
Abstract
Background:
Although numerous studies have reported the clinical outcomes of meniscal allograft transplantation (MAT), no systematic review has clearly clarified its overall efficacy or the factors influencing clinical results.
Purpose:
To systematically evaluate clinical outcomes and graft survival across different follow-up periods following MAT and analyze potential factors that may influence postoperative outcomes.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review was conducted via PubMed, Embase, and the Cochrane Central Register of Controlled Trials to identify studies on MAT published between 2015 and 2025. Only studies involving meniscal transplantation for meniscal defects were included. The methodological quality of the included studies was assessed via the methodological index for non-randomized studies scale. The primary outcomes were the Lysholm score, visual analog scale score, Tegner activity score, Knee injury and Osteoarthritis Outcome Score, and International Knee Documentation Committee score. Data on graft survival rates and return-to-sport rates were also extracted. Additionally, exploratory subgroup analyses were conducted on the basis of follow-up duration, graft laterality (medial vs lateral), rehabilitation protocol, and fixation technique, with the Lysholm score used as the primary outcome measure for subgroup comparisons.
Results:
A total of 24 studies comprising 3251 patients were included. Significant improvements were observed across all reported clinical outcome scores following MAT (P < .001), but all had high heterogeneity (I2 > 90%). Both the clinical and the surgical graft survival rates decreased with increasing follow-up duration. Among the subgroup analyses, only follow-up duration had a statistically significant effect on postoperative improvement in the Lysholm score, with longer follow-up times associated with a smaller degree of improvement. No significant differences were found in the other subgroup comparisons. Metaregression revealed that body mass index, the lateral-medial ratio, and follow-up time constituted the major sources of heterogeneity.
Conclusion:
MAT is an effective treatment for patients with symptoms following meniscectomy. It results in significant improvements in knee function, pain relief, and quality of life. Lack of standardized patient selection, surgical technique, and rehabilitation limit the ability to identify factors that may influence outcomes. While it presents a promising alternative to meniscectomy, its long-term efficacy and broader applicability require further investigation.
Registration:
CDR420251001961 (PROSPERO database).
Meniscal allograft transplantation (MAT) has become an increasingly considered option for patients experiencing persistent symptoms following partial or total meniscectomy, particularly in young, active individuals aiming to restore load-bearing function and delay joint degeneration.12,38,55 Meniscectomy is a prevalent procedure, with over 690,000 cases performed annually in the United States alone. 2 However, it is associated with long-term biomechanical compromise, including reduced joint stability and an increased risk of osteoarthritis.21,55 Although MAT has been demonstrated to enhance knee contact mechanics 46 and is hypothesized to offer chondroprotective effects, 47 its function in clinical practice remains contentious. The body of high-level evidence supporting its superiority over nonoperative management is limited, 48 and consensus on appropriate indications and patient selection is lacking.14,46 Furthermore, the variability in surgical techniques, graft-processing methods, and outcome definitions has hindered the establishment of standardized procedures. Despite the potential benefits of MAT, it is not frequently performed. There is an urgent need for a clearer understanding of its clinical efficacy across patient and surgical subgroups.
A number of recent systematic reviews and meta-analyses have examined various aspects of MAT, offering valuable insights while also highlighting critical gaps in the literature. In the study by Dong et al, 11 a comparison was made between the use of MAT and meniscal scaffold implantation (MSI) across a total of 83 studies, encompassing 2859 cases of MAT and 1073 cases of MSI. The findings indicated that while both interventions demonstrated improvements in patient-reported outcomes (PROs), MSI exhibited higher 10-year survival rates and a reduced incidence of complications. In a similar vein, Li et al 33 concluded that synthetic grafts outperformed MAT in terms of Knee injury and Osteoarthritis Outcome Score (KOOS), visual analog scale (VAS), and Lysholm scores. However, both reviews noted limitations in long-term data quality and heterogeneity in methodologies. Beyond the realm of treatment comparisons, prior studies on MAT have predominantly concentrated on isolated factors such as graft fixation techniques,4,43 medial versus lateral compartment outcomes,5,14,16 and the impact of concomitant procedures such as high tibial osteotomy or anterior cruciate ligament (ACL) reconstruction.7,13,20,29 However, the majority of these analyses have been observational in nature, frequently lacking a comprehensive synthesis of how these variables interact to affect overall clinical efficacy. Furthermore, although certain studies have sought to identify prognostic factors for success, extant meta-analyses have frequently examined MAT outcomes in broad patient populations, without sufficient subgroup analyses based on demographic variables (eg, age, sex), graft preservation methods (eg, fresh-frozen vs cryopreserved), or surgical techniques.27,37,8,52 The return-to-sport (RTS) rate, a key functional outcome for active individuals, has been partially addressed,6,17,54 yet its relationship with activity level, baseline function, and graft status remains inadequately explored. In addition, although a number of studies have made comparisons between rehabilitation protocols, 42 the limited sample sizes and heterogeneity in reporting of these studies have a detrimental effect on the reliability and applicability of their conclusions. Taken together, although MAT shows promise in restoring function and delaying joint degeneration, the current evidence base remains fragmented. There is a need for a thorough synthesis that incorporates both surgical and patient-specific factors to more accurately define the clinical efficacy of MAT and to inform decision-making.
The objective of this study was to provide an updated and comprehensive meta-analysis of MAT by synthesizing available evidence on multiple clinical efficacy indicators. These indicators include functional improvement, failure and complication rates, graft survival, RTS, and PRO measures (PROMs). The incorporation of both surgical variables (eg, fixation technique, graft type) and patient characteristics (eg, age, body mass index [BMI]) is intended to facilitate a more nuanced understanding of the factors influencing the success of MAT. It is hypothesized that MAT significantly improves functional outcomes and slows osteoarthritis progression, with variations depending on demographic characteristics, immobilization techniques, and rehabilitation protocols.
Methods
This systematic evaluation and meta-analysis followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 39 The study protocol was registered with the National Institute for Health Research's PROSPERO database on March 21, 2025.
