
Abstract
Background:
Quadriceps tendon autografts are increasingly used for anterior cruciate ligament reconstruction (ACLR), harvested either with a patellar bone block (quadriceps tendon bone block [QTBB]) or as an all–soft tissue graft (quadriceps tendon soft tissue [QTST]). However, comparative data on outcomes remain limited and heterogeneous.
Hypothesis:
It was hypothesized that there would be no significant differences in patient-reported outcomes, objective stability, return to sports, or complication rates between QTBB and QTST grafts used for primary ACLR.
Study Design:
Systematic review and meta-analysis; Level of evidence, 4.
Methods:
A systematic review of 4 databases (PubMed, Embase, Scopus, and SportDISCUS) was conducted through November 2024. Studies reporting outcomes after primary ACLR using QTBB or QTST autografts were included (Levels 1-4 evidence). Random-effects meta-analyses pooled outcomes for each graft; meta-regression compared grafts while adjusting for follow-up duration and publication year. Risk of bias was assessed using Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I), and certainty of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework.
Results:
A total of 44 studies (n = 2083; QTBB = 1104; QTST = 979) met the inclusion criteria with a mean follow-up of 29 months. International Knee Documentation Committee scores averaged 79.7 (95% CI, 74.8-84.6) for QTBB and 85.4 (95% CI, 80.9-89.8) for QTST autografts (β = 5.2; P = .11). There were no significant between-group differences in Lysholm, Tegner, or Knee injury and Osteoarthritis Outcome Score subscale scores. Instrumented laxity (KT-1000/2000) was higher for QTBB (1.75 mm [1.30-2.21]) versus QTST grafts (0.50 mm [0.35-0.65]) (β = −1.25 mm; P = 0.087), although this difference was not statistically significant and QTST results were driven by a single high-volume cohort. No significant differences were found in Lachman, pivot-shift, or anterior drawer grades. Return to sports (RTS) rates were 82% for QTBB and 81% for QTST grafts (P = .82). Graft failure (both 6%), anterior knee pain (8% vs 7%), and infection (~1%) rates were comparable (all P > .70). Heterogeneity was high for patient-reported outcome measures (I2 >75%) but low for complications. Most studies had a moderate risk of bias, and the certainty of evidence was graded as very low across outcomes due to inconsistency, imprecision, and the observational nature of included studies.
Conclusion:
This systematic review and meta-analysis found no clinically meaningful differences in short-term patient-reported outcomes, graft integrity, RTS rates, or complications between QTBB and QTST grafts in primary ACLR.
Keywords
Anterior cruciate ligament (ACL) rupture is one of the most frequent and function-limiting knee injuries,3,46 with an annual United States incidence of ≈69 per 100,000 inhabitants, equating to >200,000 new cases each year. 6 Injuries cluster in adolescents and young adults who participate in pivoting or cutting sports, and women are disproportionately impacted.37,55 Although nonoperative care is appropriate for some, surgical reconstruction remains the standard for restoring knee stability and enabling return to sports (RTS), with a typical postoperative rehabilitation lasting 9 to 12 months. 16
Among the many technical and patient-related variables that influence surgical success, graft selection is among the most powerful and modifiable.41,49 In addition to tunnel positioning, concomitant meniscal pathology, and demographic variables, graft choice independently predicts revision risk and functional recovery.41,49 Historically, bone-patellar tendon-bone (BPTB) and hamstring tendon (HT) autografts dominated clinical practice. During the past decade, however, the quadriceps-tendon (QT) autograft has gained popularity as it provides comparable stability, patient-reported outcome measures (PROMs), and failure rates while producing less anterior-knee pain and donor-site morbidity than BPTB.1,25,50
Two distinct QT constructs are now available. A QT with patellar bone block (QTBB) offers bone-to-bone healing in the femoral tunnel and a robust cortical fixation site but creates a small patellar defect. Alternatively, an all–soft tissue QT (QTST) eliminates bony harvest, simplifying graft preparation and avoiding the risk of patellar fracture while relying on soft tissue–to–bone healing. Early comparative studies report similar graft-rupture rates and functional scores,45,46 but isolated series describe modest superiority of QTST in the Knee injury and Osteoarthritis Outcome Score subscales, or of QTBB in pivot-shift control. 34 Evidence remains fragmented: PROMs are variably reported, complications such as anterior knee pain, arthrofibrosis, or deep vein thrombosis (DVT) are rarely synthesized, and most previous reviews pool the 2 QT constructs together, preventing construct-specific inference.
Although both QTBB and QTST grafts have demonstrated promising results, previous syntheses have notable limitations. Crum et al 8 conducted a dedicated systematic review comparing these 2 constructs but included only 9 studies totaling 399 patients, focusing primarily on failure rates, pivot-shift testing, and objective laxity. Although PROMs were extracted, they were not quantitatively pooled or meta-analyzed. Since that publication, at least 8 additional primary studies—including large-scale national registry analyses encompassing over 1000 QT reconstructions— have been published, substantially expanding the available PROM and complication data.34,48,54
Accordingly, the purpose of this systematic review and meta-analysis was to compare both patient-reported and objective outcomes after primary ACL reconstruction (ACLR) using QTBB versus QTST autografts. This study incorporates the most recent data and uses meta-regression techniques to adjust for differences in study follow-up and era. We hypothesized that the QTBB graft would demonstrate statistically significant but not clinically meaningful differences in PROMs compared with the QTST graft, owing to its advantage in bone-to-bone healing.
Methods
Protocol and Reporting
This review was conducted and reported in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Although the protocol was not registered with the International Prospective Register of Systematic Reviews (PROSPERO), a prespecified protocol was developed and finalized before screening initiation, and no deviations were made during the study. This protocol defined the eligibility criteria, search strategy, data extraction methods, and planned analyses.
