
Abstract
Background:
Proximal hamstring avulsion injuries (PHAIs) are significant but rare injuries that might require surgical repair. However, limited data exist on postoperative complication rates, associated risk factors, and long-term musculoskeletal outcomes.
Purpose:
To analyze the complication rate following PHAI surgery, identify risk factors for non-rerupture complications, and investigate the incidence of associated musculoskeletal conditions.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This prospective cohort study included 757 patients (mean age, 47.3 years) surgically treated for PHAI between 2002 and 2023. Patients with revision surgery or bony avulsions were excluded. Primary outcomes were complication rates and associated risk factors. Secondary outcomes included the functional outcomes of patients with or without complications, assessed through the Parisian Hamstring Avulsion Score (PHAS), Tegner Activity Scale, and UCLA score (University of California, Los Angeles).
Results:
The overall complication rate was 10.4% (79/757), including a 5.6% rerupture rate and 4.7% non-rerupture complication rate. Most complications (75%) occurred within 5.5 months postsurgery. Significant risk factors for non-rerupture complications included work-related accidents (odds ratio, 5.59; 95% CI, 1.43-37.0; P = .029) and isolated semimembranosus injuries (odds ratio, 12.1; 95% CI, 2.13–227; P = .020). Moderate to severe sitting discomfort was reported in 5% of the cohort but was not associated with postoperative complications. Functional outcomes were worse in the complication group, with lower PHAS (P = .0053) and reduced return-to-sport rates at the preoperative level (31.3% vs 65.0%; P = .0137).
Conclusion:
PHAI surgery has a 4.7% complication rate excluding reruptures and 10.4% including them. These complications notably impair functional outcomes. Work-related accidents and isolated semimembranosus injuries are risk factors for non-rerupture complications. Moderate to severe sitting discomfort occurs in a minority of patients (~5%) and does not appear directly linked to postoperative complications.
Registration:
NCT02906865 (ClinicalTrials.gov identifier).
Proximal hamstring avulsion injuries (PHAIs) are rare but significant injuries that primarily affect athletes and individuals involved in physical activities.4,6,11,24 These injuries typically occur owing to sudden and forceful hip flexion combined with knee extension, leading to the detachment of the hamstring tendons from their origin at the ischial tuberosity.2,3,16 The management of PHAI often requires surgical intervention, particularly in cases where nonoperative treatment fails or when the injury involves complete avulsion or partial avulsion with retraction >2 cm.4,6,10,20 However, the decision to opt for surgery versus nonoperative treatment remains controversial, with ongoing debates in the literature regarding the best approach. §
The complexity of managing PHAI is compounded by the risk of complications associated with surgical repair.6-8,12,17,18 A recent systematic review by Lawson et al 8 highlighted that the overall complication rate after proximal hamstring tendon repair is 15.3%, with major complications occurring in 4.6% of cases. These complications include sciatic nerve injury, venous thromboembolism, reoperation, rerupture, and deep infection. Minor complications are also notable, such as posterior femoral cutaneous nerve injury, persistent hamstring myopathy, and sitting pain. However, these complication rates were derived from 43 articles that included various surgical techniques and different surgeons and exhibited a high level of heterogeneity. This variability highlights the need for more precise epidemiologic data from homogeneous cohorts to better understand the incidence and nature of complications. While successful tendon reattachment can lead to excellent functional recovery, the occurrence of complications can profoundly affect recovery. Furthermore, the long-term outcomes, including the development of associated musculoskeletal conditions, remain poorly understood, with a notable absence of studies investigating these epidemiologic aspects of hamstring pathology.
In this context, the aim of this study was to determine the complication rate after primary surgical repair of PHAI and to identify the risk factors associated with these complications. It is hypothesized that certain patient demographics (eg, age, body mass index), injury characteristics (eg, chronicity, completeness, retraction), and surgical factors (eg, type of incision, surgeon experience) are significantly associated with an increased risk of postoperative complications after PHAI surgery.
Methods
Study Design and Inclusions
This prospective cohort study was conducted at a sports surgery referral center between 2002 and 2023 targeting all patients operated for primary PHAI. The study is part of the Proximal Hamstring Avulsion Cohort Study (clinical trial identifier: NCT02906865) and was approved by the local ethics committee. Patients’ consents were obtained at the beginning of the enrollment in the cohort.
Inclusion criteria included adult patients >18 years old, primarily treated with PHAI repair with a minimum follow-up of 12 months. Exclusion criteria included revision surgery, allograft usage, preoperative motor sciatic nerve palsy, and bony avulsion of the ischial tuberosity.
