
Abstract
Objective
Visual inspection of the lower limb is often part of standard clinical practice during a physical examination at the outpatient clinic. This study aims to investigate how reliable visual inspections are in terms of detecting lower limb malalignments without additional tools and physical examinations.
Design
This study enrolled 50 patients. Each patient underwent a whole leg radiograph (WLR); in addition, a standardized digital photograph was taken of the lower limbs. Four persons (different experience levels) visually rated the digital photograph twice (unaware of the hip knee angle [HKA] on the WLR) and placed them in the category: severe valgus (>5°); moderate valgus (2°-5°); neutral, moderate varus (2°-5°); and severe varus (>5°). Visual ratings were compared with the measured HKA on WLRs for correlation using Spearman’s rho. Linear ordinal regression models with significance when P < 0.05 were used to test whether body mass index (BMI), age, gender, and HKA were possible risk factors for incorrect visual HKA assessment.
Results
Spearman’s rho between the visual assessment and measured HKA on the WLR was moderate with 0.478 (P < 0.01). Women had an increased odds ratio of 3.7 (P = 0.001) for incorrect visual assessment. Higher HKA also increased the odds ratio for erroneous visual assessment with 1.4 (P = 0.003). BMI and age did not significantly increase the odds of erroneous visual leg axis assessments in this study.
Conclusions
Visual assessment of the lower limb alignment does not provide clinically relevant information. Lower limb malalignment diagnoses cannot be performed using only a visual inspection. Physical examination tests and radiographical assessments are advised.
Level of evidence:
Diagnostic level II
Introduction
Varus malalignment is present in 53% to 76% of individuals with unicompartmental knee osteoarthritis (OA). 1 Malalignment increases the risk of developing and progressing OA due to loading imbalance of the knee joint.2,3 Realignment surgery is considered a good treatment option for unicompartmental knee OA with varus malalignment.4,5 Next to the management of unicompartmental OA, lower limb (mal)alignment is an important variable in multiple knee pathologies. Treatment outcome increases in osteochondritis dissecans, meniscal lesions, ligamentous injuries, and (osteo)chondral lesions management when combined with a favorable limb alignment. 6
During physical examination, several methods are available for the assessment of lower limb alignment.1,7,8 These methods make use of goniometers, calipers for intercondylar and intermalleolar distances, inclinometers, and physical tests.1,7 All these alternatives for whole leg radiographs (WLRs) were tested and compared with the measured leg axis on WLRs for correlations, ranging from low to good.1,7,8 In case of a suspected malalignment, physicians could indicate obtaining additional WLRs. 9 These physical examination methods are advantageous in terms of lower radiation exposure, decrease in health care costs, and in cases of no available WLR system.1,7
The reliability of only a visual inspection (visual observation of the patient in stance on both legs in the examination room) for the detection of lower limb malalignment is to the best of our knowledge unknown. This potentially affects decision making during clinical workup when physicians rely too much on only a visual assessment and omit further investigations in the examination room and/or additional radiographs such as a WLR.
Our goal was to investigate whether visual inspection of the leg alignment is a reliable method. The hypothesis of this study is that only a visual inspection of the lower limb is not sufficient for the detection of lower limb malalignment.
Materials and Methods
This study was approved by the local ethics board of the medical center (METC number 20-568). Patients were recruited at the outpatient clinic of the University Medical Center (UMC) Utrecht, a tertiary orthopedic referral center for knee pathology. Patients were eligible when a WLR was obtained on the same day as their appointment at the outpatient clinic. Exclusion criteria were age below 18 years; inability to read, communicate, and/or speak the Dutch language; and incapable of providing informed consent. When willing to participate, informed consent was signed. Body mass index (BMI), age, gender, and possible surgical indication were subtracted from the electronic health records.