Literature Search
A comprehensive search was conducted by a medical librarian (S.H.) in 4 electronic databases (PubMed, Embase, Scopus, and SportsDISCUS) on May 1, 2020, and updated on November 13, 2024. The search strategy, detailed in the supplementary materials (Supplementary Table 1), included a combination of keywords and appropriate controlled vocabulary related to quadriceps tendon autografts, with any mention of bone. Given the low yield of initial searches, the concepts for ACLR and outcome measures were not included in the search; thus, they could be included via screening. All results were imported into EndNote and screened using the Covidence platform (Veritas Health Innovation Ltd). Duplicate entries were removed automatically by Covidence, and 2 reviewers (A.T. and T.K.) independently screened all retrieved records in duplicate, first by title and abstract, then by full text. Discrepancies at either stage were resolved through discussion, with consensus reached in all cases (Figure 1)
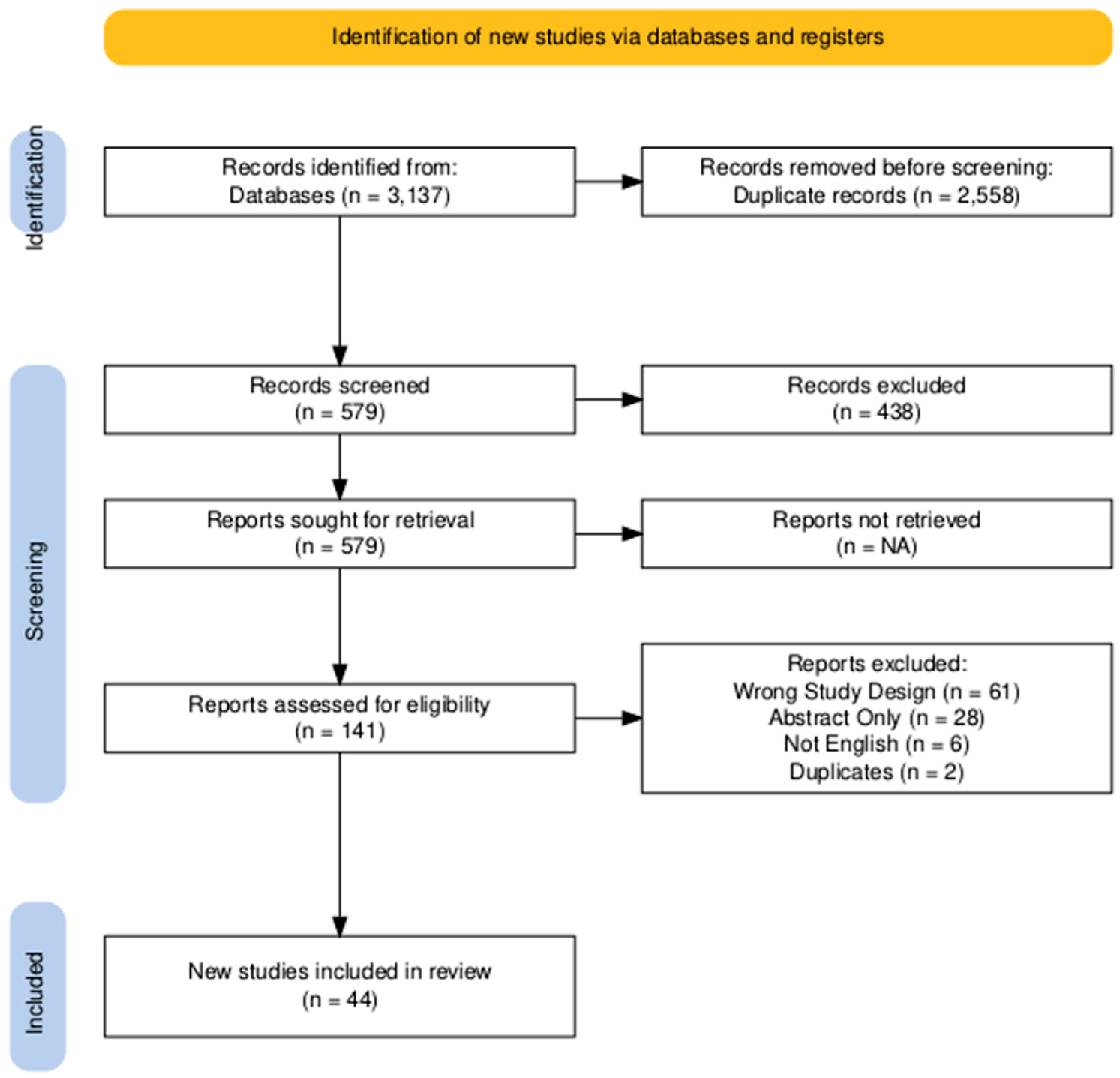
PRISMA flowchart of included studies. 17 NA, not applicable; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Eligibility Criteria
Studies were included if they (1) reported on primary ACLR using QT autografts with or without a bone block (QTBB vs QTST); (2) were published in English or included an English translation; (3) had a level of evidence between 1 and 4; and (4) reported quantitative data on PROMs, objective knee stability measures, RTS, or postoperative complications. Studies were excluded if they involved skeletally immature pediatric patients undergoing nontransphyseal techniques, revision ACLR, multiligament ACLR, combined graft constructs, or if they did not clearly distinguish between QTBB and QTST grafts. Studies including adolescent patients undergoing transphyseal ACLR with mature or maturing physes were eligible for inclusion. Case reports, reviews, abstracts, non-English studies without translation, and studies lacking quantitative data extractable from the text were also excluded. For quantitative analysis, only studies reporting extractable numerical data (eg, means with standard deviations or proportions with sample sizes) were included.
