
Abstract
Background:
Many studies have evaluated the management of knee dislocations (KDs) and multiligamentous knee injuries (MLKIs). However, no study to date has analyzed the quality of the most cited articles in this literature.
Hypothesis:
There is a positive correlation between the number of article citations in the KD and MLKI literature and their methodologic quality.
Study Design:
Systematic review.
Methods:
The Web of Science online database was searched to identify the top 50 cited articles in KD and MLKI care. Demographic data were recorded for each study. The Modified Coleman Methodology Score (MCMS) and the Methodological Index for Non-randomized Studies (MINORS) were used to analyze the methodological quality of each article. Spearman correlation coefficients (r s) were then calculated.
Results:
The articles identified were published between 1958 and 2015 in a wide variety of peer-reviewed journals (n = 16). The majority of study level of evidence (LOE) was of low quality (level 5, 16%; level 4, 54%; level 3, 16%; level 2, 14%). There were no studies of level 1 evidence. The mean MCMS and MINORS scores were 29.0 (SD, 19.1; range, 3-72) and 6.1 (SD, 3.7; range, 0-14), respectively. No significant correlation was identified between the number of citations and the publication year, LOE, MCMS, or MINORS (r s = 0.123 [P = .396]; r s = 0.125 [P = .389]; r s = 0.182 [P = .204]; and r s = 0.175 [P = .224], respectively). Positive correlations were observed between improved MCMS and MINORS scores and more recent year of publication (r s = 0.43 [P = .002]; r s = 0.32 [P = .022]) as well as improved study LOE (r s = 0.65 [P < .001]; r s = 0.67 [P < .001]).
Conclusion:
The top 50 cited articles on KD and MLKI care consisted of low LOE and methodological quality, with no existing level 1 articles. There was no significant correlation between the number of citations and publication year, LOE, or study methodological quality. Positive correlations were observed between later publication date and improved methodological quality.
Knee dislocations (KDs) and multiligamentous knee injuries (MLKIs) have historically been viewed as rare injuries. While still rare when compared with isolated knee ligament injuries, KDs and MLKIs are occurring with increased prevalence. 66 Reasons for increased prevalence include the diagnosis of spontaneously reduced KDs, changes in automotive design, the obesity epidemic, and the growing popularity of extreme sports. 69 Ultra-low-velocity KDs (ULVKDs) in the morbidly obese are becoming increasingly more common, and treatment of these injuries is difficult. Azar et al 5 published a retrospective cohort study in 2011 examining the outcomes of 13 obese and morbidly obese patients with ULVKD and MLKI. In this group, patient-reported outcomes, including International Knee Documentation Committee score, were “severely poor” regardless of surgical or nonsurgical treatment. However, Hospital for Special Surgery knee scores (fair vs poor) were significantly better for those undergoing ligamentous reconstruction as compared with those treated nonoperatively. Additionally, this study found increasing body mass index to correlate with increased complication risk, including deep vein thrombosis, amputation, peroneal nerve injury, and/or vascular injury. 5 Little has been published regarding the long-term functional outcomes of KD and MLKI, and excellent lasting results from reconstruction are rarely achieved. 52
Because of the rarity of these injuries, treating surgeons must often rely on the published experience of other surgeons for guidance in clinical management. Increased recognition of these injuries has led to larger published clinical series on treatment outcomes. Surgical treatment of KDs has been shown to improve outcomes, but many patients are still unable to return to prior occupations or sporting activities. 17 However, given the relatively uncommon nature of KD and significant variation in presenting concomitant pathology, it has been suggested that little high-quality evidence exists to guide physicians on the best management of these challenging injuries. 67
As the number of published academic studies grows, there is greater motivation to examine the quality of those publications. 23 Increased article citations has historically been used as a measure of an article’s academic impact. 2,12,70 In addition to the frequency of citation, it is important for readers to be aware of the methodological quality of a paper. The MCMS (Modified Coleman Methodology Score) and MINORS (Methodological Index for Non-randomized Studies) criteria are 2 validated outcome tools used in the evaluation of a study’s methodologic quality. 24,57
Analyzing the most frequently cited topics in a field, as well as examining the methodological quality, can give insight into the strength of treatment recommendations and can suggest gaps in knowledge that should be addressed by future researchers. Several studies within orthopaedics have looked to analyze available literature relating to subspecialties, including pediatrics, foot and ankle, and shoulder and elbow surgery. 6,8,21 Other studies have expanded on this by examining the methodologic quality of studies regarding treatment of specific conditions, such as knee articular cartilage injuries, rotator cuff repair, and ulnar collateral ligament reconstruction. 4,20,23,24,29,58 To our knowledge, this is the first study to examine the methodologic quality of frequently cited articles relating to treatment of KD and MLKI.