Digital Photograph of Lower Limbs
Included patients were all placed in the examination room following the WLR protocol used at our radiology department. 10 The conditions for obtaining the digital photograph were kept similar to the WLR, making the images from the 2 modalities consistent for assessments. The patient’s feet were placed 10° externally rotated and 10 cm apart on a template. The knees were in full extension and both arms alongside the body. The researcher also placed the hips and upper body of the patient straightforward. In addition, the researcher instructed the patients to distribute their weight equally over both legs. A Sony Cybershot digital camera was used to obtain visual digital photographs of the lower limbs in a standing position. Digital photographs were taken from knee height, with 2 meters from the patient (Fig. 1).
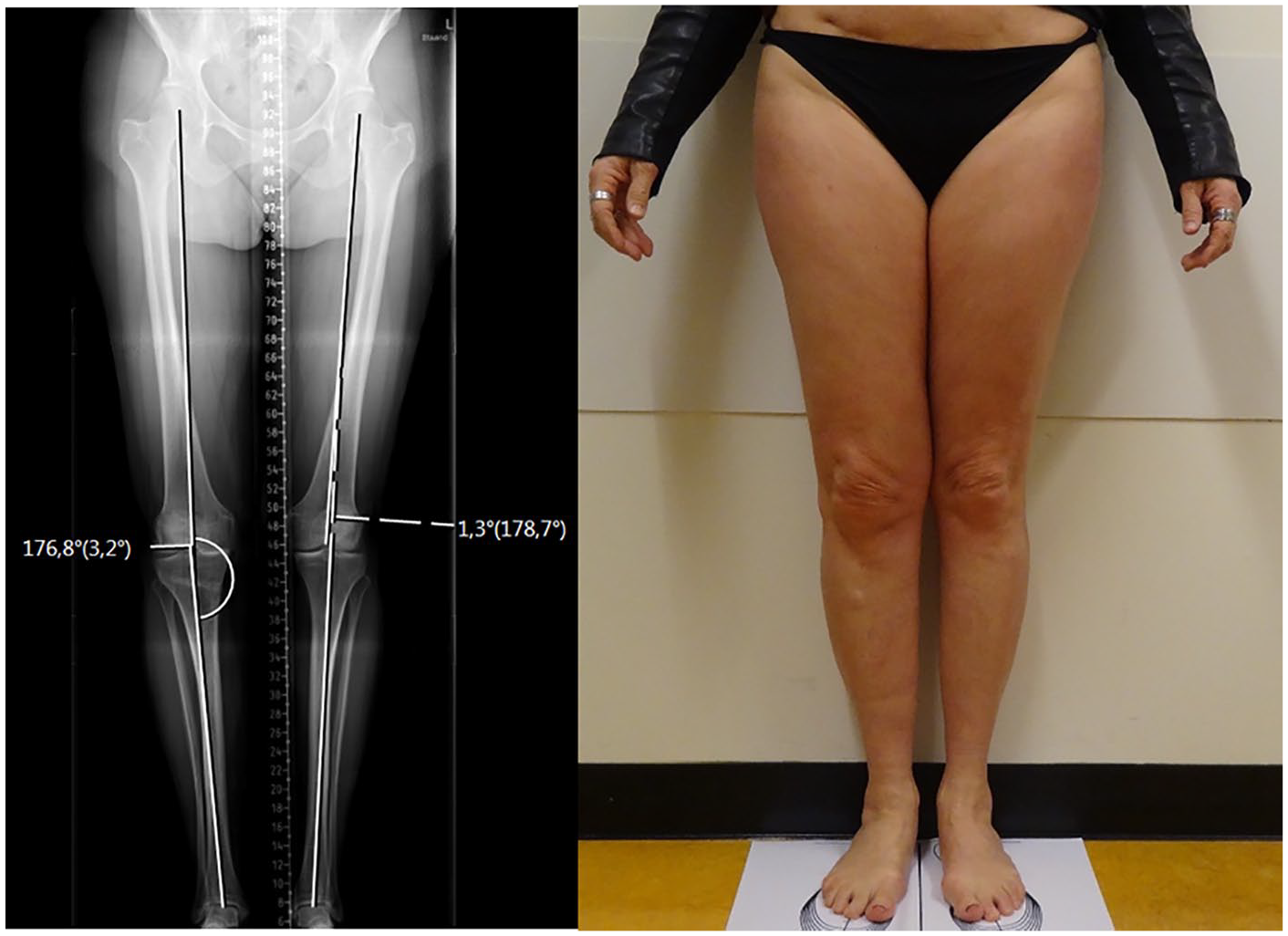
Included patient with on the left her WLR and on the right her digital photograph. The HKA measured on the WLR was 1.3° valgus for the left leg and 3.2° varus for the right leg. All observers overlooked the varus deformity present in the right leg and classified it as neutrally aligned. WLR = whole leg radiograph; HKA = hip knee angle.
