
Abstract
Background:
Functional outcomes and patient characteristics of knee and hip osteoarthritis (OA) have been described in general populations; however, this has yet to be investigated in former professional American-style football (ASF) players.
Purpose:
To explore ASF exposures, previous injuries, health factors, and radiographs in order to understand contributions to function using the Knee injury and Osteoarthritis Outcome Score (KOOS) and Hip Disability and Osteoarthritis Outcome Score (HOOS) in former ASF players.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Living former ASF players who participated in ASF between 1960 and 2022 were identified through the NFL Players Association and invited to participate in the study. Enrolled participants were selectively recruited by condition (cardiometabolic disease, chronic pain, neurocognitive impairment, or sleep apnea) and completed the KOOS, HOOS, and a survey on comorbidities, previous injuries, and ASF exposures. Weightbearing radiographs were obtained for hips and knees for radiographic severity. Backward stepwise linear regression examined the association between KOOS or HOOS subscales and function, reported health, and ASF characteristics, and results were weighted for selection effects.
Results:
Most former ASF players (n = 90; age, 48.3 ± 7.7 years; Black, 55.6%) had evidence of knee (n = 89; 89.9%) or hip (n = 95; 95.9%) OA. Higher pain severity, higher body mass index (BMI), prior anterior cruciate ligament (ACL) surgery, and greater radiographic severity were associated with lower KOOS values corresponding to worse knee functional outcomes. Higher HOOS values indicating better hip function were associated with meeting physical activity standards and longer professional careers, but there was no association with radiographic severity.
Conclusion:
Variability was found within HOOS and KOOS measures. Radiographic findings appeared to correspond with functional status in former ASF players with knee OA but not hip OA. Higher BMI and pain severity were associated with worse function in knee OA, and ACL surgery was associated with worse function in symptom severity and sports function on KOOS. These findings may contribute to obtaining functional measures, history, and radiographs to evaluate limitations associated with knee and hip OA in this population.
Keywords
Osteoarthritis (OA) is a common condition characterized by joint pain and stiffness, resulting in impaired function.32,54 The knee and hip are among the most common locations and contribute to global disability,10,54 affecting up to 300 million people worldwide.15,53 In the United States, the age-standardized prevalence is 23.2%. 53 However, the prevalence data are derived from surveys of radiographic findings and may miss early stages of OA when symptoms develop before imaging changes.10,42 Additionally, multiple OA phenotypes exist outside of traditional age-related primary OA.12,48 Posttraumatic OA (PTOA) resulting from joint trauma and injuries such as anterior cruciate ligament (ACL) injury is common in athletes, 61 with 50% to 90% of ACL tears progressing to PTOA. 33 Previous literature has described a higher prevalence of knee and hip OA in former athletes compared with the general population, including at younger ages.17,44 Although American-style football (ASF) is a collision sport, studies describing the prevalence of arthritis in former ASF players are limited. 18 In a population of 2864 former ASF players, arthritis was more prevalent across ages when compared with the general population, affecting 22% of 25- to 29-year-olds and more than half of those age 50 to 59 years. 18 Advanced OA may result in patients being indicated for arthroplasty, and in a population of 3913 former ASF players, 12.3% and 8.1% reported total knee or hip arthroplasty by a mean age of 53 years. 58
The high prevalence of knee and hip OA in former ASF players supports the need to understand factors associated with this condition, including those specific to physical demands of ASF play. In the general population, identified risk factors for OA include sex, race, advanced age, genetics, higher body mass index (BMI), and physical inactivity.42,47,49,60 Anatomic and biopsychosocial factors such as anxiety, depression, and pain sensitization may also contribute to the onset of OA.14,23,37,39,50,60 In contrast, features associated with or contributing to knee and hip OA are not well characterized in former ASF players. Although ACL injuries and concomitant meniscal tears have been suggested to lead to cartilage damage associated with progression to PTOA in active populations,33,40 the limited work in former ASF players has identified joint injuries, including ACL tears, and higher BMI as possible contributors to knee OA.16,34 Research is limited in identifying factors associated with symptomatic hip OA in this population. One study reported older age, lineman position, and previous hip injury as risk factors for hip arthroplasty in former NFL players, 11 but to our knowledge, no current studies have investigated factors associated with hip OA alone.
The standard method to detect knee and hip OA is through combined history and physical examination, with weightbearing radiographs commonly obtained to evaluate radiographic severity. However, radiographic findings may not correspond to symptoms in OA.28,29 Patient-reported outcome measures may be used to characterize the functional limitations resulting from knee and hip OA and to evaluate changes over time. Common measures of function for individuals with knee and hip OA include the Knee injury and Osteoarthritis Outcome Score (KOOS) and Hip Disability and Osteoarthritis Outcome Score (HOOS).4,41,51 Although previous studies in formers professional ASF players have used other subjective outcome measures when assessing physical function and musculoskeletal history, including the Short Form-36 Measurement Model for Functional Assessment of Health and Well-Being (SF-36) 27 and Patient Reported Outcomes Measurement Information System (PROMIS) physical scales, 59 we are unaware of any studies that have used arthritis-specific outcome measures to assess knee and hip function in this population.