Surgical Technique and Postoperative Rehabilitation Protocol
All patients were treated following the surgical technique described by Lefèvre et al. 9 Surgery was conducted with the patient in the prone position, hip slightly flexed (∼20°), and knee flexed to relax the hamstrings. The incision was made vertically or transversely in the gluteal fold, depending on tendon retraction and chronicity. A transverse incision was preferred for acute tears with minimal retraction, whereas a vertical incision was specifically used for more retracted and chronic injuries, as it provides greater proximal-distal exposure and facilitates identification and mobilization of retracted tendon stumps. The sciatic nerve was systematically identified and protected, with neurolysis performed when fibrotic adhesions were present. Tendon reinsertion was achieved by using 3 or 4 metal or absorbable suture anchors (Lupine Loop Anchor; DePuy Mitek) in a modified Mason-Allen configuration.
Postoperatively, patients were immobilized with the knee in 30° to 45° of flexion with an articulated brace for approximately 6 weeks, allowing flexion but limiting extension. Partial weightbearing and early isometric rehabilitation were initiated as tolerated. All patients received routine pharmacologic deep vein thrombosis prophylaxis (low-molecular-weight heparin) according to institutional protocol for 6 weeks. Indications for surgery include complete PHAI and partial tendon tears. Most were treated by the senior surgeon (N.L.). The remaining patients were treated by senior sports surgeons belonging to the same surgical crew following the same technique.
All patients underwent magnetic resonance imaging for both hips at 6 months postsurgery to screen for healing, rerupture, and any other detectable complication.
Outcome Measures
The primary outcome measure was the complication rate after PHAI surgery.
The study analyzed risk factors associated with all causes of complications, excluding rerupture, which was investigated separately in a different study. 12 Additionally, the study examined risk factors related to neurological complications.
The potential risk factors analyzed were age, body mass index, and other patient demographics, such as sex, injury side, sports level, injury circumstances, and lesion characteristics (including chronicity, completeness, and retraction). Technical details (eg, type of incision) and surgeon experience were also analyzed as potential risk factors. Surgeon experience was measured by the number of previously operated cases at the time of surgery, referred to as the surgeon's case volume at the time of each procedure. These data were studied as both a continuous variable and a categorical one based on a receiver operating characteristic (ROC) threshold. A learning curve was also drawn.
The secondary outcome measures included the patients’ reported outcome measures at final follow-up. Of note, patients who underwent an operation for rerupture were not in the functional outcome analysis. The functional outcomes of patients with complications (excluding operated rerupture) were also reported and compared with those without complications. For these outcomes, additional exclusions were applied to ensure a minimum follow-up of 2 years. These outcomes included the Parisian Hamstring Avulsion Score (PHAS), which is a recently validated 20-item score that ranges from 1 to 100 with a higher score indicating a better outcome. Other outcomes were the Tegner Activity Scale 22 and the UCLA scale (University of California, Los Angeles),1,28 which are used to evaluate the level of physical activity and the quality of joint function, respectively.
Furthermore, the rate of return to sport (RTS) at 2 years postoperatively was reported as a binary outcome (yes/no). The quality of RTS was also evaluated by the patient's perception of performance, categorized as the same as or below the preinjury level.
Data Collection
All data were collected prospectively via internet-based software (Websurvey). The data software was accessed and filled by surgeons for physical examination findings, imaging results, and technical details. It was also accessed by patients for demographic characteristics and outcome scores. Chronicity was defined as injury-surgery delay >4 weeks.
Participants and Sample Size
During the study time frame, 949 patients were eligible for inclusion in the study. Of them, 192 were excluded (Figure 1). The final sample size was 757 patients.

CONSORT flowchart.
Statistical Analysis
Descriptive statistics included frequencies and percentages for categorical variables. For continuous variables, the mean and standard deviation were reported if the variables followed a normal distribution, as determined by the Shapiro-Wilk test. If normality was not observed, the median and interquartile range (IQR) were used. Comparisons between patients with and without complications were performed by the Student t test or Wilcoxon rank sum test for continuous variables and the chi-square test or Fisher exact test for categorical variables, depending on the sample size.
Univariate analyses were performed with logistic regression to identify potential risk factors associated with postoperative complications. Additionally, a ROC curve analysis was conducted to determine if there was a threshold in the number of surgical procedures already performed by a surgeon that significantly reduced the risk of complications.