Search Strategy and Selection Process
A comprehensive literature search was conducted on January 26, 2025, in PubMed, Cochrane, and Embase via the following search terms: (((((((((((((((((((Allograft) OR (Homograft)) OR (Homografts)) OR (Homologous Transplant)) OR (Homologous Transplants)) OR (Transplant, Homologous)) OR (Transplants, Homologous)) OR (Allogeneic Graft)) OR (Allogeneic Grafts)) OR (Grafts, Allogeneic)) OR (Graft, allogeneic)) OR (Allogeneic Transplantations)) OR (Allogeneic Transplant)) OR (Transplant, Allogeneic)) OR (Transplants, Allogeneic)) OR ("Allografts[Mesh]"))) AND ((Transplantations) OR ("Transplantation[Mesh]"))) AND ((Menisci) OR (Meniscal) OR ("Meniscus[Mesh]")) OR ("Meniscus/transplantation[Mesh]"). A comparison of the search results was conducted to ascertain the extent to which they were complete. Two authors (Y.Z. and C.K.) independently screened the titles and abstracts of the studies, following the Cochrane Handbook guidelines, to identify studies for full-text review and inclusion. Disagreements were resolved through discussion with a colleague (Y.T.). The reference lists of the included studies were also screened to capture any additional relevant articles.
Eligibility Criteria
The inclusion criteria were as follows: (1) published studies, including randomized controlled trials (RCTs), cohort studies, case-control studies, and both prospective and retrospective clinical trials; (2) study population consisting of patients who underwent MAT after meniscectomy; (3) studies reporting clearly defined clinical outcomes, with ≥1 quantifiable outcome measure; (4) the follow-up duration had to exceed 1 year.
The exclusion criteria were as follows: (1) biomechanical, anatomical, or animal studies and literature reviews, technical notes, case reports, and similar nonoriginal research articles; (2) studies not reporting outcome measures or if outcomes were not presented as mean±standard deviation (SD); (3) studies involving underage patients or immature menisci.
Methodological Quality Assessment and Risk of Bias
The methodological quality of the included comparative studies was evaluated via the methodological index for non-randomized studies (MINORS) tool (Slim et al 45 ). The tool is composed of 12 assessment criteria, of which the first 8 are applicable to noncomparative studies, while the remaining 4 are employed for comparative studies. The items were evaluated on a scale ranging from 0 to 2, with higher scores denoting a lower risk of bias. The classification of studies with controls was determined by total scores, with studies receiving designations of high quality (≥18 points), moderate quality (12-17 points), or low quality (≤11 points). In contrast, studies lacking a control group were classified as high quality (≥12 points), moderate quality (9-11 points), or low quality (≤8 points). The risk of bias of the included randomized controlled trial was assessed using the Cochrane Risk of Bias 2 (RoB 2) tool. The RoB 2 tool evaluates 5 domains of potential bias and provides an overall risk-of-bias judgment based on a prespecified algorithm.
Data Extraction
The extraction of data was conducted independently by 2 researchers (Y.Z. and Y.T.), with any discrepancies resolved through a joint review process. The data that were extracted included the author of the publication, the year of publication, the country in which the study was conducted, the level of evidence, the study type, the sample size, the follow-up time, the patient demographics, the details of the meniscectomy (time since meniscectomy, surgical site, concurrent surgery and previous surgery, graft), the PROs, the survival rates, and the complications. The PROMs included in the study encompassed the Lysholm score, the visual analog scale (VAS), the International Knee Documentation Committee (IKDC) subjective score, the Tegner activity score, and the KOOS. Furthermore, we extracted the fixation method of MAT and the postoperative rehabilitation plan for subgroup analysis. Meniscal allograft fixation techniques were categorized into bone fixation and soft tissue fixation. Bone fixation involved grafts with bone plugs or a bone bridge secured within tibial bone tunnels or a keyhole slot to achieve anatomic horn placement. Soft tissue fixation techniques used suture-based methods without bone blocks, in which the graft horns were attached to surrounding soft tissues or residual meniscal tissue. Postoperative rehabilitation protocols were classified as standard or accelerated. Standard protocols required nonweightbearing for 4 weeks, partial weightbearing at 4 to 6 weeks, and full weightbearing at 8 weeks, with knee range of motion progressing from ≤90° in the first 2 weeks to 120° at 4 weeks and 135° at 6 weeks. Accelerated protocols permitted earlier progression, with nonweightbearing limited to 1 week, partial weightbearing by 2 weeks, and full weightbearing by 6 weeks; range of motion advanced to 100° within 2 weeks, 120° by 3 weeks, and 135° by 4 weeks. 42
Statistical Analysis
The continuous results were calculated and expressed as mean ± MD. The heterogeneity between studies was quantified using the I2 statistic. The I2 values of 25%, 50%, and 75% were regarded as indicative of low, medium, and high heterogeneity, respectively. The utilization of a fixed-effects model was deemed appropriate when I2 was found to be <50%, whereas a random-effects model was employed in instances where I2 was >50%. To assess the robustness of the pooled estimates and to explore potential sources of heterogeneity, pre-specified subgroup analyses were performed according to follow-up duration, geographical location, fixation method, and rehabilitation protocol, using the Lysholm score as the outcome measure. Between-subgroup heterogeneity was assessed using the χ2-based Q statistic (Qb), and the proportion of heterogeneity explained by moderators was estimated using R2. Statistically significant results were defined as P values <.05. All statistical analyses were conducted utilizing the R Foundation for Statistical Computing (Version 4.2.2) and Stata (Version 18.0; StataCorp LLC).
Results
Literature Search Results
The selection process for the study is illustrated in the PRISMA flowchart in Figure 1. A comprehensive literature search was conducted, yielding a total of 1257 studies, encompassing 593 studies from PubMed, 644 studies from Embase, and 20 studies from the Cochrane Library. Following a thorough review of the existing literature, a total of 484 duplicate studies were identified and removed from the analysis. Following a thorough evaluation of the titles and abstracts, 644 studies were excluded from the analysis. The remaining 129 articles were subsequently retrieved and thoroughly reviewed, resulting in the inclusion of 24 articles in the study, as shown in Table 1. The final inclusion criteria were as follows: 10 retrospective cohort studies, 9 case series, 4 prospective cohort studies, and 1 RCT were reviewed. The level of evidence of the 24 studies included was 1 to 4 (including 1 level 1, 4 level 2, 12 level 3, and 7 level 4); and 23 studies, with the exception of 1 RCT, were evaluated for quality via the MINORS tool. All of the studies were of a high quality (the specific scores are presented in Appendix Table A1). The included randomized controlled trial was assessed using the Cochrane RoB 2 tool and was judged to be at high risk of bias overall, primarily due to Domain 5 (bias in selection of the reported result) indicating concerns regarding selective reporting. 50

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram of article selection.
