
Abstract
Background:
Multiligament knee reconstruction is a technically demanding procedure with a steep learning curve and carries the potential for significant complications if technical accuracy is not achieved. Although optimal tunnel trajectories to prevent convergence have been described, it remains unclear how accurately these theoretical trajectories are executed in practice and whether patient-specific guides can improve precision and reduce tunnel convergence.
Purpose:
To evaluate the effectiveness of patient-specific guides in preventing tunnel convergence and improving surgical accuracy in multiligament knee reconstruction.
Study Design:
Controlled laboratory study.
Methods:
Computed tomography scans from a single case were used to create accurate 3-dimensionally printed femur models. Each of the 8 participating orthopaedic surgeons performed tunnel placement on 2 models: 1 using the freehand technique and 1 using a custom-designed guide. Tunnels of the anterior cruciate ligament (single bundle) and posterior cruciate ligament (double bundle consisting of the anterolateral and posteromedial bundles) were constant. Surgeons created femoral tunnels for posterolateral structures (fibular collateral ligament, popliteus tendon) and posteromedial structures (medial collateral ligament, posterior oblique ligament). Postprocedure computed tomography was used to assess tunnel convergence, intertunnel distances (>2 mm defined as safe), and tunnel entry accuracy.
Results:
Lateral tunnel convergence occurred in 11 of 16 tunnels via freehand—primarily between the popliteus tendon and anterior cruciate ligament (7/8)—and none of the patient-specific guide models (0/16; P = .001). Medial convergence was reduced from 10 of 16 via freehand to 2 of 16 via the guide (P = .001), most commonly between the posterior oblique ligament and posterior cruciate ligament–posteromedial bundle. Mean intertunnel distances were significantly greater via the guide. Tunnel entry accuracy was 100% with the guide.
Conclusion:
The use of patient-specific guides significantly reduces tunnel convergence and improves tunnel entry point precision in multiligament reconstruction simulation. Freehand tunneling highlights the prominent influence of human error.
Clinical Relevance:
Surgical success in multiligament reconstruction relies on anatomic graft function, yet tunnel convergence may jeopardize graft integrity and lead to failure. Therefore, avoiding tunnel convergence is of utmost importance for a successful reconstruction.
Multiple-ligament knee injury (MLKI) is defined as the disruption of at least 2 of the 4 cardinal ligamentous structures of the knee: anterior cruciate ligament (ACL); posterior cruciate ligament (PCL); the posterolateral corner (PLC), most notably involving the fibular collateral ligament (FCL) and popliteus tendon (PLT); and the posteromedial corner (PMC), most notably involving the medial collateral ligament (MCL) and posterior oblique ligament (POL). Fortunately, these injuries are rare, accounting for 0.02% to 0.2% of all orthopaedic injuries, and most cases are secondary to knee dislocations arising from high-energy trauma. 5 Various accompanying problems may be encountered, such as meniscal, chondral, and neurovascular injuries.14,22 The inability to return to previous activity levels and progression to osteoarthritis are highly probable.
There is no gold standard treatment of MLKI, and numerous areas of uncertainty exist in the current literature concerning the timing of surgery and appropriate graft selection, reconstruction technique, and tunnel orientation. Nevertheless, recent literature favors surgical reconstruction that promotes better functional and clinical outcomes, as well as a superior rate of return to previous level of activity.1,19,24,25,27,28 Nonoperative treatment of MLKI should be reserved for sedentary patients and polytrauma cases with comorbidities that preclude surgical intervention. 11 Surgical management entails anatomic reconstruction of torn ligaments to attain optimal stability, necessitating the placement of multiple extra- and intra-articular tunnels without convergence.