Visual Assessment
Each digital photograph was randomly assessed twice bilaterally by 4 observers with 1 week in-between, with varying experience levels (orthopedic surgeon with 10 years’ experience, orthopedic surgeon with 5 years’ experience, orthopedic resident, and researcher). All observers were blinded from the hip knee angle (HKA) present on WLRs during visual observations. HKA alignment was divided into four categories: severe valgus (>5°); moderate valgus (3°-5°); neutral, moderate varus (3°-5°); and severe varus (>5°). During the visual assessments, observers classified the lower limbs in 1 of the 5 ordinal categories. To test whether there was a possible bias between real-life visual observations and digital photographs, 1 observer (H.C.N., researcher) assessed all the leg axes in real life next to the digital photographs.
Visual assessments were compared with the measured HKA present on WLR of the same patient, also categorized into the same groups. Visual assessments were classified as incorrect when the visually assessed lower limb category did not correspond with the measured category on the WLR.
WLR HKA Measurement
The researcher measured the HKA twice randomly, with 1 week in-between for intra-observer reliability analyses. HKA measurements on the standardized WLR used in our center were proven excellent reliable between one and multiple observers with measurement errors below 0.9°. 11
Whole Leg Radiograph
This study used the Philips DigitalDiagnost v4.0 (Philips, Amsterdam, the Netherlands) for radiographical imaging. The fixed distance between the x-ray beam source and detector plate was 265 cm. The system had a fixed x-ray beam source height, which obtained 3 different bilateral images (proximal femur, knee joint, distal tibia) by pivoting the source toward the upper, middle, and lower parts of the lower limbs. The 3 separate images were then combined into 1 WLR by Philips DigitalDiagnost v4.0 software. The x-ray settings were kept the same for each patient, with kV set at 81 and varying mAs. Patients were positioned following a proven reliable protocol. 11
Statistical Analyses
As the primary outcome, the visual assessments and measured HKAs on WLRs were tested for ordinal correlation using Spearman’s rho, with statistical significance when P < 0.05. Only the second visual assessment was used for analysis, except for the intra-rater reliability analyses. Two-way mixed intraclass correlation coefficient (ICC) analyses for the absolute agreement were performed for intra- and inter-observer reliabilities of the visual assessments. A chi-square test for homogeneity was used to analyze whether there was a significant difference between real-life visual and digital photograph visual assessments. Linear ordinal regression models with significance when P < 0.05 were used to test whether BMI, age, gender, and HKA were possible risk factors for inducing incorrect visual leg axis assessment. HKA measurements on the WLRs were tested for intra-observer reliability using 2-way random ICC for absolute agreement.
Results
This study included 50 WLRs of patients, of which 31 (62%) were males and 19 (38%) females. The median age was 37 (18-58) years, the mean BMI was 25.4 (SD = 4.2), and the mean HKA was 178.9 (SD = 2.7). Reported surgical indications included an osteotomy, total/partial knee arthroplasty, and (osteo)chondral lesion treatment, for example, autologous chondrocyte implantation and microfracture. Characteristics of each alignment group are listed in Table 1.