The primary purpose of this study was to explore how sports participation characteristics, previous injuries, current health, and radiographs were correlated with the KOOS and HOOS in this population of former ASF players. We hypothesized that aspects of ASF play, such as longer career duration and previous ACL injury, would be associated with worse outcomes using KOOS and HOOS. A secondary purpose was to assess the association of radiographic severity of OA with pain and function as measured by KOOS and HOOS. We hypothesized that former players with greater radiographic severity in the knee or hip would report higher levels of pain and worse function.
Methods
Participants
This research is part of the Football Players Health Study at Harvard University (FPHS), an ongoing study evaluating health outcomes in living former ASF players. Recruitment methods for FPHS have been described in previous literature. 63 Briefly, living former ASF players who participated in ASF between 1960 and 2022 were identified through the NFL Players Association and invited to enroll via emailed and hardcopy invitations. 63 Survey completers were screened for eligibility to participate in a 3-day in-person assessment (IPA), which ended in 2022. 8 This sample was a subset of the larger pool of former ASF players specifically selected to have equal representation of Black and White players. Enrolled former ASF players completed a questionnaire before IPA participation. Participants were recruited to participate in the IPA on the basis of whether they met criteria of self-reported questionnaire responses for 0, 1, or >2 affliction states (cardiometabolic disease, chronic pain, neurocognitive impairment, and sleep apnea) within the specified current age range of 28 to 55 years at the time of enrollment into the larger cohort, such that all participants would be between 30 and 60 years of age at the time of assessment. The study was approved by the Harvard T.H. Chan School of Public Health (No. 2018P001929), and participants provided written informed consent in accordance with institutional policies.
Health Questionnaire
All eligible former ASF players were sent a survey on health status, current function, and football exposure using available contact information. Demographic data included age and race as defined in a previous publication. 13 The questionnaire contained items related to position, years of play, and surgeries during active playing years, including ACL reconstruction. Players were asked the following: (a) “How many seasons did you actively play professional football?” (b) “What was the last calendar year that you played professional football?” (c) “Select the positions that you most often played during your professional football career from the following: offensive line, defensive line, linebacker, defensive back, running back, wide receiver, tight end, quarterback, kicker/punter, special teams.” Player position was categorized as lineman (defensive line, linebacker, and offensive line) or nonlineman. (d) “Has a healthcare provider ever told you that you have arthritis?” (e) “During your active playing years, did you have ACL reconstruction?”
In-person Assessment
At the time of participation in the IPA, 8 additional surveys were collected including current pain severity based on a continuous numeric pain rating scale, where 0 = no pain and 10 = worst pain imaginable, and level of physical activity as measured by the International Physical Activity Questionnaire (IPAQ) 9 to capture current level of function. 8 This was assessed as a categorical variable as having met or not met physical activity standards. Each participant also completed the KOOS and HOOS. The KOOS and HOOS contain items used to generate scores for 5 subscales: Pain, Symptoms, Activities of Daily Living (ADLs), Sport, and Quality of Life (QOL). The Sport subscale measures the ability to perform more physically demanding activities such as squatting, running, twisting, or kneeling. This domain captures the functional challenges that go beyond basic daily living and is especially relevant for active individuals or former athletes. Development and details of each subscale have been previously described. 52 Responses to each item are based on a Likert scale of 5 choices ranging from no problems (0) to extreme problems (4). Scores are transformed to a 0 to 100 scale, with zero representing extreme hip or knee problems and 100 representing no hip or knee problems. 51 Both have demonstrated good psychometric properties for knee and hip pain and function associated with OA as well as joint injury including ACL and joint replacement.6,41,43,51
Height and weight were obtained to calculate BMI. Each participant completed early-onset scoliosis (EOS) radiographs that captured both hips and knees. EOS is a biplane radiographic imaging system manufactured by EOS Imaging (formerly Biospace Med) that is conducted in a weightbearing position and uses less radiation than standard imaging techniques. 35 EOS was selected over traditional knee and hip radiographs to allow for measuring joints with weightbearing while reducing total ionizing radiation. Before scans were analyzed, an internal review was performed between radiologists and a physician specializing in orthopaedics to ensure good agreement. Each EOS scan was reviewed by a physician with extensive experience in management of OA 8 and was graded 0 to 3 for both knees and hips; grade 0 indicated no arthritis; grade 1, mild arthritis; grade 2, moderate arthritis; and grade 3, severe OA. A separate composite score for the hip and for the knee was recorded to score radiographic severity of OA.
Responses from the survey, KOOS and HOOS results, and EOS scans were collected and tabulated using REDCap for online surveys or Scantron for paper surveys. 58
Statistical Analyses
Means (with standard deviations) and frequencies (with percentages) were used to describe continuous and categorical variables, respectively. To address bias that may have occurred due to the health-based selection criteria for the in-person study, we calculated stabilized inverse probability weights for inclusion, which were applied in multivariable regression models (Appendix Tables A1-A3).5,21,22 Backward stepwise linear regression was used to identify variables associated with each KOOS and HOOS subscale score (Pain, Symptoms, ADL, Sport, QOL) out of the following candidate variables: age, race, current BMI, lineman status, career duration, meeting physical activity standards, pain severity (excluding Pain subscale), previous ACL surgery (KOOS models only), and knee and hip radiographs. White players, nonlinemen, participants with career durations <3 years, participants not meeting physical activity standards, participants with ACL surgery, and participants with no OA served as reference groups in analytical models. Age and BMI were scaled and are reported in units of standard deviation. At each step, variables were chosen based on the Akaike information criterion (AIC), which was used to set a limit on the total number of variables included in the model. The least significant variable was iteratively removed at each step, and the model with the lowest AIC value was considered the best fit model for each subscale. Results are reported as beta estimates in units of the scale score and 95% CIs. All statistical modeling was conducted using R Language for Statistical Computing, 46 with significance defined as P < .05.