The challenge in multiple-ligament reconstruction is to fit too many tunnels into a narrow space without convergence. This challenge is mainly faced on the femoral side rather than the tibial side. Convergence of the tunnels can disrupt graft fixation and/or stability, eventually leading to reconstruction failure.7,21 Careful planning and execution of the drilling angles are necessary to prevent tunnel convergence. Various researchers have addressed this issue in different studies, exploring techniques and methodologies to determine the most effective tunnel positioning. Moatshe et al 21 eliminated tunnel collision of the FCL and PLT tunnels to the ACL by directing the tunnel 35° anteriorly. Similarly, collisions were avoided on the medial side when the superficial MCL (sMCL) [40, 40] and POL tunnels [20, 20] were directed anteriorly and proximally. Note that, throughout this study, all tunnel angulations are uniformly expressed in brackets as [axial, coronal] angles. In this format, the axial angulation reflects anterior-posterior deviation within the axial plane, while the coronal angulation indicates proximal-distal deviation within the coronal plane; for example, [40, 20] corresponds to 40° axial (anterior) and 20° coronal (proximal) angulation. However, the position of the tunnel trajectories is adjusted by the previous tunnel positions and still heavily depends on the spatial imagination capacity of the surgeon.
Recent technological developments have significantly increased the accessibility of patient-specific guides (PSGs) and 3-dimensional (3D) printing for orthopaedic surgery, yielding promising results.9,12,31 Replication of previous studies that defined the optimal routes to avoid tunnel convergence via PSGs may combine the potential benefits of PSGs and reduce dependence on surgical competency, thereby enhancing accuracy.
We hypothesized that PSG utilization on the femoral side in multiple-ligament reconstruction may lead to (1) an increased safe distance between tunnels, (2) a reduced tunnel convergence rate, and (3) a more accurate tunnel entry site.
Methods
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. No personal information was disclosed, and all personal data were anonymized to protect the participants’ privacy and confidentiality. All digital data used in this study were in line with the ethical standards of the Institutional Research Committee. This study was approved by the Acıbadem University Ethics Committee (approval 2024-12/516; August 15, 2024).
Establishment of 3D-Printed Model
High-resolution computed tomography (CT) angiography images of the contralateral, uninjured, average-sized knee of a 30-year-old woman with MLKI were obtained for model creation to mimic the original bony anatomy and simulate a lifelike scenario. Images were obtained from a Sectra PACS system with the following parameters: slice thickness, 0.75 mm; matrix size, 512 × 512. Images were processed to generate a mesh volume file. Subsequently, the segmented mesh design was transferred to Fusion 360 (Autodesk Inc) to create a 1:1 size digital 3D model of the patient. A tunnelable digital model was created to represent the worst possible scenario (Schenck KD-4) of knee injury. The senior author subsequently positioned the single-bundle femoral tunnel of the ACL and the double-bundle femoral tunnels of the PCL as constants in the 3D model, as described.4,13,32 Socket sizes of the ACL, anterolateral PCL, and posteromedial PCL were adjusted as 10 × 25, 11 × 25, and 7 × 25 mm, respectively. Subsequently, the FCL, PLT, sMCL, and POL tunnels were incorporated into the digital 3D model according to the specifications outlined by Moatshe et al. 22 Then, the absence of tunnel convergence was verified on the digital 3D model.
3D model printings were performed with an Ultimaker S3 printer by using fused deposition modeling technology and Ultimaker Cura Enterprise software (Version 4.13.2). The optimal variation of infill form, infill percentages, and wall thickness was selected to simulate an actual surgical experience for the sensation of surgical drilling. For printing, Ultimaker PC Transparent material, 0.4-mm nozzle, and 0.1-mm layer height were chosen for more accurate and drillable models. Distal femoral 3D models were printed including the single-bundle ACL and double-bundle PCL tunnels. Then, medial and lateral PSGs with femoral-aiming drill holes that fit on the medial and lateral epicondyles with a 0.1-mm gap were printed (Figure 1).

(A) Creation of the digital 3-dimensional model and placement of the tunnels. (B) Design of the guides according to the plan. (C) Production of the distal femur models and compatible guides.
