
Abstract
Background:
No study has compared functional outcomes measured by validated Patient-Reported Outcomes Measurement Information System (PROMIS) measures of physical function (PF) and pain interference (PI) between augmented and nonaugmented Broström procedures.
Purpose:
To determine whether the augmented Broström procedure is associated with improved PROMIS scores compared with the nonaugmented procedure.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
All patients who underwent lateral ankle ligament reconstruction at a single institution (2013-2024) were retrospectively reviewed. Revisions, allografts, nonanatomic reconstructions, flexor digitorum longus transfers, progressive collapsing foot deformities, concomitant hindfoot arthrodesis, associated ankle arthroplasties, concomitant fractures, and those without a minimum of 2 years of follow-up were excluded. A total of 97 eligible patients (97 ankles) completed postoperative surveys containing PROMIS and were included for final analysis. Augmentation was performed using the InternalBrace system (Arthrex). Bivariate comparisons of PROMIS were made using t tests. A weighted linear regression model with robust standard errors was fitted to examine associations between PROMIS and the Broström technique, adjusting for clinically relevant covariates. Type-3 analysis of variance was performed to assess the significance of each predictor. Inverse probability of treatment was used to balance the distribution of covariates across techniques.
Results:
Of 97 patients, 56 (58%) underwent augmented Broström procedures, and 41 (42%) underwent nonaugmented Broström procedures. In unadjusted comparisons, the augmented type had a higher mean PF (51.2 ± 8.5 vs 48.5 ± 9.4; P = .16) and a lower PI (49.3 ± 9 vs 50.9 ± 10.5; P = .42) than the nonaugmented type. In adjusted models, the augmented type was associated with 4.68 (95% CI, 1.27 to 8.09) higher PF (P < .01) and 3.76 (95% CI, −7.85 to 0.33) lower PI (P = .07) compared with the nonaugmented type. Higher body mass index was associated with significantly worse PROMIS PF and PI in both unadjusted (P< .01 and P < .01) and adjusted analysis (P < .01 and P < .01). Varus deformity was associated with significantly lower PF compared with those with isolated ligamentous instability (–4.23 [95% CI, −8.42 to −0.04). No significant differences were observed in PF or PI at follow-up beyond 2 years (P = .55 and P = .37, respectively).
Conclusion:
Our study showed that the augmented Broström procedure was associated with significantly improved PROMIS scores compared with the nonaugmented Broström procedure to a degree that reaches the minimal clinically important difference for PROMIS. The augmented Broström procedure, therefore, may serve as an effective surgical option to maximize functional outcomes for patients suffering from chronic lateral ankle instability.
Chronic lateral ankle instability (CLAI) affects up to 25% to 40% of individuals, including 23% of all athletes.14,22 Also, 70% of people who sustain an ankle sprain may develop CLAI within months after the initial sprain. 14