Results
Among the 3099 former ASF players who completed the enrollment survey at the start of the IPA, 1161 (37.5%) were eligible to participate in the in-person study. Among this group, 254 received an invitation via phone call, among whom 147 (57.9%) agreed to be screened and 111 (43.7%) opted to participate in the IPA. Of this group, 3 people were excluded because of missing HOOS or KOOS values and 4 because of missing physical activity standards (n = 4). Additionally, we excluded participants with total hip (n = 4) or knee arthroplasty (n = 5) because this would influence composite scores or joint function. This resulted in a cohort of 95 former ASF players included in the final analysis (Figure 1).
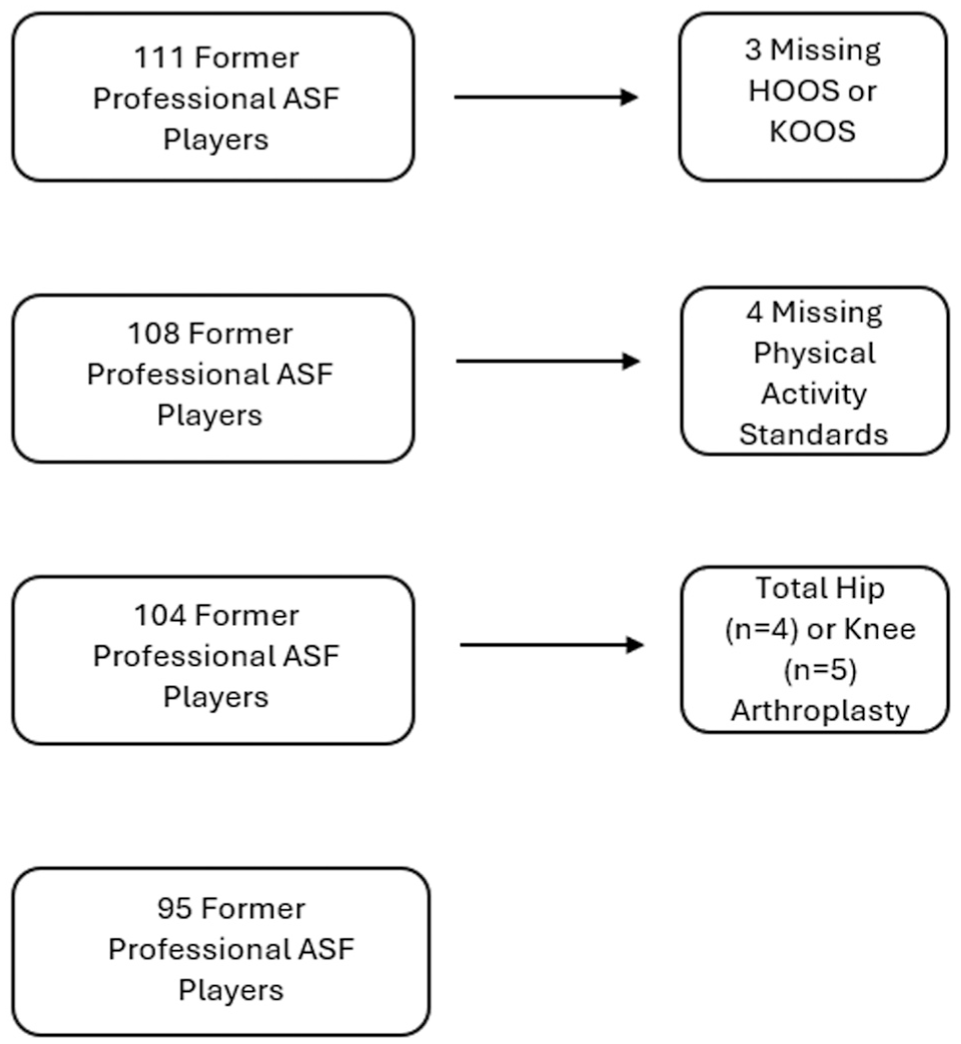
Inclusion flow chart. Participants were excluded if they were missing HOOS or KOOS values, were missing physical activity standards, or had undergone a total hip or knee arthroplasty. ASF, American-style football; HOOS, Hip Disability and Osteoarthritis Outcome Score; KOOS, Knee injury and Osteoarthritis Outcome Score.
Participant Characteristics
In the unweighted population of 95 former ASF players, participants were on average in the fourth decade of life. Half identified as Black, the mean BMI was >30, and half reported primary position as lineman and a mean career duration of 5 years (Table 1).
Descriptive Characteristics of Former American-Style Football Players a

ACLR, anterior cruciate ligament reconstruction; OA, osteoarthritis.
Within our sample recruited by health status (Appendix Table A1), 8 although not all players had OA, the majority of players had radiographic evidence of knee (89%) or hip (96%) OA (Table 1). Within the population who sustained an ACL injury and had surgical repair during their playing years (n = 17), 15 had mild or moderate knee OA and 2 had severe knee OA of affected joint (Figure 2).
