
Abstract
Background:
In patients undergoing medial open-wedge high tibial osteotomy (MOWHTO), the contralateral knee adduction moment (KAM) increases significantly postoperatively, indicating an increased risk of knee osteoarthritis. However, the factors associated with an increased KAM on the nonoperated side remain unexplored.
Purpose:
To identify the factors associated with KAM changes on the nonoperated side before and after MOWHTO.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Thirty participants scheduled to undergo MOWHTO were recruited between August 2020 and November 2022. Physical findings and knee alignment were assessed preoperatively and 1 to 2 years postoperatively with 3-dimensional gait analysis. Gait data were collected with a 3-dimensional motion analysis system and 2 force plates. Multiple regression analysis was performed to identify the factors associated with changes in the first and second KAM peaks on the nonoperated side after MOWHTO.
Results:
The hip adduction moment on the nonoperated side (standard partial regression coefficient [SPRC], 0.45; P = .008; 95% CI, 0.37-2.29) and knee adduction angle on the nonoperated side (SPRC, 0.34; P = .041; 95% CI, 1.66-71.41) were significantly associated with the first KAM peak on the nonoperated side (R2 = 0.31). Hip adduction moment on the nonoperated side (SPRC, 0.56; P = .001; 95% CI, 0.58-1.97) and frontal pelvic obliquity angle (SPRC, 0.32; P = .040; 95% CI, 0.30-12.25) were significant factors associated with the second KAM peak on the nonoperated side (R2 = 0.48).
Conclusion:
Changes in the first and second KAM peaks on the nonoperated side were significantly associated with surrounding alignment and joint moments during gait. In post-MOWHTO gait, controlling the knee adduction angle during the initial stance phase and contralateral pelvic drop during the terminal stance phase may be associated with a reduced risk of KOA development on the nonoperated side.
Medial open-wedge high tibial osteotomy (MOWHTO) is a surgical procedure performed in patients with medial unicompartmental knee osteoarthritis (KOA). This procedure significantly improves dynamic knee joint load and prevents or delays the progression of KOA. 7 However, a notable challenge after MOWHTO is the potential for progressive deformity and increased risk of surgery in the contralateral knee. 14
Knee deformity progresses under excessive external knee adduction moment (KAM) during gait; the risk of progression of KOA increases 6.46 times with a 1% increase in KAM. 23 KAM is correlated with the internal medial contact force and the medial to total contact force ratio. 37 In patients who underwent MOWHTO, the KAM of the nonoperated side significantly increased postoperatively, indicating an increased risk of KOA developing on the nonoperated side after MOWHTO. 20 Avoiding an increase in KAM is crucial for preventing the progression of KOA on the nonoperated side. Therefore, it is critical to understand the factors that contribute to increased KAM.
KAM is generally associated with the movements of the foot, hip, pelvis, and trunk. In healthy individuals and patients with KOA, previous studies have revealed the relationship between KAM and the kinetics and kinematics of other regions, including pelvic obliquity angle9,11 and external hip adduction moment (HAM). 1 Dunphy et al 11 reported that changes in frontal plane hip motion and pelvic drop were highly correlated with changes in KAM. Abdallah and Radwan 1 demonstrated a significant positive correlation between HAM and KAM during gait, which was likely attributable to the ground-reaction force (GRF) passing medial to the axes of both joints. Previous studies have also reported this relationship in trunk bending angle,29,35 foot progression angle (toe-in or toe-out),10,21,35 and external ankle eversion moment.1,36 While one study indicated increases in KAM with fatigue, 34 other studies found no significant correlation between hip abductor strength and KAM.18,19,32 In patients undergoing MOWHTO, the causal relationship between KAM and its kinetics and kinematics remains unclear.
The purpose of this study was to identify the factors associated with changes in KAM on the nonoperated side before and after MOWHTO to prevent KOA progression on the nonoperated side after MOWHTO. We hypothesized that the pelvic obliquity angle and HAM during gait are associated with KAM on the nonoperated side.
Methods
This longitudinal cohort study was conducted at the authors’ affiliated hospital and was approved by the Medical Research Ethics Committee. All participants provided written informed consent before participation. Measurements were conducted preoperatively and 1 to 2 years postoperatively.
