
Abstract
Background:
Surgical treatment of patients with proximal hamstring avulsions provides good results; however, less is known about the outcome in patients who are offered conservative treatment.
Purpose:
To investigate the effect of surgical or conservative treatment (decided by a shared decision strategy) of proximal hamstring avulsions.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A total of 24 patients with magnetic resonance imaging–verified proximal hamstring avulsion were included and had either surgical treatment (11 patients, 45% women; mean age, 50 ± 16 years) or conservative treatment (13 patients, 46% women; mean age, 50 ± 17 years). At baseline, 6 months and 12 months, all patients answered the Perth Hamstring Assessment Tool (PHAT) (0-100 scale) and Hip Sports Activity Scale (0-8 scale). Patients had their maximal hip extension strength and maximal strength at 30° and 90° of knee flexion measured in newton meters per kilogram using a handheld dynamometer. A minimal important change in PHAT was considered >7 points and a minimal important change in strength was considered >0.15 N·m/kg, respectively.
Results:
The surgical group had a shorter time from injury to initiation of treatment compared with the conservative group (median: 15 vs 64 days; P = .02). The surgical group had a greater amount of retraction of the tendons compared with the conservative group (3 vs 2 cm; P = .04). From baseline to 12-month follow-up, the surgical and conservative groups improved their mean PHAT scores (35 points [95 CI, 24-45 points] and 20 points [95% CI, 9-31 points], respectively) reaching a median of 79 points (interquartile range [IQR], 66-95 points) in the surgical group and 75 points (IQR, 66-85 points) in the conservative group at the 12-month follow-up. Their Hip Sports Activity Scale levels at 12 months were 3 points (95% CI, 1-4 points) and 1 point (95% CI, 0-3 points) (not significant). Furthermore, the surgical and conservative groups improved their maximal hip extension strength by 0.61 N·m/kg (IQR, 0.42-0.80 N·m/kg) and 0.62 N·m/kg (IQR, 0.13-1.10 N·m/kg), respectively. Their maximal knee flexion strength at 30° improved by 0.52 N·m/kg (IQR, 0.29-0.74 N·m/kg) and 0.32 N·m/kg (IQR, 0.12-0.52 N·m/kg) and their maximal knee flexion strength at 90° improved by 0.28 N·m/kg (IQR, 0.19-0.37 N·m/kg) and 0.22 N·m/kg (IQR, 0.02-0.41 N·m/kg). At the 12-month follow-up, the side-to-side difference in maximal muscle strength was 6% and 7%, respectively, during hip extension and 19% to 25% and 16% to 17%, respectively, during knee flexion.
Conclusion:
Twelve months after treatment of proximal hamstring avulsion, good clinical outcomes were seen when using a shared decision strategy regardless of whether the strategy led to surgical or conservative treatment.
Keywords
Injuries to the hamstring muscle-tendon complex are among the most common soft tissue sporting injuries and occur during running or slipping accidents.2,9,14 Most often, hamstring muscle injuries occur in the muscle belly, while proximal and distal tendon injuries are less common. 14 The proximal hamstring originates from the lateral aspect of the ischial tuberosity and is composed of the semimembranosus, semitendinosus, and the long head of the biceps femoris. 4 The m. semitendinosus and long head of the m. biceps femoris together form the conjoint tendon. In very severe injuries, which typically occur with a hyperextended knee and hyperflexed hip, the hamstring tendons (1-3 tendons) are partially or completely avulsed from the ischial tuberosity. This typically results in a large hematoma on the back of the thigh, stiffness, pain during walking and sitting, and loss of strength. 1 Proximal hamstring avulsions have an incidence of 3% to 10% in the elite athlete population. 23 However, proximal hamstring avulsions seem to affect middle-aged, nonelite athlete patients predominantly and degenerative changes in the tendon likely plays a role in the pathogenesis. 7
Treatment of proximal hamstring avulsions depends on the degree of avulsion, time from injury to consultation, level of participation in physical activities, and patient preferences.4,9,23 Patients can be treated either surgically or conservatively. 4 Although a recent systematic review 4 highlighted that surgery seems to result in good outcomes and high patient satisfaction in both partial and complete ruptures, less evidence exists regarding conservatively treated patients.4,9,17 In order to provide the right treatment for the right patient at the right time, it is important to build evidence around different treatment options for different levels of impairment. Hereby we can provide the patients with the best evidence-based treatment that fits their injury. Although some injuries should be treated surgically, others would be better treated conservatively. 11 Conservative treatment of patients could comprise pain control, mobilization, and strength training of the hamstrings. Little evidence exist investigating both treatment options (publication bias), 23 it is of great importance to expand the body of evidence regarding treatment options for patients with proximal hamstring avulsions.