Characteristics of Included Studies a
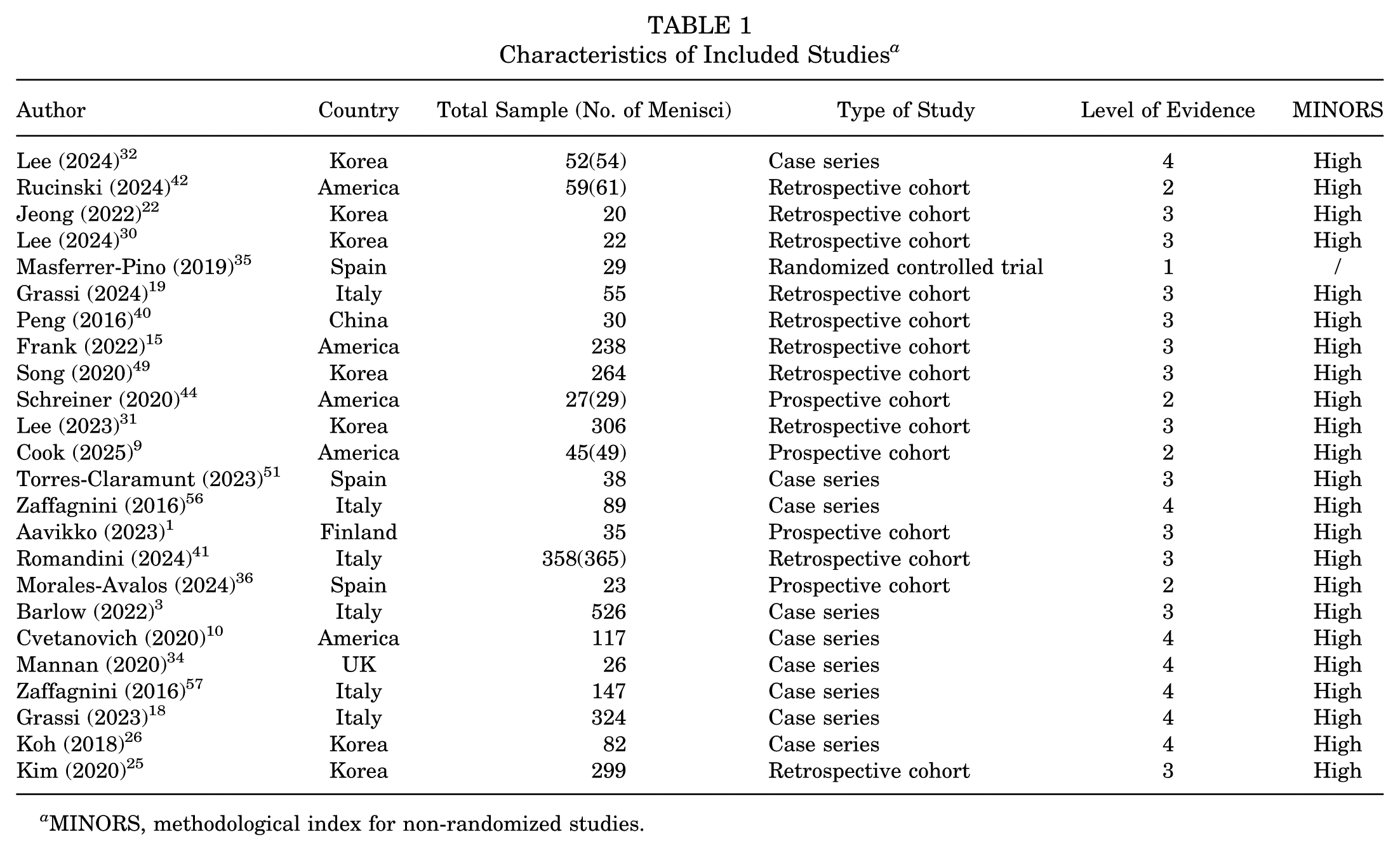
MINORS, methodological index for non-randomized studies.
Demographics
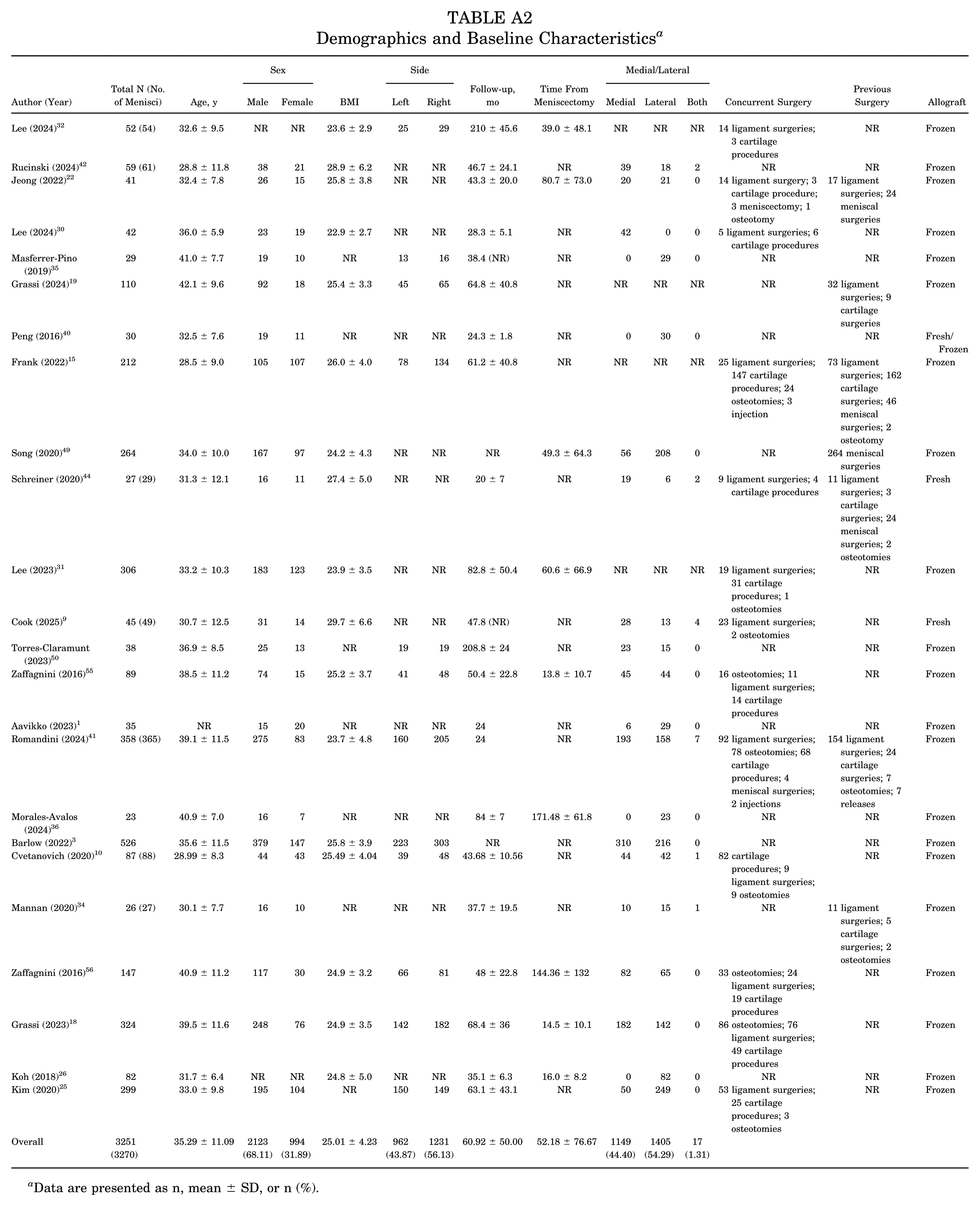
In 24 studies, a total of 3251 patients and 3270 menisci were included, with patient characteristics displayed in Table 2 (a more comprehensive table is presented in Appendix Table A2). A total of 22 studies reported follow-up times (two articles did not report standard deviations), and the overall weighted mean follow-up time was 60.92 ± 50.00 months, stratified as follows: 6 studies were conducted with a short-term follow-up duration of <36 months, 12 studies were conducted with a midterm follow-up duration of 36 to 80 months, and 4 studies were conducted with a long-term follow-up duration of >80 months. The mean age of the patients was 35.29 ± 11.09 years. Of the 3117 patients, 2123 (68.11%) were male; sex was not reported in two articles. The overall weighted mean BMI was 25.01 ± 4.23. The mean time from meniscectomy was 52.18 ± 76.67 months. The concurrent surgeries with MAT and previous surgeries are illustrated in Appendix Table A2. Concomitant surgeries were reported in only 13 of the 24 included studies. Among these, the most common procedures were ligament surgery and osteotomy. In contrast, prior meniscal surgery and ligament surgery were the most frequently reported previous procedures.
