
Abstract
Background:
Anterior cruciate ligament (ACL) reconstruction (ACLR) using quadriceps tendon (QT) autograft is associated with lower rates of graft rupture and favorable functional outcomes compared with hamstring (HS) autograft in adolescents. The ACL-deficient knee is at increased risk of injury to secondary stabilizers of the knee, including the menisci, although studies have not reported differences in rates of subsequent meniscal tear between HS and QT groups.
Purpose:
The goal of this study was to compare rates of graft rupture and subsequent meniscal tear after adolescent ACLR using HS or QT autograft.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This was a retrospective review of adolescent patients (age, 10-19 years) who underwent ACLR with either HS or QT autograft between 2009 and 2023 at an urban tertiary care pediatric hospital. Patients with ≥2 years of clinical follow-up were included. Patient characteristics, surgical details, and reinjury rates were calculated and compared between the 2 subgroups. Multivariable logistic regression was performed to evaluate the relationship between graft failure and relevant variables.
Results:
A total of 467 patients (52.0% female) with mean age 14.6 ± 1.9 years and median follow-up of 3.1 (range, 2.0-13.4) years were included. The QT subgroup more commonly underwent concomitant anterolateral ligament reconstruction/lateral extra-articular tenodesis at the time of primary ACLR (P < .001), were slightly older (P = .04), had higher baseline body mass index (P = .01), had a shorter period of follow-up (P < .001), and more commonly had concomitant medial meniscal tear compared with the HS group (P = .047). Graft rupture was lower among patients treated with QT versus HS (7.2% vs 23.2%; P < .001). The rate of subsequent meniscal tear was not statistically significantly different among patients treated with QT versus HS (4.6% vs 9.2%, respectively; P = .08). Regression analysis showed that graft type was associated with risk of graft failure (QT vs HS: odds ratio, 0.29; P < .001) but was not clearly associated with subsequent meniscal tear (QT vs HS: odds ratio, 0.47; P = .09).
Conclusion:
Adolescent patients undergoing ACLR with QT autograft have significantly lower risk of graft rupture compared with those treated with HS autograft. There was no statistically significant difference in rate of subsequent meniscal tear between the QT and HS groups.
Anterior cruciate ligament (ACL) ruptures are among the most common adolescent knee injuries with the per capita incidence of ACL reconstruction (ACLR) peaking around 175 per 100,000 people in patients around age 16 to 17 years. 3 Alarmingly, rates of ACL injury in young patients have been on the rise in recent decades, highlighting the need for high-quality outcomes research in this demographic.2,7
Studies have shown that ACLR using autograft in the adolescent population is associated with good functional outcomes and high rates of return to sport.1,26 However, research has consistently found higher rates of graft rupture among adolescents and young adults after ACLR compared with older adults, with the estimated risk of ACL graft rupture decreasing by about half from ages 16 to 30 years.6,8,11,16,22,24,25 In the STABILITY trial by Getgood et al, 9 which included patients aged <25 treated with ACLR using autograft hamstring (HS), 11% of patients treated without an additional lateral procedure experienced graft rupture at 2-year follow-up. Further, the rate of clinical failure, either graft rupture or significant rotatory laxity on examination, for this subgroup was even higher at 40%. Meanwhile, a meta-analysis by Cruz et al 4 estimated a 16.6% graft rupture rate for patients ≤19 years of age treated with ACLR using HS. In contrast, several studies have shown promising early- and mid-term results for ACLR using quadriceps tendon (QT) in adolescents, with multiple meta-analyses finding graft rupture rates of ≤7.5% for these patients.15,17 This research, as well as direct comparisons suggesting lower graft rupture rates and better functional outcomes for QT compared with HS, 10 has fueled increasing interest in the use of QT for adolescents undergoing ACLR.
Prior research has also found a protective effect of ACLR against subsequent meniscal tears,5,13,20 highlighting the fact that the ACL-deficient knee is at increased risk of injury to secondary stabilizers of the knee, including the menisci. Thus, not only frank graft rupture, but also subsequent meniscal tear may be a sign of ACL graft insufficiency. However, because most studies have focused only on graft rupture as a marker of ACLR failure, true rates of graft failure among adolescents and adults may be underestimated.
Thus, the goal of the current study was to determine both the rate of graft rupture and the rate of subsequent meniscal tear for adolescent patients undergoing ACLR with autograft HS or QT. It was hypothesized that, compared with HS autograft, QT autograft would be associated with lower rates of both graft rupture and subsequent meniscal tear.