All statistical analyses were conducted in R software (Version 4.2; R Foundation for Statistical Computing), with a 2-tailed significance level of P < .05.
Results
Patient Characteristics
The study population included 757 patients. The demographic and clinical characteristics are summarized in Table 1.
Characteristics of the Study Population (N = 757)

Rate of Complication
Among the 757 patients in the study, 78 experienced all-cause complications, resulting in an overall complication rate of 10.3% (Table 2). These complications predominantly occurred within the first year postoperatively, with 50% of cases presenting within 48 days and 75% within 5.5 months. The mean time to complication was 97.3 days (SD, 134.2), with a median time of 48 days (IQR, 11-169).
Frequency and Type of Complication After Proximal Hamstring Avulsion Surgery (N = 757) a

Certain patients may have >1 complication.
Rerupture, the most common major complication, was observed in 43 patients (5.6%). Other major complications included deep venous thrombosis in 5 patients (0.66%) and deep infection in 1 (0.13%). Minor complications occurred in 30 patients (3.9%) (Table 2). Interestingly, among patients excluded owing to revision surgery, 2 had preoperative sciatic nerve palsy. All neurological complications were transient, resolving spontaneously or with conservative management. No permanent motor or sensory deficits were observed at final follow-up.
Sitting Tolerance
Discomfort when sitting for prolonged periods was evaluated among the 517 patients with at least 2 years of follow-up. Overall, 275 patients (53%) reported no difficulty, 142 (28%) mild discomfort, 71 (14%) moderate discomfort, 23 (4%) severe discomfort, and 6 (1%) an inability to sit for prolonged periods. Of these 6 patients, 5 belonged to the noncomplication group and 1 to the complication group, indicating that sitting pain was not specifically associated with postoperative complications.
Risk Factors for All-Cause Complications Excluding Rerupture and Learning Curve
In the risk factor analysis, work-related accidents (odds ratio [OR], 5.59; 95% CI, 1.43-37.0; P = .029) and injuries involving the semimembranosus tendon alone (OR, 12.1; 95% CI, 2.13-227; P = .020) were identified as significant predictors of non-rerupture complications (Table 3). All isolated semimembranosus ruptures were repaired with a vertical incision. No significant association was found between incision type and tendon involvement among patients with complications (P = .67), suggesting that the higher complication rate in semimembranosus injuries was not incision related. Other factors, such as age, sex, body mass index, type of sport, injury chronicity, and surgeon case volume, were not significantly associated with complications (P > .05).
Risk Factor Analysis for All-Cause Complications Excluding Rerupture a

Bold indicates P < .05.
When complications were analyzed in a subgroup formed of only chronic injuries, no significant difference was observed in the impact of surgeon experience on the complication rate, whether measured by total surgical procedures (OR, 0.99 for every 10 additional procedures; 95% CI, 0.96-1.02) or by surgeons with <200 surgical procedures (OR, 0.56; 95% CI, 0.20-1.48; P = .244). In the analysis of risk factors related to neurological complications, there were no associated factors (P > .05)
The ROC curve analysis confirms the results of the regression analysis and demonstrates that surgeon experience, measured by the number of previously operated cases, has no significant predictive value for complications excluding rerupture (Figure 2).

Receiver operating characteristic (ROC) curve assessing the predictive value of surgeon experience on complication rates.
Impact of the Complication Excluding Rerupture on the Functional Scores and RTS at Last Follow-up
Among the 35 patients with non-rerupture complications, 9 were not in the functional outcome analysis owing to missing 2-year follow-up data (Table 4). Complications were associated with significantly poorer functional outcomes. The complication group had a lower median PHAS score (85.3; IQR, 58.0-97.0) as compared with the noncomplication group (94.0; IQR, 84.5-98.5; P = .0053). Similarly, the median Tegner Activity Scale score was reduced in the complication group (3.0; IQR, 3.0-5.0) versus the noncomplication group (4.0; IQR, 3.0-6.0; P = .0182). UCLA scores also differed significantly, with a median 6.0 (IQR, 4.0-9.0) in the complication group as compared with 8.0 (IQR, 6.0-10.0) in the noncomplication group (P = .0063).