Demographics and Baseline Characteristics a

Data are presented as n, mean ± SD, or n (%).
PRO Measures
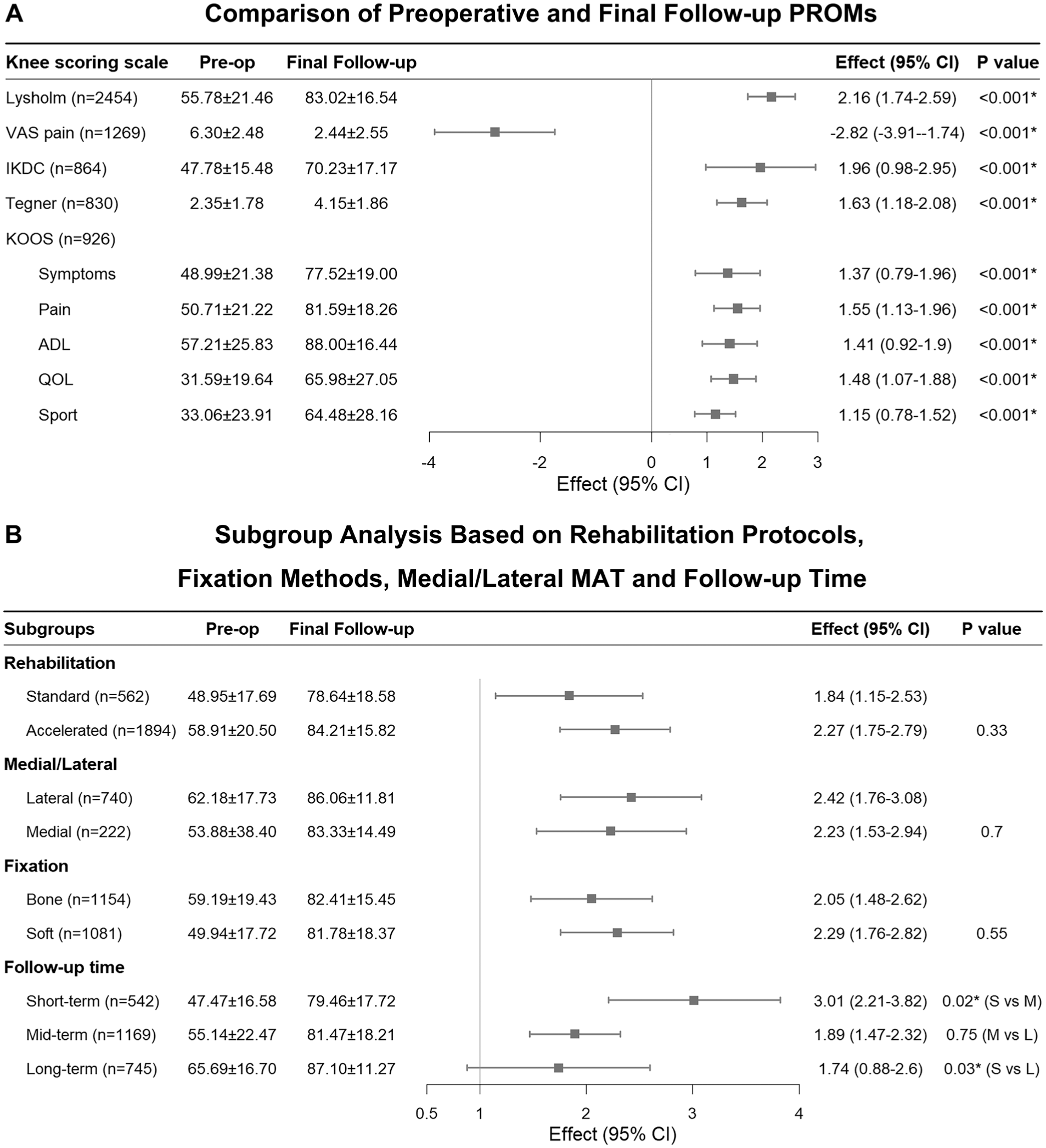
The primary outcome measures in this study included the Lysholm score, which is the most commonly reported metric across the included studies, along with the VAS scale for pain, the IKDC subjective form, the Tegner activity score, and the KOOS, as demonstrated in Table 3 and Figure 2A.
Comparison of Preoperative and Final Follow-up PROMs and Improvements in MAT a

Data are presented as n or mean ± SD. Statistically significant P values are indicated by bold font. ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; MAT, meniscal allograft transplantation; PROM, patient-reported outcome measure; QOL, Quality of Life; Sport, Sport and Recreation; VAS, visual analog scale.