When CLAI is present, patients may elect to undergo lateral ligament reconstruction to restore ankle stability. Multiple strategies for reconstruction exist, including both anatomic and nonanatomic methods. 1 Traditionally, the Broström procedure is performed, which is an anatomic reconstruction of the anterior talofibular ligament (ATFL) and the calcaneofibular ligament (CFL). To strengthen the repair, various strategies exist, such as the modified Broström, which incorporates the inferior extensor retinaculum and distal fibular periosteum into the reconstruction. 13
More recently, Broström with suture tape augmentation has been utilized, as the addition of suture tape is thought to further reinforce the repair's stability and strength.19,23 Previous studies suggest that augmented Broström may improve ankle stability, 2 but data are mixed on whether Broström with suture-tape augmentation improves functional outcomes compared with nonaugmented Broström. Several studies indicate that suture-tape augmentation may improve outcomes—including return to activity, foot and ankle outcome scores, Foot and Ankle Disability Index, American Orthopaedic Foot and Ankle Society (AOFAS) scores, Foot and Ankle Ability Measure (FAAM) scores, and Cumberland Ankle Instability Tool (CAIT) scores.1,3,4,9,10,17,18, 25,28,31,33 Others have found no significant differences in patient-reported outcomes (PROs) between augmented and nonaugmented Broström.5,20,21,26,32
While multiple types of suture tape exist, the InternalBrace (Arthrex) has proven particularly effective. Jain et al 17 demonstrated that InternalBrace augmentation resulted in lower time to return to preinjury activity level, higher rate of return to preinjury activity, and modest, nonsignificant improvements in visual analog scale (VAS) or Manchester-oxford foot questionnaire scores. Coetzee et al 4 revealed that the InternalBrace augmentation produced favorable AOFAS and FAAM scores. Moreover, a recent prospective study evaluating 127 patients found that Broström with InternalBrace augmentation generated both statistically and clinically significant improvements as measured by CAIT compared with nonaugmented Broström. 10
Few studies, however, have utilized validated Patient-Reported Outcomes Measurement Information System (PROMIS) computerized adaptive tests of physical function (PF) and pain interference (PI) to assess outcomes after Broström procedures. Unlike many commonly used legacy instruments—including FAAM, Foot Function Index, AOFAS scores, and VAS—PROMIS exhibits greater responsiveness, decreased floor and ceiling effects, time efficiency, and easily interpreted t score–based scoring systems.7,16,30 Scheinberg et al 29 found that patients achieved population-mean PROMIS scores after Broström-Gould procedures. However, this study did not compare PROMIS scores between Broström alone and Broström with augmentation.
No previous studies have compared augmented and nonaugmented Broström in terms of PROMIS scores. Therefore, this study aimed to determine whether Broström augmented with InternalBrace is associated with improved PROMIS scores compared with Broström without augmentation. We hypothesized that augmented Broström would result in higher PROMIS scores than nonaugmented Broström.
Methods
Population