Functional Outcomes and Return to Sport in Patients With and Without Complications, Excluding Rerupture a
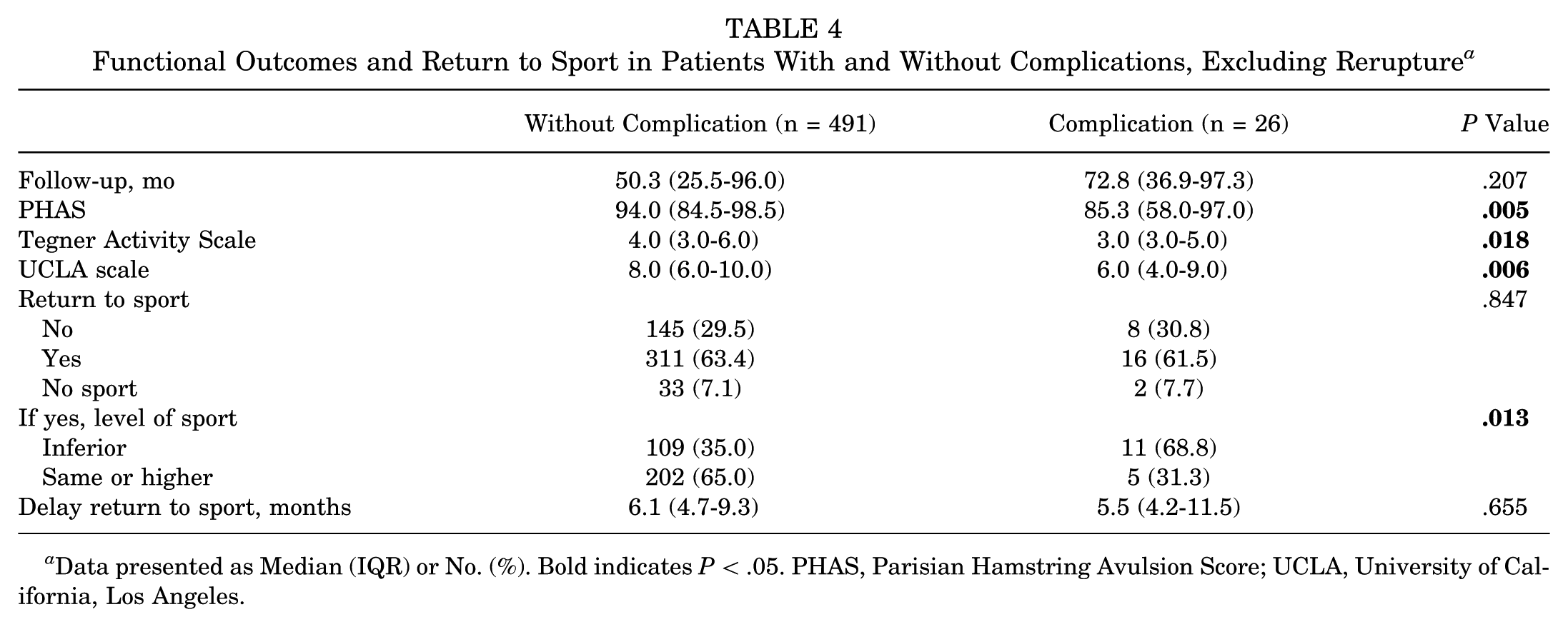
Data presented as Median (IQR) or No. (%). Bold indicates P < .05. PHAS, Parisian Hamstring Avulsion Score; UCLA, University of California, Los Angeles.
While the overall RTS rate was similar between groups, the RTS level was significantly affected. Among those who returned to sport, 31.3% of the complication group returned at the same preoperative level, as compared with 65.0% in the noncomplication group (P = .0137).
Impact of Neurological Complications on Functional Outcomes
A dedicated subgroup analysis focusing on neurological complications (n = 11) revealed an even greater functional impact (Table 5). These patients showed a markedly reduced PHAS (median, 60.0; IQR, 54.0-88.0; P = .0006) and UCLA score (median, 4.0; IQR, 4.0-9.0; P = .0075), with a trend toward lower Tegner values (P = .0505). While overall RTS rates remained comparable, only 31.3% of these patients resumed sport at their preinjury levels versus 64.8% in the noncomplication group (P = .009).