Participants
We recruited Japanese participants aged ≥40 years who were scheduled to undergo MOWHTO between August 2020 and November 2022. The participants were diagnosed with KOA per the American College of Rheumatology clinical criteria. 4 The exclusion criteria were as follows: history of trunk or lower extremity surgery or orthopaedic problems, apparent fractures of the subchondral bone, diagnosis of posttraumatic KOA, and chest pain resulting from cardiac disease. Additionally, participants were excluded owing to refusal, human and capacity constraints, or fall on the day before measurement. The participants were recruited through posters placed in the hospital. Thirty participants were included in the study after the application of inclusion and exclusion criteria (Figure 1).
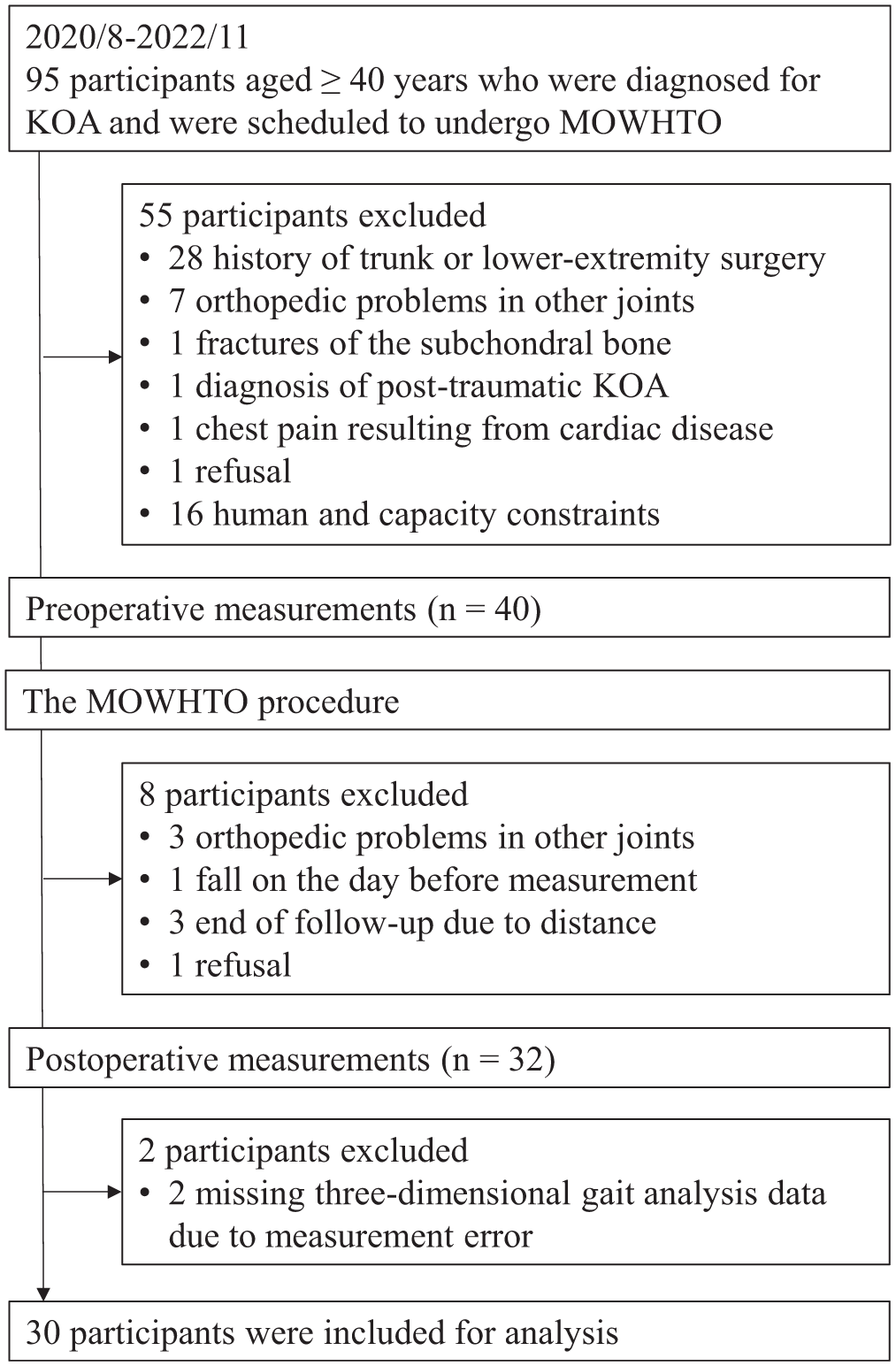
CONSORT flow diagram for participant selection. KOA, knee osteoarthritis; MOWHTO, medial open-wedge high tibial osteotomy.
