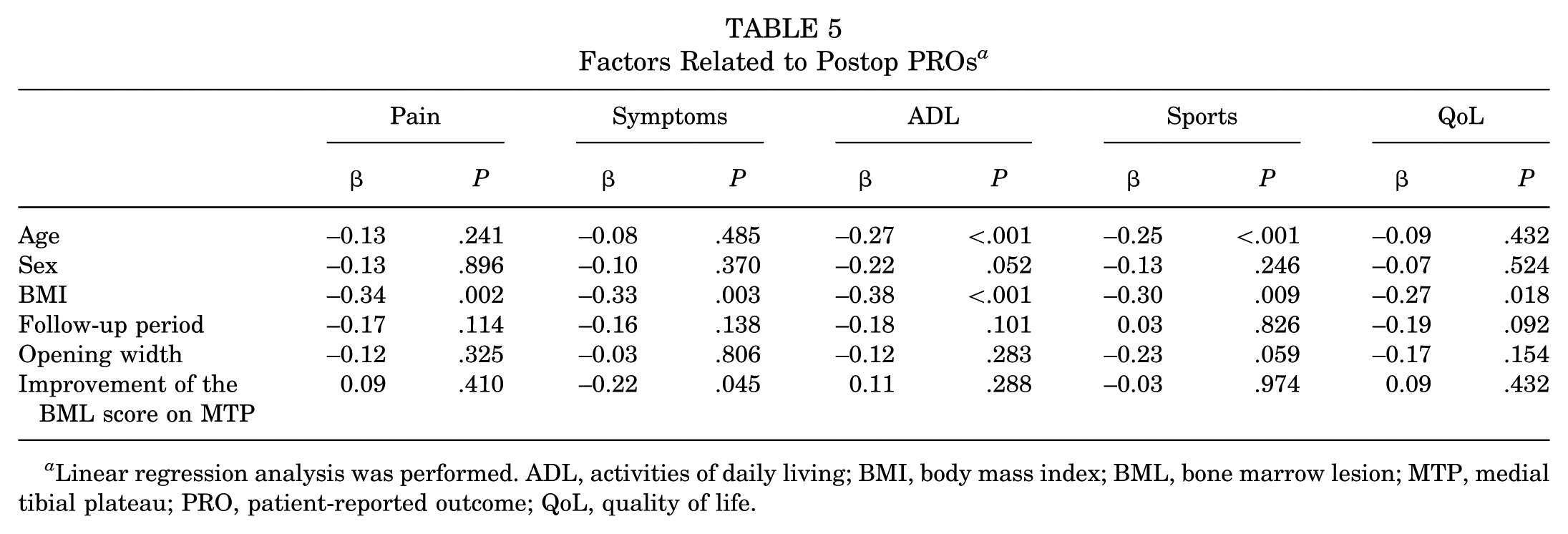
Linear regression analysis was performed. ADL, activities of daily living; BMI, body mass index; BML, bone marrow lesion; MTP, medial tibial plateau; PRO, patient-reported outcome; QoL, quality of life.
Discussion
The primary finding of the present study was that the preoperative smaller BMLs in the MTP were associated with cartilage improvement after OWHTO. Furthermore, improvement in the BML score in the MTP after OWHTO was associated with better postoperative KOOS symptom scores. These results suggest that the preoperative smaller BMLs predict cartilage regeneration-like tissue and reduced BML area at 1 year after OWHTO, reflecting more favorable short- to midterm outcomes after OWHTO.
BMLs are common in OA knees and reflect microcracks, bone remodeling, edema, fibrosis, and subchondral bleeding. Kon et al 21 reported that BMLs usually occur in the affected articular region, indicating bone remodeling. Koushesh et al 23 identified 7 histopathologic characteristics of BMLs: (1) cysts; (2) fibrosis; (3) hypervascularity; (4) cartilage islands; (5) trabecular thickening; (6) loss of tidemark integrity; and (7) inflammatory cell infiltration. Several authors have reported methods for evaluating BMLs. Hunter et al 11 reported imaging evaluation, and Koushesh et al 23 reported pathologic evaluation. BMLs are associated with pain and may be useful for evaluating treatment responses. 39
Cartilage improvement after HTO is generally attributed to fibrocartilage filling the lesion areas, with reported15,18 rates ranging from 35% to 92%.14,18,37 Cartilage improvement is affected by age, sex, BMI, preoperative cartilage status, and postoperative limb alignment.15,18,22,37,42 Kumagai et al 25 reported a significantly higher incidence of cartilage improvement in the MFC, in patients with a lower BMI, in cases with higher preoperative ICRS grades, and in knees that were overcorrected. 25 Otsuki et al 32 reported that a higher WBLR was associated with improved cartilage and clinical outcomes. Tsushima et al 38 reported that a smaller pre- and postoperative joint-line convergence angle was associated with improved ICRS grade and favorable midterm outcomes. In the present study, a low BMI, high ICRS grade with severe cartilage damage at the time of HTO, and BMLs in the MTP were factors associated with cartilage improvement. The findings regarding BMI and ICRS grade are similar to those reported in previous studies. Because OWHTO results in a valgus alignment, the contact pressure on the medial articular surface is reduced, 1 which could have improved BMLs and cartilage in the present study. In this study, only the BML in the MTP was found to be associated with cartilage improvement.
Several studies report that OWHTO reduces postoperative BMLs in the femur and tibia.4,24 One reason is that OWHTO shifts the axial load laterally, thereby relieving stress on the medial compartment. Therefore, a reduction of the BML score or area indicates recovery of the damaged subchondral lesion after surgery. In this case series, no direct association was observed between the postoperative WBLR and cartilage improvement. Postoperative WBLR was, however, associated with ΔBML scores in the MTP, which, in turn, were related to knee symptoms.
Kim et al 17 reported that postoperative valgus alignment reduces BMLs and that postoperative BML reduction correlates with positive postoperative outcomes. While some reports indicate that the larger the preoperative BML, the better the postoperative KOOS, 40 others report that the size of preoperative BMLs does not correlate with postoperative outcomes, 41 requiring further evaluation. In this study, ΔBML in the MTP was associated with KOOS symptoms. Although Kim reported that improvement of BMLs correlates with KOOS scores (eg, Pain, Symptoms, and ADL), 17 few studies have investigated whether a postoperative decrease in BMLs is associated with favorable postoperative PROs, and it remains unclear whether a decrease in BMLs after OWHTO is associated with favorable PROs based on KOOS scores.
This study has several limitations, primarily due to its retrospective and nonrandomized design. In addition, while the ICRS grade was evaluated by consensus of the operating surgeons, BMLs were measured by a single person. For a more accurate BML assessment, measurements should be obtained by several individuals. Furthermore, we report short- to midterm results with varying follow-up lengths. Also, many patients declined follow-up MRI because of the cost, leading to a smaller number of patients in the follow-up cohort. Finally, the surgeries were not performed by a single surgeon, introducing potential variations in plating techniques that could lead to under- or overcorrection.
Conclusion
Smaller preoperative BMLs were associated with improvement by cartilage-like tissue postoperatively after OWHTO with optimal correction. Furthermore, postoperative WBLR was significantly associated with improvement in BMLs at the MTP, which was significantly related to better knee symptoms in short- to midterm PROs after OWHTO. Therefore, this study revealed that fewer BMLs preoperatively and optimal lower limb alignment postoperatively might positively affect short- to mid-term outcomes after OWHTO.
Footnotes
Final revision submitted December 30, 2025; accepted January 4, 2026.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the ethics committee of Hirosaki University (No. 2019-1096-2).