
Abstract
Background:
The outcomes of Achilles tendon tears have been minimally investigated in adolescents and young adults, with sparse literature-based evidence to guide management.
Purpose/Hypothesis:
The purpose of this study was to describe the demographics, presentation, treatment, complications, and long-term functional follow-up including patient-reported outcomes (PROs), and return-to-sport (RTS) rates of adolescent and young adult athletes with Achilles tendon ruptures. It was hypothesized that despite high activity demands, perioperative complication rates would be low and RTS rates high.
Study Design:
Case series; Level of evidence, 4.
Methods:
Records were reviewed of all patients aged <25 years treated at 1 of 2 pediatric tertiary care centers for an Achilles tendon tear or laceration between 2004 and 2018. Demographics, imaging, treatment, and clinical follow-up data were retrospectively collected. Patients ultimately managed without surgery were rare and excluded. Patients with >1 year of clinical follow-up or those who responded to prospective patient outreach for PRO collection were investigated for clinical outcomes, utilizing the Achilles Tendon Total Rupture Score (ATRS), Foot and Ankle Outcome Score (FAOS), Tegner Activity Scale (TAS), and questions about reinjury and RTS.
Results:
Of the 38 patients identified, 24 (63%; mean age, 18.9 years; range, 10.4-22.8 years; 42% male) were analyzed for clinical outcomes. A total of 22 patients (92%) had complete tears, 2 had partial tears. Twenty patients (83%) returned questionnaires at a median 6.3 years (IQR, 3.4-9.7 years) while the other 4 patients were seen in clinic at a median of 1.2 years (IQR, 1.0-1.8 years) following injury. The median postoperative ATRS score was 96 (IQR, 82-100) and median TAS score was 6 (IQR, 4-8). Median FAOS scores were excellent for symptoms (91), pain (100), activities of daily living (100), and sports (98) and good for quality of life (88). The 6-month RTS probability was 47% (95% CI, 19%-66%) and at 12 months was 95%. The median time to RTS for partial tears was 5.6 months versus 6.6 months for complete tears (P = .05). Seven patients (29%) experienced a perioperative complication including 3 cases of delayed wound healing (13%) and 1 tendon retear (4%), which underwent revision repair.
Conclusion:
Adolescent and young adult athletes surgically treated for high-grade Achilles injuries had favorable long-term outcomes, low rerupture rates, and median RTS timing (~6 months) similar to that reported in adult studies.
Achilles tendon tears are significant ankle injuries that occur most commonly in men in their fourth, fifth, or sixth decade of life, but are rare in children and adolescents.14,29 These tears have been shown to affect about 5.5-31.17 per 100,000 people annually, although recent literature has demonstrated that the incidence may be increasing.14,22,29 High-demand sports, played either competitively or recreationally, are commonly associated with this injury, and the underlying mechanism is often caused by a sudden contraction of the muscle, associated with jumping, landing, or forcefully pushing off the ground.14,18,20,29 While not directly studied, injury mechanisms are believed to be similar in the pediatric population with the exception of a higher number of Achilles injuries due to lacerations.
Management of Achilles tendon tears remains controversial, with both surgical and nonsurgical treatment showing generally favorable outcomes.4,19,28 A variety of surgical techniques have been described but most commonly consist of open or percutaneous suture-based tendon repair, while nonoperative methods typically rely on initial immobilization in a cast or functional brace, followed by progressive activity.4,18,28 Literature in favor of surgical repair has noted a significant decrease in rerupture rates and an overall benefit in patient-derived utility values.15,22 Surgical repair potentially allows for earlier motion during the rehabilitation process, which may result in superior functional results. 25 In contrast, other studies have shown no significant differences in rerupture rates between the 2 treatment groups and have reported that surgical repair leads to higher complication rates.4,19,26 However, nearly all of these data are reported on adult populations, and to our knowledge, there are no studies describing treatment and outcome of Achilles injuries specifically in adolescents and young adults.
The primary purpose of this study was therefore to describe details of the demographics, presentation, treatment, complications, patient-reported outcomes (PROs), and return-to-sport (RTS) rates of adolescent and young adult athletes with Achilles tendon tears that were surgically managed. The study hypothesis was that the perioperative complication rates would be low and RTS rates high for this unique subpopulation.
Methods
Patient Selection
After institutional review board approval, queries were performed on orthopaedic departmental databases at 2 different pediatric centers to identify all patients <25 years of age who were treated for a partial or complete Achilles tear between January 1, 2004, and December 31, 2018. The search resulted in 41 patients, for whom demographic, imaging, and treatment data were retrospectively collected from the patients’ medical records. Demographic data included age at surgery, sex, body mass index (BMI), laterality, sport during which injury occurred, mechanism of injury, and any comorbidities. Imaging, such as magnetic resonance imaging (MRI) and/or ultrasound, was reviewed for the location of the tear. Categorization of tear location was divided into thirds, based on typical tendon length with “distal” tendon tears quantified as <2.5 cm from the calcaneal tendon insertion, “midtendinous” tears as 2.5 cm to 5.0 cm from the insertion, and “proximal” tears as >5.0 cm from the insertion. Tear location and gap size, as measured in millimeters, were measured by 1 of 3 senior authors (D.E.K., J.J.B., B.E.H.), based on MRI, or based on radiologist-described ultrasound reports. Treatment data included surgical repair versus nonsurgical management, time from injury to surgery, size of incision, repair technique, duration of immobilization (cast versus boot), and time to initiation of posttreatment weightbearing. Three patients were nonsurgically managed and, given the small number, were excluded from analysis, leaving a final total of 38 patients. A total of 24 patients who were followed for ≥1 year postinjury with either a clinic visit or a PRO collection response were included in the outcome analysis and were termed the “clinical outcomes cohort.”
