
Abstract
Background:
Sports injuries are a leading cause of pediatric emergency department (ED) visits in the United States (US), accounting for approximately 20% of all injury-related visits, with 41% requiring operation. Football, basketball, baseball, soccer, and ice hockey are the 5 most popular US sports by viewership and participation, and pose a high risk of lower-extremity orthopedic injury. Despite increasing youth participation, previous studies have focused on a single sport or diagnosis, leaving limited population-level data to compare injury patterns across sports and sexes.
Purpose:
This study used nationally representative ED data to characterize the epidemiology, anatomical distribution, and temporal trends of pediatric lower extremity injuries from 2015 to 2024 across the 5 most popular US sports.
Study Design:
Descriptive epidemiology study.
Methods:
Pediatric lower extremity injuries from January 1, 2015, to December 31, 2024, in football, baseball, basketball, ice hockey, and soccer were queried using the National Electronic Injury Surveillance System (NEISS). Descriptive data, injury site, diagnosis, and product codes were recorded for patients aged between 0 and 18 years. National estimates (NEs) were calculated using NEISS sample weighting, and injury trends were evaluated using linear regression modeling.
Results:
A total of 77,654 cases representing an estimated 2,308,476 national injuries were identified, with a mean age of 13.74 ± 2.85 years. The injury distribution by sport was as follows: basketball (41.9%); football (27.7%); soccer (24.7%); baseball (4.8%); and ice hockey (0.9%). The most injured body parts were the ankle (42.9%) and the knee (29.3%). Sprains/strains accounted for 50.6%, followed by fractures (13.6%) and contusions (10.2%). Injuries occurred most frequently in boys, accounting for 78.7% of cases; however, girls experienced disproportionately higher rates of sprains/strains, ankle, and knee injuries. Injury levels peaked in 2015, with a 53.5% decline between 2019 and 2020 during the coronavirus disease 2019 pandemic. By 2024, injury frequencies rebounded to 94.9% of prepandemic levels.
Conclusion:
Despite a temporary pandemic-related decline, pediatric lower-extremity injuries remain prevalent and have nearly returned to prepandemic levels. While injury rates were highest among boys, girls experienced disproportionately high rates of noncontact injuries in soccer and basketball. Targeted prevention efforts should address sport- and sex-specific risks to improve youth athlete safety.
Pediatric lower-extremity injuries inundate emergency departments (EDs) nationally and can result in long-term, deleterious outcomes. These injuries often necessitate surgical intervention, carry a high risk of rehospitalization, and frequently result in suboptimal outcomes.8,18 Notably, lower extremity trauma accounts for approximately 20% of pediatric trauma hospitalizations, with 41% of these cases requiring operative intervention. 23 The risk for long-term consequences is substantially higher in pediatric populations, with potential growth plate damage leading to stunted growth and chronic pain. 27 Beyond these physical implications, there is also a significant psychological impact and financial burden to both families and health care systems associated with lower-extremity injuries.1,10,11,19,21
A more refined understanding of the epidemiology, paradigms, and sport-specific patterns surrounding pediatric lower-extremity injuries can augment hospital decision-making and inform clinical workflow. This is especially important given the rising intensity and year-round participation of youth in organized sports. Football, basketball, baseball, soccer, and ice hockey represent the 5 most popular United States (US) sports by viewership and participation. 22 These sports are widely participated in across pediatric age groups, accounting for nearly 50% of teen athletes in the US.3,12 These sports impose various biomechanical demands and loading patterns, often resulting in diverse trauma cases despite similar mechanisms of injury.4,17 For example, an ankle sprain in football may affect the peroneal tendons and anterior talofibular ligament. In contrast, a congruently termed sprain in basketball may affect the tibialis anterior muscle and the distal fibula.30,31 Understanding the variations and prevalence of these injury mechanisms is critical for tailoring treatment and rehabilitation protocols. Equipped with insights into sport-specific epidemiology and injury patterns, health care providers can optimize care, implement targeted prevention strategies, and guide patients through informed discussions during preventive visits or postoperative follow-up. Although previous studies have examined pediatric injuries within these individual sports, there is currently no national cross-sport comparative analysis in the literature.29,32
This study aimed to use nationally representative ED data to comprehensively characterize the epidemiology, anatomical distribution, types, and temporal trends of pediatric lower-extremity injuries sustained across the 5 most popular US sports over the last decade. We hypothesized that the epidemiology of pediatric lower-extremity injuries would differ significantly across sports and sexes, with female athletes demonstrating higher relative rates of sprains and soft-tissue injuries than male athletes. We further hypothesized that national injury frequencies would decline during the coronavirus disease 2019 (COVID-19) pandemic and subsequently rebound toward prepandemic levels.