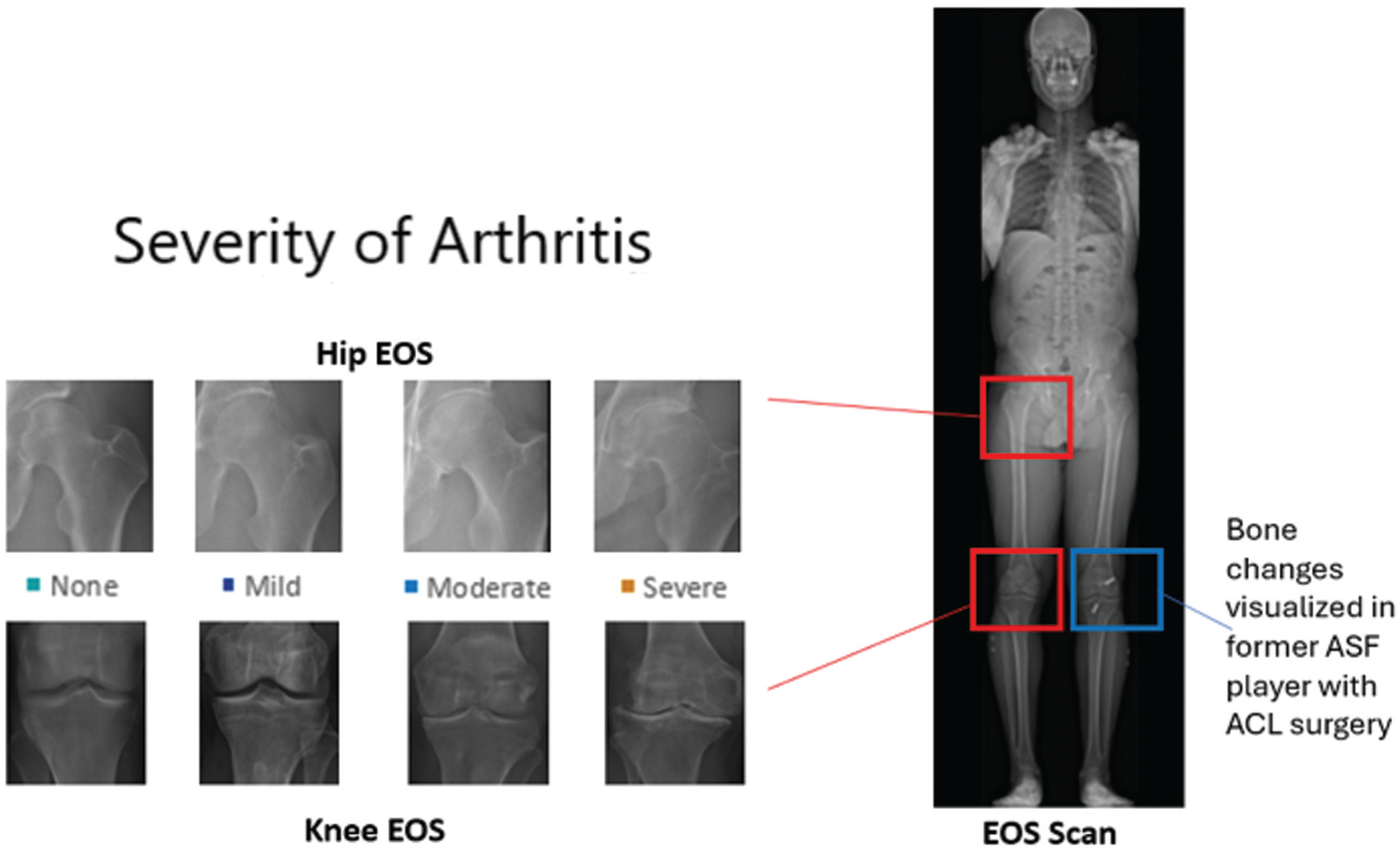
Radiographic evidence of hip or knee osteoarthritis in former professional American-style football (ASF) players. Radiographic severity for each knee and hip was graded as none, mild, moderate, or severe in each player using early-onset scoliosis (EOS) scan that captured each joint in weightbearing status. ACL, anterior cruciate ligament.
Factors Associated With KOOS
The mean KOOS subscale scores ranged 58 to 76 (Figure 3). In weighted backward selection regression models, greater pain severity was associated with greater symptom severity (KOOS Symptoms score: β estimate = −4.00; 95% CI, −5.56 to −2.44), reduced ADL (KOOS ADL score: β estimate = −4.94; 95% CI, −6.34 to −3.54), lower sport function (KOOS Sport score: β estimate = −5.99; 95% CI, −8.15 to −3.84), and reduced QOL (KOOS QOL score: β estimate = −6.09; 95% CI, −8.17 to −4.00). Higher BMI was associated with worse ADL (KOOS ADL score: β estimate = −6.60; 95% CI, −11.10 to −2.13) and lower sport function (KOOS Sport score: β estimate = −8.37; 95% CI, −14.8 to −1.97) (Figure 4).