Procedure
According to power analysis, 8 senior surgeons experienced in multiple-ligament reconstructions were selected for participation in the study. Two identical models were created for each surgeon: one for freehand (FH) and the other for the PSG procedure. Surgeons performed on a single patient model to specifically assess intersurgeon variability and the effect of PSGs under identical anatomic conditions. Before the process, each participant was reminded of the anatomic tunnel entry points and given instructions to avoid tunnel convergence as outlined by Moatshe et al, 21 as well as time to read them. Each participant was then asked to drill lateral (FCL and PLT) and medial (sMCL and POL) tunnels at the prescribed length and orientation on the femoral model, which was fixed parallel to the working table (Figure 2). To ensure methodological consistency and reproducibility, tunnel diameters were standardized across all procedures. These sizes were based on the work of Moatshe et al, which provided safe drilling angles and femoral tunnel dimensions in anatomic PMC and PLC reconstructions (Table 1).15-18,21

Stepwise workflow of the surgical simulation. The process illustrates the sequential phases of the experimental protocol: briefing, planning, and tunnel placement for the lateral and medial tunnels. PSG, patient-specific guide.
Description of the Anatomic Footprint Localization Relative to Anatomic Landmarks a

Relevant anatomic studies are notated. FCL, fibular collateral ligament; PLT, popliteus tendon; POL, posterior oblique ligament; sMCL, superficial medial collateral ligament.
The anatomic description of the tunnel entry points relative to the anatomic landmarks was maintained by the participants throughout the procedure. All participants determined the tunnel entry points by surgical rulers and marker pens. The time taken to decide on the tunnel entry point to the end of the drilling process was recorded as the medial and lateral procedure time. Each participant subsequently performed medial and lateral tunnel preparations by FH and with a custom-made PSG that provided press-fit seating on the medial and lateral epicondyles. Ultimately, 8 participants completed the cycle, and 16 models were evaluated for statistical analysis. All models underwent CT scanning. Tunnel entrance locations, intertunnel distances, and tunnel convergences were evaluated by 2 independent orthopaedic surgeons who did not participate in procedures. The location of each tunnel aperture was assessed through superimposed 3D CT reconstructions, with quantitative metrics of center-to-center distances and geometric overlapping of apertures were computed. An overlap ratio >51% between the intended and actual apertures was judged correct to ensure binary categorical classification (correct/incorrect) for intersurgeon comparison. Tunnels with a minimum distance >2 mm at their nearest point were deemed safe; otherwise, they were defined as converging (Figure 3).6,21

Demonstration of tunnel convergence on computed tomography scans. Corresponding slices were obtained at the same anatomic level to enable direct comparison. Dotted lines indicate tunnel borders. The anatomic structures represented include the anterior cruciate ligament (ACL), fibular collateral ligament (FCL), posterior cruciate ligament–anterolateral bundle (PCL_ALB), and posterior cruciate ligament–posteromedial bundle (PCL_PMB). FH, freehand; PSG, patient-specific guide.
Statistical Analysis
A power analysis was performed in G*Power software (Version 3.1.9.2) to determine the sample size. The calculations yielded an effect size of d = 3.820. To attain 99% power at a significance threshold of α = 0.01, a minimum of 6 groups is necessary. Each pair consisted of 1 model that had undergone the procedure via the FH technique and 1 via a PSG. To account for potential data loss or procedural complications, 2 additional pairs were included, resulting in 8 paired samples. Quantitative variables were presented as mean, standard deviation, median, minimum, and maximum values, while qualitative variables were depicted by descriptive statistical methods, including frequency and percentage. The Shapiro-Wilk test and box plot diagrams were used to assess normal distribution. The Kruskal-Wallis test was used to compare variables without normal distribution across ≥3 groups, and the Wilcoxon signed rank test was used for assessments of dependent groups.
The interclass correlation coefficient was used to assess the level of agreement between observers. Chi-square test, Yates continuity correction, and Fisher exact test were used to compare qualitative data. The data were assessed at a 95% confidence interval, with significance defined as P < .05. NCSS 2020 Statistical Software (Number Cruncher Statistical System; NCSS LLC) was used to the analyze statistical data.
Results
Interobserver reliability was calculated with the intraclass correlation coefficient based on CT-derived tunnel metrics, including intertunnel distances and tunnel entry point localization relative to anatomic landmarks. The interclass correlation coefficient was calculated as 0.996, indicating excellent agreement (P = .001).