The purpose of this study was to (1) identify the top 50 most cited articles related to management of KD and MLKI, (2) determine whether there is a correlation between the number of citations and their corresponding level of evidence (LOE), and (3) determine whether there is a correlation between study methodological quality and number of citations. We hypothesized that the overall methodological quality of the top 50 cited articles would be low, that there would be a correlation between methodological quality and number of article citations, and that more recent publications would demonstrate a higher methodological quality.
Methods
Our literature review was performed by obtaining articles through the Web of Science Online Database (v 5.30) in October 2018 to reflect the most up-to-date top 50 most cited articles relating to KD and MLKI. The individually searched terms that were used to conduct the review were “knee dislocation,” “multiple or multi-ligament knee reconstruction,” “multiple ligament repair of the knee,” and “tibio-femoral dislocation.” Limitations were placed on articles for humans only and English language. There were no restrictions placed on publication date. After initial review, 9 studies did not meet inclusion criteria of being directly related to KDs; thus, 9 additional studies were pulled to bring the total to 50 articles. Of the 9 articles removed, 3 were in regard to knee arthroplasty, 1 discussed osteoarthritis in the knee, 1 related strictly to anterior cruciate ligament knee injuries, 2 studies focused on patellar dislocations, 1 studied meniscal allograft transplantation, and 1 study was on total knee amputations. The top 50 overall articles for KDs, not including patellar dislocations, were then arranged by number of citations.
All articles were assessed for number of total citations, date of publication, journal of publication, country of origin, and type of study (randomized controlled trial, prospective cohort, retrospective cohort, mechanism-based reasoning, literature review, systematic review, case-control, or case series). Each article’s LOE was critiqued per the Oxford Centre for Evidence-Based Medicine LOE scale. MCMS and MINORS were used to evaluate the methodological quality for each article meeting inclusion criteria. 24,57
MCMS and MINORS scores were tested for normal distribution with the Shapiro-Wilk test. Both measures were right skewed and not normally distributed, so nonparametric analyses were used. Spearman coefficients (r s) were used to determine correlations between the top cited articles (by number of citations) and their corresponding LOE and study methodological quality. Our correlation analyses (r s) had >80% power for detecting associations if the absolute value of the correlation was at least 0.39 (2-sided alpha = 0.05). Nonparametric 2-sample Wilcoxon tests and Kruskal-Wallis tests were used to test equality of medians among subgroups. P < .05 was defined as significant.
Results
Demographic data of the top 50 most cited articles on KD and MKLI, including title, country of origin, study type, number of citations, LOE, MCMS, and MINORS score, are included in Appendix Table A1. These articles were published between 1958 and 2015, and the majority (54%; n = 27) were published during the decades of 2000 to 2009 (Table 1).
Characteristics of the Top 50 Most Cited Articles on Knee Dislocations and Multiligamentous Knee Injuries

a Beginning year of decade.
Studies were analyzed for change over time. There was no significant correlation between year published and improved LOE (r s = 0.206; P = .152). However, statistically significant positive correlations were observed between more recent year of publication and increased MCMS (r s = 0.43; P = .002) and MINORS (r s = 0.32; P = .022) (Figures 1 and 2).

Association between Modified Coleman Methodology Score (MCMS) and year of study.

Association between Methodological Index for Non-randomized Studies (MINORS) score and year of study.
There was no significant correlation between number of citations and year of publication (r s = 0.123; P = .396). The mean ± SD number of citations of the top 50 articles was 83.2 ± 33.8, with a minimum of 44 and maximum of 223 (Appendix Table A1 and Table 2).