Methods
Data Collection
Data were collected from the National Electronic Injury Surveillance System (NEISS), a publicly available, de-identified database that records information on injuries treated in approximately 100 hospital EDs across the US. Participating hospitals, all with a 24-hour ED and at least 6 beds, are strategically selected based on geographic region and size to emulate a nationally representative probability sample. 24 Trained coders review and input all ED data on patient characteristics, injury characteristics, treatment, associated products, and activity involvement into the NEISS database. Health care providers also report a narrative that describes the injury. National estimates (NEs) of injuries across the US are then calculated using the NEISS statistical sample weight assigned to each patient case at the given hospital. 32
Variables
The NEISS database was retrospectively queried for all pediatric lower extremity injuries associated with football, baseball, basketball, ice hockey, and soccer that were treated in US EDs between January 1, 2015, and December 31, 2024. Patients aged between 0 and 18 years were included. Recorded variables for each case included patient age, sex, injured body part, discharge disposition, and the date of the hospital visit. Product codes indicating the consumer product or activity involved at the time of injury were used to categorize each sport. Specifically, product codes 1211, 1205, 5041, 1279, and 1267 were used to identify injuries that occurred during baseball, basketball, football, ice hockey, and soccer, respectively. Only injuries involving the lower-extremities were included, defined as those affecting the knee, ankle, lower leg, upper leg, foot, or toe (injury codes 35, 37, 36, 81, 83, 93). The injuries analyzed were sprain/strains, fracture, contusion, dislocation, laceration, hematoma, and other injuries (injury codes 64, 57, 53, 55, 59, 58, 71). The Other category reflects injuries assigned to NEISS diagnosis codes that do not fall into the above groups, such as a nerve injury, crush injury, internal injury, or an unspecified diagnosis.
Statistical Analysis
The data were analyzed using IBM SPSS Statistics Version 28.0 (IBM Corp) and Microsoft Excel (Microsoft Corp). The distribution of injuries by age, sex, injured body part, and diagnosis was analyzed by descriptive statistics and reported in NEISS cases, NEs, and associated percentages. Linear regression analysis was used to assess trends in lower-extremity injury over time, and the associated P values and 95% CIs were reported. Injury frequency and sex were the outcomes of interest, and the year of injury was the independent variable for simple linear regression analysis over time.
Results
A total of 78,654 NEISS cases from 2015 to 2024 were identified, corresponding to a weighted national estimate of 2,308,476 sports-related lower-extremity injuries in pediatric athletes aged between 1 and 18 years, with a mean age of 13.74 ± 2.85 years (Table 1). Of these, 78.7% occurred in boys (n = 1,815,822) and 21.3% in girls (n = 492,639). The majority of injuries occurred in adolescents aged between 14 and 18 years (61.7%), followed by children aged between 9 and 13 years (34.4%). Also, 97.2% of cases were categorized as a disposition of treated and released, with an additional 1.5% resulting in hospitalization.
Patient Characteristics a

National estimate of pediatric lower-extremity injuries presenting to US EDs between 2015 and 2024 stratified by sex, age, and race. ED, emergency departments; NEISS, National Electronic Injury Surveillance System; US, United States.
Linear regression analysis of annual lower-extremity injuries showed no statistically significant change over the study period in boys (P = .209 [95% CI, −16,669.81 to 4268.06]) or girls (P = .078 [95% CI, −5373.79 to 352.20]) (Figure 1). However, there was a significant decrease in total injuries during the prepandemic period (2015-2020) (P = .050 [95% CI, −58.06 to −20.71]) and a significant increase during the postpandemic period (2021-2024) (P = .0244 [95% CI, 8.48 to 45.36]).

Frequency of yearly NEs for boys versus girls.