Tunnel Convergence
On the lateral side, 11 tunnel convergences were observed in the FH group (7 for FCL–ACL and 4 for FCL–PLT), while no convergences were noted in the PSG group, achieving 100% avoidance. On the medial side, 10 tunnel convergences were encountered in the FH group (3 for MCL–PCL_PMB and 5 for POL–PCL_PMB) and 2 in PSG group, indicating 80% avoidance. On the medial side, most tunnel convergences were observed between the POL and PCL–PMB (n = 5) and the MCL and PCL–PMB (n = 3). Two tunnel collisions were observed between the POL and PCL_PMB in the PSG group, even though the entry point was correct. Ten convergences were observed on the medial side for the FH group, and PSG utilization avoided 80% of convergences (Table 2).
Tunnel Convergence Instances Between Tunnels a
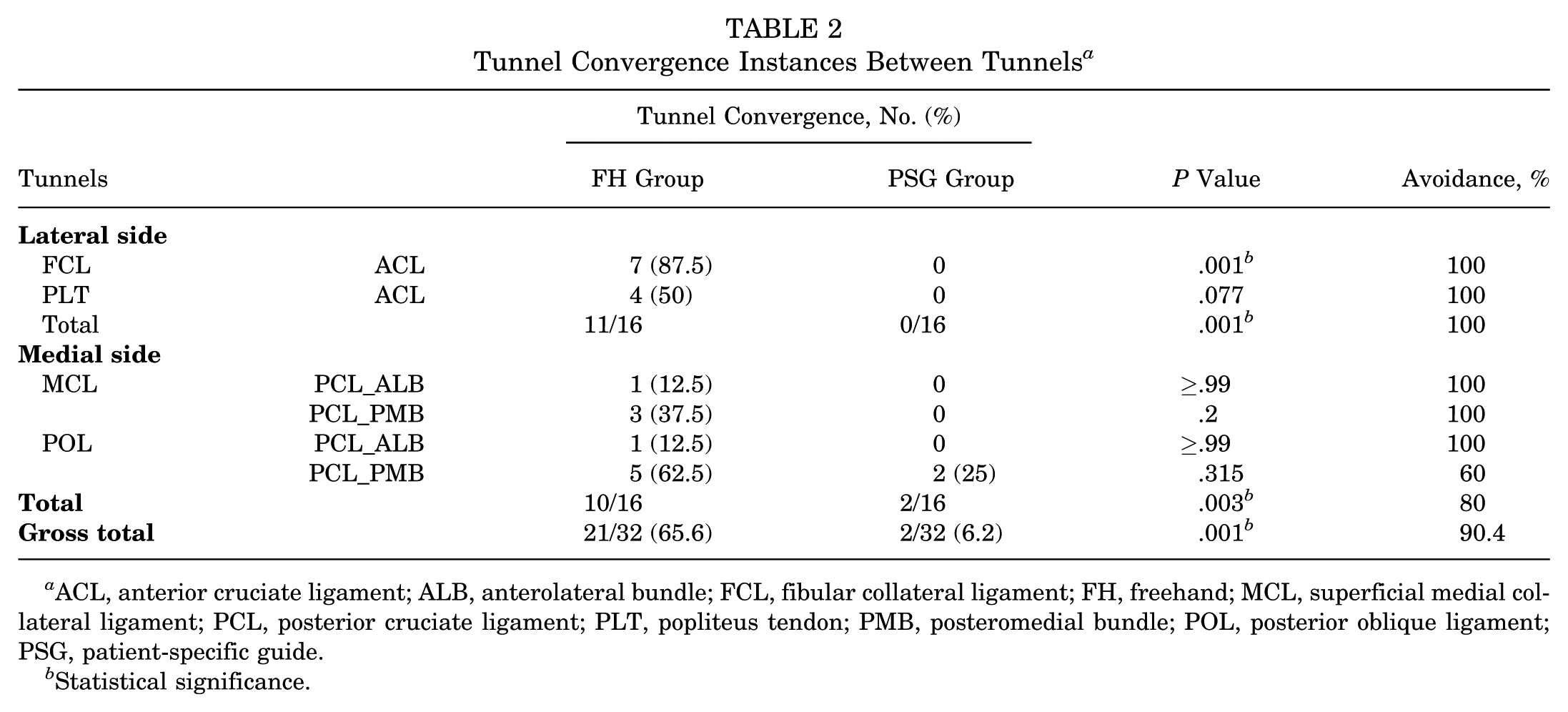
ACL, anterior cruciate ligament; ALB, anterolateral bundle; FCL, fibular collateral ligament; FH, freehand; MCL, superficial medial collateral ligament; PCL, posterior cruciate ligament; PLT, popliteus tendon; PMB, posteromedial bundle; POL, posterior oblique ligament; PSG, patient-specific guide.