Outcomes
Primary outcomes were PROMs—including the International Knee Documentation Committee (IKDC), Lysholm, Tegner, and Knee injury and Osteoarthritis Outcome Score (KOOS) subscales. Secondary outcomes included side-to-side difference in KT-1000/2000 testing, pivot-shift grades, return to sport, graft failure, and complication rates. Continuous outcomes were extracted from reported summary statistics as mean and standard deviation values. Only studies that reported continuous outcomes as means with corresponding standard deviations were eligible for inclusion in the pooled meta-analysis. Binary outcomes were extracted as event counts and total sample sizes.
Statistical Analysis
For each outcome, a random-effects meta-analysis was conducted using the restricted maximum likelihood estimator to account for both within- and between-study heterogeneity. Separate 1-arm meta-analyses were performed for the QTBB and QTST groups. Between-group comparisons were conducted via indirect meta-regression, with graft type as a categorical moderator and follow-up duration (in months) and study publication year as continuous covariates. The Mantel-Haenszel method was used to compute pooled proportions and odds ratios when applicable.
Forest plots were generated for each outcome to display pooled estimates and 95% CIs. Heterogeneity was assessed using the I2 statistic and the Cochran Q test. Meta-regression results were summarized with β coefficients, confidence intervals, and P values. Effect sizes from proportion meta-analyses were reported on the logit scale and back-transformed to the original scale for interpretation.
Study characteristics were tabulated and summarized descriptively.
Risk of Bias Assessment
Risk of bias was evaluated using the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I, Version 2) tool, which assesses 7 domains of potential bias: (1) bias due to confounding; (2) bias in selection of participants; (3) bias in classification of interventions; (4) bias due to deviations from intended interventions; (5) bias due to missing data;(6) bias in measurement of outcomes; and (7) bias in selection of the reported result.
Given that all included studies investigated primary ACLR using quadriceps tendon autografts, certain domains, specifically, bias due to confounding, classification of interventions, and deviations from intended interventions, were considered less likely to introduce variability in this context. Accordingly, our formal assessment focused on the 4 most pertinent domains: participant selection, missing data, outcome measurement, and selective reporting.
Each study was independently assessed by 2 reviewers (A.T. and T.K.), with discrepancies resolved through discussion and consensus. No third-party adjudication was required. Following ROBINS-I guidance, the overall risk of bias for each study was determined by the highest level of risk recorded in any single domain.
Domain judgments were operationalized as follows:
Low risk indicated that the study met all criteria for minimizing bias in that domain, with no evident methodological limitations.
Moderate risk was assigned when a study had minor limitations or unclear reporting that might influence interpretation but were unlikely to substantially bias results.
Serious risk denoted clear methodological flaws, such as selective outcome reporting, substantial attrition, or poorly described outcome assessment methods, that could plausibly distort study findings.
A rating of critical risk would indicate severe methodological limitations that rendered study results unusable for inference.
Certainty of Evidence
Certainty in the body of evidence for each outcome was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework. For each outcome, evidence from randomized trials was initially considered high certainty, and evidence from observational studies was initially regarded as low certainty, with subsequent downgrading based on 5 domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. Observational evidence could be strengthened if large effect sizes, dose-response relationships, or plausible confounding were present. Two reviewers (A.T. and T.K.) independently performed GRADE assessments, and disagreements were resolved by consensus. Certainty ratings (high, moderate, low, or very low) were assigned for each outcome.
Sensitivity Analyses
Sensitivity analyses were not performed due to the limited number and heterogeneity of included studies, which precluded meaningful subgroup exclusions. Moreover, given that the certainty of evidence across outcomes was already rated very low, additional sensitivity testing would not have materially changed the overall conclusions.
Software
All statistical analyses were performed using R 4.4.3 (R Foundation for Statistical Computing), including the metafor and meta packages for meta-analysis and meta-regression. Template data extraction forms, extracted data, and analytic code are available from the corresponding author upon reasonable request.
Results
Study and Patient Characteristics
A total of 44 studies were included, encompassing 2083 patients who underwent ACLR using quadriceps tendon autografts: 1104 with QTBB and 979 with all–soft tissue constructs (QTST). †† The included studies varied in design, with most being retrospective cohort studies, supplemented by several prospective series and registry-based investigations (Table 1).