Basketball and soccer were the most common sports associated with lower-extremity injuries in both sexes (Figure 2). The injury distribution for each sport was as follows: basketball (41.9%); football (27.7%); soccer (24.7%); baseball (4.8%); and ice hockey (0.9%) (Table 2). Basketball accounted for 40.7% of injuries among boys, followed by football (33.4%) and soccer (19.5%). In contrast, girls experienced the highest proportion of injuries while playing basketball (46%) and soccer (44.1%), with football-related injuries constituting only 6.8%.

Distribution of injuries by sport for boys versus girls.
Injury Incidence by Sport for Boys Versus Girls a
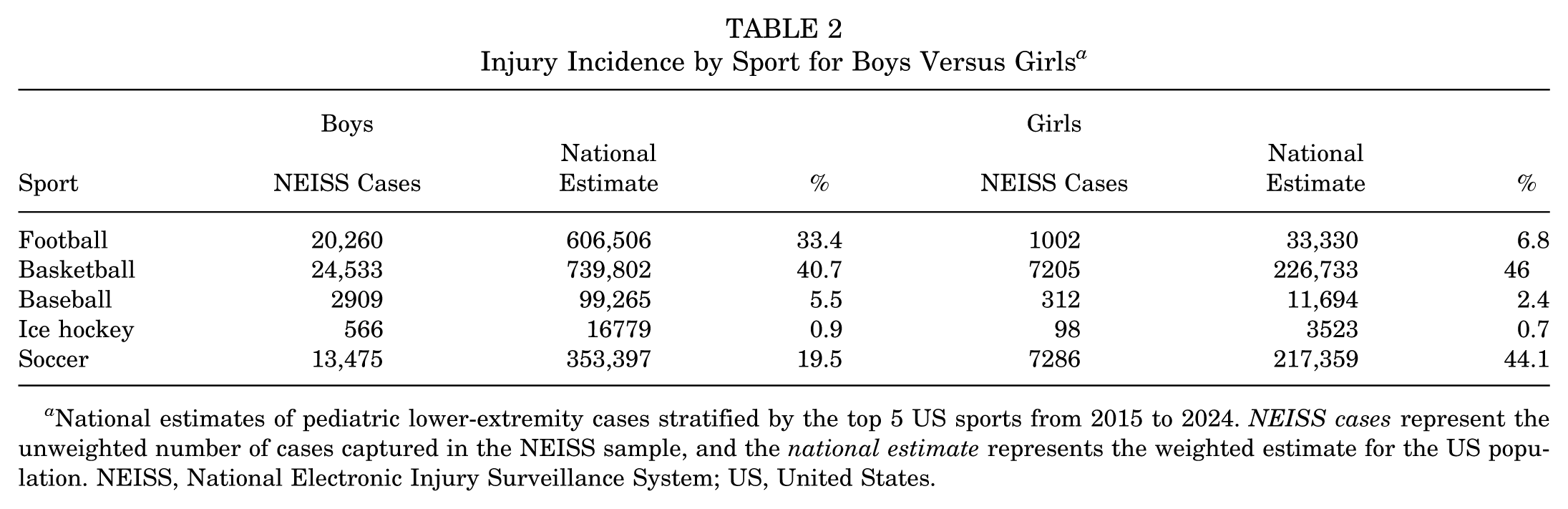
National estimates of pediatric lower-extremity cases stratified by the top 5 US sports from 2015 to 2024. NEISS cases represent the unweighted number of cases captured in the NEISS sample, and the national estimate represents the weighted estimate for the US population. NEISS, National Electronic Injury Surveillance System; US, United States.
Sprains and strains were the most frequent diagnoses across all sports, accounting for 50.6% of all injuries, followed by fractures (13.6%), contusions (10.2%), and dislocations (2.6%) (Table 3). Fractures were significantly more common in boys (15%) than in girls (8.4%). Notably, female athletes experienced a higher proportion of sprains and strains (56.4%) than male athletes (49%). Contusions and lacerations were particularly notable among male participants in contact sports such as football and basketball.
Primary Diagnosis and Injury Site by Sport a

Data are presented as n (%). National estimates of pediatric lower-extremity primary diagnoses and body parts injured from 2015 to 2024, stratified by the top 5 US sports. US, United States.