Surgical Procedure and Rehabilitation
The MOWHTO procedure followed the Staubli method. 33 Preoperatively, the mechanical axis was shifted laterally to the 57% point on the tibial plateau's transverse diameter, and the opening width was measured on the radiograph of the standing full-length view of the lower limbs. During surgery, the osteotomy site was opened to the planned width, and limb alignment was monitored fluoroscopically to control the knee position of the alignment rod. Wedge-shaped beta-tricalcium phosphate grafts were then inserted. The open osteotomy site was fixed with locking screws with a TriS plate (TriS Medial HTO Plate System; Olympus Terumo Biomaterials). All surgeons were board-certified orthopaedic specialists with >10 years of experience in knee surgery. All procedures were performed under the supervision of 1 surgeon with >20 years of experience.
Postoperative rehabilitation consisted of range of motion and quadriceps, gluteus maximus, and gluteus medius exercises for 40 minutes a day. These exercises started on day 1 after the operation and were performed 5 days a week during hospitalization. Weightbearing progressed as follows: one-third on day 2, two-thirds on day 7, and full weightbearing on day 14, all with crutches. Upon discharge, participants continued independent training, supervised by a physical therapist at the outpatient clinic.
Pain and Physical Measurements
Knee pain during gait was assessed by the visual analog scale.2,15 The reliability of this method in participants with KOA was reported as an intraclass correlation coefficient (ICC) of 0.97. 15
Knee joint flexion and extension angles were measured by 2 physical therapists using a goniometer, as reported in previous studies. 8 Angles were measured in 1º increments. One measurement was adopted as the representative value. Measurement reliability was reported as an ICC between 0.97 and 0.99. 8
Knee extension and hip extension and abduction muscle strength were measured twice by 2 physical therapists using a handheld dynamometer (μ-Tas F1; Anima) with a belt, as reported in previous studies. 17 All tests involved maximal voluntary isometric contraction. The mean value was used as the representative value. Muscle strength was normalized by leg length and body weight (newton-meters/kilogram).24,27 The reliability of this method was reported as an ICC between 0.98 and 0.99. 17
In the 10-m walk test, speed and step length in a comfortable gait were measured twice with a stopwatch, and the mean values were adopted as representative values. The measurement was recorded from the first step past the starting point to the first step past the finishing point. The reliability of this method was reported as an ICC between 0.96 and 0.98. 28
Knee Alignment
The Kellgren-Lawrence grade, percentage of mechanical axis, mechanical axis length, hip-knee-ankle angle, and medial proximal tibial angle were measured by 2 board-certified orthopaedic surgeons using radiographs of the standing full-length view of the lower limbs by a software system (mediCAD Classic; Toyo Corporation). Percentage of mechanical axis was defined as the position at which the line connecting the center of the femoral head to the center of the ankle crosses the tibial plateau, expressed as the percentage of the total tibial plateau width. Mechanical axis length was the straight-line distance measured from the center of the femoral head to the center of the ankle joint. Hip-knee-ankle angle was the angle formed by the femoral mechanical axis (from the femoral head center to the intercondylar notch) and the tibial mechanical axis (from the tibial interspinous point to the ankle center). Medial proximal tibial angle was the medial angle formed by the tibial mechanical axis and the proximal tibial joint orientation line. The reliability of the method for this system was reported as an ICC between 0.89 and 0.99.25,31
Three-dimensional Gait Analysis
Three-dimensional gait analysis was performed as previously described. 26 All participants were dressed in prepared athletic attire, comprising a spandex shirt and shorts, and were barefoot. Measurements were taken by a 3-dimensional motion analysis system (Motive; Acuity) with 8 cameras operating at a sampling rate of 100 Hz and 2 force plates (TF-4060; Tech Gihan) placed side-by-side on the ground at a sampling rate of 1000 Hz. This 3-dimensional motion analysis system demonstrated high accuracy in a previous study. 5 Forty infrared reflective markers (9-mm spheres) were attached to various anatomic locations using the Plug-in-Gait full-body model (Oxford Metrics LTD). The participants walked at a comfortable speed. Successful measurements were obtained when the participant's foot was placed on the surface of the force plate. The 3-dimensional and ground-reaction data were smoothed by a second-order Butterworth low-pass filter with a cutoff frequency of 10 Hz and then imported into the SKYCOM software (Acuity).