Statistical significance.
Intertunnel Distances
On the lateral side, the intertunnel distance between the ACL and FCL and the ACL and PLT was significantly higher in the PSG group (P = .001) (Table 3). The mean intertunnel distances were significantly higher in the PSG group for MCL–PCL_ALB and POL–PCL_ALB (P = .012). Additionally, the mean intertunnel distances between the PLT and FCL footprints were significantly higher in PSG group (19.25 ± 1.46 vs 14.81 ± 3.42 mm; P = .012) (Figure 4).
Intertunnel Safe Distances Measured via Computed Tomography Scan a
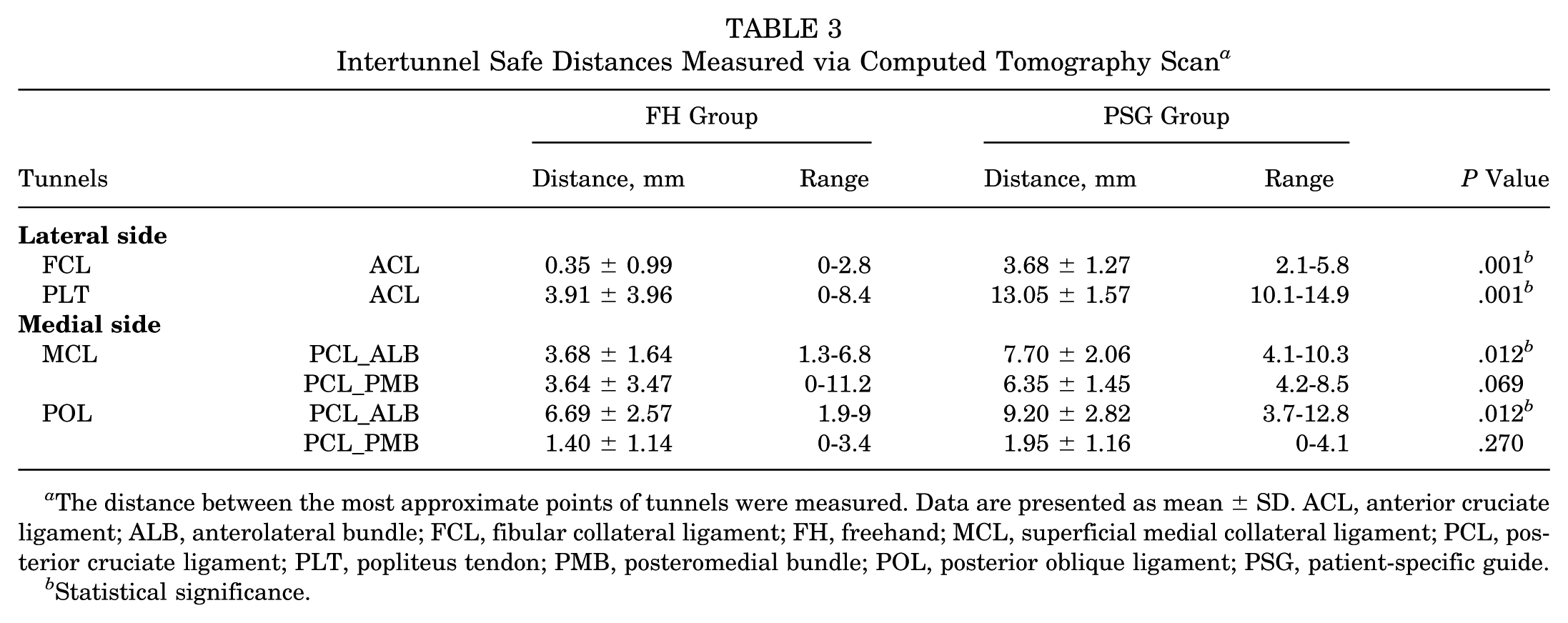
The distance between the most approximate points of tunnels were measured. Data are presented as mean ± SD. ACL, anterior cruciate ligament; ALB, anterolateral bundle; FCL, fibular collateral ligament; FH, freehand; MCL, superficial medial collateral ligament; PCL, posterior cruciate ligament; PLT, popliteus tendon; PMB, posteromedial bundle; POL, posterior oblique ligament; PSG, patient-specific guide.