This investigation was an institutional review board-approved (STU00210935, approved 11/19/2019) retrospective review of all patients who underwent lateral ankle ligament reconstruction at a single institution from January 2013 to January 2024. Two investigators (M.P. and A.R.K.) independently evaluated all cases. Revisions, allografts, nonanatomic reconstructions, flexor digitorum longus transfers, progressive collapsing foot deformities, concomitant hindfoot arthrodesis, associated ankle arthroplasties, and concomitant fractures were all excluded. Those without a minimum 2-year follow-up were also excluded. These 133 patients who were eligible for the study were contacted to complete postoperative surveys via REDCap, containing PROMIS computerized adaptive tests of PF and PI. Patients were contacted 5 times (3 emails and 2 phone calls from December 2024 to January 2025) before ceasing contact. Of 133 patients, 97 (97 ankles) completed the postoperative questionnaire and were included in the final analysis (see Figure 1 for study flowchart and Table 1 for baseline characteristics).
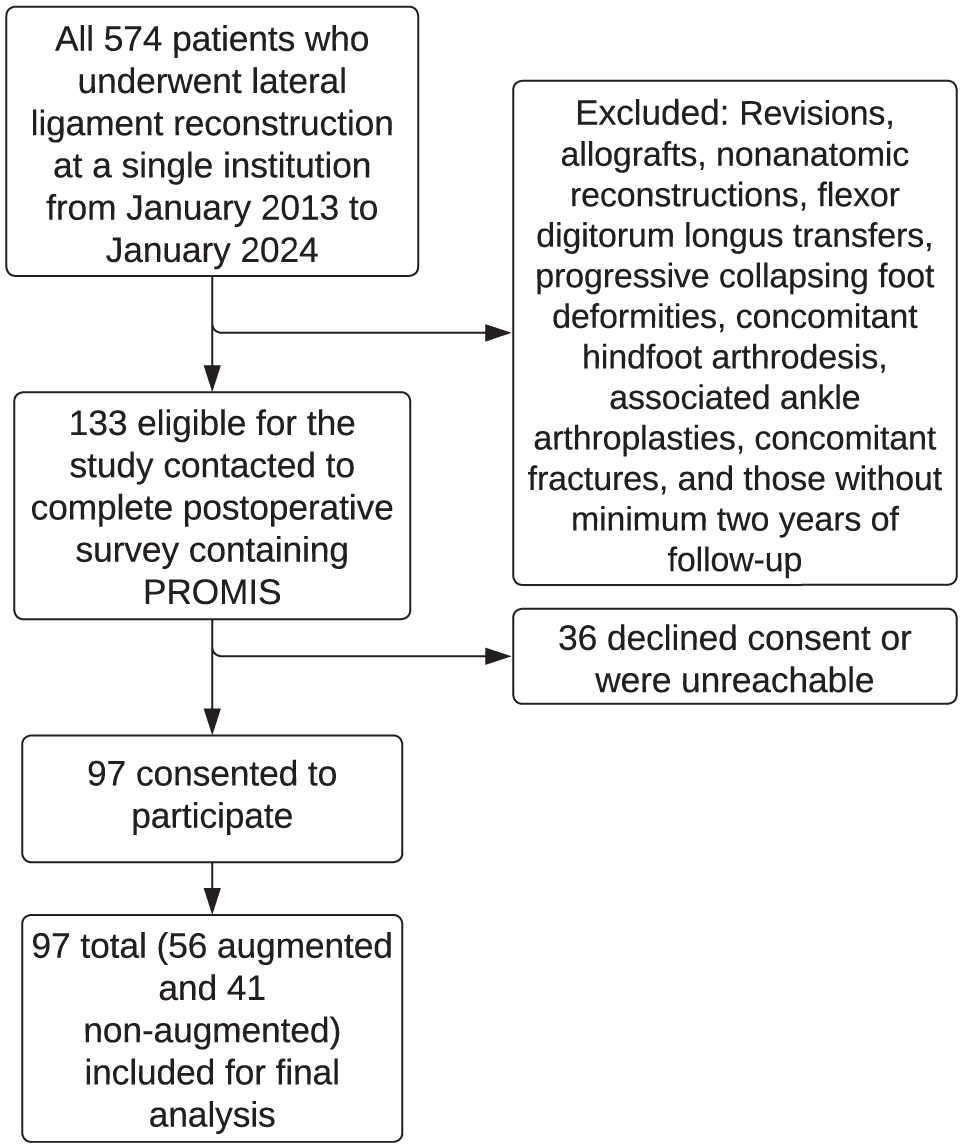
Study flowchart.
Baseline Characteristics a

BMI, body mass index; IQR, interquartile range.
Surgeon preference determined whether the Broström procedure was augmented or nonaugmented. Both augmented and nonaugmented Broström procedures were executed with the Gould modification. 13 Augmentation was performed using the InternalBrace system (Arthrex). A greater proportion of patients underwent Broström with augmentation after 2017 because the authors’ institution began performing more augmented than nonaugmented Broström procedures based on evidence suggesting that augmented Broström may result in improved outcomes.2,4,9,17
Patients were also classified based on CLAI cause: isolated ligamentous instability (CLAI without anatomic deformity, n = 54), osteochondral defect (OCD) (n = 12), or deformity (varus deformity, n = 31). Cavovarus deformity was defined radiographically by an increased talo-first metatarsal angle, or the Meary angle (>4° convex upward), elevated calcaneal pitch (>30°), increased first metatarsal-calcaneal angle, or the Hibb angle (>45°), and a decreased talocalcaneal angle (<20°).
Outcomes
The primary outcome was PROMIS PF and PI. PROMIS is a validated PRO metric specifically for ankle pathologies.15,16 Both PROMIS measures correspond to age-matched norms for the United States general population, with a mean score15,16 of 50. Higher PF designates better PF. Conversely, higher PI indicates greater pain interference with activity. The minimal clinically important difference (MCID) is a change of 3 to 30 in PROMIS scores.15,27
Statistical Analysis
The Pearson chi-square and the Fisher exact test were used to compare the distribution of characteristics across Broström techniques. Bivariate comparisons of PROMIS scores were performed using t tests for 2-group comparisons and 1-way analysis of variance for ≥3 groups. A weighted linear regression model with robust standard errors was fitted to examine the association between PROMIS scores and the Broström technique, adjusting for CLAI cause, body mass index (BMI), age, and sex. Inverse probability weighting was used to balance the distribution of covariates across the Broström technique. After weighting, the standardized mean difference across groups was <0.1. An a priori power analysis indicated that at α = .05, the study had 80% power to detect a minimum effect size of 0.52 (Cohen's d), corresponding to differences of 4.37 for PF and 4.60 for PI.