Citation Number and Methodologic Quality of Studies by Publication Region and Journal a
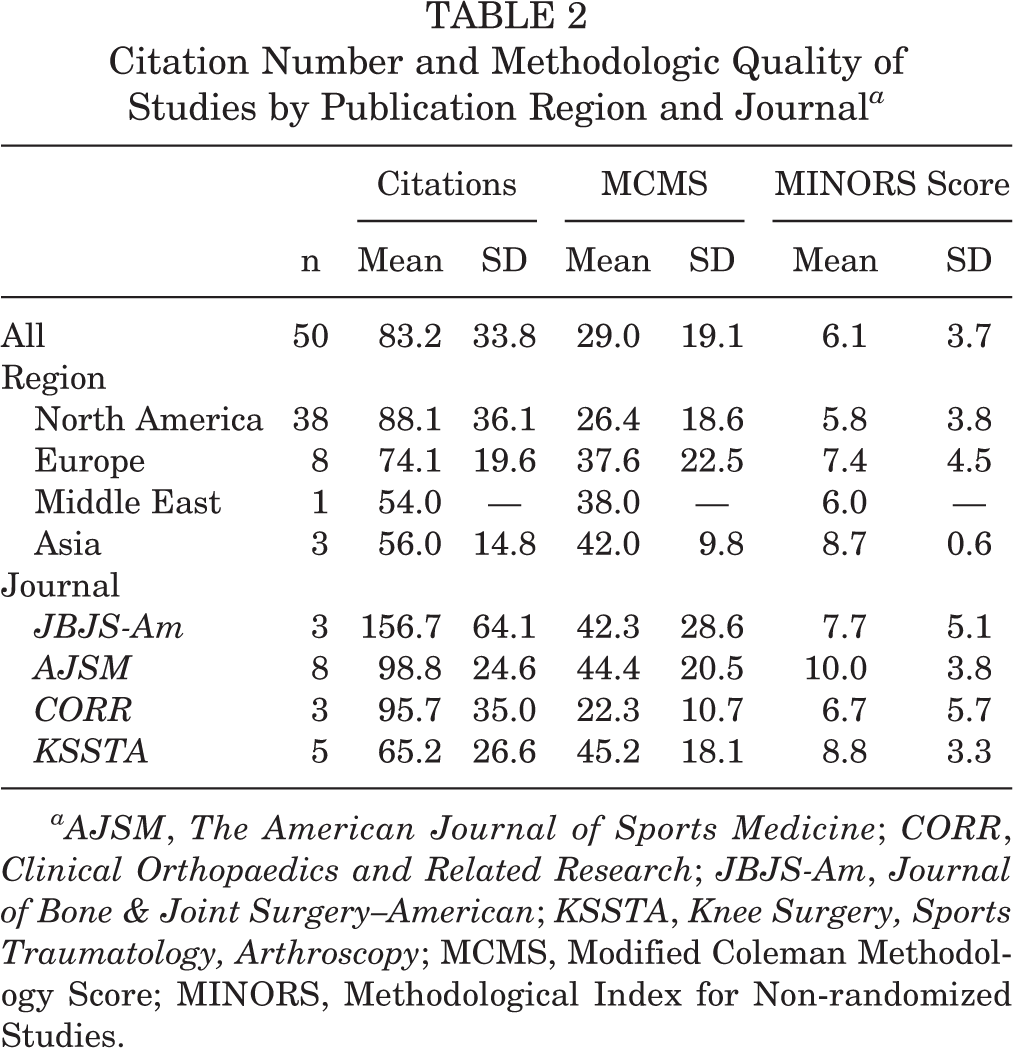
aAJSM, The American Journal of Sports Medicine; CORR, Clinical Orthopaedics and Related Research; JBJS-Am, Journal of Bone & Joint Surgery–American; KSSTA, Knee Surgery, Sports Traumatology, Arthroscopy; MCMS, Modified Coleman Methodology Score; MINORS, Methodological Index for Non-randomized Studies.