Statistical significance.

Comparison of PLT – FCL footprint distances between groups. The patient-specific guide (PSG) group demonstrated significantly higher intertunnel distances, while the freehand (FH) group showed greater variability. Data are presented as median (line), interquartile range (box), and minimum-maximum values (error bars).
Tunnel Entry Points
The number of correct tunnel entry locations for the FH group was 3, 2, 3, and 0, whereas the PSG group had 8 of 8 for the FCL, PLT, MCL, and POL, respectively. Overall tunnel entry point accuracy was 8 of 32 (25%) in the FH group versus 32 of 32 (100%) in the PSG group (P = .001) (Figure 5). The mean distance between anatomic footprints of the PLT and FCL was significantly greater in the PSG group (mean ± SD, 19.25 ± 1.46 mm) as compared with the FH group (14.81 ± 3.42 mm; P = .035).

Heat map of the tunnel entry apertures in relation to anatomic landmarks. Green circle: entry area within the ranges described. Red circle: out-of-range tunnel entry area. Dotted circle: target tunnel entry area. FCL, fibular collateral ligament; MCL, superficial medial collateral ligament; PLT, popliteus tendon; PMB, posteromedial bundle; POL, posterior oblique ligament; PSG, patient-specific guide.
Discussion
The most important finding of the study is that PSG utilization in multiligament tendon reconstruction (1) reduced tunnel convergence, (2) enhanced intertunnel distance, and (3) increased tunnel entry point precision. Although proper avoidance angles have been described to avoid tunnel intersections, manual tunnel placement relies heavily on the surgeon's skill.
Safe drilling angles to prevent tunnel violation for posterolateral tunnels have been widely investigated in cadavers, sawbones, and computer models.3,8,10,23,26 Tunnel collision during multiple-ligament injury surgery leads to graft failure, resulting in incomplete restoration of stabilization and ultimately inferior clinical outcomes. Many variations of the tunnel angulations have been proposed to avoid tunnel convergence.
PLC reconstruction with ACL reconstruction poses a risk of tunnel convergence on the lateral side. Schuler proposed [40, 0] angulations to avoid convergence and suggested limiting the tunnel depth to 25 mm and avoiding coronal angulation; however, the convergence rate still reached 29%. 26 Similarly, Camarda et al 3 showed that there is a high risk of convergence when drilling the FCL tunnel in a coronal plane at 20° and 40° as compared with 0°. In contrast, Narvy et al 23 [40, 20] and Kim et al 14 [20, 10] proposed slight proximal (coronal plane) deviation and postulated that there is a high risk of trochlear violation if anterior (axial plane) angulation is excessive and that even more convergence occurs in smaller femurs. Contrary to the previous trend of intentionally creating proximal deviation for the FCL tunnel, Gelber et al 10 demonstrated that a [30,0] trajectory could effectively avoid tunnel convergence without the need for such coronal deviation. Yet, they still suggested a proximal deviation for the PLT [30, 30] tunnel to extend the tunnel length. Gali et al 8 demonstrated that 0° of coronal angulation carries the risk of intercondylar notch penetration and excessive axial angulation (>40°) carries the risk of trochlear penetration; therefore, they offered [20, 20] angulations for the FCL and PLT. These studies vary widely in terms of femur size, test material used, drill diameter, and ACL tunneling technique, each of which is a factor that affects the convergence rate. Each author sought the optimal drilling angle and addressed a solution to another challenge. Building on prior work, Moatshe et al 21 combined previous findings and optimized drilling angles for FCL [35, 0] and PLT [30, 30] for simultaneous PLC and PMC anatomic reconstruction and successfully prevented tunnel convergence by 100% on the lateral side. Nonetheless, the extent to which a newly opened tunnel matches the intended position remains unclear. There is a void in the literature regarding the discrepancy between the intended tunnel placement and the accuracy of its actual implementation. However, the