Surgical Technique
A standard anterolateral approach to the ankle was used, and the soft tissue cuff containing the ATFL and CFL was sharply elevated from the anterior and distal fibula, preserving a full-thickness periosteal cuff laterally. The anterior fibula was then decorticated, and 2 all-suture anchors (FiberTak; Arthrex) were placed—one proximal and one distal—into the prepared surface. Sutures were passed in a mattress fashion through the ligamentous cuff and tied down to reattach the tissue to bone, followed by reinforcement with figure-of-eight 0-Vicryl stitches. The Gould modification is then performed by advancing the inferior extensor retinaculum over the repaired ligaments to provide an additional layer of stability. This completes the nonaugmented Broström procedure. The augmented Broström with InternalBrace involves additional fixation using a 4.75-mm SwiveLock anchor in the talus and a 3.5-mm SwiveLock anchor in the fibula, with FiberTape sutures (Arthrex) tensioned in 10° of plantarflexion. Postoperative protocols vary based on the type of procedure. 17 Patients who underwent standard Broström began weightbearing at 2 weeks in a controlled ankle motion (CAM) boot, progressed to a lace-up brace with proprioceptive therapy at 6 weeks, and returned to impact activities by 4 to 5 months. In contrast, patients who underwent augmented Broström advance faster, with unrestricted therapy by 4 weeks and impact sports allowed by 6 weeks, unless delayed in cases of adjunctive osteochondral defect repair, in which return to impact sports is delayed an additional 3 months.
Results
A total of 97 patients (97 ankles) were included in this analysis. Of 97 patients, 56 (58%) underwent an augmented Broström procedure, and 41 (42%) underwent a Broström procedure without augmentation (Table 1). Augmented Broström was more common in deformity cases (77% of all deformity cases) (P = .02). Other characteristics were balanced (see Table 1). The mean follow-up was 4.4 ± 0.8 years in those who underwent augmented Broström versus 7.2 ± 2.4 years in those who underwent nonaugmented Broström (P < .001).