Lysholm Score
A total of 17 studies reported Lysholm scores at the final follow-up. The postoperative scores ranged from 71.58 ± 20.56 to 90.5 ± 6.5, whereas the preoperative scores ranged from 39.1 ± 8.15 to 73.9 ± 17.5. The functional outcomes demonstrated a significant enhancement following surgical intervention, with mean Lysholm scores escalating from 55.78 ± 21.46 preoperatively to 83.02 ± 16.54 postoperatively (I2 = 97.34%; P < .001) (Table 3).
VAS Score for Pain
A total of 12 studies reported the VAS scores. The postoperative scores ranged from 1.1 ± 1.2 to 3.2 ± 2.7, whereas the preoperative scores ranged from 2.6 ± 2.5 to 8.21 ± 0.97. Patients experienced significant pain relief following surgery, with mean VAS scores decreasing from 6.30 ± 2.48 preoperatively to 2.44 ± 2.55 postoperatively (I2 = 99.41%; P < .001).
International Knee Documentation Committee
Nine studies assessed the IKDC subjective score. The postoperative scores ranged from 57.0 ± 20.5 to 80.5 ± 8.8, whereas the preoperative scores ranged from 38.5 ± 14.3 to 55.9 ± 15.2. A substantial enhancement in knee function was evident postoperatively, with a rise from 47.78 ± 15.48 to 70.23 ± 17.17 (I2 = 98.55%; P < .001).
Tegner Activity Score
Five studies reported the Tegner activity score, with postoperative scores ranging from 4.0 ± 0.7 to 4.5 ± 2.6 compared with 1.4 ± 0.7 to 3.5 ± 2.0 preoperatively. The postoperative group demonstrated a marked enhancement in activity level, with a significant increase from 2.35 ± 1.78 to 4.15 ± 1.86 (I2 = 99.23%; P < .001).
Knee Injury and Osteoarthritis Outcome Score
A total of 7 studies evaluated the KOOS and reported substantial improvements across all subdomains, including Pain, Symptoms, Sport and Recreation, Activities of Daily Living (ADL), and Quality of Life (QOL) (P < .001). The preoperative and postoperative KOOS scores for Pain (I2 = 92.5%; P < .001), Symptoms (I2 = 96.4%; P < .001), Sport and Recreation (I2 = 91.5%; P < .001), ADL (I2 = 94.7%; P < .001) and QOL (I2 = 92.1%; P < .001) are shown in Table 3. The findings indicate that there are substantial improvements in functional status and quality of life following MAT.
Survival Analysis
Among the 24 articles reviewed, 15 reported survival rates, incorporating a total of 2635 meniscal samples. The clinical and surgical success rates at 2, 5, 7, and 10 years were measured and are presented in Table 4. The established criteria for clinical failure included a Lysholm score of <65. Reoperation and surgical failure were defined as cases in which reoperation was necessary because of complications such as tearing and extrusion of the graft.
Clinical and Surgical Survival Rates at 2, 5, 7, and 10 Years of Follow-up

A total of 7 articles (1530 menisci) documented the nature of the reoperation, as illustrated in Figure 3. The most prevalent procedures included meniscal resection, removal, release, and repair. However, not all articles specified the rationale for undergoing repeat surgery, which may be attributable to factors such as pain, limited mobility, and traumatic lesions, among others. Among them, only 5 reported complications, mainly infection, joint effusion, hematoma, joint fibrosis, and so forth.
Forest plot for (A) comparison of preoperative and final follow-up PROMs and (B) subgroup analysis based on rehabilitation protocols, fixation methods, medial/lateral MAT, and follow-up time. ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; L, long-term; M, mid-term; MAT, meniscal allograft transplantation; Pre-op, preoperative; PROM, patient-reported outcome measure; QOL, Quality of Life; S, short-term; Sport, Sport and Recreation; VAS, visual analog scale.
Return to Sport
The RTS rate was documented in a mere 4 studies, as illustrated in Table 5. The mean weighted RTS rate was 83.22% (ranging from 74.2% to 100%). The mean weighted return to preinjury level rate was 28.36% (ranging from 21.2% to 49.4%) in the 3 reported studies. The mean RTS time was 9.6 ± 5.5 months.
RTS Rate and RTS Time a

RTS, return to sports.
Weighted average RTS time.
Subgroup Analysis
Despite the greater improvement in postoperative scores in comparison with preoperative scores, considerable heterogeneity was observed. In order to explore potential sources of heterogeneity, subgroup analyses of the Lysholm score were conducted on the basis of follow-up duration, location, fixation method, and rehabilitation protocol. The results are summarized in Figure 2B. Among these subgroups, only follow-up duration exhibited significant between-group disparities (Qb = 8.26; P = .02). Specifically, a significant discrepancy was identified between the short- and midterm follow-up groups (Qb = 5.86; P = .02) and between the short-and long-term follow-up groups (Qb = 4.50; P = .03), with the short-term group demonstrating a significantly greater improvement in the Lysholm score than the other 2 groups. However, no substantial difference was observed between the mid- and long-term follow-up groups (Qb = 0.10; P = .75). In addition, a univariate metaregression analysis was performed on continuous variables, including age (R2 = 4.92; P = .17), BMI (R2 = 0.00; P = .64), sex ratio (R2 = 0.00; P = .89), the medial/lateral (M/L) ratio (R2 = 25.67; P = .02) and follow-up duration (R2 = 15.87; P = .06). In addition, a multivariate metaregression was conducted, which indicated that the M/L ratio, follow-up time, and BMI were the primary contributors to heterogeneity (total R2 = 100%; P < .001).