Methods
This was a study of adolescent patients who underwent ACLR using either HS or QT autograft between 2009 and 2023 at an urban tertiary care pediatric hospital. After institutional review board approval, retrospective review of all patients aged 10 to 19 years at the time of surgery was performed. Patients with <2 years of clinical follow-up, those with congenital absence of the ACL, and those who underwent reconstruction with a graft other than HS or QT autograft were excluded. Demographic information, anthropometric data, injury details, surgical details, and follow-up events were catalogued. Follow-up events included both ACL graft rupture and subsequent isolated meniscal tear without ACL graft rupture. We also analyzed a composite endpoint to describe graft insufficiency, which was having ACL graft tear and/or isolated meniscal tear. Meniscal and ACL tears were identified on magnetic resonance imaging, which was obtained for all follow-up events. A subsequent meniscal tear was defined as a new tear (if the meniscus was deemed stable intraoperatively at the time of primary ACLR) or a retear (if the same meniscus was torn and repaired at the time of primary ACLR).
Surgical Details
Five surgeons contributed cases to this study (including T.J.G. and K.J.M.). Prior to 2020, HS autograft with suspensory fixation on each side was routinely used for ACLR at the host institution. A 4-strand graft consisting of folded-over gracilis and semitendinosus autograft was routinely used. In occasional circumstances, 1 or both of the grafts was tripled over to increase graft diameter. Due to accruing evidence showing lower failure rates with QT autograft, our group switched to the routine use of QT autograft with suspensory fixation on both sides in 2020. All cases of QT were all–soft tissue grafts. These were routinely harvested 10-mm wide and partial thickness, with the typical graft measuring 9 to 11 mm in diameter after graft preparation. Allograft supplementation was not done in any case.
Statistical Analysis
Descriptive statistics for patient characteristics, surgical details, and follow-up details were calculated and reported as n (%) for categorical variables, mean ± SD for normally distributed continuous variables, or median (range) for non-normally distributed continuous variables (based on Shapiro-Wilk testing). Bivariate analysis was then performed to evaluate the relationship between graft source (HS vs QT autograft) and other independent variables. Chi-square and Fisher exact tests were performed for categorical variables depending on sample size. t tests were performed for normally distributed continuous variables. Mann-Whitney U tests were performed for nonnormally distributed continuous variables. Multivariable logistic regression was then performed to evaluate the relationship between graft failure endpoints and relevant variables. This was done using an initial model with all considered independent variables and employing a backward selection technique with a threshold to retain of P≤ .20. Regression analysis was also conducted for the outcome of subsequent meniscal tear (without graft rupture) and for the composite outcome of graft rupture or subsequent meniscal tear. Statistical significance was set at P < .05.
Results
Between 2009 and 2023, 2115 patients aged 10 to 19 years underwent ACLR using either HS or QT autograft at our institution. A total of 1647 patients were excluded for having <2 years of clinical follow-up. One patient was excluded for congenital absence of the ACL. This left 467 of 2115 (22.1%) patients (52.0% female) with mean age at the time of surgery of 14.6 ± 1.9 (range, 10.1-19.9) years (Table 1, Figure 1). Median follow-up was 3.1 (2.0-13.4) years. The majority of patients were White (69.8%). Most patients underwent ACLR using HS autograft (67.5%), and 73.7% of the cohort were determined to also have a meniscal tear at the time of primary ACLR. The QT subgroup more commonly underwent concomitant anterolateral ligament reconstruction/lateral extra-articular tenodesis (ALL/LET) at the time of primary ACLR (9.2% vs 1.3%; P < .001), exhibited slightly higher age (14.9 vs 14.5; P = .04), had higher baseline body mass index (BMI) (22.3 vs 21.7 kg/m2; P = .01), had a shorter period of follow-up (2.8 vs 3.4 years; P < .001), and more commonly had concomitant medial meniscal tear compared with the HS group (33.6% vs 24.8%; P = .047). All-epiphyseal technique was more common in the HS subgroup (17.5% vs 2.6%; P < .001). No significant relationship was found between graft source and sex, race, or laterality.