Distribution of Patients’ Leg Alignments Categorized into Severe Valgus (HKA > 185°), Valgus (HKA 183°-185°), Neutral (HKA 182°-178°), Varus (HKA 177°-175°), and Severe Varus (HKA < 175°).
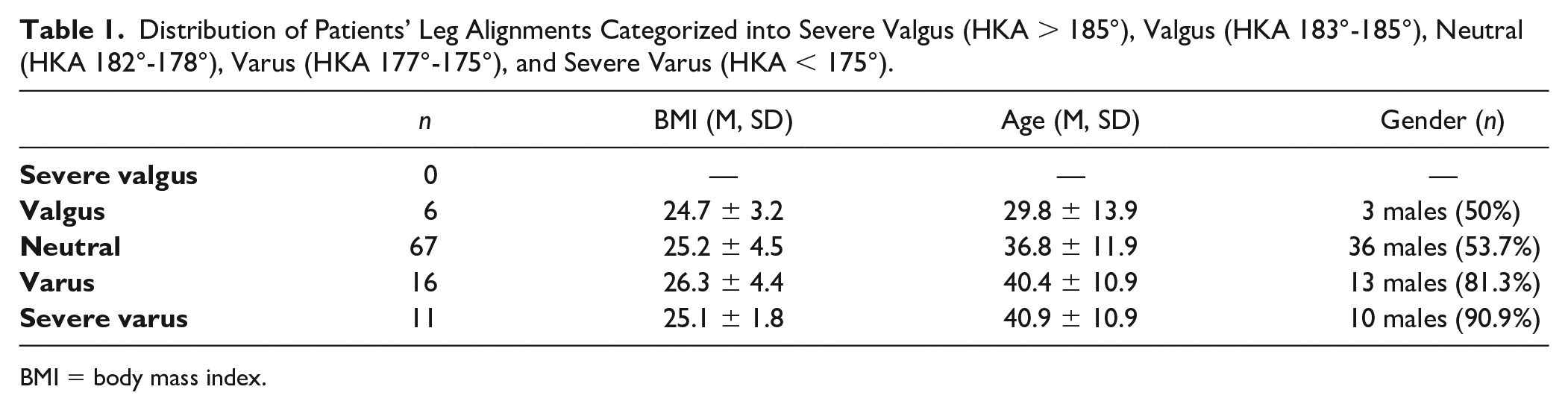
BMI = body mass index.
Visual Assessments
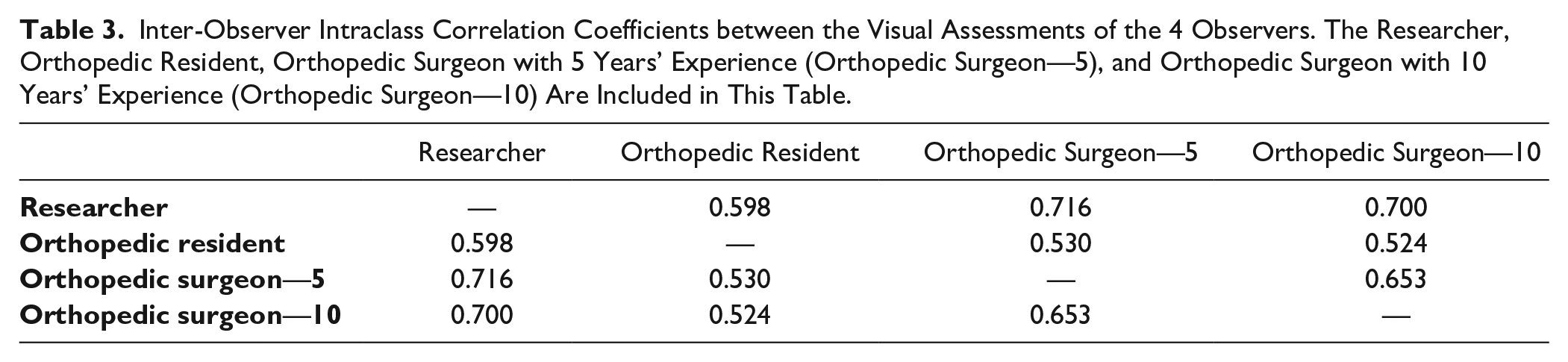
Spearman’s rho between the visual leg axis assessment of all observers and measured HKA on WLRs was moderate with 0.478 (P < 0.001). ICCs between the first and second assessments of the observers are moderate to good and listed in Table 2. Table 3 summarizes the inter-observer correlations between the 4 observers included in this study, which were all moderate. All visual assessments of patients’ leg axes are presented in Figure 2. The histogram plots the visual assessments per patient lower limb alignment, based on the measured HKA on the WLR.