Study-Level Characteristics a
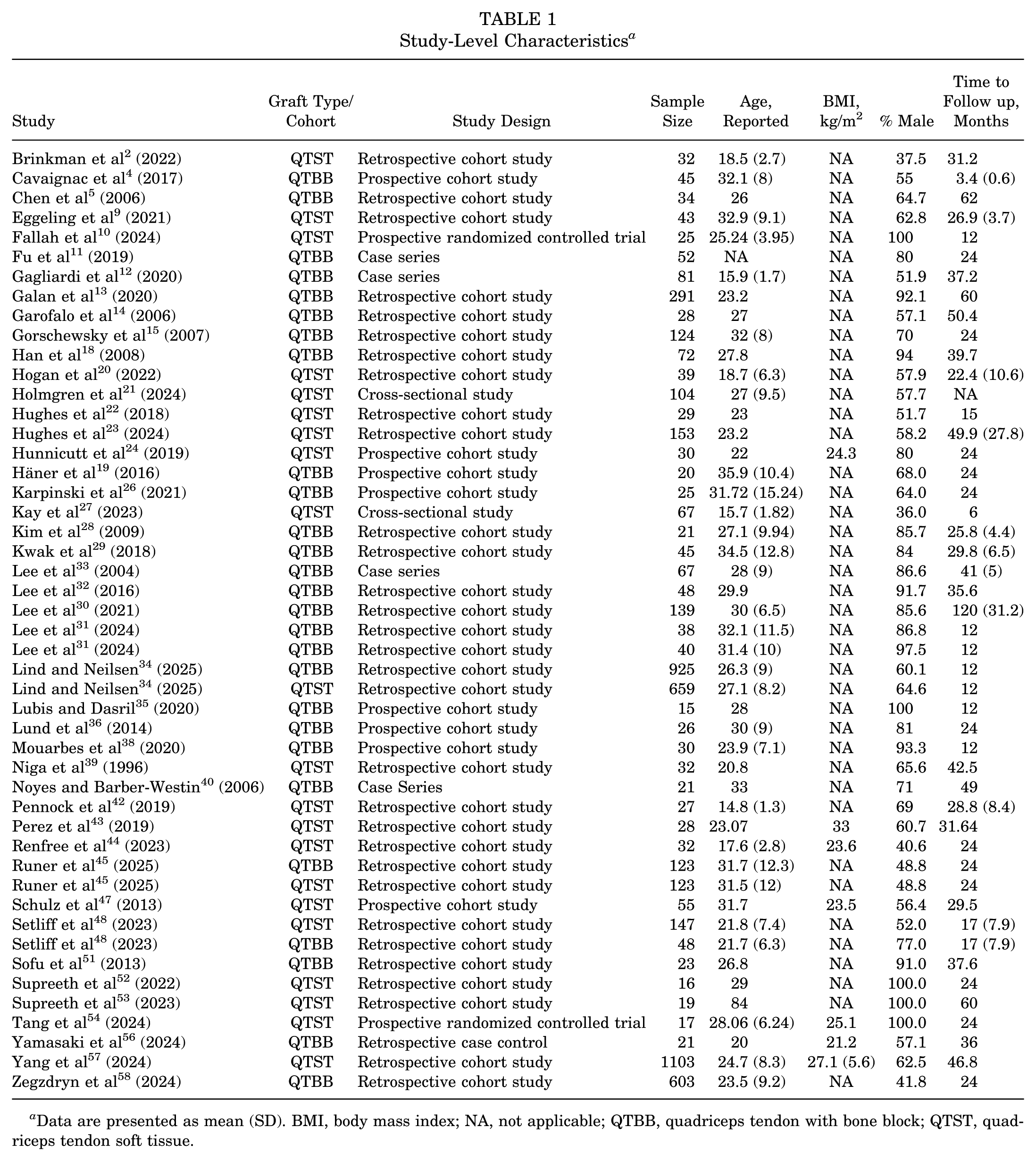
Data are presented as mean (SD). BMI, body mass index; NA, not applicable; QTBB, quadriceps tendon with bone block; QTST, quadriceps tendon soft tissue.
Studies that initially appeared to meet the inclusion criteria but were excluded after full-text review are listed in Supplementary Table 2, along with the specific reasons for exclusion. Considerable heterogeneity was observed in surgical technique, reporting methods, and follow-up duration, with sample sizes ranging from 15 to 1103 patients (Table 1).
Baseline patient-level characteristics are shown in Table 2. The mean age was slightly higher in the QTBB group than in the QTST group (28 vs 26.7 years; P = .027). The proportion of male patients was similar between groups (75% vs 65%; P = .085). Follow-up duration was comparable, with QTBB and QTST studies reporting a mean of 31 and 27 months, respectively (P = .6). Due to inconsistent reporting, body mass index data were not analyzed between groups.
Overall Patient Level Characteristics a
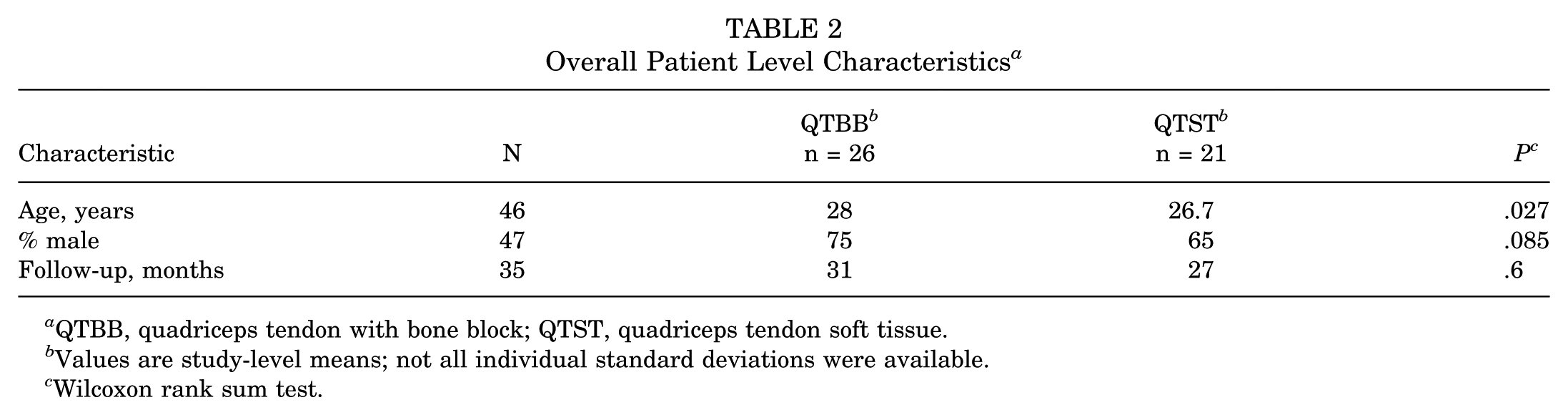
QTBB, quadriceps tendon with bone block; QTST, quadriceps tendon soft tissue.
Values are study-level means; not all individual standard deviations were available.
Wilcoxon rank sum test.