The knee flexion excursion was calculated by subtracting the knee flexion angle at initial contact from the peak knee flexion angle during the stance phase. The lateral trunk bending angle was calculated as the angle relative to the pelvis and was defined as positive for lateral bending toward the operated side and negative for lateral bending toward the nonoperated side. The frontal pelvic obliquity angle represents an absolute angle in space and was defined as positive for pelvic drop on the operated side and negative for pelvic drop on the nonoperated side. Joint moments represent external joint moments and were normalized to body weight and height (percentage body weight × height). A stance phase was identified from heel contact to toe-off, and these gait events were determined with a 10-N threshold on the vertical GRF. 16 All kinematic and kinetic variables for each participant represented 1 successfully measured trial. The GRF, lower limb joint angles and moments, and pelvic and trunk tilt angles at the first and second KAM peaks on the nonoperated side were extracted.
Statistical Analysis
Participant demographics are presented by descriptive statistics. The normality of the data was confirmed with a histogram and the Shapiro-Wilk test. Pre- and postoperative outcomes were compared. Pain and muscle strength were analyzed by Wilcoxon signed rank tests, and other outcomes were analyzed by paired t tests. P values were adjusted by the Bonferroni correction with a corrected significance level of P < .0016 (0.05/30). The changes in muscle strength, walking speed, step length, and GRF, as well as the changes in pain, joint angles, and joint moments, were calculated. The postoperative value was expressed as a percentage relative to the preoperative value: (postoperative value / preoperative value) × 100. Additionally, the absolute change was calculated as the difference between these time points (postoperative value − preoperative value). Correlation coefficients were determined between the pre- and postoperative changes in each item and the changes in the first and second KAM peaks on the nonoperated side. Independent variables (P value up to .1) were included in further multiple regression analysis. 6 Multiple regression analysis using a forward-backward stepwise method was performed to assess the effect of independent variables on KAM on the nonoperated side. All statistical analyses were performed in SPSS 23.0 (IBM Corp). The significance level was set at 5%. The number of participants required to test the hypotheses was also calculated. A priori sample size calculation was performed in G* Power software 3.1.9.7. 12 Based on a previous study 20 that analyzed KAM during gait, the minimum number of participants required was 18 (2-tailed effect size, 0.74; alpha error, .05; power, 0.80). Based on a previous study 3 predicting KAM on the nonoperated side, a sample size of 49 participants was required if a multiple regression model with 5 predictors were to be used (effect size, 0.30; alpha error, .05; power, 0.80).
Results
Of the 30 participants, 10 were men and 20 were women. The mean ± SD age was 58.10 ± 8.54 years with a mean height of 1.62 ± 0.07 m and weight of 65.83 ± 9.77 kg. Fourteen participants underwent surgery on the right knee and 16 on the left knee. Kellgren-Lawrence grades on the operated side were as follows: 0 (n = 0), I (n = 10), II (n = 8), III (n = 9), and IV (n = 3). On the nonoperated side, Kellgren-Lawrence grade distribution was as follows: 0 (n = 4), I (n = 12), II (n = 6), III (n = 7), and IV (n = 1).
Pain and physical findings showed significant postoperative increases in hip abductor and adductor muscle strength on the operated and nonoperated sides, gait speed, and step length (Table 1). Knee alignment assessment on the operated side showed a significant postoperative increase in percentage of mechanical axis, mechanical axis length, hip-knee-ankle angle, and medial proximal tibial angle.
Pre- and Postoperative Comparison of Pain During Gait, Physical Findings, and Knee Alignment a

Values are presented as mean ± SD or median (IQR). HKA, hip-knee-ankle angle; %MA, percentage of mechanical axis; MAL, mechanical axis length; MPTA, medial proximal tibial angle; VAS, visual analog scale.
P < .05.
P < .0016 (Bonferroni correction).
During comfortable walking, the first and second KAM peaks on the operated side significantly decreased postoperatively. On the nonoperated side, the first and second KAM peaks significantly increased postoperatively (Table 2, Figure 2). The knee extension angle in terminal stance on the operated side significantly increased postoperatively. Figure 2 shows mean and SD data throughout the stance phase of the gait cycle.
Pre- and Postoperative Comparison of the 3-dimensional Gait Analysis a

Values are presented as the mean ± SD. BW, body weight; Ht, height; KAM, knee adduction moment.
P < .05.