Intra-Observer ICCs between the 2 Visual Assessments on Different Moments of the Observers, with 95% Confidence Intervals.
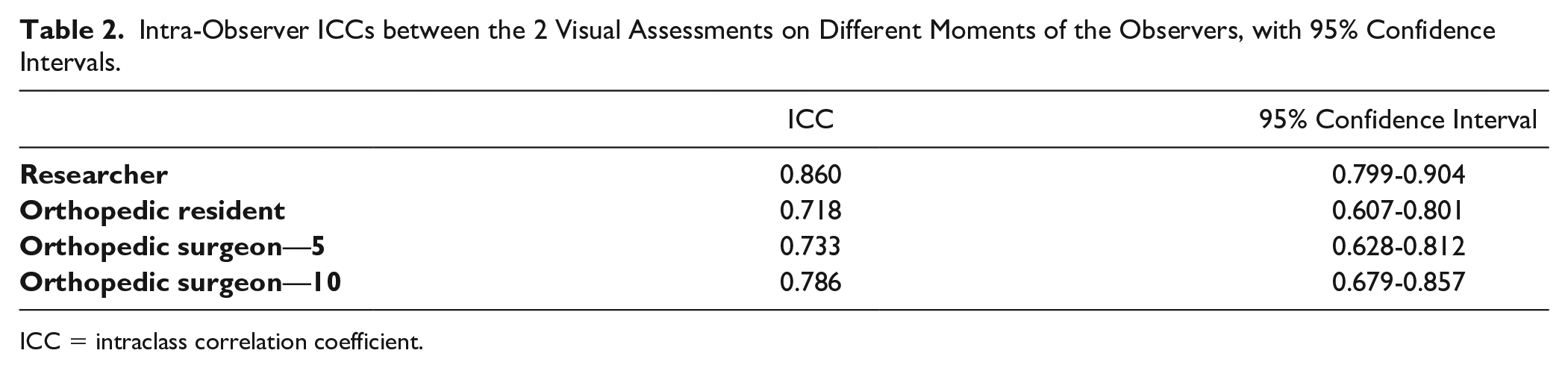
ICC = intraclass correlation coefficient.
Inter-Observer Intraclass Correlation Coefficients between the Visual Assessments of the 4 Observers. The Researcher, Orthopedic Resident, Orthopedic Surgeon with 5 Years’ Experience (Orthopedic Surgeon—5), and Orthopedic Surgeon with 10 Years’ Experience (Orthopedic Surgeon—10) Are Included in This Table.