implementation of theoretical knowledge in the field remains unknown. In our study, all participants were asked to open tunnels according to the instructions described by Moatshe et al to test reproducibility. Seven convergences (87.5%) were observed between the FCL and ACL and 4 (50%) between the PLT and ACL. In total, 11 tunnel convergences occurred in the FH group and 0 in the PSG group at the lateral side (P = .001). Despite careful planning and surgical expertise, human error remains a potential factor in complex procedures. The use of a PSG mitigates these errors and reduces reliance on the surgeon's spatial imagination. Wolf et al 30 stated that a range of variations has consistently been shown during tunnel placement, even among experienced surgeons. In MLKI surgery, the margin of error is limited, and tunnel collisions may elevate the already high complication rate. Moreover, revision remains a potential complication, occurring in up to 9% of cases after MLKI surgery. Consequently, bone stock is of significant value and should not be wasted. 2 Our findings demonstrate that PSG utilization may overcome these drawbacks. We attribute this to the capability of the PSG to optimize placement by minimizing deflections.
On the medial side, a 20° coronal angulation of the sMCL tunnel was demonstrated to increase the likelihood of convergence with the PCL tunnel, particularly in smaller femurs; thus, an angulation of 20° to 40° is recommended to avoid convergence. 3 Gelber et al 10 demonstrated that the [30, 30] configuration of the sMCL and POL avoided 100% convergence for single- and double-bundle PCL tunnels. Moatshe et al 21 showed that the sMCL [20-40, 40] and POL [20, 20] configuration decreased the convergence rate by 86% and 100% for the sMCL and POL, respectively. In this study, PSG utilization avoided tunnel convergence by 100% between the sMCL and PCL, and overall medial side tunnel convergence was avoided by 80%, dropping from 10 (62.5%) to 2 (12.5%; P = .003). Consistent with the findings of Moatshe et al, the highest convergence rate was observed between the POL and PCL_PMB (62.5%), and there were 2 convergences in the PSG group. Interestingly, even when the tunnel entry point was correct, 2 tunnel convergences were observed in the PSG group, indicating that intraoperative challenges and human error are still possible when restrictions are applied and that guide-stabilizing elements should be reinforced in the design. We attribute this to the close proximity of these tunnels, relatively small femur size, and a sense of unfamiliarity with the novel technique.
Successful outcomes are highly probable when reconstruction is well executed. 20 Therefore, an adequate intertunnel distance is paramount to ensure optimal bone-ligament integrity and avoid complications caused by future tunnel widening. A proximity of at least 2 mm between the tunnels was shown to be safe. 21 The instructions proposed by Moatshe et al 21 are accurate, and the anterior angulation provides a broader safe range, consistent with previous studies.3,21,23 Similarly, in the PSG group, tunnel convergence was avoided by 100%, and the safe distance increased between the sMCL and PCL_ALB (P = .012). Consistent with previous findings, proximal and anterior angulations enhance safe distance.3,10 For the POL tunnel, the distance to the PCL_ALB tunnel significantly increased in the PSG group (P = .012), but no significant increase was observed in the distance to the PCL_PLB tunnel (P = .27). Our study demonstrated that PSG utilization not only reduced convergence but also increased the safe distance of the tunnel of the ACL between the FCL and PLT tunnels (P = .001).
The 18.5-mm distance between the PLT and FCL footprints is a reliable anatomic reference for verifying correct tunnel placement. 17 Preserving this distance serves as a useful indicator that the reconstructed tunnels closely replicate native anatomy. In our study, the distances between footprints were 14.81 ± 3.42 and 19.25 ± 1.46 mm for the FH and PSG groups, respectively (P = .035), indicating that footprint anatomy can be accurately restored via the PSG.