In unadjusted comparisons, augmented Broström had a higher mean PF (51.2 ± 8.5 vs 48.5 ± 9.4; P = .16) and a lower PI (49.3 ± 9 vs 50.9 ± 10.5; P = .42) compared with nonaugmented Broström (Table 2).
Unadjusted Comparisons of PROMIS Scores a
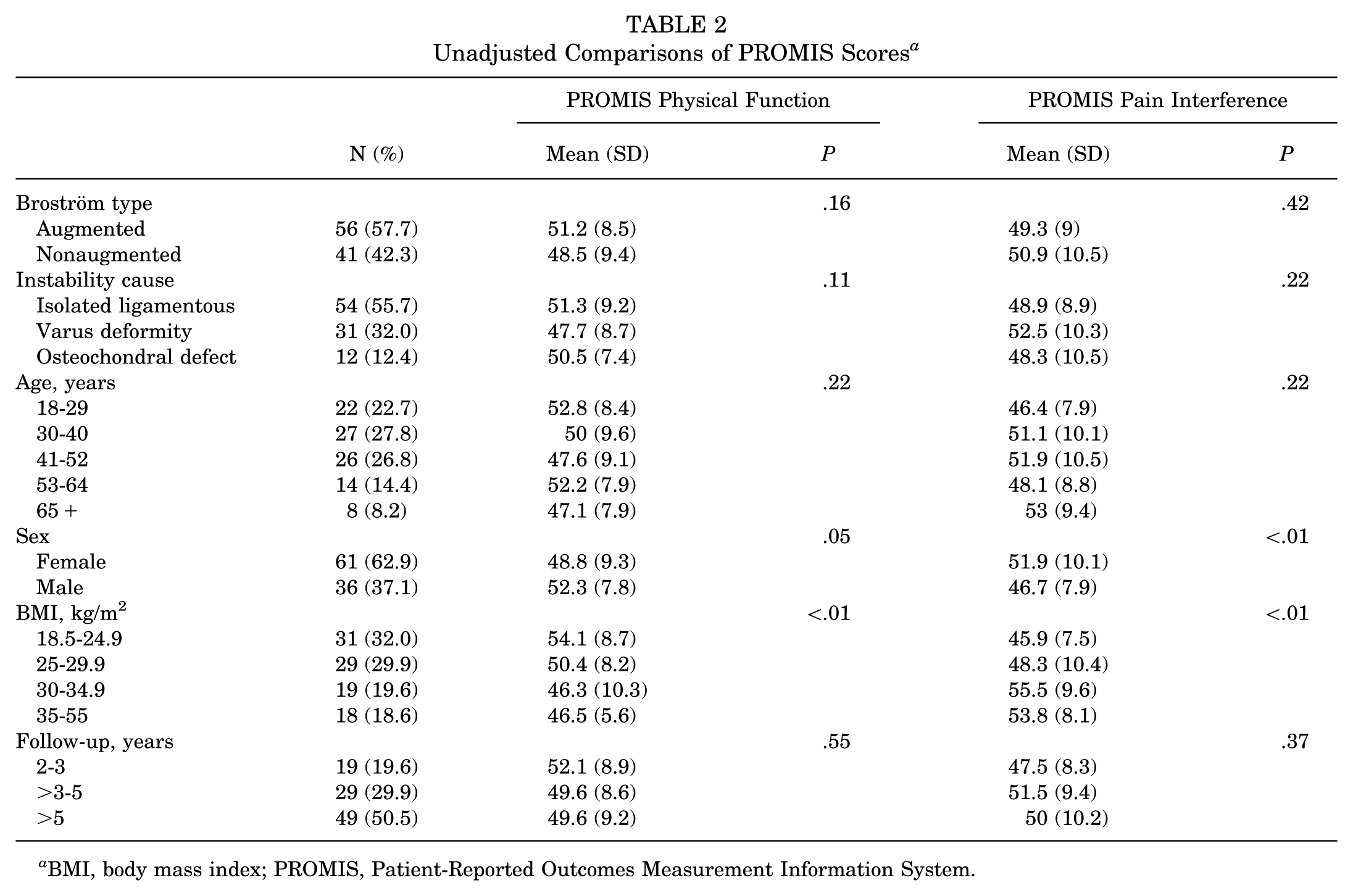
BMI, body mass index; PROMIS, Patient-Reported Outcomes Measurement Information System.
In inverse probability of treatment weighting–adjusted linear regression, augmented Broström was associated with 4.68 (95% CI, 1.27 to 8.09) higher PF (P < .01) and 3.76 (95% CI, −7.85 to 0.33) lower PI (P = .07) compared with nonaugmented Broström (Table 3).
Inverse Probability Weighted Linear Regression a

Bold P values indicate statistical significance. BMI, body mass index; PROMIS, Patient-Reported Outcomes Measurement Information System.
BMI was significantly associated with both PF (P < .01) and PI (P < .01): patients with a BMI >30 kg/m2 (N = 37) had the lowest mean PF and the highest mean PI (Table 2). In weighted regression models (Table 3), BMI was associated with significantly lower PF (Cohen’s d = −0.42 [–0.69 to −0.15]; P < .01) and significantly higher PI (Cohen’s d = 0.50 [95% CI, 0.17 to 82]; P < .01).
Deformity was not associated with significantly lower PROMIS scores in unadjusted comparisons (Table 2). However, in regression models, deformity was associated with significantly worse PF than in those with isolated ligamentous instability, with a PF difference of 4.23 points (95% CI, 8.42 to 0.04). Men had significantly higher PF and lower PI compared with women in unadjusted analysis (Table 2); however, in adjusted models, male sex was no longer associated with significantly higher PF and significantly lower PI (β = 2.48 [95% CI, −0.94 to 5.89]; P = .15 and β = −3.29 [95% CI, −7.48 to 0.9]; P = .12, respectively) (Table 3).
No significant differences in PF or PI were observed at follow-up durations beyond 2 years (P = .55 and P = .37, respectively).