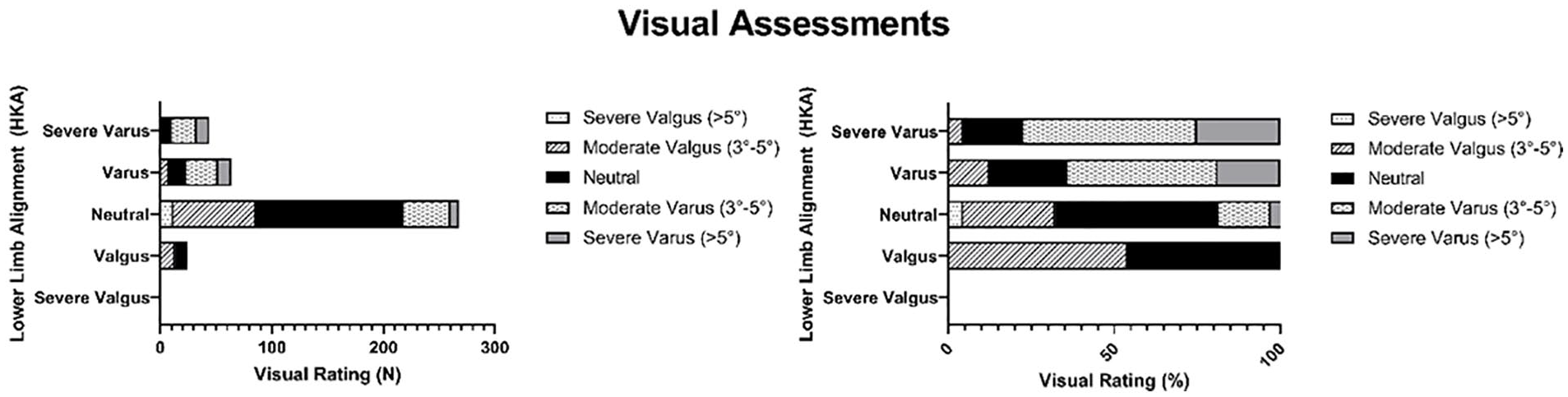
Visual assessments in numbers (n) and percentages (%) of patients’ leg axes per category, based on measured hip knee angle (HKA) on whole leg radiographs (WLRs): severe valgus, valgus, neutral, varus, and severe varus patients. The y-axis illustrates the alignment categories based on the measured HKA on the WLR. The x-axis summarizes the 400 observations of 4 observers of 100 lower limbs, while the bars with different gray scales denote the visual assessment.
Radiographic Assessment
Radiographic assessment of the 100 included legs resulted in 11 severe varus, 16 moderate varus, 67 neutral, 6 moderate valgus, and 0 severe valgus (based on the HKA measured on the WLR) cases.
Incorrect Visual Assessments
The percentage of incorrect visual leg axis assessments ranged between 45.8% and 75.0% (Fig. 3). The errors were lowest in patients with a moderate valgus alignment and highest when the patient presented a severe varus deformity (Fig. 3). Figure 3 also visualizes the 4 observers with different experience levels separately. Chi-square tests for homogeneity between the 4 observers resulted in no significant differences (χ2 = 1.651, P = 0.199). Figure 1 illustrates an example case, in which all the observers visually assessed the leg axis incorrectly.
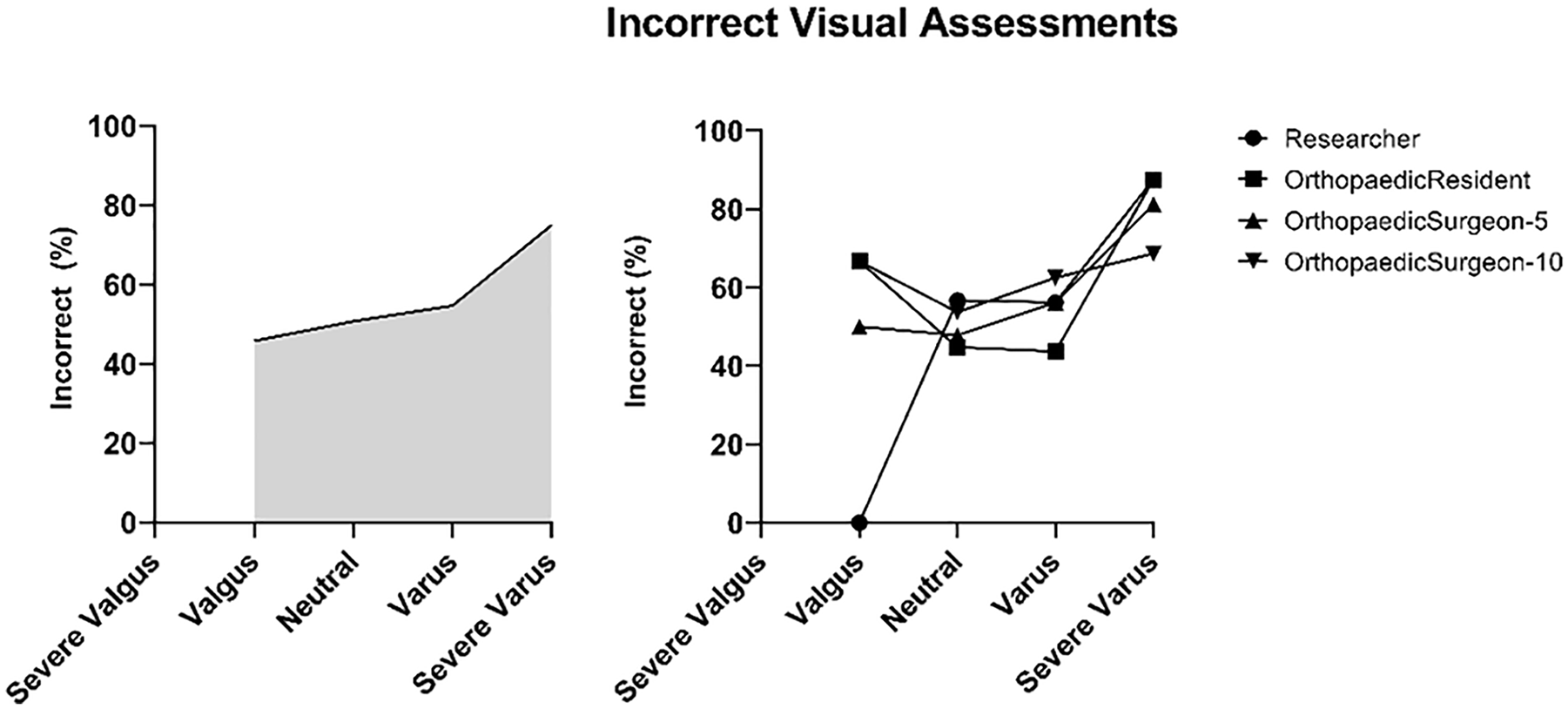
Percentage of erroneous visual assessments by all observers on the left. On the right is the percentage of erroneous visual assessments by the different observers. Researcher, orthopedic resident, orthopedic surgeon (5 years’ experience), and orthopedic surgeon (10 years’ experience).