Twelve countries in 4 geographic regions accounted for the top cited literature (Table 1). North America accounted for the largest percentage (76%; n = 38) of the top cited literature (United States, 74% [n = 37]; Canada, 2% [n = 1]) and was also noted to have the studies with the lowest methodological quality (MCMS = 26.4 ± 18.6; MINORS = 5.8 ± 3.8). The other regions with top cited literature were Europe (16% [n = 8]; MCMS = 37.6 ± 22.5; MINORS = 7.4 ± 4.5), Asia (6% [n = 3]; MCMS = 42.0 ± 9.8; MINORS = 8.7 ± 0.6), and the Middle East (2% [n = 1]; MCMS = 38; MINORS = 6.0) (Table 2).
A wide variety of journals were found to have top cited articles, with 16 journals represented. The Journal of Trauma—Injury, Infection, and Critical Care had the most selected articles (18%; n = 9), with The American Journal of Sports Medicine (AJSM) (16%; n = 8) having the second most and The Journal of Bone & Joint Surgery–British Volume (10%; n = 5) and Knee Surgery, Sports Traumatology, Arthroscopy (10%; n = 5) having the third most (Table 3).
Number and Percentage of Top Cited Articles by Journal of Publication

The 3 journals with the highest mean number of citations (minimum 2 articles) were the Journal of Bone & Joint Surgery–American Volume (JBJS-Am) (156.7; n = 3), AJSM (98.8; n = 8), and Clinical Orthopaedics and Related Research (95.7; n = 3). The 3 journals with the highest methodological quality studies (minimum 2 articles) were Knee Surgery, Sports Traumatology, Arthroscopy (mean MCMS = 45.2; mean MINORS = 8.8), AJSM (MCMS = 44.4; MINORS = 10.0), and JBJS-Am (MCMS = 42.3; MINORS = 7.7) (Table 2).
A majority of the top cited articles were case series (54%; n = 27) (Table 1). The studies had levels of evidence ranging from level 2 to level 5, with 54% being classified as level 4 (n = 27). There was no significant correlation between the mean number of citations and the LOE (r s = 0.125; P = .389) among the studies included in the review.
The mean MCMS was 29.0 ± 19.1 (range, 3-72) (Table 4). There was no significant correlation between the mean number of citations and MCMS (r s = 0.182; P = .204). The mean MINORS score was 6.1 ± 3.7 (range, 0-14) (Table 4). There was no significant correlation between the mean number of citations and MINORS (r s = 0.175; P = .224). There were 13 comparative and 37 noncomparative studies included for evaluation. The overall methodological quality of the comparative studies was higher, demonstrating statistically significant improvements in MCMS (49.6 ± 16.8) and MINORS score (10.4 ± 3.2) as compared with the noncomparative studies (21.8 ± 14.0 and 4.8 ± 2.8; P = .0001 and P < .0001, respectively) (Table 4).
MCMS and MINORS Score Summaries for Top 50 Studies on Knee Dislocations and Multiligamentous Knee Injuries a

a MCMS, Modified Coleman Methodology Score; MINORS, Methodological Index for Non-randomized Studies.
A positive correlation was observed between improved methodologic quality (MCMS and MINORS) and higher LOE (r s = 0.65 and r s = 0.67, respectively; P < .001 for both) (Figures 3 and 4).

Association between Modified Coleman Methodology Score (MCMS) and level of evidence.

Association between Methodological Index for Non-randomized Studies (MINORS) score and level of evidence.
Discussion
This study identified from a single database the top 50 most cited articles relating to treatment of KD and MKLI in patients. There was no significant correlation between the number of citations of the top 50 cited articles and their LOE or methodological quality. Our correlation analyses (r s) had >80% power for detecting associations if the absolute value of the correlation was at least 0.39 (2-sided alpha = 0.05), demonstrating adequate power for all statistically significant correlations except MINORS score and year of study (r s = 0.32; P = .022).
To our knowledge, no prior study has examined the methodological quality of the most cited literature in KD and MKLI. There have, however, been more recent studies evaluating the literature with regard to other orthopaedic conditions, such as shoulder surgery, 40 rotator cuff surgery, 29,58 spine surgery, 65 and elbow ulnar collateral ligament injuries. 23 These studies found similar results regarding the timing of publication, with a majority of the most cited articles being published in the 1990s and 2000-2009 period. Typically this would not intuitively make sense, as increasing time since publication would provide a natural increase in the likelihood of citations. Our findings may be related to an increase in recognition of KD and MLKI in patients, leading to increases in the overall number of publications in recent years. Additionally, only 2 of the prior studies examined the methodological quality of the most cited literature with regard to a specific pathology. 23,58 Corroborating what has been previously described, our findings show a continued need for emphasis on high-quality studies in terms of treatment of KD and MLKI in patients.