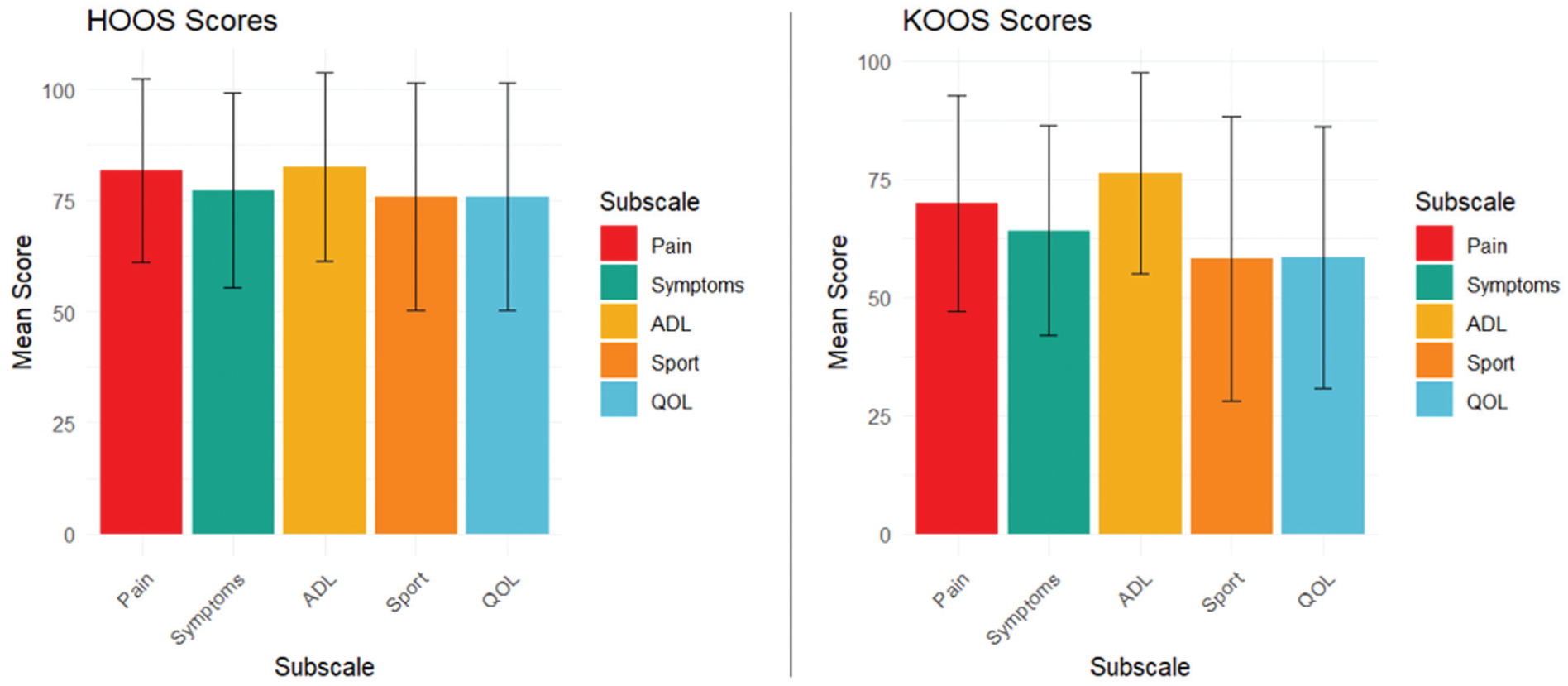
Hip Disability and Osteoarthritis Outcome Score (HOOS) and Knee injury and Osteoarthritis Outcome Score (KOOS) in former professional American-style football (ASF) players with knee and hip osteoarthritis. Unweighted KOOS and HOOS mean values with standard deviation bars are presented to illustrate level of pain and function for each of the 5 subscales (Pain, Symptoms, Activities of Daily Living [ADL], Sport, and Quality of Life [QOL]) in former professional ASF players with knee and hip osteoarthritis. Higher scores indicate reduced pain and better function.

The association between knee function and factors related to sports exposure, prior injury, and health in former American-style football players. Stepwise linear regression illustrating the association between Knee injury and Osteoarthritis Outcome Score (KOOS) subscales (Pain, Symptoms, Activities of Daily Living [ADL], Sports, Quality of Life [QOL]) and factors of sports exposure, prior injuries, and health. The models controlled for age, race, current body mass index (BMI), lineman status, career duration, meeting physical activity standards, pain severity (excluding Pain subscale), previous anterior cruciate ligament (ACL) surgery, and knee radiographs. Results are presented as scale point β estimates with 95% CIs. Lower estimate scores indicate more symptoms or poorer function. OA, osteoarthritis.
Presence of severe arthritis on knee radiographs was notable for greater symptom severity (KOOS Symptoms score: β estimate = −24.92; 95% CI, −45.28 to −4.55), worse ADL (KOOS ADL score: β estimate = −25.22; 95% CI, −42.96 to −7.48) and sports function (KOOS Sport score: β estimate = −52.47; 95% CI, −76.96 to −27.97), and reduced QOL (KOOS QOL score: β estimate = −63.59; 95% CI, −88.05 to −39.13) (Figure 4). ACL surgery was associated with greater symptom severity (KOOS Symptoms score: β estimate = −17.11; 95% CI, −26.80 to −7.42) and reduced sports function (KOOS Sport score: β estimate = −13.38; 95% CI, −26.71 to −0.05) (Figure 4). Black players reported less pain (KOOS Pain score: β estimate = 15.47; 95% CI, 7.48 to 23.47) and symptom severity (KOOS Symptoms score: β estimate = 10.96; 95% CI, 3.42 to 18.49). Additionally, when the KOOS result was related to radiographic measures, these were found to increase in parallel, suggesting that worse KOOS values were associated with greater radiographic severity of knee OA scores (Figure 4).
