
Abstract
Purpose:
The objective of this study is to discuss the fact that whether graft rupture after successful anterior cruciate ligament (ACL) reconstruction surgery is due to graft failure or re-injury to the reconstructed ACL.
Methods:
In total, 340 sportspersons, meeting our inclusion criteria, were assessed for rupture of ipsilateral ACL graft and ACL injury of the contralateral knee. Patients with ipsilateral ACL graft rupture were labelled as group 1, while those with contralateral ACL injury were labelled as group 2. Both groups were compared for potential risk factors for ACL injury, and statistical analysis was performed to study whether the graft acted as an additional risk factor.
Results:
Of the 340 sportspersons, 25 patients suffered a total of 26 injuries. Ipsilateral graft rupture rate was 2.4% (8 of 340) at a mean follow-up of 25.5 ± 40.57 months, and the contralateral ACL injury rate was 5.3% (18 of 340) at a mean follow-up of 18.11 ± 19.97 months, with an overall re-injury rate of 7.6%. Both groups were comparable for risk factors for ACL injury: age (p = 0.255), gender (p = 0.534), mode of re-injury (p = 0.523), level of sports activity, type of graft used (p = 0. 918), graft diameter (p = 0.607), duration from injury to index surgery (p = 0.492), duration from index surgery to re-injury (p = 0.638), timing of return to sports after index surgery (p = 0.303), duration of sporting activity before second injury (p = 0.657), and Tegner’s level of sports activity (p = 0.486).
Conclusion:
Because the rate of contralateral ACL injury is higher than the ipsilateral graft rupture and the risk factors for ACL injury are comparable in both groups at a follow-up period, which is suggestive of ligamentization of the graft, we suggest that it might be an ACL re-injury rather than graft failure.
Keywords
Introduction
Injury to anterior cruciate ligament (ACL) is one of the most common and serious knee injuries occurring in sportspersons. 1 The incidence of primary ACL injury has been reported to be around 1.5–1.7% per year in healthy athletic population. 2 Furthermore, a re-injury in the form of rupture of ipsilateral graft or a tear of contralateral native ACL is a devastating outcome following successful ACL reconstruction, rehabilitation and return to sports. 3 Systematic review of prospective studies identified the ACL graft rupture risk to be 1.8–10.4% and risk of ACL injury in the contralateral knee to be 8.2–16.0%. 4,5 There are multiple risk factors responsible for the primary knee injury such as age, gender, level of sports activity, anatomical variability like posterior tibial slope, narrow notch width, small size ACL, limb alignment and multiple neuromuscular factors. 6 O of these risk factors, the anatomical risk factors remain non-modifiable. In addition to these, there are other risk factors for re-injury which include mode of re-injury, type of graft used in primary surgery, graft diameter, tunnel positioning, duration between primary surgery and re-injury, which predispose the operated knee or contralateral knee to a second injury. 6
Literature is silent over the argument that whether graft rupture occurring in a technically sound ACL reconstruction surgery, with satisfactory postoperative rehabilitation and successful return to sports, is due to graft failure or re-injury to the reconstructed ACL.
We hypothesize that ACL graft rupture (after successful ACL reconstruction and return to sports) might be a re-injury, not a graft failure.
Materials and methods
The principal author is one of the senior most surgeons at our centre and in charge of the sports injury centre at our institute. We, at this centre, have performed 1936 ACL reconstruction surgeries in the past 10 years using two types of graft techniques, that is, bone patellar tendon bone (BPTB) graft and semitendinosus–gracilis graft (STG). 7 All the surgeries have been performed by the first author. Records of all the patients are kept in the department, and the patients are evaluated on regular follow-up. In this study, we have evaluated ACL graft re-injury/failure and contralateral ACL injury in sportspersons. This is a retrospective evaluation of meticulously maintained data of ACL reconstruction surgery performed in the last 10 years.
Inclusion criteria for this study were as follows:- Sportspersons operated for isolated ACL tear at our centre in the last 10 years Age: 16–40 years Patients who were willing to participate Patients who had returned back to sports after the index surgery
Exclusion criteria were as follows:- All patients with multi-ligamentous tears Simultaneous ACL injury to both knees Patients operated earlier for any knee problem other than ACL reconstruction
These patients were divided into two groups, depending upon the type of second injury. The cohort of patients with ipsilateral graft re-injury/failure was labelled as group 1, while the cohort of patients with contralateral ACL injury was labelled as group 2. Both groups were compared for potential risk factors for ACL injury: age, gender, mode of re-injury, type of graft used in index surgery, graft diameter, activity level (International Knee Documentation Committee (IKDC)) 8 at the time of re-injury, duration from injury to index surgery, duration from index surgery to re-injury, timing of return to sports after index surgery, duration of sporting activity before second injury and Tegner’s level of sports activity 9 at the time of re-injury.
Statistical analysis
Quantitative data were presented as mean ± SD or median and interquartile range, as appropriate. Normality of data was checked by Kolmogorov–Smirnov tests of normality. For skewed data or scores, Mann–Whitney test for two groups was applied. For normally distributed data, two groups were compared using independent t-test. Proportions were compared using the χ 2 or Fisher’s exact test, depending on their applicability. All the statistical tests were two-sided and performed at a significance level of α = 0.05. The analysis was conducted using IBM SPSS STATISTICS (version 22.0).
Results
Of the 1936 ACL reconstruction surgeries performed in the last 10 years, a total of 340 patients (314 males, 26 females) fulfilled the inclusion criteria. Oof these, 25 patients suffered a total of 26 injuries (7.6%). There were 21 males and 4 females.;8 patients suffered from ipsilateral graft rupture (group 1) and 18 patients suffered from contralateral ACL injury (group 2). Ipsilateral graft rupture rate was 2.4% (8 of 340) and contralateral ACL injury rate was 5.3% (18 of 340) with an overall re-injury rate of 7.6% (Table 1). One patient suffered both, contralateral ACL injury at 12 months and ipsilateral graft rupture at 125 months.
Ipsilateral graft rupture rate, contralateral ACL injury rate and overall re-injury rate.