The aim of the study was to investigate the outcome of surgical or conservative treatment (decided using a shared decision strategy) of proximal hamstring avulsions 12 months after initiation of treatment. We hypothesized that both treatment options would provide clinically relevant improvements at the 12-month follow-up.
Methods
Study Design
The study is a prospective cohort study after the Strengthening the Reporting of Observational Studies in Epidemiology statement. 22 All patients gave written informed consent before participation in the study. We followed the Helsinki Declaration II. The Regional Ethical Committee waived the need for ethical approval of the study (case No. 46/2019). Permission to handle data was granted by the data protection committee of the Middle Region of Denmark (ID 1-16-02-75-19). The cohort was registered at ClinicalTrials.gov (NCT03868826) before initiation of the study. Data were collected between 2019 and 2021. The study was performed at Horsens Regional Hospital, Horsens, Denmark.
Patients
Patients were referred from either the emergency department, general practitioners, or other hospitals to our orthopaedic outpatient clinic. The initial clinical examination was performed by a senior consultant in orthopaedic surgery (J.O.S.). The patients went through a thorough clinical examination, including assessment of gait, pain during gait, and ability to flex the knee while standing. Lying supine, the active and passive range of motion of the hip was assessed. Lying prone, the active and passive range of motion of the knee was assessed together with palpation of the injury site and visual inspection of the hematoma. 1 Knee flexion strength was manually assessed at 30° and 90° compared with the contralateral leg. An ultrasound examination was also performed. Magnetic resonance imaging (MRI) was used to visualize the proximal hamstring tendon avulsion(s) and retraction. MRI was conducted using 3 projections: axial, coronal, and sagittal. Scans were described by experienced musculoskeletal radiologists and diagnostic criteria according to numbers of tendons ruptured together with degree of retraction.
Patients were included in the study if they were older than 18 years and had a MRI-verified proximal hamstring avulsion (partial [1 or 2 tendons] or complete [3 tendons]). Exclusion criteria were as follows: conditions that contraindicate muscle strength testing, such as cancer or neurological conditions, and inability to speak or understand Danish.
Interventions
Treatment allocation to either surgery or rehabilitation was based on a shared decision between the patient, a sports physical therapist (K.S.), and the surgeon (J.O.S.). The decision strategy was based upon that of Lempainen et al 11 regarding numbers of avulsed tendons and activity level. Furthermore, we included other injury factors (Table 1).
Factors Related to Treatment Allocation
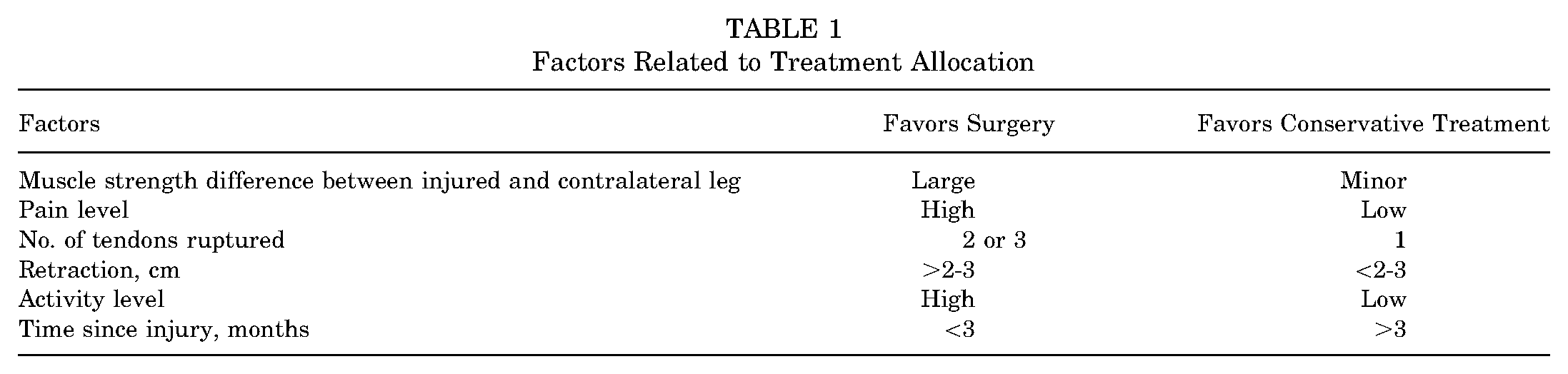
Treatment allocation was, in all cases, based on injury and patient characteristics. Initially, patients with proximal hamstring injuries involving at least 2 tendons, tendon retraction of 2 to 3 cm, substantial physical impairment due to the injury, and sciatic nerve affection were offered surgery. 1 Conservative treatment was primarily offered to physically impaired individuals, in whom time since injury was >3 months. During the study time, however, conservative treatment became more frequently used as the treatment of choice, concurrently with a growing experience in the clinicians with treatment of this rare injury.