Functional Outcomes and Return to Sport in Patients With and Without Neurological Complications a
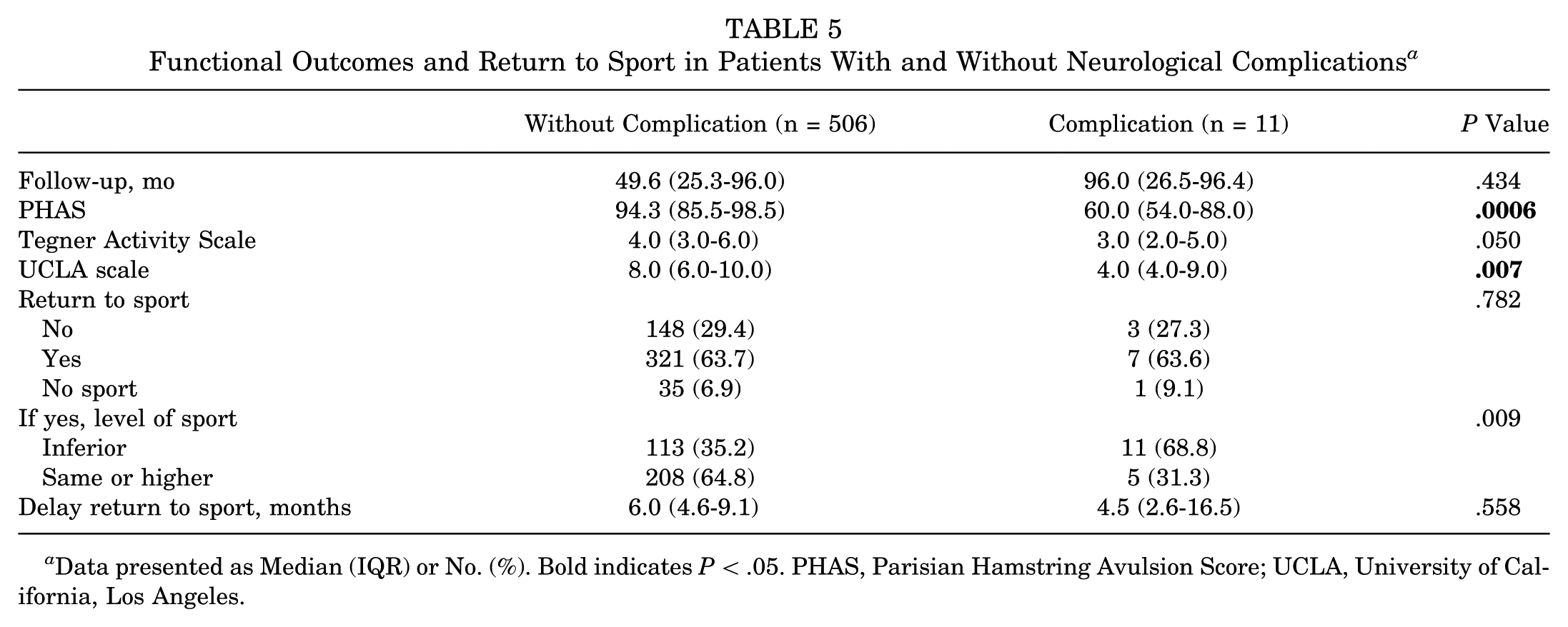
Data presented as Median (IQR) or No. (%). Bold indicates P < .05. PHAS, Parisian Hamstring Avulsion Score; UCLA, University of California, Los Angeles.
Discussion
The main finding of this study is that PHAI surgery is associated with a 4.7% rate of non-rerupture complications and a 10.4% rate when reruptures are included.
These figures align with the literature, as Lawson et al, 8 in their systematic review of 2833 PHAI repairs, reported a 15.3% overall complication rate with 4.6% attributed to major complications. Notably, the Lawson et al review highlighted the variability of specific complication rates: sciatic nerve injuries (1.7%-17.4%), venous thromboembolism complications (0.5%-5.3%), reruptures (1.5%-12.2%), and reoperations (1.1%-16.7%). Minor complications, such as posterior femoral cutaneous nerve injuries, ranged from 0.8% to 45.5%, and postoperative hamstring myopathy ranged from 2.9% to 63.6%. 8 We believe that meticulous identification and protection of the sciatic nerve remain essential, while neurolysis should be limited to cases with fibrotic adhesions or restricted nerve mobility. The choice of incision—vertical or transverse—should balance optimal exposure and cosmetic outcomes while minimizing traction on cutaneous nerve branches. Although most complications were minor and transient, their negative impact on patient-reported outcomes likely reflects the sensitivity of patient-reported outcome measures to discomfort, paresthesia, and delayed functional recovery.