In the current study, the majority of highly cited articles were published in either trauma journals or sports medicine journals. These findings are somewhat different from previously published literature on rotator cuff surgery and ulnar collateral ligament surgery, which found a majority of articles published on these topics were in JBJS-Am and The Journal of Shoulder and Elbow Surgery, 23,58 although, AJSM was also a top cited journal. The difference in journal publication is not unexpected, as KD and MLKI are clearly different injuries than shoulder and elbow pathology and cross the disciplines of orthopaedic trauma and sports medicine. However, the large variety of journals identified with top cited publications in KD and MLKI (16 total journals, each accounting for 2%-18% of the top cited articles) speaks to the paucity of high-quality literature on this topic and the heterogeneity of the patient population. Had there been improved methodologic quality regarding these publications, we believe that a higher percentage of them would have been published in journals with the highest impact factors in the orthopaedic surgery literature.
Most (74%) of the top 50 cited articles on KD and MLKI were published in journals based in the United States. This trend is consistent with prior studies examining top cited literature across multiple disciplines, including plastic surgery, general surgery, trauma, and orthopaedic surgery. 31,36,43,45 As suggested previously, this could represent a bias in the literature toward American authors, given that many of the top journals are based in the United States and are published in the English language.
Prior literature has also shown that a majority of the published articles in orthopaedic surgery are level 4 case series studies. 23,29,31,58 This finding was analogous to our finding in the KD and MLKI literature that a majority were level 4 studies (56%) and case series design (56%). Although there has been a recent push to improve evidence-based medicine in orthopaedic literature, our study found no significant correlation between improved LOE and year of publication. There was, however, statistically significant improvement in the methodologic quality of the top cited publications over time. Even with this improvement, we found no level 1 evidence studies on KD and MLKI, and the majority of the most cited literature in this topic were of low methodological quality. This is not to imply that the findings of studies of lower LOE on these injuries should be disregarded, as they are important foundational building blocks to our knowledge and treatment of KD and MLKI. Rather, we advocate for there to be continued energy to perform additional high-quality studies to help guide treatment measures for these injuries. Given the complex presentation and relative rarity of these injuries, the difficulty of designing a high-quality prospective randomized trial regarding their treatment and outcomes will undoubtedly require multicenter collaboration.
Spearman correlations were performed to analyze relationships among number of citations, LOE, methodologic quality, and year of publication of the top 50 cited articles in KD and MLKI. No statistically significant correlations were observed between number of citations and increased LOE, improved methodologic quality (MCMS or MINORS), or year of publication. However, improved methodologic quality (MCMS and MINORS) was shown to have statistically significant positive correlations with increased LOE (moderate to strong) and more recent year of publication (moderate). Thus, it does appear that higher-quality studies with increased levels of evidence are currently being performed. As this trend continues into the future, a prospective multicenter level 1 study (STaR Trial) is under way to evaluate surgical and rehabilitation timing as well as other issues related to the treatment of these complex injuries.
The importance of critically evaluating the available literature cannot be overstated. It is imperative that orthopaedic surgeons and the broader medical community base clinical decision making more heavily on higher-quality literature rather than number of citations or publications in higher-impact journals. The methodological quality deficiencies identified in this study should propel clinicians to improve their methodology and study design to achieve higher-quality articles in the future. As with previous studies, 23,58 the current review should serve as an appropriate guide for future studies aiming to evaluate the quality of available literature on other topics in orthopaedic surgery.
The current study has several limitations. This was the first to analyze the quality of the most cited articles in KD and MKLI literature. The number of articles (N = 50) was arbitrarily chosen based on previous literature. 6,21,23,29,40,58 This is important because this number could have excluded other potentially relevant articles with higher methodological quality but lower number of total citations. Another limitation of this study was the use of only 1 database, Web of Science, in the identification of most cited articles, as this is currently the only database to which our institution subscribes. The addition of a similar Scopus database search would have decreased the likelihood of omitting relevant articles from our evaluation. In an attempt to minimize article omissions, we did not limit our search protocol to “known” orthopaedic journals.