Patient-Reported Outcome Measures
International Knee Documentation Committee
Pooled IKDC scores indicated good outcomes for both graft types: 80.2 (95% CI, 75.8-84.6) for QTBB grafts and 85.4 (95% CI, 80.9-89.8) for QTST grafts. ‡‡ The between-group difference was not statistically significant in random-effects meta-regression (β = 5.2 [95% CI, −1.1 to 11.4]; P = .11), although heterogeneity was high (I2 90.7% for QTBB, 92.4% for QTST) in both subgroups (Table 3).
Pooled Outcomes by Graft Type a
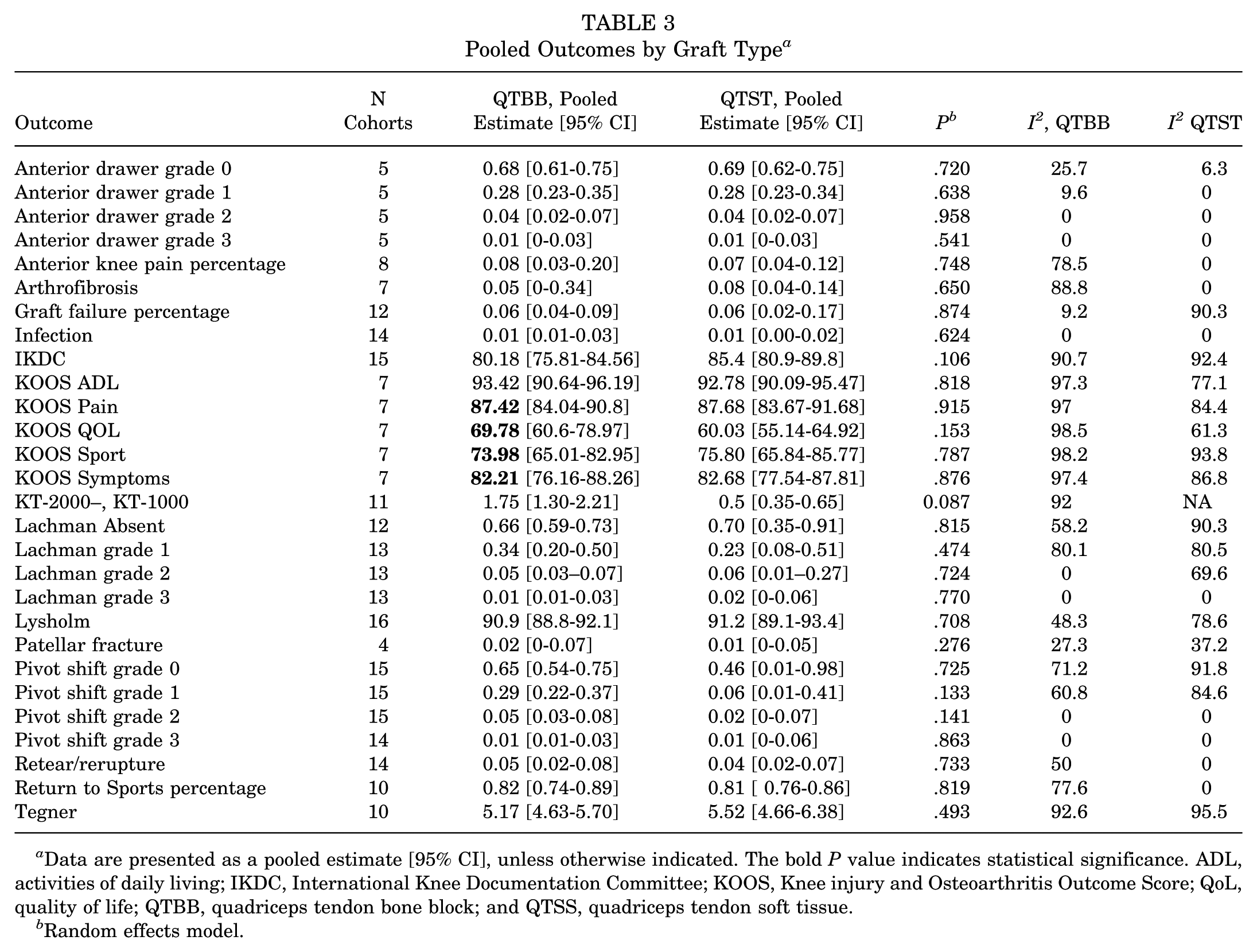
Data are presented as a pooled estimate [95% CI], unless otherwise indicated. The bold P value indicates statistical significance. ADL, activities of daily living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; QoL, quality of life; QTBB, quadriceps tendon bone block; and QTSS, quadriceps tendon soft tissue.
Random effects model.
Lysholm Scores
Lysholm scores were similarly high: 90.9 (88.8–92.1) for QTBB and 91.2 (89.1–93.4) for QTST grafts. §§ No statistically significant difference was found (β = 0.30[ 95% CI −1.42 to 2.03]; P = .71), although heterogeneity remained moderate to considerable (I2 = 48%, 79%, respectively) (see Table 3).
Tegner Scores
Tegner activity scores were comparable: 5.17 (4.63–5.70) for QTBB and 5.52 (4.66–6.38) for QTST grafts, with no significant subgroup difference (β = 0.35 [95% CI, −0.67 to 1.38]; P = .49). ‖‖ heterogeneity was also present (I2 >90 %) (see Table 3).