While Lefèvre et al 12 identified chronicity (>32 days delay to surgery) and complete injuries as significant risk factors for rerupture, there is limited research analyzing risk factors for other complications. Our data address this gap, demonstrating that work-related accidents (OR, 5.59; 95% CI, 1.43-37.0; P = .029) and isolated semimembranosus tendon injuries (OR, 12.1; 95% CI, 2.13-227; P = .020) are significant predictors of non-rerupture complications. The higher rate of reported complications in work-related injuries may partly relate to the subjective nature of paresthesia and sensory complaints, as recently discussed by Lefèvre et al 14 in a matched cohort study showing that workers’ compensation status is associated with poorer perceived functional outcomes after proximal hamstring avulsion repair. As for isolated semimembranosus tears, these cases are technically more demanding given their deep and medial location, which makes surgical exposure and neurovascular protection more challenging and may contribute to the higher complication rate observed in these patients. It should be noted that the OR for isolated semimembranosus tendon injuries (OR, 12.1; 95% CI, 2.13-227) presents a wide confidence interval, indicating limited statistical precision because of the small number of cases. Similarly, the finding for work-related accidents (OR, 5.59; 95% CI, 1.43-37.0) also shows a wide confidence interval and should therefore be interpreted with caution.
Interestingly, our study did not identify risk factors for neurological complications, contrasting with findings by Hillier-Smith and Paton, 6 who reported a 3.5% overall rate of sciatic nerve symptoms postoperatively. According to their meta-analysis, chronic repairs (5.1%) and complete injuries (3.6%) were associated with a higher incidence of these symptoms as compared with acute repairs (0.7%) and partial injuries (1.5%), respectively. The low incidence of sciatic nerve complications (0.66%) when compared with rates in the literature (1.7%-17%)4,6,26 may be explained by the study design and inclusion criteria, which excluded revision cases and patients with preoperative motor sciatic palsy. Moreover, all procedures were performed by fellowship-trained surgeons in a high-volume center using a standardized technique. This contributed to the reduced rate observed.
Our deep venous thrombosis rate (0.66%) was lower than that in a recent nationwide database study by Wang et al, 25 who found a venous thromboembolism rate of 2.73% after proximal hamstring repair. Differences may reflect our systematic thromboprophylaxis protocol, the predominantly athletic makeup of our cohort, and the prospective standardized follow-up used in the PHAS registry.
Our data demonstrate that the surgeon's experience, measured by the number of previously performed operations, is not associated with the risk of complications. While this may be expected in open surgery, it should be interpreted prudently. All participating surgeons were fellowship trained and specialized in managing these injuries, and the majority of cases (84%) were performed by 1 senior surgeon, potentially introducing a clustering effect. This uneven distribution limits the statistical power to detect intersurgeon differences, and as such, results regarding experience must be viewed prudently. Notably, in 2 revision cases excluded from the study according to inclusion criteria, patients underwent surgery elsewhere and presented with preoperative motor sciatic nerve palsy, a complication not observed in our cohort. In this view, the Hillier-Smith and Paton meta-analysis reported a 3.5% rate of sciatic nerve injury and identified injury chronicity as a risk factor for this injury. 6
Not surprisingly, our data demonstrate that complications after PHAI repair significantly affect patient-reported outcome measures.
Limitations
This study, while one of the largest cohorts for PHAIs, has a relatively small sample size for certain subgroup analyses. The comparison of functional outcomes should be interpreted cautiously given the small size of the complication subgroup and the potential for type I error. In addition, RTS was self-reported without objective testing, which may introduce bias. The absence of a control group limits direct comparisons. While the study involved multiple operators, this was necessary to evaluate the impact of surgeon experience. Missing data, particularly on functional outcomes, may have influenced the findings. The minimum follow-up for inclusion in the complication and associated condition analysis was limited to 1 year; however, this period is justified as 75% of complications occur within the first 5.5 months postoperatively, ensuring the capture of most relevant events.
Conclusion
PHAI surgery shows a 4.7% complication rate excluding reruptures and 10.4% when reruptures are included, with work-related accidents and isolated semimembranosus injuries identified as significant risk factors for non-rerupture complications. These complications notably impair functional outcomes, as reflected in lower patient-reported outcome measure scores and diminished RTS levels. Moderate to severe sitting discomfort occurs in a minority of patients (~5%) and does not appear directly linked to postoperative complications.
Footnotes
Final revision submitted December 6, 2025; accepted December 9, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: N.L. is a consultant for Websurvey Society, Paris, France. A.H. is a consultant for Arthrex and Depuy. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Pitié-Salpêtrière University Hospital ethics committee.
Data Availability Statement
Data are available from the authors upon reasonable request.