Factors Associated With HOOS
The unweighted mean scores for all HOOS subscales were >70 (Figure 3). Fewer demographic, football-related, and health factors were associated with HOOS compared with KOOS (Figure 5). Meeting physical activity standards was associated with reduced pain (HOOS Pain score: β estimate = 8.10; 95% CI, 1.24 to 14.96), and older age was associated with reduced symptom severity (HOOS Symptoms score: β estimate per standard deviation = 3.78; 95% CI, 0.52 to 7.03). Midrange career duration (3-6 professional years) was related to worse sports function (HOOS Sport score: β estimate = −12.55; 95% CI, −23.86 to −1.24) compared with players with <3 seasons, whereas greater pain severity (HOOS Symptom score: β estimate = −1.73; 95% CI, −3.24 to −0.22) was associated with greater symptom severity (Figure 5). Radiographs were not associated with function in contrast to the KOOS, suggesting no relationship between radiographic severity and hip symptoms and function (Figure 5). When looking at player position, linemen vs nonlinemen, we found no differences by KOOS and HOOS results (data not shown).

The association between hip function and factors related to sports exposure, prior injury, and health in former American-style football players. Stepwise linear regression illustrating the association between Hip Disability and Osteoarthritis Outcome Score (HOOS) subscales (Pain, Symptoms, Activities of Daily Living [ADL], Sports, Quality of Life [QOL]) and factors of sports exposure, prior injuries, and health. The models controlled for age, race, current body mass index, lineman status, career duration, meeting physical activity standards, pain severity (excluding Pain subscale), and hip radiographs. Results are presented as scale point β estimates with 95% CIs. Lower estimate scores indicate more symptoms or poorer function.
Discussion
The major findings of our study demonstrated that factors associated with functional limitations from knee OA were different than those associated with hip OA, when using the KOOS and HOOS. Specifically, lower KOOS values corresponding to more symptomatic knee OA were associated with higher pain severity, higher BMI, more likely previous ACL surgery, and greater radiographic severity. Findings suggest that more severe radiographic evidence of OA is associated with high numbers of lower KOOS subscale measures. In contrast, radiograph findings did not correspond with symptoms attributed to hip OA using the HOOS. Former ASF players meeting physical activity standards had better HOOS values, whereas those with midrange career duration scored poorly on the HOOS. Collectively, these results suggest different health characteristics in former ASF players may be important to identify and address when understanding knee and hip OA.
We found high prevalence of radiographic evidence of knee (91%) and hip (98%) OA in this selected population recruited to overrepresent health conditions including chronic pain, cardiometabolic disease, neurocognitive impairment, and sleep apnea. Nearly all former ASF players had radiographic evidence of knee and hip OA. Results weighted to account for selection effects noted that radiographic severity was associated with worse knee function but was not associated with hip function. In the general population, evidence is conflicting as to whether radiographs correspond with symptoms. Although most previous studies have identified an association between greater radiographic severity and worse knee pain and function,20,30,38,55 a separate investigation did not find radiographs as concordant to knee OA symptoms. 56 More limited work has investigated the association between clinical and radiographic hip OA and reported no clear association between hip pain and function with radiographic severity.28,29 In a study of former elite male athletes, 24 knee and hip symptoms and clinical examination were similar to healthy controls even though former athletes had a higher prevalence of radiographic OA. The KOOS and HOOS may not be specific to joint OA and may reflect other pathologies that cause pain, suggesting that history and examination may help with radiographic interpretation. Our results suggest that pain and function may be discordant with the rate of progression of radiographic severity and that we should continue to obtain radiographs as part of our standard assessment when evaluating former athletes with suspected knee or hip OA to facilitate early detection of silent disease and intervention.
We identified that previous ACL injuries sustained during ASF career were associated with greater functional limitations in knee OA. These findings are consistent with previous reports2,31,45,57,62 on high rates of knee PTOA resulting from ACL injuries, 32 with evidence of PTOA within the first 5 years after ACL reconstruction surgery. 2 It is possible that former ASF players who sustained ACL injuries had developed PTOA, which may contribute to reduced function. The results also suggest the potential for ongoing impairments in the years after ACL repair that may overlap and be difficult to distinguish from symptoms attributed to knee OA. Previous evidence links concomitant meniscal and cartilage injuries as increasing the risk for developing PTOA. 62 However, we did not investigate other traumatic knee injuries, and this should be noted as a limitation in our study. These findings highlight the importance of better understanding methods to improve long-term function in former ASF player with ACL injury beyond surgical repair, including optimizing rehabilitation and early interventions to mitigate OA.