Demographics and ACLR Details by ACL Graft Source a
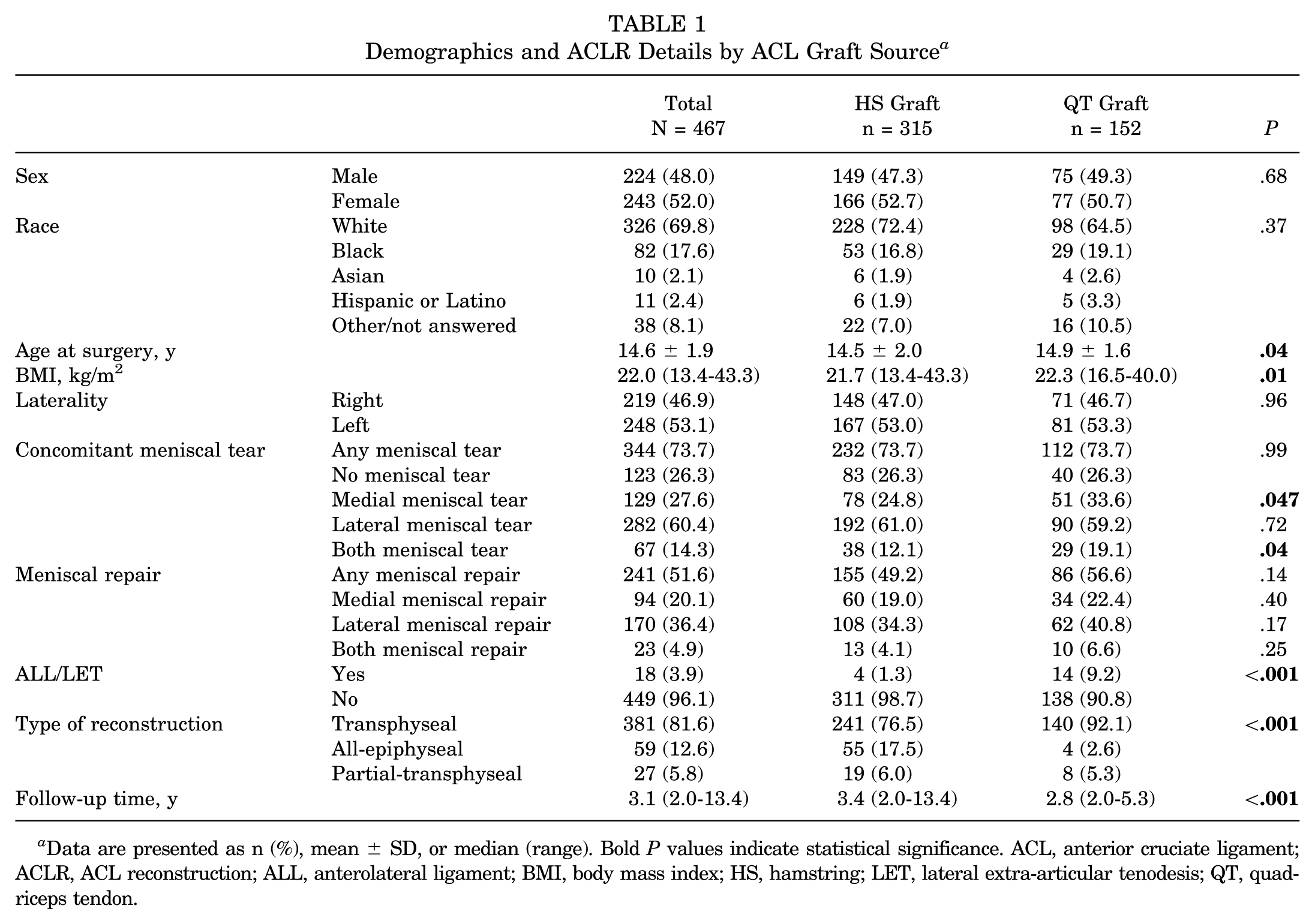
Data are presented as n (%), mean ± SD, or median (range). Bold P values indicate statistical significance. ACL, anterior cruciate ligament; ACLR, ACL reconstruction; ALL, anterolateral ligament; BMI, body mass index; HS, hamstring; LET, lateral extra-articular tenodesis; QT, quadriceps tendon.

CONSORT (Consolidated Standards of Reporting Trials) study diagram. ACL, anterior cruciate ligament; HS, hamstring; QT, quadriceps tendon.