The ankle was the most injured body part in both sexes, representing 41.8% of male and 46.7% of female injuries (P < .001) (Table 4). Knee injuries followed, comprising 28.9% of male and 31.1% of female cases (P < .001). Boys exhibited significantly higher rates of lower-leg and upper-leg injuries than girls (10.6% vs 6.8% and 3.2% vs 1.6%, respectively; P < .001 for both), whereas foot and toe injuries showed more modest sex-based differences.
Rates of Body Part Injuries in Boys Versus Girls a

National estimates of pediatric lower extremity injuries from 2015 to 2024 of the body part injured stratified by sex.
Over the 10-year study period, the annual estimated number of sprains/strains peaked in 2015 (n = 164,742) and again in 2024 (n = 111,351) after a notable decline during the COVID-19 pandemic in 2020 (n = 55,919) (Table 5). Similarly, fractures decreased sharply in 2020 (n = 15,518) and rebounded in 2024 to 37,324. Overall, injury levels declined by 53.5% between 2019 and 2020 during the COVID-19 pandemic, then rebounded to 94.9% of prepandemic levels.
National Estimates and 10-Year Trends of Sprain/Strains and Fractures a

National estimate of the top 2 pediatric lower-extremity injury diagnoses by year from 2015 to 2024. NEISS cases represent the unweighted number of cases captured in the NEISS sample, and the national estimate represents the weighted estimate for the US population. NEISS, National Electronic Injury Surveillance System; US, United States.
Discussion
The major findings of this study demonstrate that pediatric lower-extremity injuries in the 5 most popular US sports remain a substantial national burden, with 78,654 NEISS cases corresponding to an estimated >2.3 million injuries over the 10 years. Basketball, football, and soccer accounted for approximately 95% of all injuries, with basketball contributing the largest share (41.9%). Sprains and strains were the predominant diagnosis (50.6%), followed by fractures (13.6%) and contusions (10.2%). Female athletes continue to bear a disproportionate burden of ankle and knee sprains, representing 46.7% and 31.1% of their injuries, respectively, despite male athletes comprising the majority of overall injury volume (78.7%). This reflects persistent sex-based differences in injury patterns. Injury rates declined sharply during the COVID-19 pandemic, falling 53.5% from 2019 to 2020, but rebounded to 94.9% of prepandemic levels by 2024.
Between 2015 and 2024, an estimated 2.31 million ED visits were attributed to sports-related lower-extremity trauma in children and adolescents, with 61.7% of all cases and nearly three quarters of female cases occurring in high-school aged athletes, consistent with national epidemiologic data showing the predominance of injuries in older youth and a higher proportion of female injuries in sports with balanced participation such as basketball and soccer.5,16,25 The 53.5% drop in injuries seen in 2020 mirrors the 60% reduction reported for organized team sports overall, reflecting the nationwide cancellation of youth athletics during the COVID-19 pandemic, a trend also observed in basketball and concussion epidemiology.16,20 Given the borderline slope estimate before 2020, we interpret prepandemic declines as hypothesis-generating rather than definitive, and we avoid attributing them to specific causal factors that cannot be assessed with NEISS. Nevertheless, injuries rebounded to 94.9% of 2019 levels by 2024, underscoring the need for graded return to play protocols after prolonged interruptions, as recommended by the American College of Sports Medicine and the American Medical Society for Sports Medicine. 15
Injury distribution by sport reinforces that participation demographics drive risk. Five sports accounted for virtually the majority of the injury burden: basketball (41.9%), football (27.7%), soccer (24.7%), baseball (4.8%), and ice hockey (0.9%), with basketball and soccer generating 90% of female injuries and football, baseball, and ice hockey producing >60% of male injuries, reflecting sex-based participation patterns.6,14
Pandemic-era trends differed accordingly: injuries in football, baseball, and ice hockey fell more steeply in 2020 and have yet to return fully to prepandemic volumes, whereas basketball and soccer rebounded faster, paralleling the swifter resumption of practices and competitions in those sports.14,16,20 However, NEISS cannot disentangle changes in participation exposure from changes in care-seeking or ED availability; therefore, inferences about the causes of decline or the pace of recovery across sports should remain cautious.