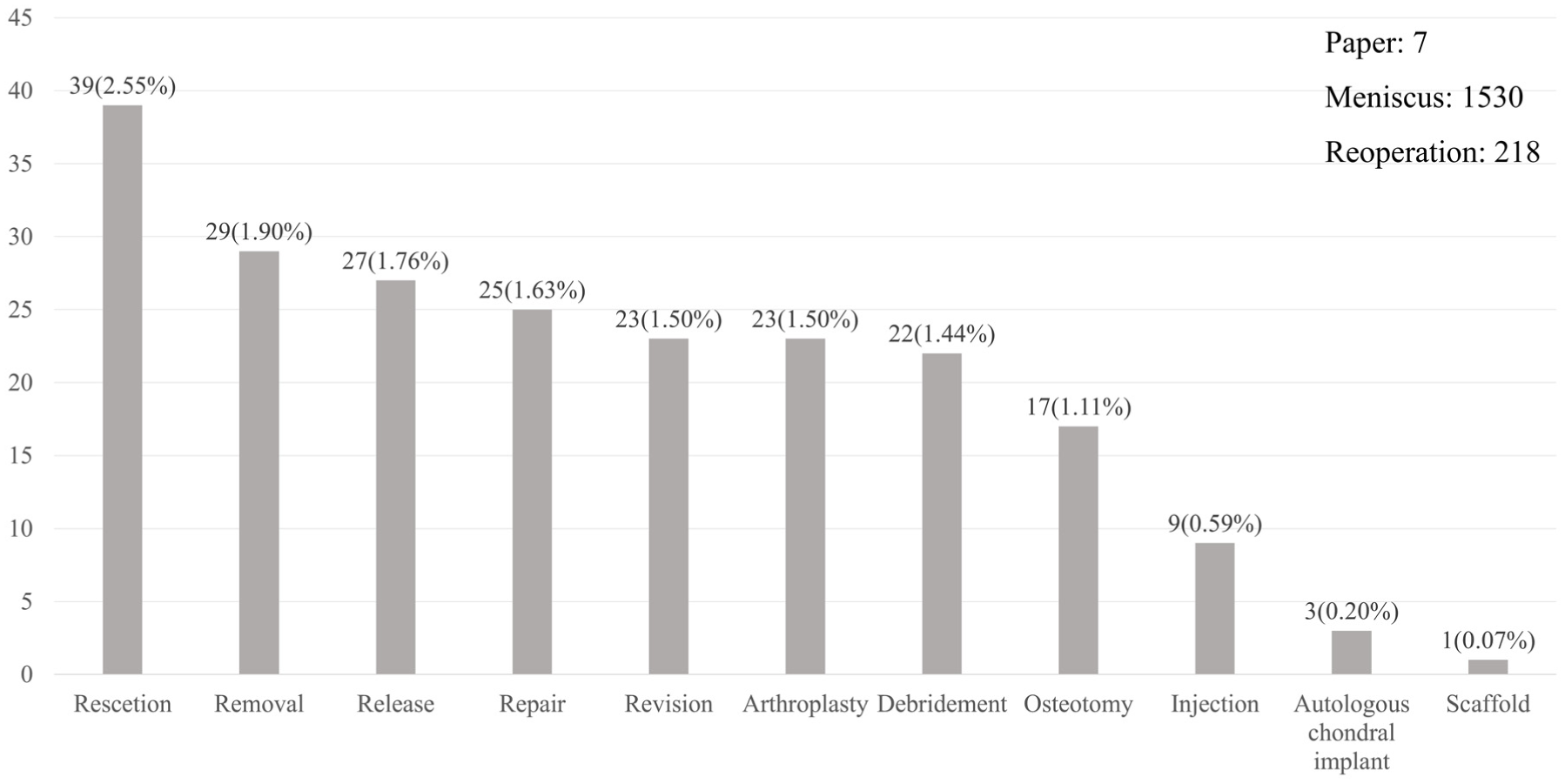
Main reoperations during the follow-up periods.
Discussion
This systematic review and meta-analysis demonstrates marked improvement in PROMs of MAT in patients with meniscal defects. As demonstrated by the findings of this study, significant improvements were shown across a range of outcome measures that have been validated (P < .05). These findings are consistent with the existing literature, which indicates that MAT effectively restores knee function, alleviates postmeniscectomy pain, and enhances mobility.20,45,55 A subsequent long-term outcome analysis revealed excellent surgical survival rates, thereby supporting the durability of MAT as a treatment option. Despite the occurrence of complications, including graft extrusion, reoperation, and progression of cartilage degeneration, their incidence remained within acceptable limits when considered against the therapeutic benefits of the procedure. The RTS data demonstrated that 83.22% of patients were able to resume athletic activities; however, only 28.36% returned to their preinjury performance level. This suggests that although MAT facilitates sports participation, complete return to high-impact or competitive sports may be limited by factors such as rehabilitation protocols, patient expectations, and concomitant joint pathology.
The findings of this study suggest that, among the patient characteristics examined, age alone does not significantly influence the clinical outcomes of MAT. This finding is consistent with those of previous studies by Frank et al 15 and Song et al, 49 who reported overall favorable symptom improvement and high graft survival rates across different age groups. However, it is important to note that age-related factors, such as cartilage degeneration and the duration of time since meniscectomy, may exert a more substantial influence on the outcomes of MAT. As Frank et al observed, older patients are more likely to ultimately undergo total knee arthroplasty, a trend likely attributable to more advanced cartilage degeneration commonly observed with increasing age. In line with these observations, Wang et al 53 found that patients undergoing immediate MAT and subsequent ACL reconstruction exhibited superior clinical outcomes compared with those with delayed MAT, including better cartilage preservation, slower Kellgren-Lawrence (K-L) osteoarthritis progression, and lower rates of graft degeneration and tearing. This finding indicates that the timing of MAT relative to meniscectomy may be a crucial factor in cartilage preservation and the overall success of treatment, particularly in older individuals with preexisting cartilage damage. Nevertheless, the limited sample size (N = 19) in Wang et al's study, as well as the lack of large-scale comparative studies on this factor, precludes definitive conclusions from meta-analysis. Consequently, there is an urgent need for further high-quality research to clarify the precise influence of these factors on MAT outcomes.
Another salient factor to consider in the context of MAT outcomes is BMI. Obesity, defined by a BMI ≥30, has been associated with an increased risk of complications in various orthopaedic surgeries, including MAT. A higher BMI has been demonstrated to contribute to greater joint loading and altered biomechanical stress patterns. These factors may lead to accelerated cartilage degeneration and increased strain on the graft. Research has indicated that patients with a high BMI may demonstrate inferior functional recovery and elevated graft failure rates in comparison with those with a normal BMI.23,31 Consequently, emphasis should be placed on preoperative weight management, as this has the potential to enhance postoperative outcomes and mitigate the risk of early graft degeneration. Jeong et al 22 and Kim et al 25 reported that lateral MAT (LMAT) achieved more accurate anatomic restoration than medial MAT (MMAT). LMAT demonstrated a tendency to maintain the graft's anterior root closer to its native position, whereas MMAT exhibited significant posterior displacement and internal rotation (P < .05), a phenomenon that is presumably attributable to the anatomic constraints of the medial compartment and potential interference with the ACL tunnel. However, the present study did not observe any significant differences in clinical outcomes between LMAT and MMAT, suggesting that, despite anatomic differences, both techniques can provide comparable functional benefits when performed in an appropriate manner.