Higher BMI was a factor associated with worse knee but not hip function. Evidence in the general population is conflicting on whether higher BMI is associated with worse knee and hip function in those with knee and hip OA. Several studies demonstrate an association between high BMI and worse knee pain and function,1,49 but not all studies have identified higher BMI as a predictor of worse knee function in those with knee OA. 55 Although this relationship in the hip has been less well studied, current literature demonstrates a similar relationship between high BMI, higher pain, and reduced function in those in the general population with more symptomatic hip OA.25,26 Although research in this area is sparse in former elite athletes, higher BMI has been associated with worse pain and function in former Olympians with both knee and hip OA. 7 Our findings suggest that future research should prospectively investigate whether higher BMI is a risk factor for development of knee OA, which may inform future interventions. Our models found that physical activity was associated with greater hip function but was not associated with knee function. This may suggest that former ASF players have greater functional limitations at the knee. Previous literature has identified that former National Football League players have greater prevalence of knee than hip arthroplasty and rates are higher by age compared with the general US population.11,58 Given that severe and symptomatic OA often guides decisions on elective arthroplasty, understanding strategies to improve physical function in former ASF players is critical, especially for those with knee OA. Pain severity was associated with worse functional outcomes in both the knee and the hip. Football is an aggressive contact sport that exposes players to repeated physical trauma during their playing years that can increase their risk of developing joint-related pain. Previous work found that former ASF players with hip or knee arthroplasty or self-reported arthritis had reduced physical function and increased pain interference compared with those without. 3 Our study demonstrates that pain severity is specifically associated with knee and hip function due to knee and hip OA and supports the importance of pain management interventions and a need for a greater understanding of pain mechanisms in former players 36 with these diagnoses. Additionally, ASF players are defined by diverse racial and ethnic backgrounds, and understanding how these are related to pain may provide valuable insight in better characterizing this population. Former White players were more likely to report symptomatic arthritis than Black players. This is in contrast to previous work in former ASF player that identified an increased pain burden among former elite Black players. 13 Understanding these differences by race in describing functional limitations related to pain and pain interference from OA should be further investigated.
Several limitations should be considered in interpretation of our findings. Only a single KOOS and HOOS outcome measure was collected from each former player, and laterality was not specified; therefore, we are unable to assign the KOOS and HOOS values to each knee. This could be addressed in future research by obtaining joint-specific functional outcome scores. Although the KOOS and HOOS are outcome measures used in patients with OA, these measures are not specific to OA but include other knee pathologies, and thus a direct correlation between radiographic OA and function cannot be determined. Additionally, previous ACL surgery was associated with reduced KOOS results. As mentioned earlier, other traumatic knee injuries such as meniscal pathology were not specifically queried in the survey, nor were previous hip injuries or hip surgery collected: This limits our understanding of the association of these injuries and surgeries to symptomatic OA. We used the EOS scan to evaluate multiple joints during weightbearing on a single digital image; this allowed for zoom-in features for a single provider to grade imaging severity but did not include standard views obtained for clinical practice and was not graded by a radiologist. Furthermore, this was a cross-sectional study, so causality cannot be inferred. It is likely that relationships are bidirectional. For example, midrange of career duration was associated with worse sport function in the hip and may be related, in part, to healthy worker effects, as suggested in our previous study. 19 Moreover, we did not account for ceiling effects on the KOOS and HOOS in this active population, and alternative functional outcome measures may have been more appropriate to explore the association between knee and hip OA and function. We categorized position as lineman vs nonlineman based on differences in style of play and body mass; however, we did not perform a position-by-position analysis due to not having adequate statistical power, and future studies may consider investigating by individual positions. Finally, participants were selected using criteria for having a number of participants with 0, 1, or >1 of the following disease categories: cardiometabolic disease, chronic pain, neurocognitive impairment, sleep apnea. Although statistically this was controlled by applying selection weights, we recognize that results would be generalizable only to the broader population of ASF players eligible for the IPA to the extent that the weighting successfully accounted for factors driving selection into the IPA.
Conclusion
Our study found variability within HOOS and KOOS measures. Radiograph findings appeared to correspond with functional status in former ASF players with knee OA but not hip OA. Higher BMI and pain severity were associated with worse function in knee OA, and ACL surgery was associated with worse function in symptom severity and sports function on KOOS. These findings may contribute to obtaining functional measures, history and radiograph to evaluate limitations associated with knee and hip OA in this population.