Surgical Intervention
Surgery was performed with the patient under general anesthesia and in the prone position. Both hips were supported and both hips were in slight flexion to present the ischial tuberosity. Lower legs were also supported and positioned with slight flexion in the knees. The surgical area was draped so that the affected limb could be freely moved during surgery. An image intensifier was used to identify the correct level and then either a longitudinal or transverse incision was used depending on the degree of tendon retraction. For patients with more retraction, a longitudinal incision was used. Dissection was performed carefully until the hematoma was reached and lavage of the hematoma was performed. The sciatic nerve was identified and spared. The tendon rupture was then identified, and the tendon ends were cleaned. Next, metal screw anchors were inserted into the avulsion site. In each case, 2 to 3 anchors were used and the tendons were sutured down with a “baseball suture” technique. Tension of the sutured tendons was tested. Finally, the wound was carefully closed with surgical staples, and a sterile dressing was placed on the skin. No knee bracing was routinely used postoperatively.
Rehabilitation After Surgery
Patients used crutches for 6 weeks, with increasing weightbearing starting with touchdown of approximately 15 kg for 2 weeks, 15% to 40% weightbearing for weeks 3 to 4, and weightbearing according to the patient's experience of pain for weeks 5 to 6. In 3 cases, the surgeon recommended a knee brace fixed at 90° and no weightbearing for the first 2 weeks to protect the tendon repair. Two weeks after surgery, all patients who had surgery were examined by a specialized sports physical therapist (K.S.) and had staples removed. At 6 weeks postoperatively, all patients were referred to supervised rehabilitation with a local physical therapist, guided by our sports physical therapist (K.S.). Patients were recommended 10 to 12 weeks of sick leave.
All patients receiving surgery followed a specific rehabilitation program consisting of 4 levels. 20 The levels considered the healing of the tendon, the patients’ general health, and the degree of the injury. Progression to the next level was allowed when the patient fulfilled the actual level criteria; however, time since surgery also had to be taken into account (level 1: preoperative to 6 weeks; level 2: 6 weeks postoperatively; level 3: initiation usually 3 months postoperatively; and level 4: initiation 4 to 5 months postoperatively). Further details are listed in Supplemental Table S1.
Conservative Treatment
Patients who were treated conservatively began supervised rehabilitation as soon as possible after the diagnosis was confirmed with a local physical therapist. The local physical therapist was advised to follow the same rehabilitation protocol as the surgically treated patients (please, see section ‘Rehabilitation After Surgery’). In the beginning, patients were advised not to perform hyperflexion of the hip in combination with hyperextension of the knee to avoid stretching on the injured tissue.
Outcomes
Patient-Reported Outcomes
The Perth Hamstring Assessment Tool (PHAT)3,16 was used to investigate patient symptoms. PHAT was originally developed in Perth, Australia, for patients with hamstring problems. It has been translated and cross-culturally adapted into Danish. 21 PHAT investigates pain and limitations. PHAT consists of 3 questions describing pain on a visual analog scale (VAS) from 0 to 10 during sitting, during walking with long strides, and while relaxing. Thereafter, it follows 3 questions where the patients on a 5-level scale indicate the maximal time possible they can sit on a chair and drive a car and at which level they can run. Finally, the patients indicate the level of soreness at the ischial tuberosity. 16 All the questions are added together in a total composite score in the range of 0-100, with 100 indicating no problems. We calculated a minimal important change (MIC) as 0.5 × standard deviation of the baseline score as conducted in another study. 18 This resulted in a MIC of 7 points on PHAT.
Furthermore, patients completed an overall health VAS (range, 0-100), answering: “Please indicate your overall health today where 0 indicates the worst level of health you can imagine and 100 indicates the best level of health you can imagine.” A MIC was also calculated here as 0.5 × standard deviation of the baseline scores. As 1 group had a larger standard deviation than the other, we took the largest standard deviation in the calculation and ended with a MIC of 11.5 points.