P < .0016 (Bonferroni correction).

Pre- and postoperative KAM throughout the stance phase of the gait cycle and knee flexion angle throughout the gait cycle. (A, C) Operated- and nonoperated-side KAM throughout the stance phase of the gait cycle. (B, D) Operated- and nonoperated-side knee flexion angle throughout the gait cycle. BW, body weight; Ht, height; KAM, knee adduction moment.
Changes in the first KAM peak on the nonoperated side were positively correlated with changes in HAM on the nonoperated side. They negatively correlated with changes in hip abductor muscle strength on the operated and nonoperated sides and ankle eversion moment on the nonoperated side. Changes in the second KAM peak on the nonoperated side were positively correlated with changes in HAM on the nonoperated side and frontal pelvic obliquity. Furthermore, they negatively correlated with changes in hip abductor muscle strength on the nonoperated side (Table 3).
Correlation Between Changes in KAM on the Nonoperated Side and Changes in Each Parameter a

Bold indicates P < .05. AEM, ankle eversion moment; GRF, grand reaction force; HAM, hip adduction moment; KAM, knee adduction moment; VAS, visual analog scale.
The changes in muscle strength, walking speed, step length, and GRF, as well as pain, joint angles, and joint moments, are presented as the mean change or the mean percentage of the postoperative value relative to the preoperative value.
The values in the 3-dimensional gait analysis are presented for the first / second peaks of KAM.
Stepwise multiple regression analysis was performed to identify factors associated with changes in the first KAM peak on the nonoperated side using 5 independent variables: hip abductor muscle strength on the operated and nonoperated sides, HAM on the nonoperated side, knee adduction angle on the nonoperated side, and ankle eversion moment on the nonoperated side. The analysis revealed that HAM (standard partial regression coefficient [SPRC], 0.45; P = .008; 95% CI, 0.37-2.29) and knee adduction angle on the nonoperated side (SPRC, 0.34; P = .041; 95% CI, 1.66-71.41) were significant factors associated with the first KAM peak on the nonoperated side (coefficient of determination; R2 = 0.31). The Durbin-Watson statistic was 2.15, and no outliers >3 SD from the measured values were observed. Factors related to changes in the second KAM peak on the nonoperated side were identified through stepwise multiple regression analysis with 4 independent variables: hip abductor muscle strength on the operated and nonoperated sides, HAM on the nonoperated side, and frontal pelvic obliquity angle. The analysis revealed that HAM on the nonoperated side (SPRC, 0.56; P = .001; 95% CI, 0.58-1.97) and frontal pelvic obliquity angle (SPRC, 0.32; P = .040; 95% CI, 0.30-12.25) were significant factors associated with the second KAM peak on the nonoperated side (R2 = 0.48). The Durbin-Watson statistic was 1.91, and no outliers >3 SD from the measured values were observed.
Discussion
The results of this study showed that the first and second KAM peaks decreased on the operated side postoperatively but increased on the nonoperated side. Changes in the first KAM peak on the nonoperated side were associated with the HAM and knee adduction angle on the nonoperated side during gait. Changes in the second KAM peak on the nonoperated side were associated with the HAM on the nonoperated side and frontal pelvic obliquity angle during gait. This study supports the hypothesis that the pelvic obliquity angle and HAM are associated with changes in KAM on the nonoperated side.
Lind et al 20 reported an increase in the first KAM peak on the nonoperated side after MOWHTO but no change in the second KAM peak. They mentioned that the small sample size of 11 participants was a limitation of the study that could have compromised the generalizability of the results. Our study of 30 participants revealed that the first and second KAM peaks on the nonoperated side significantly increased postoperatively. These results indicate increased mechanical stress on the nonoperated side after MOWHTO.
Changes in the first KAM peak on the nonoperated side were associated with changes in the HAM and knee adduction angle on the nonoperated side during gait. Previous studies in patients with KOA have reported the following. (1) The first KAM peak and HAM were positively correlated (r = 0.268). This might be attributed to their occurrence at almost the same time as GRF located medial to the axes of both joints. 1 (2) The first KAM peak and knee adduction angle were positively correlated (r = 0.762). An increase in the knee adduction angle during gait led to an increase in the first KAM peak. The knee adduction angle predicted 58% of the variance in the first KAM peak. 30 Our study demonstrated similar results in the nonoperated side after MOWHTO. It is possible that avoiding an increase in HAM and/or knee adduction angle is important for preventing an increase in KAM during the early stance phase.