ACL: anterior cruciate ligament.
Age distribution
The average age distribution of patients in group 1, group 2 and in all the cases of index ACL surgery is summarized in Table 2. Comparison of age distribution between group 1 and group 2 is statistically insignificant.
Age distribution.

ACL: anterior cruciate ligament.
Gender distribution
The gender distribution of patients in group 1, group 2 and in all the cases of index ACL surgery is summarized in Table 3. Comparison of gender distribution between group 1 and group 2 is statistically insignificant.
Gender distribution.

Mode of re-injury
The mode of re-injury in patients of both groups is summarized in Table 4. Comparison between both groups is statistically insignificant.
Mode of re-injury.

Type of graft used in index surgery
Details of type of graft used in index surgery in both groups are given in Table 5. Comparison between the two groups is statistically insignificant.
Type of graft used in index surgery.

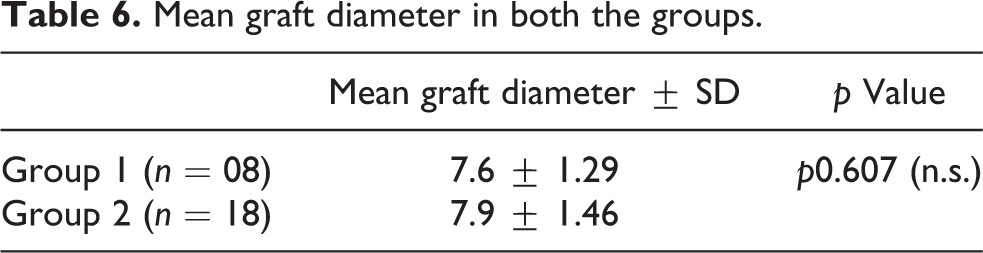
Graft diameter
The average graft diameter in both groups is summarized in Table 6. Comparison between the two groups is statistically insignificant.
Mean graft diameter in both the groups.
Activity level (IKDC) at the time of re-injury
Distribution of patients depending on the activity level classification is summarized in Table 7. Comparison between the two groups is statistically insignificant.
Activity level (IKDC) at the time of re-injury.

Mean duration between injury and index surgery
Mean duration between injury and index surgery in both the groups is summarized in Table 8. Comparison between both the groups is statistically insignificant.
Duration between injury and index surgery.

Mean duration between index surgery and re-injury
The mean duration between index surgery and re-injury in both groups is summarized in Table 9. Comparison between the two groups is statistically insignificant.
Duration between index surgery and re-injury.