Finally, patients completed the Hip Sports Activity Scale (HSAS) where they had to rate their preinjury activity level and current activity level on a Likert scale with 0 indicating “No participation in physical activities” and 8 indicating the level of an athlete. 12 We summarised at the level of sport at 12-months follow-up and the percentage of patients who participated in physical activities at the 12-month follow-up.
Objective Measures
Maximal hip extension strength and maximal knee flexion strength at 30° and 90° were measured with a handheld dynamometer (Commander Muscle Testing; By Land). In the prone position, the maximal hip muscle strength of the hip extensors was tested with the hip in 0° and the knee flexed to 90°. Likewise, the patients’ knee flexion strength was measured in the prone position but with the knee flexed to 30° or 90°. The positions for testing hip extension and knee flexion at 90° were conducted following standardized protocols.10,19 We added knee flexion at 30° as we, by experience (both surgeon and physical therapist), knew that in this position it was specifically demanding for the hamstrings to perform maximal torque. Hence, it was interesting to investigate this position along with the standardized positions. The patient's body weight and length of the femur and tibia were measured in meters to adjust maximal muscle strength to newton meters per kilogram. A MIC of 0.15 N·m/kg has been used in another study, which we applied here as well. 8
Statistical Analysis
All data were inspected visually using histograms and normality was tested using the Shapiro-Wilk test. Normally distributed data were presented as mean and standard deviation and statistical tests comparing the 2 patient groups were conducted using unpaired t tests. Nonparametric data were presented with medians and 25th and 75th quartiles, data from before treatment to 6 and 12 months after treatment were compared using the Wilcoxon signed rank test in the groups, and between-group differences (surgical vs conservative treatment) were investigated using the 2-sample Wilcoxon rank-sum (Mann-Whitney U) test. The significance level was set at .05, and Stata 13 (StataCorp) was used for all statistical analyses.
Results
A total of 26 patients were screened. Two patients were excluded as no avulsion was found during surgery, leaving 24 patients. Baseline characteristics are shown in Table 2, and a flowchart of the study is shown in Figure 1.
Baseline Characteristics a

Data are expressed as n, mean ± SD, or median (interquartile range). BMI, body mass index; HSAS, Hip Sports Activity Scale; PHAT, Perth Hamstring Assessment Tool.

Flowchart of patients in the study. *Two patients were excluded as no avulsion was found during surgery. PHA, proximal hamstring avulsion.
Patient-Reported Outcomes
From baseline to follow-up, both patient groups improved their PHAT and overall health (Figure 2 and Table 3) with 92% of patients exceeding MIC in their PHAT and 54% of patients exceeding MIC in their overall health score. At the 12-month follow-up, 100% of patients participated in some sport in the surgical group and 55% (6 patients) were back at the same or higher level of sport than before their injury. For the conservative group, 69% (9 patients) participated in some sport at the 12-month follow-up and 46% (6 patients) participated at the same or higher level of sport than before their injury. Individual data for HSAS are seen in Supplemental Figures S1 and S2.