Real-Life and Digital Photograph
Chi-square test for homogeneity between real-life and photographic visual leg axis assessment resulted in no significant differences (χ2 = 0.520, P = 0.471) between the 2 methods.
Risk Factors in Visual Leg Axis Assessment
Women had an increased odds ratio of 3.7 (P = 0.001) for incorrect visual leg alignment assessment. Also, an increasing HKA itself had a significant (P = 0.003) effect on incorrect visual assessments with an odds ratio of 1.4. Other patient characteristics like BMI and age did not significantly increase the odds of erroneous visual leg axis assessments in this study.
Intra-Rater Reliability HKA Measurement
ICC between the first and second moment of HKA measurements on the WLR was excellent, 0.993 (CI, 0.989-0.995), with a mean absolute error between the 2 measurements of 0.15° (SD = 0.29°).
Discussion
This study researched the reliability of a visual inspection in terms of detecting lower limb malalignments. The visual inspections of the observers were moderately correlated to the measured HKA on WLR. The percentage of incorrect assessments ranged between 45.8% and 75.0%, making a visual inspection as a standalone diagnostical method unreliable. Patients with a neutral leg alignment were assessed to be pathological in 50.7% of the times. Given this, patient indication for undergoing additional examinations such as WLRs based on only a visual inspection is not sufficient.