Other factors that were not specifically accounted for in this study but should be discussed are the potential for artificially inflated number of citations owing to “self-citation” and the “snowball effect.” These occur when high-volume authors cite their own work and when other authors are more likely to cite articles because of previous citations rather than content quality, respectively. Disadvantages to newer published articles having less time to accrue citations has been discussed as well, although this did not seem to be a factor in our study, given that a majority of the top cited literature for KD and MLKI was published from 2000 to 2009. A final limitation is that the number of times that an article is cited is constantly changing, and our search was performed at a moment in time (October 2018). As data on KD and MLKI continue to be published, there will be shifts in highly cited articles based on changes in practice techniques rather than content or quality of articles.
Conclusion
The top 50 cited articles in KD and MLKI care comprise a variety of geographic regions and journals. These studies were primarily of relatively low LOE (level 4) and low methodological quality when evaluated by MINORS and MCMS criteria, with no existing level 1 articles published to date. Statistically significant positive correlations between improved methodologic quality (MCMS and MINORS) and (1) more recent year of publication and (2) increased article LOE were observed in our review.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: D.A.H. has received grant support from Arthrex and educational support from Smith & Nephew and Gemini Mountain Medical. A.C.O. has received grant support from Arthrex; educational support from Smith & Nephew, Gemini Mountain Medical, and Tital Surgical Group; and hospitality payments from Zimmer Biomet. G.P.T. has received educational support from Arthrex, Desert Mountain Medical, and Gemini Mountain Medical. A.J.V. has received educational support from Arthrex and Gemini Mountain Medical and honoraria from Desert Mountain Medical. D.C.W. is a paid associate editor for The Orthopaedic Journal of Sports Medicine and has received grant support from Stryker, educational support from Arthrex and Gemini Mountain Medical, and hospitality payments from Desert Mountain Medical. R.C.S. has received educational support from Arthrex and Gemini Mountain Medical; grant support from DJO; and hospitality payments from Smith & Nephew, Zimmer Biomet, and Desert Mountain Medical. D.L.R. has received educational support from Arthrex and Gemini Mountain Medical and hospitality payments from Stryker and Desert Mountain Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Appendix
Top 50 Most Cited Articles on Knee Dislocations and Multiligamentous Knee Injuries a

| Rank | Article: First Author (Year) | Reference | Country | Type | Citations, n | Level of Evidence | MCMS | MINORS Score |
|---|---|---|---|---|---|---|---|---|
| 1 | Green (1977) | 19 | USA | Case series | 223 | 4 | 15 | 2 |
| 2 | Chhabra (2004) | 13 | USA | Case series | 152 | 4 | 40 | 9 |
| 3 | Wascher (1997) | 69 | USA | Case series | 143 | 4 | 9 | 4 |
| 4 | Sisto (1985) | 56 | USA | Case series | 135 | 4 | 13 | 5 |
| 5 | Levy (2009) | 33 | USA | Systematic review | 125 | 3 | 30 | 6 |