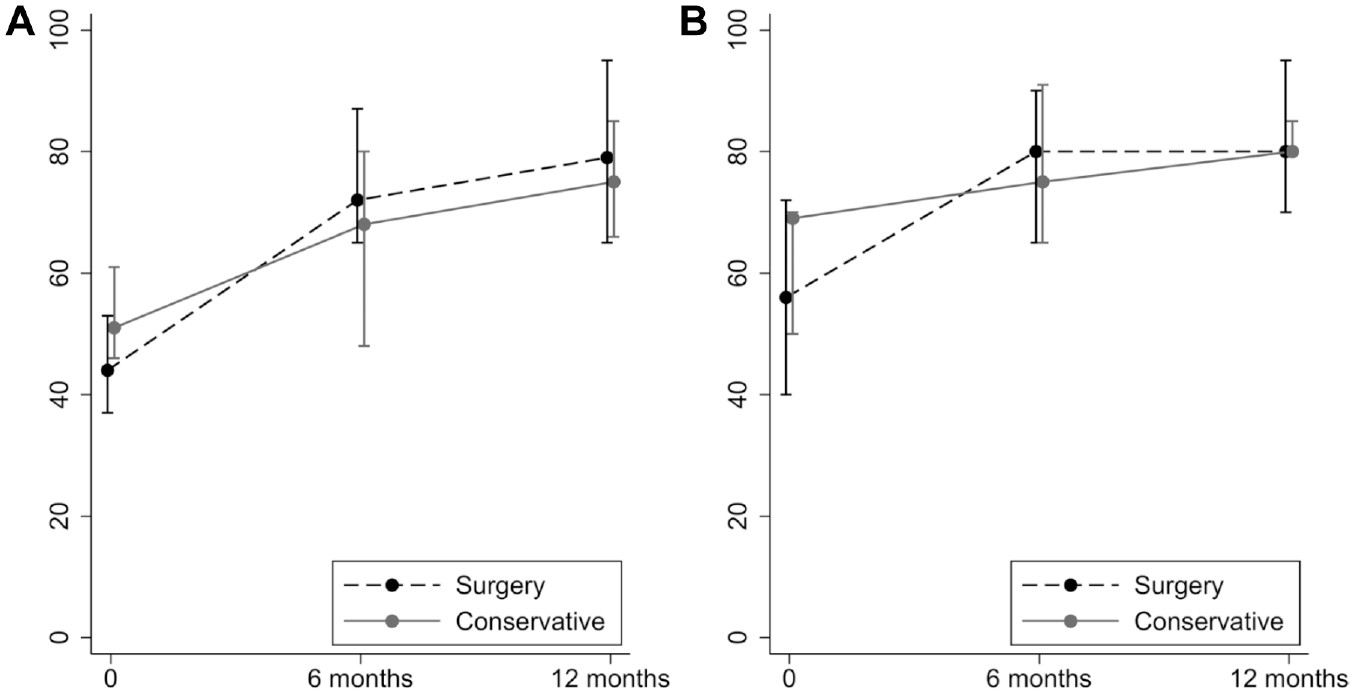
Patient-reported outcomes from baseline to 12-month follow-up. (A) PHAT score (0-100 points). (B) Overall health score (0-100 points). PHAT, Perth Hamstring Assessment Tool.
Outcome Scores With Change Scores From Baseline to 12-Month Follow-up a

HSAS, Hip Sports Activity Scale; IQR, interquartile range; CI, confidence interval; N·m/kg, newton meters per kilogram; PHAT, Perth Hamstring Assessment Tool; VAS, visual analog scale.
Maximal Muscle Strength
Both patient groups improved their hip extension strength and knee flexion strength at 30° and 90° (Table 3 and Figure 3), with 83% of patients exceeding the MIC for maximal hip extension strength, 75% of patients exceeding the MIC for maximal knee flexion at 30°, and 58% of patients exceeding the MIC for maximal knee flexion at 90°. Furthermore, patients’ difference in strength between the affected leg and their contralateral leg was reduced at 12 months (Table 3 and Figure 4).

Maximal muscle strength over time of the affected leg. (A) Hip extension strength. (B) Knee flexion strength at 30°. (C) Knee flexion strength at 90°.

Percent difference in maximal muscle strength between the affected and contralateral legs. (A) Hip extension strength. (B) Knee flexion strength at 30°. (C) Knee flexion strength at 90°.
Discussion
The most important finding from this study is that when using a shared decision strategy, patients with a proximal hamstring avulsion improved in patient-reported outcomes and in functional outcomes 12 months after initiation of their treatment regardless of treatment choice.
Reporting “100” on the PHAT score indicates no problems. At 12 months, the patients in the current study improved much in the PHAT score and the median score reached 79 points (IQR, 66-95 points) in the surgical group and 75 points (IQR, 66-85 points) in the conservative group, indicating that “no problems” was close for some of the patients. Our results are similar to those of van der Made et al, 23 who found that surgical or conservative treatment resulted in good clinical results in a Dutch population of patients when using a shared decision strategy. We used the same rehabilitation program as van der Made et al. 23 Hence, our study adds to the body of evidence using a shared decision-based treatment strategy for patients with a hamstring avulsion and indicating both surgical and conservative treatment strategies provide good results for the patients.