Discussion
The major findings of our study showed that Broström with InternalBrace augmentation was associated with statistically and clinically significant improvements in PROMIS PF compared with nonaugmented Broström (PF, 4.68 points higher; P < .01). Our study also found that augmented Broström was associated with clinically relevant lower PI scores compared with nonaugmented (PI, 3.76 points lower). However, this score did not reach statistical significance (P = .07).
In adjusted models, the mean PROMIS PF with augmented Broström was estimated to be 4.68 points higher compared with nonaugmented Broström, which reaches the minimal clinically important difference (MCID) reported in the literature for PROMIS PF. Augmented Broström also had an estimated PI 3.76 points lower than nonaugmented Broström, which also exceeds the lower end value of the MCID reported in the literature for PROMIS PI.15,27 Broström with InternalBrace augmentation, therefore, may result in clinically important improvements in functional outcomes measured by PROMIS. Consequently, our findings suggest that augmented Broström may be an effective surgical approach for maximizing function and minimizing pain in patients with CLAI, with clinically relevant and statistically significant improvements in PROMIS PF and PI compared with nonaugmented Broström.
We believe that augmentation may generate improved PF and PI compared with nonaugmented Broström because of its ability to restore improved stability to the ankle relative to nonaugmented Broström. Broström repair with InternalBrace augmentation exceeds the native ATFL strength, does not violate normal tissue, and helps protect the ligament repair while it matures, allowing early mobility during recovery and a quicker return to activity.4,10,17
While no studies have compared PROMIS scores between augmented and nonaugmented Broström, a previous study conducted by Scheinberg et al 29 evaluating PROMIS scores after Broström found a mean PF of 50.5 and a mean PI of 48.2, which is consistent with our findings that patients are able to achieve population mean outcomes after Broström. Another study evaluating 80 patients who underwent augmented Broström revealed that patients were able to achieve population mean functional outcomes as measured by PROMIS. 11 In this study, which assessed the influence of fear of reinjury on functional outcomes, those without fear achieved PROMIS scores superior to the population mean. 11 While we do not have preoperative PROMIS baseline scores, these findings suggest that patients with substantial preoperative functional impairment due to CLAI can achieve satisfactory outcomes with augmented Broström compared with the standardized mean score of 50 in the PROMIS framework.
We found that higher BMI was associated with worse PF and PI. These findings corroborate previous literature demonstrating higher BMI as a risk factor for worse outcomes after Broström.6,8 Importantly, BMI does not directly measure obesity, as some patients, such as extremely athletic, heavily muscular patients, may have high BMIs. BMI, therefore, may not be the best measure of obesity, especially in highly athletic individuals. In our general population, not necessarily American football athletes, BMI may be more closely related to obesity than if it had been composed solely of football offensive linemen. Not every patient with a high BMI in our study did poorly, suggesting that some were highly muscular and athletic. Our study ultimately failed to differentiate between these 2 high-BMI populations. Ultimately, further details—such as body fat percentage—when evaluating BMI are needed. We did not have this information available; thus, future investigations should include an assessment of body fat percentage in addition to BMI. It remains unclear whether worse outcomes are driven specifically by obesity and high body fat percentage, or merely by increased load regardless of low fat percentage and high muscle mass.
Those with varus deformities had worse PROMIS scores than those with isolated ligamentous injuries with OCDs. This finding may be attributed to more severe ankle instability preoperatively in patients with deformities, as previous research demonstrates that deformity is a risk factor for worsening CLAI. 24 Previous literature also revealed that among patients with varus deformity specifically, augmented Broström resulted in significantly improved functional outcomes compared with nonaugmented Broström, which may further support augmented Broström as an effective surgical management strategy for severe ankle instability. 12 Future research into strategies to improve outcomes in these patients is still needed.