Postoperative stability depends on how successfully the natural anatomy can be restored. The locations of the anatomic tunnel entry points are guided intraoperatively by reproducible anatomic landmarks, such as the epicondyles, which serve as surgical reference points. Although quantitative data exist to define these entry points based on measurable distances from such landmarks, the accuracy of tunnel placement with the FH technique remains largely dependent on the surgeon's skill. In our study, a low rate of correct tunnel entry site was observed in the FH group (25%) and significantly increased with use of the PSG (100%; P = .001); interestingly, none of the surgeons could perfectly determine the POL tunnel entry site using the FH technique. In the absence of the PSG, the placement of the tunnels is left to the surgeon's skill. In conformity with the findings of Fernández-Poch et al, 7 actual tunnels can be effectively established with a deviation <2 mm from the planned tunnel via a PSG.
The use of a PSG provides static, anatomy-based accuracy in tunnel placement. Emerging technologies include navigation, and augmented reality technologies provide real-time intraoperative feedback to minimize error. 29 Although these advanced modalities offer dynamic adaptability, they are related with higher costs, steeper learning curves, and sophisticated hardware requirements. The next frontier will likely to be the artificial intellegence integration into existing systems. Therefore, the present study should be regarded as a foundational step that may be integrated into existing navigation workflows as a core layer for data validation for dynamic, instantaneous feedback-based systems. In the long term, artificial intelligence–driven systems will rely on the large, comprehensive data lakes derived from this and similar studies, involving anatomically precise datasets that are essential for pioneering data-driven surgical technologies. The current study can be seen as a single drop to this evolving lake that will eventually nourish artificial intelligence–assisted surgical systems in the future.
This study has several limitations. First, although a model identical to lifelike dimensions has been created, there is limited feedback on parameters such as friction and tissue hardness that activate the tactile sense during drilling. Second, radiologic navigation of the tunnel entry points was not performed. However, all the participants had clear instructions during the procedure. Third, PSG concept–related drawbacks include time and labor requirements at the planning phase, logistic demand and costs, and, most important, the challenge in achieving optimal guide fitting under real surgical conditions owing to the presence of surrounding soft tissue. Furthermore, larger surgical exposure and extensive soft tissue dissection may be required to obtain adequate bone contact, which may offset the procedural efficiency observed in this study. The absence of soft tissue likely contributed to prominent improvement in speed and precision; therefore, cadaveric validation of the current findings is required before surgical translation. At last, individual variations in ACL and PCL tunnel anatomy were not considered and may affect guide performance in vivo. Such anatomic variations should be taken into account at the planning phase. In real-world application, modular add-on sleeves that allow drill diameter adjustments with a similar tunnel centerline could accommodate size variability. Further validation of guide performance in cadaveric models before clinical application is required.
We are aware that the whole procedure takes time, but deciding the positions of the tunnels and executing them are the keystones of MLKI surgery. Last, the use of a single anatomic model enabled a controlled assessment of intersurgeon variability under standardized conditions. While repeating the procedure across multiple anatomic models could further decipher intersurgeon differences, this remains an area for future investigation. In this study, a single consistent model was intentionally selected to better isolate technique-related variation across participating surgeons.
Conclusion
High collision rates were detected in manual tunneling, indicating that relying solely on the surgeons’ theoretical knowledge without considering their spatial skills led to a significant failure rate. The implementation of a PSG enhances the applicability of theoretical information and mitigates avoidable mistakes in practical scenarios. PSGs are a useful tool for implementing knowledge in actual scenarios by reducing the convergence rate and increasing the tunnel entry accuracy.
Footnotes
Final revision submitted December 19, 2025; accepted December 25, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the TÜBİTAK 1512 Entrepreneurship Support Program (project 2210902). The scientific content of this publication is solely the responsibility of the authors and does not necessarily reflect the views of TÜBİTAK (The Scientific and Technological Research Council of Turkey). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Acibadem University Ethics Committee (approval 2024-12/516; August 15, 2024).