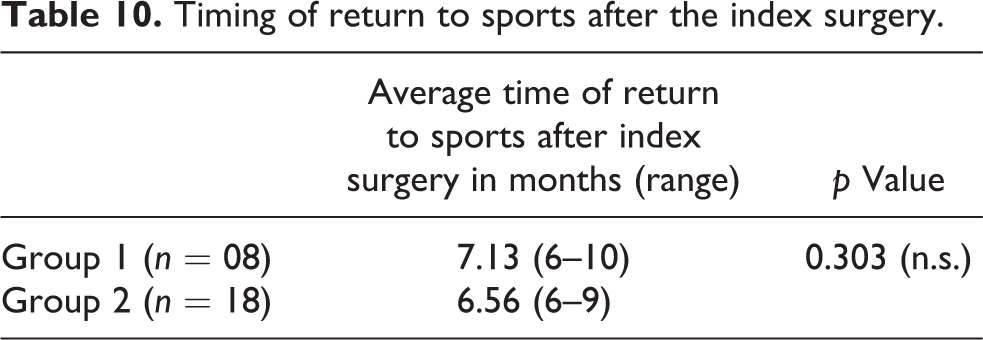
Timing of return to sports after the index surgery
Average time to return to sports after the index surgery in both groups is summarized in Table 10. Comparison between both groups is statistically insignificant.
Timing of return to sports after the index surgery.
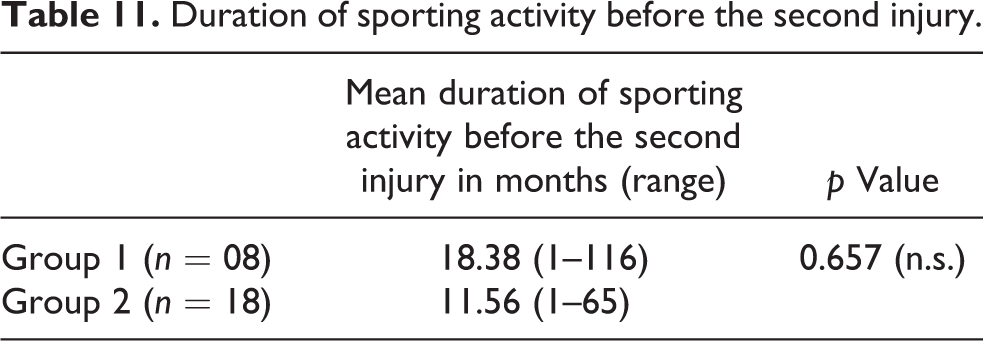
Duration of sporting activity before the second injury
Average duration of sporting activity before the second injury in both groups is summarized in Table 11. Comparison between both groups is statistically insignificant.
Duration of sporting activity before the second injury.
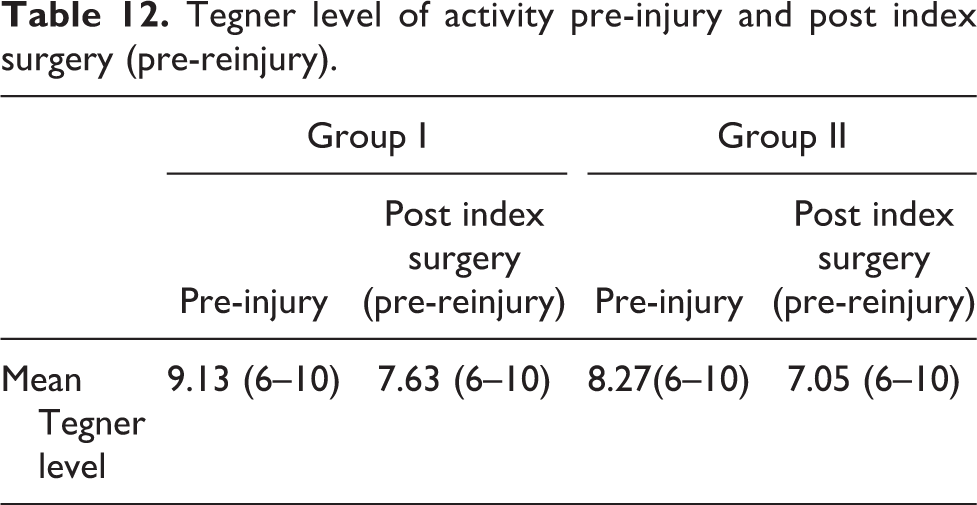
Tegner level of activity pre-injury and post index surgery (pre–re-injury)
Tegner level of activity pre- and post-index surgery (pre-reinjury) in both groups is summarized in Table 12. Comparison between both groups in terms of Tegner level of activity pre-reinjury is statistically insignificant (p = 0.486)
Tegner level of activity pre-injury and post index surgery (pre-reinjury).
Discussion
Despite the extensive literature available on the outcome of ACL reconstruction surgery using BPTB and STG autografts, no consensus has yet been reached over the superiority of one over the other. 10 –15 Some studies consider BPTB graft as the gold standard for ACL reconstruction in sportspersons due to its low level of laxity, high durability and a larger graft diameter as compared to the STG graft. 16,17 However, comparable anterior knee laxity between BPTB and hamstring grafts, over a long-term follow-up, has also been reported. 18 Hence, it would be unwise to attribute every graft rupture to graft failure without ruling out whether the graft actually acts as a risk factor. Our study points against the graft acting as a risk factor for failure as a re-injury occurring after 12–24 months of index surgery is bound to cause tear of contralateral ACL (native) or reconstructed ACL (which behaves like a native ACL eventually over a long-term follow-up) independent of each other.
In the current study, ipsilateral graft rupture rate was 2.4% (8 of 340) at a mean follow-up of 25.5 ± 40.57 months and contralateral ACL injury rate was 5.3% (18 of 340) at a mean follow-up of 18.11 ± 19.97 months, with an overall re-injury rate of 7.6%. Other studies have identified a risk for ACL graft rupture in the range of 2–5% at 2 years of follow-up, 19 –23 which is consistent with the finding in our study. The contralateral tear rate at 2-year follow-up has been described to be nearer to ipsilateral graft rupture rate, 22 with rate of contralateral ACL tear increasing to almost double the ipsilateral graft tear rate at 5-year follow-up. 5 In a systematic review by Wright et al., ipsilateral ACL graft rupture risk was identified to be 1.8–10.4% and risk of ACL injury in the contralateral knee to be 8.2–16.0% at a minimum follow-up of 5 years. 5 In our study, a contralateral ACL tear rate (5.3%) of almost the double of ipsilateral graft tear rate (2.4%) has been observed at short to midterm follow-up. This increased risk for contralateral knee could be multifactorial.
However, deconditioning of the contralateral knee due to lack of rehabilitation during recovery from ipsilateral knee has been cited as a possible reason for the same. 5