Limitations
This study has limitations consistent with all studies evaluating PROs. Patients may differ in their interpretation of survey questions, introducing measurement bias. Surgeon preference determined the choice of augmented versus nonaugmented repair, which introduces selection bias, especially because a higher proportion of patients with isolated ligamentous instability received a nonaugmented repair, whereas a higher proportion of patients with varus deformity received an augmented repair. As a result, it remains unclear whether augmentation is better suited to more severe cases of instability, whereas nonaugmented Broström may be reserved for simpler cases. While BMI was higher in the augmented group and associated with significantly worse outcomes, the difference in BMI between groups was not significantly different. Regardless, BMI and instability causes were both accounted for in the statistical model. Despite patients having a minimum 2-year follow-up and no significant differences in PROMIS scores by duration of follow-up beyond 2 years, patients were at different time points postoperatively when responding (not all patients filled out surveys at 2 years postoperatively), which may introduce measurement bias. The augmented group has significantly less follow-up time than the nonaugmented group, because a greater proportion of Broströms procedures at our institution are being performed with augmentation after 2017. Therefore, a longer follow-up time may allow for more recurrent instability, repair degeneration, and long-term complications in the nonaugmented group. However, we found no significant difference in PROMIS scores by duration of follow-up beyond 2 years, suggesting that patients with longer follow-up on average did not experience any further recurrent instability, progressive degenerative changes, or complications that affected function more than those with only 2 years of follow-up. The retrospective design, combined with the lack of preoperative baseline PROMIS scores, also contributes to bias. While patients were indicated for surgery due to CLAI unresponsive to nonoperative treatment and the ankle instability resolved postoperatively, as demonstrated by another study conducted by this investigative team, demonstrating significant improvements in CAIT from pre- to postoperative scores, 10 it remains unclear to what extent patients improved from their functional baseline without preoperative PROMIS scores. Future studies should adopt a prospective approach to compare pre- and postoperative PROMIS scores. Regardless, PROMIS provides meaningful interpretive value even in the absence of an internal control group, as its T-scores are calibrated to a United States population mean score of 50. PROMIS scores, therefore, allow comparison against a validated external reference standard. This framework enables clinically relevant interpretation of patient outcomes, despite the lack of a direct comparison arm with the patients’ preoperative baseline. Of 97 patients, 133 (73%) responded to the survey, potentially introducing response bias. However, this response rate is dramatically higher than that reported in the previous literature evaluating PROMIS after Broström (64/254; 25.2%) in Foot and Ankle Orthopaedics. 29 Finally, postoperative protocols differed by technique, as the augmented repairs returned to weightbearing and high-impact athletic activity sooner than nonaugmented repairs. However, this difference in rehabilitation protocols is inherent to the surgical technique utilized. The augmented repair permits earlier mobilization because of the increased mechanical stability provided by the construct. This inherent difference may partially explain the improved PROMIS scores in the augmented group. To address concerns that accelerated rehabilitation is better, a prospective study by Kulwin et al 18 demonstrated that accelerated rehabilitation negatively affects nonaugmented repair, with fewer returning to preinjury levels of activity with an accelerated rehabilitation compared with those with an augmented repair. 18 Therefore, the difference in rehabilitation proved necessary to protect the function of patients with a nonaugmented repair. 18
Despite these limitations, this study has many strengths. Notably, this study is the first to compare PROMIS between Broström augmented with InternalBrace and Broström without augmentation, and the largest to evaluate PROMIS among Broström techniques. Due to the inconclusive evidence in the literature comparing augmented to nonaugmented Broström, this study provides essential insight into patient functional outcomes after Broström with PROMIS—an outcome metric that demonstrates increased reliability compared with other metrics of functional outcomes previously reported for comparisons between augmented and nonaugmented Broström.
Conclusion
Our study showed that augmented Broström was associated with significantly improved PROMIS scores compared with nonaugmented Broström to a degree that reaches the MCID for PROMIS. Augmented Broström, therefore, may serve as an effective surgical option to maximize functional outcomes for patients suffering from chronic lateral ankle instability.
Footnotes
Acknowledgements
The authors acknowledge Stacy Ngwa for her help with regulatory aspects of the study, including obtaining IRB approval and creating the REDCap.
Final revision submitted January 17, 2026; accepted January 26, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.R.K. has received consulting fees and royalties from Arthrex; and royalties from DePuy Synthes and Elsevier. S.M.H. has received consulting fees from HydroCision, Inc.
Ethical approval for this study was obtained from Northwestern University's Institutional Review Board (STU00210935).