Graft rupture occurred in 84 patients (18.0%), with a higher rate in the HS subgroup (23.2% vs 7.2%; P < .001). Subsequent meniscal tear (without graft rupture) occurred in 36 patients, with a higher observed rate in the HS subgroup (9.2% vs 4.6%; P = .08). The composite endpoint of graft rupture or subsequent meniscal tear was experienced by 120 patients (25.7%), with a higher rate in the HS subgroup (32.4% vs 11.8%; P < .001) (Table 2). A total of 86.9% of all graft failures (graft rupture or subsequent meniscal tear) occurred within 2 years of primary ACLR. Median time to graft failure was similar between the QT and HS subgroups (1.71 vs 1.77 years; P = .53). Though not considered to represent surgical failure, it was noted that 95 of 467 (20.3%) patients experienced a contralateral ACL tear during follow-up. There was no significant difference in the rate of contralateral ACL tear between the QT and HS subgroups (17.8% vs 21.6%, respectively; P = .34).
ACL Graft Tears and Subsequent Isolated Meniscal Tears by Graft Source a

Data are presented as n (%). ACL, anterior cruciate ligament; HS, hamstring; QT, quadriceps tendon.
Without ACL graft rupture.
Isolated meniscal tears were deemed retears if the same meniscus (medial or lateral) respective to the primary ACL injury was torn and were deemed new tears if that meniscus had not been injured at the time of primary ACL injury.
In bivariate analysis (Table 3), graft rupture was associated with HS graft source (P < .001), longer follow-up (P = .03), and lateral meniscal repair at the time of index surgery (P = .02). Subsequent meniscal tear was associated with medial meniscal tear (P = .002) and medial meniscal repair (P = .001). Meanwhile, the composite outcome of graft rupture or subsequent meniscal tear was associated with HS graft source (P < .001), longer follow-up (P = .003), and lateral meniscal repair at the time of index surgery (P = .005).
Bivariate Analysis for Relationships Between Independent Variables and 3 Different Outcomes a

Data are presented as n (%), mean ± SD, or median (range). Bold P values indicate statistical significance. ALL, anterolateral ligament; BMI, body mass index; HS, hamstring; LET, lateral extra-articular tenodesis; QT, quadriceps tendon.
A regression model was fitted using all the independent variables listed in Table 3 with graft rupture as the outcome of interest. The resulting model is detailed in Table 4, along with similar models examining different outcomes (isolated meniscal tear and graft rupture or meniscal tear). These analyses showed that, when controlling for other variables, the use of QT (compared with HS) was protective against graft rupture (odds ratio [OR], 0.29; P < .001); length of follow-up and lateral meniscal repair at index surgery were also predictive of graft rupture (OR, 1.16, P = .045; OR, 0.52, P = .02). When considering subsequent meniscal tear in isolation, the only statistically significant predictor found was concomitant medial meniscal tear at the time of index surgery (OR, 2.99; P = .002). Post hoc power analysis showed that >1100 patients would be needed to detect a difference in rate of subsequent meniscal tear with 80% power (retaining the observed allocation ratio). When considering the composite variable of graft rupture or subsequent meniscal tear, lateral meniscal repair at index surgery, length of follow-up, and graft source were significant predictors (OR, 0.54, P = .01; OR, 1.20, P = .01; OR, 0.33, P < .001).
Final Logistic Regression Models a

Bold P values indicate statistical significance.
Discussion
This study explores the rates of graft failure and subsequent meniscal tear in a large series of adolescents who underwent ACLR using HS or QT autograft at minimum 2-year follow-up. Analysis revealed that the QT group had significantly lower odds of ACL graft rupture compared with the HS group. This supports the theory that QT graft is more effective than HS tendon graft in conferring stability to the knee after ACLR in adolescents. In comparison with ACLR using HS, prior research has associated ACLR using QT with better functional outcomes, similar postoperative pain scores, and lower risk of graft rupture in adolescents and young adults.10,12,15,17-19,23 The current study builds on this base of literature, suggesting that the risk of graft rupture among adolescents treated with QT autograft is significantly lower than that of adolescents treated with HS autograft. This finding persisted when controlling for other independent variables, including length of follow-up, sex, and lateral meniscal repair at index surgery. Interestingly, the rate of graft rupture for ACLR using QT in this study is in line with rates reported in meta-analyses. 4
Although the observed rate of subsequent meniscal tear was twice as high in the HS group in this study, the associated difference did not reach statistical significance, possibly because of a lack of achieved power. This finding is provocative and potentially clinically significant because, although a subsequent isolated meniscal tear may be attributed to a failure of a treated meniscal tear to heal, it may also be the result of subtle instability in the knee due to a suboptimally functioning ACL graft. This type of ACL insufficiency may be an underappreciated presentation of surgical failure, as prior research has shown that a functioning ACLR protects against subsequent meniscal tear.5,13,20 While ACL insufficiency is one possibility, it is important to note that isolated meniscal tears also occur in knees with intact and functioning native ACLs. So, while the identified difference in subsequent meniscal tear rates does not represent definitive evidence, it does support the authors’ hypothesis that QT grafts restore functional knee stability more effectively than HS grafts.