KOOS Scores
Across the 5 KOOS subscales (Pain, Symptoms, Activities of Daily Living [ADL], Sport, and Quality of Life [QoL]), no significant differences were observed between QTBB and QTST.4,9,19,20,24,26,34,36,58 KOOS Pain scores were high in both groups: 86.8 (82.7–90.9) for QTBB and 87.7 (83.7–91.7) for QTST grafts (β≈ 0.9; P = .76). KOOS-Symptoms, ADL, and Sport also demonstrated similar group means with high heterogeneity in nearly all analyses (I2 >80%). KOOS-QoL scores were 69.8 (60.6–79.0) for QTBB and 60 (55.1–64.9) for QTST, favoring QTBB, but the between-group difference did not reach statistical significance (β = −8.3 [95% CI −21.5 to 4.9]; P = .21). (see Table 3).
KT-1000/2000 Difference
KT-1000/2000 anterior laxity measurements revealed reduced residual laxity in the QTST group. Pooled side-to-side translation was 1.75 mm (1.30–2.21 mm) for QTBB versus 0.50 mm (0.35–0.65 mm) for QTST grafts. ¶¶ Due to limited QTST data for KT-1000 measurements (single study), between-group comparisons were conducted via meta-regression rather than traditional subgroup analysis. No significant between-group difference was identified in meta-regression (β = −1.25 mm [95% CI −2.69 to 0.18]; P = 0.087) (Table 3).
Return to Sports
The pooled proportion of RTS was high in both groups: 82% (74–89%) in the QTBB group and 81% (71–88%) in the QTST group.2,12-14,33,44,45,48 No significant subgroup difference was detected in the random-effects model (β = 0.02 [95% CI, −0.10 to 0.13]; P = .74), with moderate heterogeneity across studies (I2 = 77.6% and 0% for QTBB and QTST, respectively). Although a few studies reported mean time to RTS, too few provided standard deviations to allow for pooled quantitative comparison between graft types (Table 3, Figure 2).

Forest plot of meta-analysis for RTS percentage. QTBB, quadriceps tendon–bone block; RTS, return to sport.
Complications Rates
Graft Failure
Graft failure rates were similar between graft types, 6% (4%-9%) for QTBB and 6% (2%-17%) for QTST groups, with no statistically significant difference between the 2 groups (β≈ 0.00 [95% CI, −0.12 to 0.12]; P = .87) ## (Table 3, Figure 3).

Forest Plot of meta-analysis for graft failure percent. QTBB, quadriceps tendon–bone block.
Anterior Knee Pain
Anterior knee pain was also comparable: 8% (6%-12%) after QTBB and 7% (4%-12%) after QTST (β = −0.01 [95% CI, −0.40 to 0.38]; P = .75)10,13,18,19,22,31,51 (Table 3, Figure 4).
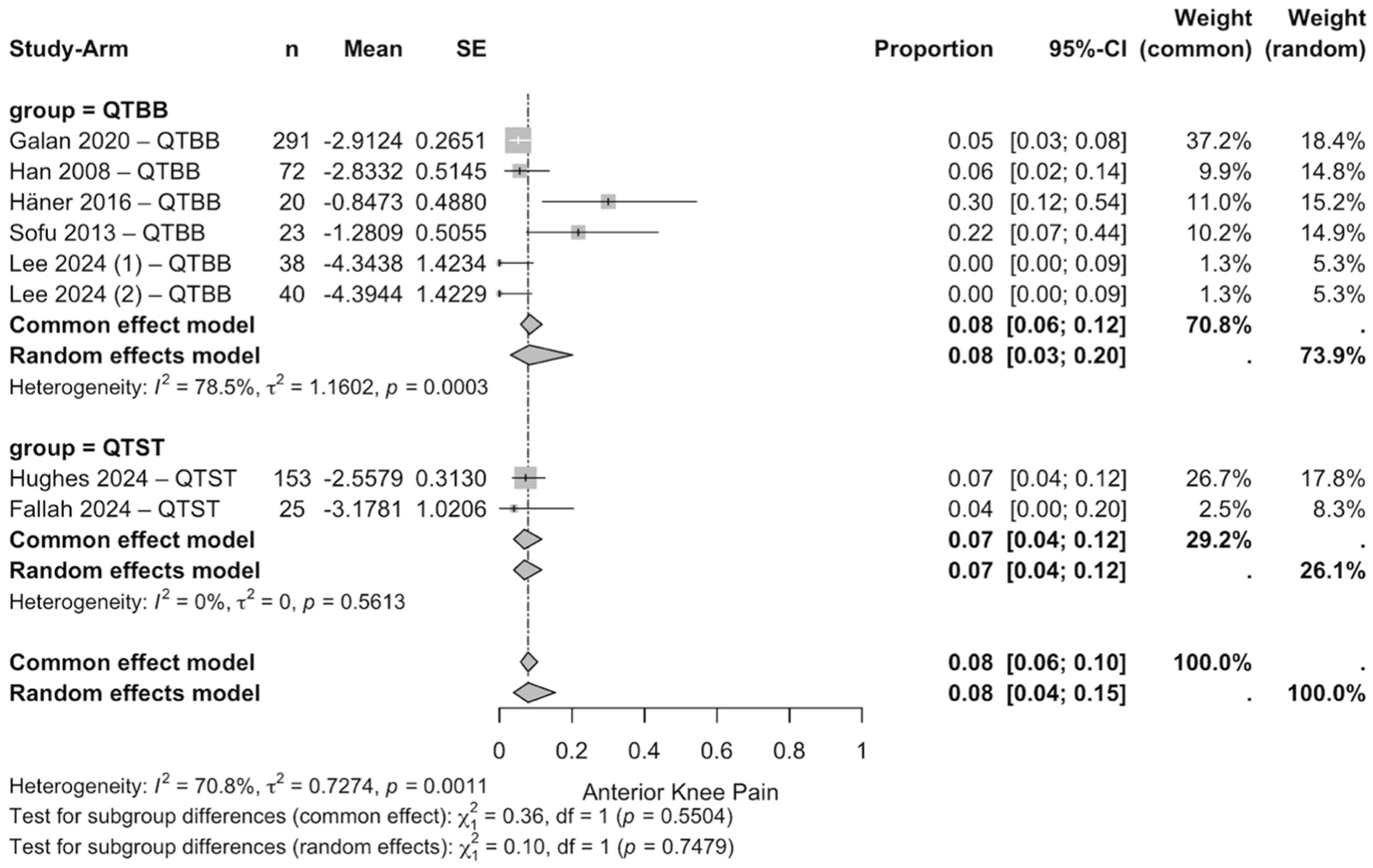
Forest plot of meta-analysis for the percentage of anterior knee pain. QTBB, quadriceps tendon–bone block; QTST, quadriceps tendon soft tissue.