Supplemental Material
sj-docx-1-ojs-10.1177_23259671261420422 – Supplemental material for Factors Associated With Functional Outcomes in Former Professional American-Style Football Players With Symptomatic Knee and Hip Osteoarthritis
Supplemental material, sj-docx-1-ojs-10.1177_23259671261420422 for Factors Associated With Functional Outcomes in Former Professional American-Style Football Players With Symptomatic Knee and Hip Osteoarthritis by Michelle M. Bruneau, Rachel Grashow, Logan Gaudette, Marc G. Weisskopf, Alicia J. Whittington, Herman A. Taylor, Meagan Wasfy, Frank E. Speizer, Ross Zafonte, Aaron Baggish, Joanne Borg-Stein and Adam S. Tenforde in Orthopaedic Journal of Sports Medicine
Footnotes
Appendix
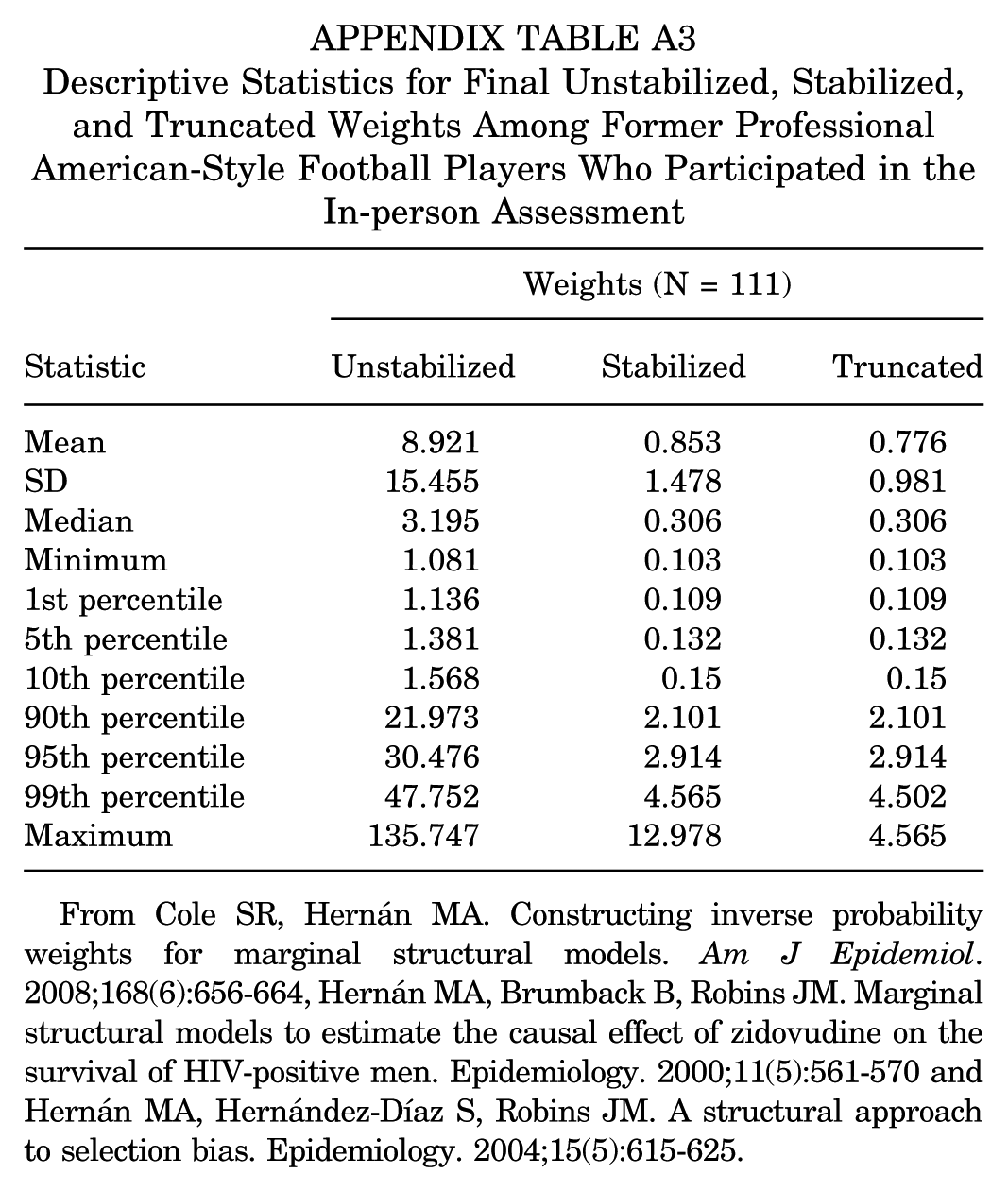
Descriptive Statistics for Final Unstabilized, Stabilized, and Truncated Weights Among Former Professional American-Style Football Players Who Participated in the In-person Assessment
| Weights (N = 111) | |||
|---|---|---|---|
| Statistic | Unstabilized | Stabilized | Truncated |
| Mean | 8.921 | 0.853 | 0.776 |
| SD | 15.455 | 1.478 | 0.981 |
| Median | 3.195 | 0.306 | 0.306 |
| Minimum | 1.081 | 0.103 | 0.103 |
| 1st percentile | 1.136 | 0.109 | 0.109 |
| 5th percentile | 1.381 | 0.132 | 0.132 |
| 10th percentile | 1.568 | 0.15 | 0.15 |
| 90th percentile | 21.973 | 2.101 | 2.101 |
| 95th percentile | 30.476 | 2.914 | 2.914 |
| 99th percentile | 47.752 | 4.565 | 4.502 |
| Maximum | 135.747 | 12.978 | 4.565 |
From Cole SR, Hernán MA. Constructing inverse probability weights for marginal structural models. Am J Epidemiol. 2008;168(6):656-664, Hernán MA, Brumback B, Robins JM. Marginal structural models to estimate the causal effect of zidovudine on the survival of HIV-positive men. Epidemiology. 2000;11(5):561-570 and Hernán MA, Hernández-Díaz S, Robins JM. A structural approach to selection bias. Epidemiology. 2004;15(5):615-625.
Final revision submitted December 9, 2025; accepted January 3, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: All authors received research funding from the Football Players Health Study at Harvard University, which is funded by a grant from the National Football League Players Association. None of the authors report a conflict of interest regarding the manuscript being submitted to OJSM.
The testing protocol was approved by the Institutional Review Board of the Harvard T.H. Chan School of Public Health, and participants provided written informed consent in accordance with institutional policies.
Author Note
Limited deidentified data are available upon reasonable request for subsequent analysis/inclusion in meta-analysis by contacting the corresponding author: Michelle Bruneau (
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.