Although logistic regression showed an association between graft rupture and lateral meniscal repair at the time of index surgery, the mechanism for this association is unclear. One possible explanation is that peripheralization of the lateral meniscus due to repair negatively affects the stabilizing function of the structure, predisposing the patient to further injury. Another possibility is that patients undergoing lateral meniscal repair have, on average, more severe pivot-shift displacement of the knee at the time of injury. This may reflect a more severe initial injury pattern, perhaps with a higher rate of subtle posterolateral corner injury that increases the risk of graft rupture. This relationship certainly calls for further research to replicate this finding and ascertain an explanation.
Limitations
Limitations of the study include the following. First, a large number of patients were excluded from this study because of lack of follow-up, which could introduce bias. It is also acknowledged that the difference in the subgroups’ event rates may be partly due to disparity in follow-up length, as surgeries with HS grafts were generally done at earlier time points than those with QT grafts, allowing for greater cumulative postsurgical risk exposure for patients with HS grafts. Despite this concern, it was noted that median time to graft failure event was similar between the QT and HS subgroups and almost 90% of graft ruptures occurred within 2 years from primary ACLR in both subgroups. Additionally, multivariable analysis accounting for follow-up length consistently showed a strong influence of graft type on outcomes, suggesting that the relationship between outcomes and graft type was not due to a lead-time effect. It is also recognized that the groups showed some significant differences, with the QT group exhibiting older age at surgery, a higher proportion of ALL/LET, and a lower proportion of all-epiphyseal reconstructions. Despite the multivariable regression, it is recognized that these differences might be sources of confounding, especially considering the improvement in graft failure associated with ALL/LET.14,21 Finally, there were no data available on graft diameter, which has been shown to be a risk factor for HS grafts.
Table 1 also reveals demographic differences among the QT and HS subgroups that are expected, given the changing treatment recommendations and demographics of patients treated at the host site. Based on research and local experience, the preferred graft for ACLR evolved from HS autograft to QT autograft at the host institution around 2019 to 2020. This was a time that the host institution treated an increasing number of older adolescents and young adults due to evolution in the regional sports medicine market. The fact that age tended to be higher for the QT subgroup is therefore not surprising. Following similar logic, the higher BMI observed in the QT subgroup is likely related to demographic changes among adolescents nationwide over the past 2 decades.
It is also recognized that the observed rates of graft rupture and subsequent meniscal tear for both the QT and the HS subgroups may be biased higher than reality in this study. This is because of the retrospective nature of our study and the requirement for a minimum 2-year follow-up, as most patients who are doing well will not return to clinic after 1 year, as many surgeons do not require regular follow-up after patients are cleared for sports. Therefore, patients who have ≥2 years of follow-up are more likely to have experienced a problem motivating their extended follow-up. By this reasoning, the reported rate of contralateral ACL rupture may also be inflated.
Additionally, the single-center nature of this study may limit generalizability. As noted above, despite including patients over a large period, this study may have been underpowered to find smaller differences between the subgroups. While the utility of lateral extra-articular procedures such as ALL reconstruction and LET are popular topics, the current study data were limited in their ability to address this topic, as there were only 18 cases of ALL/LET in the series, with 14 of 18 being in the QT subgroup. Future prospective, multicenter studies with longer-term follow-up could validate these findings and improve generalizability.
Conclusion
This study showed that adolescents undergoing ACLR with QT autograft have a significantly lower risk of graft rupture than those undergoing ACLR with HS autograft, even after controlling for potential confounding variables. Lateral meniscal repair at index surgery and length of follow-up were also predictors of graft rupture. The observed difference in subsequent meniscal tears between the QT and HS subgroups was not statistically significant, but concomitant medial meniscal tear at index injury was predictive of subsequent meniscal tears.
Footnotes
Final revision submitted November 18, 2025; accepted December 13, 2025.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Children's Hospital of Philadelphia institutional review board (No. 16-013464).