Patellar Fracture
Patellar fracture was an uncommon complication in both groups, with pooled rates of 2% (0%-7%) after QTBB and 1% (0%-5%) after QTST (β≈−0.01 [95% CI −0.04 to 0.01]; P = .28).30,45,48 Between-study heterogeneity was low for both graft types (I2 = 27% for QTBB, 37% for QTST) (see Table 3).
Infection
Postoperative infection after ACLR with a quadriceps graft is rare (≈1%) and virtually identical whether the graft is harvested as a bone block (QTBB) or an all–soft tissue strip (QTST). a No statistical heterogeneity was detected within either graft subgroup (I2 = 0%), and the random-effects test for subgroup differences was nonsignificant (P = .62) (Table 3, Figure 5).

Forest plot of meta-analysis for infection percent. QTBB, quadriceps tendon–bone block; QTST, quadriceps tendon soft tissue.
Special Tests
Lachman Test
Lachman grading was similar across groups. Grade 0 Lachman results were observed in 66% (59%-73%) of the QTBB group and 70% (35%-91%) of the QTST group (P = .81).4,9,10,14,28-33,47 Higher-grade Lachman findings were infrequent and did not differ statistically between groups (see Table 3).
Pivot Shift Test
Pivot shift findings mirrored this pattern. A grade 0 pivot shift was present in 65% (54%-75%) of patients in the QTBB group and in 46% (1%-98%) of patients in the QTST group (P = .72). b Higher-grade instability (Grades 2-3) occurred in ≤5% of patients in both groups (see Table 3).
Anterior Drawer Test
Anterior drawer test outcomes were consistent across all grades: 69% of patients had grade 0 laxity, 28% had grade 1, and only 4% were classified as grade 2 or 3, with no significant differences by graft type.10,29,30,32,33 Heterogeneity was minimal in most strata (I2 < 10%) (see Table 3).
Risk of Bias
Of the 44 individual studies included in the analysis, 3 (7%) were judged to have an overall low risk of bias, 35 (79%) moderate risk, and 6 (14%) serious risk (Table 4). The most frequent sources of bias were related to outcome measurement and result reporting, which were rated as moderate or serious in 75% and 77% of studies, respectively. Missing data was less commonly problematic, with 45% of studies rated as low risk in this domain. Notably, no study was rated as having a critical risk of bias in any domain. Studies at low risk across all domains (eg, Fu et al, 11 Fallah et al, 10 and Lund et al 37 ) were typically recent and prospective, with standardized outcome reporting and minimal attrition. In contrast, studies such as Galan et al, 13 Holmgren et al, 21 Kim et al, 28 Lee et al, 33 Lind and Nielsen 34 and Perez et al 43 exhibited serious risk of bias due to issues including unblinded outcome assessment or incomplete reporting.
Risk of Bias Summary a

ROBINS-I-V2, Risk Of Bias In Non-randomized Studies of Interventions, Version 2.
Certainty Assessment
When formally assessed with the GRADE framework, the certainty of evidence supporting comparative conclusions between QTBB and QTST was limited (Table 5). KT-1000/2000 laxity showed numerically lower values in QTST, but this difference did not reach statistical significance (P = 0.087), and the certainty was rated low due to heterogeneity, imprecision, and reliance on a single QTST cohort. For functional outcomes (IKDC, Lysholm, KOOS, Tegner), the evidence was very low certainty, reflecting high inconsistency (I2 > 80%-90%) and imprecise estimates. RTS proportions were high in both groups, but the certainty of the evidence was very low, given moderate heterogeneity and confidence intervals spanning both potential benefit and harm. Complication outcomes, including graft failure and anterior knee pain, were similarly rated as having very low certainty due to sparse data and inconsistent reporting across studies. Collectively, these findings suggest that while trends can be identified, confidence in the robustness and generalizability of these pooled estimates remains limited.
Summary of Findings (GRADE): QTST Versus QTBB in Primary ACLR a

ACLR, anterior cruciate ligament reconstruction; AKP, anterior knee pain; GRADE, Grading of Recommendations Assessment, Development and Evaluation; IKDC, International Knee Documentation Committee; MD, mean difference; QTBB, quadriceps tendon–bone block; QTST, quadriceps tendon soft tissue; and RD, risk difference; RTS, return to sport.
Risk of bias & inconsistency (−1): Evidence base predominantly nonrandomized cohorts (ROBINS-I assessed) → observational starting point. Very high heterogeneity within groups (I2≈ 92%-95%); downgraded 1 level for inconsistency.
Inconsistency (−1): Substantial heterogeneity across cohorts (eg, RTS I2≈ 71%; graft failure QTST I2≈ 90%; AKP overall I2≈ 71%-79%). Effect directions vary, and prediction intervals are wide.
Imprecision (−1): 95% CIs for the comparative effect span both clinically important benefit and harm (and rare events have few total events); thus, we downgraded for imprecision.
Absolute effect: Baseline risk = pooled QTBB random-effects proportion; QTST absolute difference is the RD × 1000 with its 95% CI.