Harris et al 6 and Best et al 2 found that patients having early surgery had better outcomes than those having later surgery. With our study, and that of van der Made et al, 23 it can be speculated that patients with “older injuries” (>3 months since injury) should be offered conservative treatment instead of surgical repair, with the positive results of conservative treatment. This is supported by the finding that fibrotic healing of the avulsed hamstring tendons occurred in conservatively treated patients (MRI proven). 14 However, this should be investigated in a future head-to-head comparison to evaluate which intervention to choose in patients with “older” injuries as specific factors such as a total rupture, high sports participation level, or other patient factors could imply that surgery is a necessity. Furthermore, a study reported acceptable results of repair of chronic injuries though inferior to acute repair. 15
For return to sports, it is considered a rule of thumb to have at least 90% strength of the injured limb compared with the uninjured limb. In this study, median scores for patients in both groups indicated a side-to-side difference <10% for maximal hip extension strength. Hence, patients are reaching healthy goals for rehabilitation for maximal hip extension strength. However, the difference was a bit larger for maximal knee flexion strength (16% to 25%). Hence, the next step in the patients’ rehabilitation process could be to keep building knee flexion strength. This is especially important as Pihl et al 13 found a correlation between higher maximal muscle strength and higher PHAT scores for patients with proximal hamstring avulsion. If patients do not aim for return to sports but more less-demanding activities, a higher side-to-side difference could be accepted, but it would be of great value in general to minimize side-to-side difference in order to obtain a good ability to participate in activities after the injury.
The clinically good results of the conservative treatment found in this study are of high value as some patients might not be surgical candidates. A review by Bodendorfer et al 4 found the mean reported complication rate to be 11% for repairs of partial hamstring avulsions and 29% for repairs of complete hamstring avulsions. Complications reported were rerupture, reoperation, infections, incisional numbness, neurological symptoms, and venous thromboembolism/pulmonary embolism. This indicates that surgery is not without risk and should only be used when deemed necessary.
Interestingly, 2 patients had no tendon ruptures confirmed during surgery despite their MRI scan suggesting major injury (retraction of 10-11 cm) and ruptured tendons. This opens the discussion of using imaging modalities during diagnostics: how certain are we that a positive scan equals a certain diagnosis? MRI is a great tool to visualize muscle injuries, and a positive MRI scan of the hamstrings is associated with a longer recovery period after injury 5 ; however, it should be investigated in future studies how certain the diagnosis is.
Strengths and Limitations
Some of the strengths of the current study are that we conducted a consecutive cohort study investigating patients treated for hamstring avulsion over a period of 2 years. Furthermore, we had full participation in the cohort with no patients declining to participate and we used scores validated for the patient group (PHAT) and functional tests measured both before and after initiation of treatment.
The study has some limitations. First, it has a small sample size. Avulsion of the hamstring is a rare injury; hence, it is difficult to get a large sample size despite recruiting from a large part of the country. Second, we did not have posttreatment imaging of the patients. Hence, we cannot evaluate the state of the hamstrings after treatment. Third, while surgical patients had a 2-week and 6-week control at the hospital, patients in the conservative group were followed by a local physical therapist near their hometown during their entire rehabilitation period. Though encouraged to use the recommended rehabilitation program, we cannot know how closely the physical therapist followed the program in the first 6 weeks. However, surgical patients were also followed near their hometown after the first 6 weeks. Hence, it was only in the first 6 weeks that there was a small difference in their rehabilitation offer. Furthermore, our results suggest that the provided rehabilitation resulted in improved outcomes. Although we cannot document the precise treatment the patients had, it seems that the current rehabilitation setup was effective. Fourth, we did not register complications after treatment. Last, there were many confounders affecting the outcome of treatment in the 2 groups. In this study, treatment was not based upon randomization but on a shared decision-making between the surgeon, the physical therapist, and the patient. Hence, from the current study, it cannot be concluded whether one treatment option is better than the other. Using the shared decision strategy with the guidelines in Table 1 seemed to be a good choice for both groups, which had good clinical outcomes, similar to those of van der Made et al. 23
Conclusion
Twelve months after the treatment of proximal hamstring avulsion, good clinical outcomes were seen when using a shared decision strategy regardless of whether the strategy led to surgical or conservative treatment.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671241275656 – Supplemental material for Proximal Hamstring Avulsions: Surgical Versus Conservative Treatment Using a Shared Decision-Making Strategy
Supplemental material, sj-pdf-1-ojs-10.1177_23259671241275656 for Proximal Hamstring Avulsions: Surgical Versus Conservative Treatment Using a Shared Decision-Making Strategy by Kasper Spoorendonk, Marie Bagger Bohn, Jens Ole Storm, Bent Lund and Signe Kierkegaard-Brøchner in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted February 20, 2024; accepted March 18, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: The Hede Nielsen Family Foundation supported the presentation of the study. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study as the study investigates current practice.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.