Physicians should perform physical tests and possibly subsequently request a WLR for reliable leg geometry measurements. 11 Additional tests during physical examination include using goniometers, calipers for intercondylar and intermalleolar distances, and inclinometers.1,7 In addition to physical tests and WLRs, plain knee radiographs are an excellent option for the measurement of femoro-tibial angles which correlates to the HKA. 12
A favorable leg axis, in which the mechanical axis passes through the healthy knee compartment, is a powerful tool in the treatment of knee pathologies.4,5,13-15 Missed lower limb deformities could therefore have a serious clinical impact. The results of this study show substantial amounts of neutrally visually assessed lower limbs, while they were severe varus (>5°), moderate varus (2°-5°), and moderate valgus (2°-5°). This study reported a rate of 18.2% in cases of severe varus deformities, where the lower limb was visually assessed to be neutral (Fig. 2). For varus deformities, the rate of overlooked deformities was 23.4% (Fig. 2). In cases of valgus deformities, the rate of neutrally assessed lower limbs was 45.8% (Fig. 2).
The difference between the severe varus and neutral categories was at least 3° (18.2% of the cases) and between the valgus categories at least 5° (4.5% of the cases). Due to the used visual rating method, the mismatch between visual rating and measured HKA could not be provided in absolute degrees. But these results indicate that a mismatch in visual assessment and actual HKA of more than 3° is common with 18.2% in severe varus legs, which is, for instance, higher than the possible clinical accuracy of <1° in osteotomies.16-18 To put this in another perspective, for the detection of varus/valgus malalignment, an accuracy of 3° from natural is needed. 19 This means that diagnoses based only on visual assessments are clinically not sufficient.
The ICC between the resident and surgeon with 10 years of experience was lowest at 0.524. This is a notable result as residents are working closely together with the surgeons as part of their training. Of note, the differences between all raters in this study were not statistically significant. The researcher and orthopedic surgeons are focused on malalignments and knee pathologies, in both their research and treatment of patients. This means that in real clinical settings, the difference in visual malalignment assessments between physicians could be higher.
The results of this study show that gender influences the visual assessment of patients’ leg axis. Women do present an increased risk for incorrect visual ratings. A possible explanation could be the difference in the anatomical axis of the femur between men and women.20,21 The femoro-tibial angle was observed to be more valgus in women and of influence on the correlation with the HKA. 20 Interestingly, BMI was also considered a possible inducer of errors, due to increased soft tissue enveloping the bones of these patients. But in this study, we found no significant effects of BMI, comparably with reports of Gibson et al.,22,23 where they included participants with a mean BMI of 31.3. A possible explanation is that high BMI ratios do not necessarily mean high-fat concentrations in the leg and therefore around the landmarks for HKA assessments. 23
Our study had some limitations. First, visual assessments were performed on two-dimensional (2D) photographs instead of physical inspection in the examination room. However, the author rated the patients in real life as on photographs with no significant differences between the 2 methods. Second, this study included no patients with severe valgus deformities. Bellemans et al. 19 reported the likelihood of severe valgus deformities to be very low (<1%). The third limitation of this study was that only one observer measured the HKAs on WLRs. Therefore, there was no control for the inter-observer reliability regarding the HKA measurements. Earlier reports, however, showed high reliabilities of HKA measurements on WLRs.11,24-27 The HKA measurements performed in this study resulted in high intra-observer reliability, with a low mean absolute error of 0.15° between the 2 measurement moments. This is comparable with most literature.11,24-27
Conclusion
Visual assessment of the lower limb alignment does not provide clinically relevant information. Lower limb malalignment diagnoses cannot be performed using only a visual inspection. Physical examination tests and radiographical assessments are advised.
Footnotes
Author Contributions
HCN conducted this study, after developing the research question together with RJHC, and HCN, HMV, RJHC, and NvE performed the measurements for this research. HCN, RJBS, and HW analyzed the data and performed the statistics. All authors contributed to the writing of the manuscript and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the ethics board of the UMC Utrecht hospital (METC number: 20-568).
Statement of Informed Consent
All included patients signed informed consent before participating in this study.