The pooled QTBB mean was subtracted from the pooled QTST random-effects mean. The 95% CI for the between-group mean difference was calculated by propagating the standard errors from each group's pooled confidence interval using an independent-groups approximation.
For dichotomous outcomes, the risk difference (QTST − QTBB) was calculated from the random-effects pooled proportions. The 95% CI was approximated by combining the standard errors from each group's pooled confidence interval using an independent-groups approximation. Baseline risks were taken from the QTBB pooled proportions.
Discussion
This systematic review and meta-analysis of 44 studies encompassing 2083 primary ACLRs found that QT autografts harvested with a patellar bone block (QTBB) and those harvested as an all–soft tissue strip (QTST) yield equivalent short-term clinical outcomes. IKDC, Lysholm, Tegner, and all 5 KOOS subscores were statistically indistinguishable between constructs, as were RTS rates (≈81%), graft-failure rates (6%), anterior-knee pain (7%-8%), patellar fracture (1%-2%), and infection (≈ 1%). Although QTST showed numerically smaller side-to-side KT-1000/2000 laxity (0.5 vs 1.75 mm; P = 0.087), this trend was primarily driven by a single large cohort and did not reach statistical significance, and this instrumented difference did not correspond to superior clinical stability based on Lachman, pivot-shift, or anterior drawer testing (Table 3). Taken together, the data suggest that construct choice can be individualized based on surgeon preference and patient-specific factors without compromising early outcomes.
These findings refine and substantially extend the work of Crum et al 8 who, analyzing only 9 studies (n = 399 patients), were unable to meta-analyze patient-reported outcomes and found no clear advantage for either construct in failure or laxity rates. By incorporating 38 additional investigations, including recent national-registry analyses34,57 published in 2024 and 2025, the present review provides the most granular comparison to date. Our results also contextualize a recent registry study reporting slightly less pivot-shift in QTBB reconstructions; 34 the current pooled analysis shows that any rotational-stability benefit is small and clinically uncertain.
From a technical perspective, QTBB affords bone-to-bone healing in the femoral tunnel but introduces a patellar defect and a 2% risk of patellar fracture, whereas QTST eliminates bony harvest at the cost of relying on soft tissue-to-bone healing. Contemporary literature indicates that these theoretical trade-offs do not translate into measurable differences in graft survival, knee stability, or functional recovery. A state-of-the-art review of quadriceps grafts similarly concluded that donor-site morbidity and kneeling pain are low regardless of whether a bone plug is included. 7 Surgeons, therefore, should consider tailoring quadriceps graft choice to factors such as patellar morphology, work-related kneeling requirements, or future revision strategies. For instance, the absence of a patellar defect after QTST may preserve bone-plug options for subsequent procedures, whereas the cortical bony interface of QTBB could theoretically simplify 2-stage revisions. Additionally, in cases where the soft tissue portion of the quadriceps tendon is relatively short (eg, <50 mm), surgeons can be reassured that including a bone block to augment graft length does not appear to increase the risk of anterior knee pain or patellar fracture.
Limitations
This review should be interpreted in the context of several limitations. Most included studies were retrospective and carried moderate or serious risk of bias, which, together with high heterogeneity and imprecision, led to very low certainty of evidence for nearly all outcomes. Variability in rehabilitation protocols, fixation methods, and outcome reporting likely contributed to the observed inconsistency, particularly for patient-reported measures. Follow-up was generally short (<3 years), limiting assessment of graft durability, osteoarthritis progression, and long-term donor-site morbidity. Concomitant meniscal pathology and its treatment were variably reported across studies. While some investigations specifically excluded patients with meniscal tears or repair, others did not document associated injuries, preventing systematic comparison between groups. Similarly, lateral extra-articular tenodesis was rarely reported. These represent potential confounders that may influence stability outcomes and failure rates. A single high-volume cohort largely drove objective laxity estimates for QTST, and few studies reported dispersion measures for RTS timing, preventing pooled analyses of recovery trajectories.
Future Directions
Future research should prioritize well-powered randomized controlled trials directly comparing QTBB and QTST with uniform rehabilitation, magnetic resonance imaging-verified graft maturation, and ≥ 5-year follow-up. Reporting should extend beyond basic PROMs to include validated measures of kneeling pain, donor-site morbidity, cost-effectiveness, and operative time. Imaging or second-look arthroscopy studies could clarify whether biological healing differs between constructs, while stratified analyses might identify patient characteristics (eg, age, activity level, patellar thickness) that meaningfully interact with graft choice.
Conclusion
This systematic review and meta-analysis found no clinically meaningful differences in short-term patient-reported outcomes, graft integrity, RTS rates, or complications between QTBB and QTST grafts in primary ACLR. Pending higher-level comparative data, graft selection may be guided by surgeon experience, intraoperative considerations, and patient-specific anatomy, without expectation of meaningful differences in early clinical outcomes. These considerations underscore the importance of aligning graft choice with patient-specific risk profiles and activity demands.
Supplemental Material
sj-docx-1-ojs-10.1177_23259671261418051 – Supplemental material for No Postoperative Difference Between Bone-Block Versus All–Soft Tissue Quadriceps Tendon Autografts for Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-1-ojs-10.1177_23259671261418051 for No Postoperative Difference Between Bone-Block Versus All–Soft Tissue Quadriceps Tendon Autografts for Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis by Aaron D. Therien, Timothy Kouo, Isabel Prado, Emily J. Luo, Cooper Williams, Jake Reed, Santita Ebangwese, Christian Zirbes, Kevin A. Wu, Clark Bulleit, Stephanie Hendren and Brian C. Lau in Orthopaedic Journal of Sports Medicine
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. Ethical approval was not sought for the present study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.