Following meniscectomy, the loss of this shock-absorbing function leads to altered joint-loading patterns and accelerated articular cartilage degeneration. It is hypothesized that the restoration of hoop stress transmission and load distribution by MAT exerts chondroprotective effects, thereby mitigating further progression of osteoarthritis. This theoretical foundation has given rise to an increased interest in the assessment of cartilage preservation as a secondary objective of MAT, extending beyond the realms of pain relief and functional enhancement. A number of longitudinal studies have reported a decrease in K-L grade progression and reduced joint space narrowing following MAT when compared with continued conservative management (Kakria et al 24 ). For instance, Smith et al 47 conducted a systematic review of radiological outcomes and determined that MAT may be associated with enhanced cartilage signal and structure on follow-up magnetic resonance imaging (MRI). However, the extent of protection appears to diminish over time. Nevertheless, the absence of standardized cartilage imaging protocols and the limited duration of follow-up in the majority of the included studies precludes the drawing of definitive conclusions. Despite the theoretical potential of MAT to protect cartilage, the evidence regarding its direct impact on cartilage preservation remains inconsistent. Factors such as graft type (fresh vs frozen), fixation technique, time from meniscectomy to transplantation, and preexisting cartilage degeneration may all influence cartilage outcomes. It is noteworthy that Wang et al 53 demonstrated superior cartilage preservation with immediate MAT compared with delayed intervention, thus highlighting the importance of surgical timing. It is recommended that future prospective studies incorporating quantitative MRI (eg, T2 mapping, delayed gadolinium-enhanced MRI of cartilage), second-look arthroscopy, or biochemical markers (eg, cartilage oligomeric matrix protein and C-terminal telopeptide of type II collagen be conducted. The purpose of these studies would be to elucidate the degree of cartilage protection conferred by MAT and to identify patient subgroups who may benefit the most from this effect. LaPrade et al 28 conducted a prospective outcomes study, which demonstrated significant pain and function improvement after MAT in postmeniscectomy patients. However, the long-term chondroprotective effect of the procedure remained uncertain.
In addition to surgical techniques, graft preservation methods and rehabilitation protocols may influence clinical outcomes after MAT. As Schreiner et al 44 and Cook et al 9 have reported, fresh allografts have been shown to provide superior pain relief and functional recovery in comparison with fresh-frozen grafts. This phenomenon may be attributed to the enhanced cellular viability and biological integration observed in the former. While these findings suggest a possible advantage in graft preservation, the evidence remains limited, particularly with respect to long-term outcomes and chondroprotection. In a similar vein, although a plethora of fixation techniques (eg, bone plug vs suture-only) have been proposed with a view to reducing graft extrusion and enhancing stability, no universally superior method has been established. 24 The present meta-analysis did not identify statistically significant differences between fixation strategies, which is consistent with the findings of previous studies. These results suggest that fixation technique may not independently affect overall clinical outcomes, although its role in graft biomechanics and cartilage preservation warrants further study using advanced imaging and second-look arthroscopy. In relation to rehabilitation protocols, Rucinski et al 42 reported superior recovery trends in accelerated programs. However, the subgroup analysis revealed no significant difference between the standard and accelerated rehabilitation groups, which may be attributable to the absence of a unified protocol and confounding clinical variables. Furthermore, the presence of considerable heterogeneity across studies, manifesting in variations in surgical technique, surgeon experience, patient selection, and intraoperative decision-making, hinders the capacity to derive definitive conclusions. Taken together, while these perioperative factors may influence outcomes at a mechanistic level, current evidence is insufficient to confirm their impact on functional recovery or cartilage protection. In order to clarify these relationships and guide the optimization of MAT on the basis of evidence, high-quality, prospective studies incorporating standardized protocols, imaging-based cartilage assessment, and patient stratification are required.
Limitations
It is imperative to acknowledge the limitations inherent in the study's design when interpreting the findings. The validity of pooled results may be compromised by significant heterogeneity in study design, patient selection, and outcome measures, emphasizing the necessity for standardized reporting and classification in future MAT research. Furthermore, our subgroup analyses were restricted to a few commonly reported variables. The investigation of other potentially influential factors, including concomitant procedures such as ligament reconstruction or osteotomy, the time interval from meniscectomy to MAT, baseline cartilage status, standardized radiographic assessments of osteoarthritis (eg, K-L grades), and RTS outcomes, was not feasible due to inconsistent and insufficient data reporting in the included studies. The use of inconsistent statistical reporting methods, such as the use of medians rather than means, and the employment of diverse scoring systems, resulted in a reduction in the size of the analyzable sample. The utilization of small cohorts, in conjunction with predominantly nonrandomized designs, has been demonstrated to elevate the risk of type II error, particularly with regard to long-term outcomes. The necessity for high-quality, multicenter RCTs with extended follow-up is evident in order to clarify the durability of MAT and its potential to delay the onset of osteoarthritis. Moreover, the absence of cost-effectiveness analyses, biomechanical assessments, and a quantitative synthesis of imaging-based progression of arthritis limits our understanding of MAT's full clinical value and its long-term chondroprotective effect. It is recommended that future studies integrate imaging, gait analysis, and economic evaluation in order to facilitate evidence-based decision-making.
Conclusion
MAT is an effective treatment for patients with symptoms following meniscectomy. It results in significant improvements in knee function, pain relief, and quality of life. Lack of standardized patient selection, surgical technique, and rehabilitation limit the ability to identify factors that may influence outcomes. While it presents a promising alternative to meniscectomy, its long-term efficacy and broader applicability require further investigation.