| 6 | Stannard (2005) | 59 | USA | Prospective cohort study | 120 | 2 | 72 | 14 |
| 7 | Noyes (1997) | 42 | USA | Prospective cohort study | 119 | 2 | 52 | 12 |
| 8 | Shapiro (1995) | 53 | USA | Case series | 115 | 4 | 30 | 10 |
| 9 | Krych (2015) | 30 | USA | Retrospective cohort study | 110 | 3 | 28 | 4 |
| 10 | Richter (2002) | 48 | Germany | Retrospective cohort study | 107 | 3 | 55 | 12 |
| 11 | Wascher (1999) | 68 | USA | Case series | 106 | 4 | 37 | 7 |
| 12 | Shelbourne (1991) | 55 | USA | Case series | 105 | 5 | 22 | 5 |
| 13 | Mills (2003) | 37 | USA | Case series | 100 | 4 | 37 | 8 |
| 14 | Liow (2003) | 35 | Scotland | Case series | 97 | 4 | 25 | 8 |
| 15 | Stannard (2004) | 60 | USA | Prospective cohort study | 95 | 2 | 72 | 12 |
| 16 | Fanelli (2005) | 18 | USA | Mechanism-based reasoning | 89 | 5 | 10 | 2 |
| 17 | Levy (2010) | 32 | USA | Retrospective cohort study | 87 | 3 | 46 | 11 |
| 18 | Treiman (1992) | 61 | USA | Case series | 85 | 4 | 31 | 8 |
| 19 | Moore (1981) | 39 | USA | Case series | 84 | 4 | 20 | 2 |
| 20 | Jones (1979) | 26 | USA | Case series | 83 | 4 | 10 | 2 |
| 21 | Twaddle (2003) | 62 | USA | Prospective cohort study | 82 | 2 | 21 | 4 |
| 22 | Kendall (1993) | 28 | Canada | Case series | 81 | 4 | 12 | 2 |
| 23 | Niall (2004) | 41 | Scotland | Case series | 81 | 4 | 24 | 7 |
| 24 | Levy (2009) | 34 | USA | Mechanism-based reasoning | 76 | 5 | 8 | 2 |
| 25 | Rihn (2004) | 49 | USA | Mechanism-based reasoning | 74 | 5 | 8 | 2 |
| 26 | Dedmond (2001) | 14 | USA | Systematic review | 74 | 5 | 34 | 4 |
| 27 | Yeh (1999) | 72 | Taiwan | Case series | 73 | 4 | 53 | 8 |
| 28 | Wascher (2000) | 67 | USA | Mechanism-based reasoning | 70 | 5 | 5 | 2 |
| 29 | Twaddle (1996) | 63 | USA | Case series | 69 | 4 | 27 | 6 |
| 30 | Rios (2003) | 50 | Spain | Case series | 69 | 4 | 44 | 7 |
| 31 | Tzurbakis (2006) | 64 | Greece | Retrospective cohort study | 69 | 3 | 57 | 13 |
| 32 | Almekinders (1992) | 3 | USA | Retrospective cohort study | 68 | 3 | 34 | 13 |
| 33 | Brautigan (2000) | 11 | USA | Mechanism-based reasoning | 64 | 5 | 5 | 2 |
| 34 | Quinlan (1958) | 46 | England | Case series | 62 | 4 | 5 | 0 |
| 35 | Miranda (2002) | 38 | USA | Prospective cohort study | 61 | 2 | 43 | 10 |
| 36 | Dennis (1993) | 15 | USA | Case series | 58 | 4 | 10 | 4 |
| 37 | Robertson (2006) | 51 | Scotland | Review | 57 | 4 | 20 | 2 |
| 38 | Owens (2007) | 44 | USA | Case series | 57 | 4 | 47 | 6 |
| 39 | Ibrahim (2008) | 22 | Kuwait | Case series | 54 | 4 | 38 | 6 |
| 40 | Reckling (1969) | 47 | USA | Case series | 53 | 4 | 3 | 2 |
| 41 | Bratt (1993) | 10 | USA | Case series | 52 | 4 | 13 | 3 |
| 42 | Yu (1995) | 73 | USA | Case series | 51 | 4 | 9 | 4 |
| 43 | Engebretsen (2009) | 16 | Norway | Prospective cohort study | 51 | 2 | 71 | 10 |
| 44 | Abou-Sayed (2002) | 1 | USA | Retrospective cohort study | 50 | 3 | 36 | 8 |
| 45 | Bin (2007) | 9 | South Korea | Case series | 49 | 4 | 39 | 9 |
| 46 | Kaufman (1992) | 27 | USA | Case series | 48 | 4 | 10 | 3 |
| 47 | Barnes (2002) | 7 | USA | Systematic review | 47 | 3 | 25 | 7 |
| 48 | Wong (2004) | 71 | Singapore | Case series | 46 | 4 | 34 | 9 |
| 49 | Johnson (2008) | 25 | USA | Review | 46 | 5 | 5 | 2 |
| 50 | Shelbourne (2007) | 54 | USA | Case series | 44 | 4 | 31 | 7 |
a MCMS, Modified Coleman Methodology Score; MINORS, Methodological Index for Non-randomized Studies.