Diagnosis patterns highlight the contrasting mechanisms of male- and female-dominated play. Sprains and strains formed the majority of cases (50.6%), followed by fractures (13.6%), contusions (10.2%), and dislocations (2.6%). Girls demonstrated a significantly larger share of sprains and strains (56.4% vs 49%), consistent with pivoting and landing forces. In comparison, boys sustained relatively more fractures (15% vs 8.4%) and contusions or lacerations, reflecting the higher-impact collisions intrinsic to football, ice hockey, and, to a lesser extent, baseball.6,9,14
The predominance of ankle and knee injuries in both sexes, with a higher burden in girls (ankle 46.7% vs 41.8%; knee 31.1% vs 28.9%) (P < .001), is consistent with large-scale epidemiologic studies and meta-analyses demonstrating that female pediatric athletes are at increased risk for lower-extremity injuries, particularly at the knee and ankle, compared with male pediatric athletes. Previous literature attributes this sex disparity to differences in neuromuscular control, ligamentous laxity, and landing mechanics. However, NEISS does not reliably capture mechanisms. Thus, our data cannot confirm mechanistic pathways.2,7,26 Boys’ higher rates of lower- and upper-leg trauma are likewise consistent with literature on collision sports such as football, but the mechanism cannot be determined from NEISS.14,28
Our findings are best interpreted as high-level trends in ED presentations rather than mechanistic explanations or evaluations of specific prevention strategies. Because NEISS lacks exposure denominators, detailed mechanisms (eg, contact vs noncontact, landing vs cutting), settings (practice vs game), and injury specificity (eg, sprain grade, fracture pattern), we cannot determine whether ankle sprains and fractures share preventable pathways or whether any particular program is effective. Accordingly, we avoid prescriptive recommendations and instead use these patterns to prioritize areas for more granular surveillance.
Implications are therefore directional: these national trends can help identify high-volume targets for deeper study (eg, ankle and knee injuries in girls’ pivoting/landing sports and fractures/contusions in collision sports) and highlight where richer, mechanism-aware surveillance would be most informative. Future work should incorporate exposure denominators to compute true incidence, link ED data with outpatient, urgent-care, and athletic-trainer surveillance to reduce severity bias and capture follow-up, standardize injury and mechanism fields, and employ prospective and quasi-experimental designs to evaluate policy, rule, or training interventions with appropriate control for participation and context. 13
Our study is not without limitations. The NEISS dataset provides valuable information on the frequency and epidemiology of lower-extremity injuries in pediatric athletics over a long period. However, NEISS case identification, product coding, and sport coding are derived from brief clinical narratives and coded fields created by trained abstractors, which are subject to variation in detail and potential misclassification. This variability in detail may have failed to capture all relevant activity types, skewing the distribution of sport-specific injuries and leading some injuries to be categorized as other. Furthermore, the NEISS dataset relies on a representative probability sample to estimate national injury incidence from approximately 100 EDs. It excludes injuries treated in urgent care centers, primary care centers, or outpatient orthopedic settings. Therefore, our data likely underestimates the actual national burden of lower-extremity injuries from these 5 sports. NEISS does not capture information beyond the initial ED presentation, which limits our ability to analyze physical examination findings or long-term injury outcomes, including hospital courses or surgical interventions. In addition, NEISS lacks exposure denominators (eg, athlete-exposures or hours), precluding incidence rate calculations and limiting between-sport or sex comparisons, and it does not provide a validated contact versus noncontact variable or consistent contextual fields (practice vs game, movement pattern, surface/footwear).
Despite these limitations, the NEISS dataset remains the only nationally representative probability sample of lower-extremity injuries among pediatric athletes in the US. It provides valuable information on ED-treated injuries across childhood and adolescence, including patients before organized high school sport participation. It supports analysis of temporal patterns in ED utilization by sport and sex.
Conclusion
Our study showed that despite a temporary pandemic-related decline, pediatric lower-extremity injuries remain prevalent and have nearly returned to prepandemic levels. While injury rates were highest among boys, girls experienced disproportionately high rates of noncontact injuries in soccer and basketball. Targeted prevention efforts should address sport- and sex-specific risks to improve youth athlete safety.
Footnotes
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. Ethical approval was not sought for the present study.