Changes in the second KAM peak on the nonoperated side were associated with changes in the HAM on the nonoperated side and the pelvic drop angle on the swing leg side during gait. Although hip abductor weakness may increase medial compartment loading, 9 no studies have directly examined the relationship between the second KAM peak and HAM. In healthy individuals, the KAM peak (r = 0.88) and impulse of KAM (r = 0.86) were positively correlated with the pelvic drop angle on the swing leg side. However, these participants were asymptomatic and practiced as many times as required to re-create the unilateral pelvic drop gait pattern during ground walking before measurement. 11 We found no studies that directly addressed the relationship between the second KAM peak and the frontal pelvic obliquity angle. The present study yielded similar results for the second KAM peak. It is conceivable that preventing an increase in HAM on the nonoperated side and/or the contralateral pelvic drop angle plays a crucial role in mitigating increases in KAM during the late stance phase.
Regarding whether factors in the operated or nonoperated limb influence the KAM on the nonoperated side after knee surgery, previous studies on total knee arthroplasty (TKA) have provided valuable insights. Increased KAM, indicative of increased joint loading, is a recognized risk factor for primary osteoarthritis progression, and reduced knee flexion excursion is a risk factor for future TKA. 3 Furthermore, gait patterns after TKA do not return to normal; patients continue to walk with flexed-knee gait patterns and attenuated sagittal plane motion on the operated side. 22 In the present study, knee flexion excursion on the operated side did not decrease after MOWHTO. Thus, unlike TKA, MOWHTO did not result in flexed knee gait patterns with attenuated sagittal plane motion on the operating side. However, KAM on the nonoperated side increased after MOWHTO. The first and second KAM peaks on the nonoperated side were affected by the variables on the nonoperated side.
Since this was an observational study, causality could not be established. However, our findings suggest that HAM on the nonoperated side, knee adduction angle on the nonoperated side, and frontal pelvic obliquity angle may contribute to increased KAM on the nonoperated side. Therefore, focus on the nonoperated side after MOWHTO may be important. In patients with KOA, a previous study reported that the use of lateral-wedge insoles reduces knee adduction angle and KAM on the affected side. 13 Similarly, a study in healthy individuals reported that hip abductor fatigue leads to decreased strength and increased KAM. 34 In the future, we aim to conduct an intervention study to enhance the efficacy of post-MOWHO physical therapy.
This study had several limitations. The larger sample size of 30 resulted in different outcomes on the nonoperated side before and after MOWHTO as compared with those reported previously. 20 However, the sample size should be enhanced to make sounder inferences based on multiple regression. Based on the sample size calculation, the statistical power of this analysis was limited. Our study included a slightly larger number of women than men. It is unclear whether the results are similar for men and women, as we did not conduct a sex-specific analysis. Muscle strength was measured by isometric contraction and open kinetic chain situation, which may differ from muscle activity by eccentric contraction and closed kinetic chain situation while walking. Furthermore, trunk muscle strength was not measured, preventing evaluation of whether trunk muscles were associated with pelvic drop. This study did not investigate rotation of the lower limbs, pelvis, and trunk. How hip rotator muscles, such as the obturator muscles, are associated with the pelvic segment needs to be clarified in future research. In a previous study, the pelvic drop angle was determined by calculating the change in the vector bisecting the bilateral anterior superior iliac spines with respect to the vertical vector in the anatomical standing position. 11 Yet, in this study, the lateral trunk bending angle was calculated as the angle relative to the pelvis, and the frontal pelvic obliquity angle represented an absolute angle in space, which differed from the previous measurement method. Given the lack of specifications regarding independent training after discharge and joint loading during the follow-up period, it remains unclear whether there was any subject bias.
Conclusion
Changes in the first and second KAM peaks on the nonoperated side were significantly associated with surrounding alignment and joint moments. In post-MOWHTO gait, controlling knee adduction angle during the initial stance phase and contralateral pelvic drop during the terminal stance phase may help reduce the risk of KOA development on the nonoperated side. Research on rehabilitation is insufficient, and further interventional studies are warranted.
Footnotes
Acknowledgements
The authors thank the members of their institution for assistance and Editage for English-language editing.
Final revision submitted December 29, 2025; accepted January 4, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by JSPS KAKENHI (grants 21K11309 and 24K12425). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Medial Research Ethics Committee of the Institute of Science Tokyo (M2019-195-02).