In the first 12 months after surgery, incidence of ACL graft rupture has been reported to be significantly higher than incidence of injury to contralateral ACL. This can be attributed to relative graft weakness, while the graft is going through stages of remodelling and maturation. 24 By 12 months, the process of ligamentization is complete and the graft behaves like a native ACL. 24,25 However, some studies suggest that maturation takes 2–3 years to complete, 26,27 but it appears that after 12 months, the graft is at no greater risk than the contralateral ACL. 24 Contrast-enhanced MRI has been reported to show ligamentization process in animal models. 28 However, its role in humans is still a topic of research and debate. Biopsy taken from the reconstructed ACL is the gold standard to confirm ligamentization, and these time frames suggested by these reports are derived from biopsy studies undertaken in humans. 29
Sixteen percent of the patients with re-injury were females (4 of 26), whereas total female sportspersons in the study group were only 7.6% (26 of 340). Some other studies have also reported higher re-injury rate in females as compared to males. 30,31 The higher incidence of re-injury may be related to extrinsic factors such as access to training facilities and conditioning factors and intrinsic factors such as anatomical and hormonal variability. 32,33
Return to a pivoting or cutting sport increases the chances of ipsilateral graft injury as well as contralateral ACL injury. 24 In our study too, most of the cases of re-injury (24 of 26) occurred in sportspersons who returned to level 1 or level 2 of activity.
Various risk factors for ACL injury and re-injury described in the literature have been studied, and comparison of these risk factors between the two groups (ipsilateral reconstructed ACL and contralateral native ACL) has been performed. Because this comparison has been performed at a mean follow-up of 18–24 months, it might be safe to assume that the graft had undergone ligamentization and was behaving like a native ACL at the time of re-injury.
Statistically insignificant comparison between the two groups at a follow-up period which is suggestive of maturation of graft further provides the indirect evidence that it might be an ACL re-injury rather than graft failure.
Thus, it is important to identify individuals with risk factors for ACL injury at the time of index surgery, so that they can be counselled about the high risk of re-injury, and stringent physiotherapy, rehabilitation and conditioning in such cases should be carried out.
Limitations
Anatomical risk factors for re-injury, such as notch width, tibial slope, knee alignment, have not been studied. Surgical factors, such as tunnel placement, graft tensioning, also play a role in causing re-injury. We were able to minimize this bias using a single experienced surgeon, standard operative technique, standard graft fixation and uniform rehabilitation protocol. Number of cases in the study is less. However, graft rupture rate in itself is low, as described in the literature 5 ; therefore, larger multicentric studies are required to further validate this study.
Conclusion
Because the rate of contralateral ACL injury is higher than the ipsilateral graft rupture and the risk factors for ACL injury are comparable in both groups at a follow-up period, which is suggestive of ligamentization of the graft, we suggest that it might be an ACL re-injury rather than graft failure.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.