Footnotes
Appendix
Demographics and Baseline Characteristics a
| Author (Year) | Total N (No. of Menisci) | Age, y | Sex | BMI | Side | Follow-up, mo | Time From Meniscectomy | Medial/Lateral | Concurrent Surgery | Previous Surgery | Allograft | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Left | Right | Medial | Lateral | Both | |||||||||
| Lee (2024) 32 | 52 (54) | 32.6 ± 9.5 | NR | NR | 23.6 ± 2.9 | 25 | 29 | 210 ± 45.6 | 39.0 ± 48.1 | NR | NR | NR | 14 ligament surgeries; 3 cartilage procedures | NR | Frozen |
| Rucinski (2024) 42 | 59 (61) | 28.8 ± 11.8 | 38 | 21 | 28.9 ± 6.2 | NR | NR | 46.7 ± 24.1 | NR | 39 | 18 | 2 | NR | NR | Frozen |
| Jeong (2022) 22 | 41 | 32.4 ± 7.8 | 26 | 15 | 25.8 ± 3.8 | NR | NR | 43.3 ± 20.0 | 80.7 ± 73.0 | 20 | 21 | 0 | 14 ligament surgery; 3 cartilage procedure; 3 meniscectomy; 1 osteotomy | 17 ligament surgeries; 24 meniscal surgeries | Frozen |
| Lee (2024) 30 | 42 | 36.0 ± 5.9 | 23 | 19 | 22.9 ± 2.7 | NR | NR | 28.3 ± 5.1 | NR | 42 | 0 | 0 | 5 ligament surgeries; 6 cartilage procedures | NR | Frozen |
| Masferrer-Pino (2019) 35 | 29 | 41.0 ± 7.7 | 19 | 10 | NR | 13 | 16 | 38.4 (NR) | NR | 0 | 29 | 0 | NR | NR | Frozen |
| Grassi (2024) 19 | 110 | 42.1 ± 9.6 | 92 | 18 | 25.4 ± 3.3 | 45 | 65 | 64.8 ± 40.8 | NR | NR | NR | NR | NR | 32 ligament surgeries; 9 cartilage surgeries | Frozen |
| Peng (2016) 40 | 30 | 32.5 ± 7.6 | 19 | 11 | NR | NR | NR | 24.3 ± 1.8 | NR | 0 | 30 | 0 | NR | NR | Fresh/ Frozen |
| Frank (2022) 15 | 212 | 28.5 ± 9.0 | 105 | 107 | 26.0 ± 4.0 | 78 | 134 | 61.2 ± 40.8 | NR | NR | NR | NR | 25 ligament surgeries; 147 cartilage procedures; 24 osteotomies; 3 injection | 73 ligament surgeries; 162 cartilage surgeries; 46 meniscal surgeries; 2 osteotomy | Frozen |
| Song (2020) 49 | 264 | 34.0 ± 10.0 | 167 | 97 | 24.2 ± 4.3 | NR | NR | NR | 49.3 ± 64.3 | 56 | 208 | 0 | NR | 264 meniscal surgeries | Frozen |
| Schreiner (2020) 44 | 27 (29) | 31.3 ± 12.1 | 16 | 11 | 27.4 ± 5.0 | NR | NR | 20 ± 7 | NR | 19 | 6 | 2 | 9 ligament surgeries; 4 cartilage procedures | 11 ligament surgeries; 3 cartilage surgeries; 24 meniscal surgeries; 2 osteotomies | Fresh |
| Lee (2023) 31 | 306 | 33.2 ± 10.3 | 183 | 123 | 23.9 ± 3.5 | NR | NR | 82.8 ± 50.4 | 60.6 ± 66.9 | NR | NR | NR | 19 ligament surgeries; 31 cartilage procedures; 1 osteotomies | NR | Frozen |
| Cook (2025) 9 | 45 (49) | 30.7 ± 12.5 | 31 | 14 | 29.7 ± 6.6 | NR | NR | 47.8 (NR) | NR | 28 | 13 | 4 | 23 ligament surgeries; 2 osteotomies | NR | Fresh |
| Torres-Claramunt (2023) 50 | 38 | 36.9 ± 8.5 | 25 | 13 | NR | 19 | 19 | 208.8 ± 24 | NR | 23 | 15 | 0 | NR | NR | Frozen |
| Zaffagnini (2016) 55 | 89 | 38.5 ± 11.2 | 74 | 15 | 25.2 ± 3.7 | 41 | 48 | 50.4 ± 22.8 | 13.8 ± 10.7 | 45 | 44 | 0 | 16 osteotomies; 11 ligament surgeries; 14 cartilage procedures | NR | Frozen |
| Aavikko (2023) 1 | 35 | NR | 15 | 20 | NR | NR | NR | 24 | NR | 6 | 29 | 0 | NR | NR | Frozen |
| Romandini (2024) 41 | 358 (365) | 39.1 ± 11.5 | 275 | 83 | 23.7 ± 4.8 | 160 | 205 | 24 | NR | 193 | 158 | 7 | 92 ligament surgeries; 78 osteotomies; 68 cartilage procedures; 4 meniscal surgeries; 2 injections | 154 ligament surgeries; 24 cartilage surgeries; 7 osteotomies; 7 releases | Frozen |
| Morales-Avalos (2024) 36 | 23 | 40.9 ± 7.0 | 16 | 7 | NR | NR | NR | 84 ± 7 | 171.48 ± 61.8 | 0 | 23 | 0 | NR | NR | Frozen |
| Barlow (2022) 3 | 526 | 35.6 ± 11.5 | 379 | 147 | 25.8 ± 3.9 | 223 | 303 | NR | NR | 310 | 216 | 0 | NR | NR | Frozen |
| Cvetanovich (2020) 10 | 87 (88) | 28.99 ± 8.3 | 44 | 43 | 25.49 ± 4.04 | 39 | 48 | 43.68 ± 10.56 | NR | 44 | 42 | 1 | 82 cartilage procedures; 9 ligament surgeries; 9 osteotomies | NR | Frozen |
| Mannan (2020) 34 | 26 (27) | 30.1 ± 7.7 | 16 | 10 | NR | NR | NR | 37.7 ± 19.5 | NR | 10 | 15 | 1 | NR | 11 ligament surgeries; 5 cartilage surgeries; 2 osteotomies | Frozen |
| Zaffagnini (2016) 56 | 147 | 40.9 ± 11.2 | 117 | 30 | 24.9 ± 3.2 | 66 | 81 | 48 ± 22.8 | 144.36 ± 132 | 82 | 65 | 0 | 33 osteotomies; 24 ligament surgeries; 19 cartilage procedures | NR | Frozen |
| Grassi (2023) 18 | 324 | 39.5 ± 11.6 | 248 | 76 | 24.9 ± 3.5 | 142 | 182 | 68.4 ± 36 | 14.5 ± 10.1 | 182 | 142 | 0 | 86 osteotomies; 76 ligament surgeries; 49 cartilage procedures | NR | Frozen |
| Koh (2018) 26 | 82 | 31.7 ± 6.4 | NR | NR | 24.8 ± 5.0 | NR | NR | 35.1 ± 6.3 | 16.0 ± 8.2 | 0 | 82 | 0 | NR | NR | Frozen |
| Kim (2020) 25 | 299 | 33.0 ± 9.8 | 195 | 104 | NR | 150 | 149 | 63.1 ± 43.1 | NR | 50 | 249 | 0 | 53 ligament surgeries; 25 cartilage procedures; 3 osteotomies | NR | Frozen |
| Overall | 3251 (3270) | 35.29 ± 11.09 | 2123 (68.11) | 994 (31.89) | 25.01 ± 4.23 | 962 (43.87) | 1231 (56.13) | 60.92 ± 50.00 | 52.18 ± 76.67 | 1149 (44.40) | 1405 (54.29) | 17 (1.31) | |||
Data are presented as n, mean ± SD, or n (%).
Final revision submitted December 10, 2025; accepted December 15, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This research was supported by the Sichuan Provincial Science and Technology Support Program (2024YFFK0297) and the National Natural Science Foundation of China (82072514). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.