Surgical Procedures
The procedures were performed under general anesthesia by 1 of 5 different surgeons (D.E.K., J.J.B., Y.M.Y., B.E.H.), with minimal variation in technique. Patients were positioned prone and a tourniquet was utilized. The contralateral ankle was assessed with the knee in flexion prior to preparing and draping to get a sense of normal Achilles tension based on ankle plantarflexion. An open approach to the tear site was then utilized centered over the gap site. The paratenon of the Achilles tendon was exposed and preserved for later repair.
Both ends of the tear were then identified. Minimal to no debridement of the tear ends was needed, as significant preexisting disease is rarely encountered in this young population. The proximal portion of the tear was freed up to allow for distalization. The tear was then repaired utilizing a nonabsorbable braided suture placed in the proximal and distal tendon sites with either direct repair utilizing traditional locking sutures (Krakow technique) or utilizing the “Giftbox” technique.13,16 In each case, tear sites were approximated with the goal of slight overtensioning compared with the contralateral side. In 1 very distal tear, an anchor was added into the calcaneus to supplement the repair. The paratenon was then repaired over the tear site.
The dermis was closed with absorbable sutures and the skin with nonabsorbable simple or mattress sutures with a posterior plaster splint or fiberglass cast placed in the resting position of the ankle in plantarflexion for the first 2 weeks. Rehabilitation then progressed, per surgeon preference, with wound inspection and transition from splint to either cast or boot with protected weightbearing at the 2- or 3-week postoperative mark. Weightbearing was allowed in a boot using Achilles wedges, at 4 to 6 weeks postoperatively, with a progressive decrease in wedge height along with physical therapy to regain range of motion and gradual progression of strengthening. RTS and activities were dictated by return of range of motion and strength in physical therapy.
Patient-Reported Outcomes
All patients were contacted via mail, then email and/or telephone outreach, and asked to complete long-term PRO questionnaires. No preoperative PROs were collected because of the retrospective design of the study. PROs included the Achilles Tendon Total Rupture Score (ATRS), 11 Tegner Activity Scale (TAS), Foot and Ankle Outcome Score (FAOS), and a self-designed Achilles Study Questionnaire (ASQ). The FAOS was broken down into subsections: symptoms, pain, activities of daily living (ADL), function in sports and recreational activities (Sports), and quality of life (QOL). Scores 90 to 100 were considered excellent, 75 to 89 were considered good, 60 to 74 were considered fair, and <60 were considered poor. The ASQ included questions about retear/reinjury, injury to contralateral Achilles, and a direct yes/no question that asked if the patient was able to return to full sports participation without limitation.
Statistical Analysis
Patient demographic, imaging, and treatment characteristics were summarized for all patients using simple descriptive statistics. Categorical characteristics were summarized by frequency and percentage, while continuous characteristics were summarized by mean and standard deviation or median and interquartile range (25th percentile–75th percentile) when data deviated from normality. Analyses were conducted on all available characteristics to compare the clinical outcomes cohort and the short-term follow-up cohort.
Outcomes from the most recent clinical follow-up or from PROs were summarized for the clinical outcomes cohort. Continuous outcomes were summarized by median and interquartile range because of data distribution, and binary outcomes were summarized by proportion and 95% CI. Comparisons in outcomes across injury subgroups were conducted using a Wilcoxon rank-sum test, Kruskal-Wallis test, or Fisher exact test, as appropriate. Spearman rank correlation was used to assess associations between continuous characteristics and continuous outcome measures.
Survivorship analysis for RTS was performed using the Kaplan-Meier product-limit method to account for censoring. The 95% confidence limits about the survivor curve were estimated using the Greenwood formula. All analyses were conducted using R Version 4.3.0 (2024; R Core Team). 21 Kaplan-Meier estimates were computed using the survival package (2021; Therneau). 24
Results
In total, 38 patients met study inclusion criteria, 24 of which either had clinic follow-up or returned the PRO questionnaires at >1 year postinjury, and were included in the clinical outcomes cohort, with the remainder deemed the “short-term follow-up cohort” (Figure 1). The 2 cohorts were compared, and no statistically significant differences were observed (Table 1).

Strengthening the Reporting of Observational Studies in Epidemiology diagram of study population.
Cohort Analysis a

BMI, body mass index; Postop, postoperatively.
Two cases of chronic repair (described below) were excluded from time of injury to surgery analysis.
The clinical outcomes cohort (follow-up ≥1 year) summary is illustrated in Table 2. This cohort included 20 (83%) patients who returned patient questionnaires at a median of 6.3 years (IQR, 3.4-9.7 years) following injury, while the other 4 patients were seen in clinic at a median of 1.2 years (IQR, 1.0-1.8 years) following injury (Table 2). A total of 22 (92%) injuries were full Achilles tears and the remaining 2 were partial.
Clinical Outcomes Cohort Summary (n = 24) a

Data are presented as n (%) or mean ± SD. BMI, body mass index.
A high rate of lacerations was seen, including 8 of 38 (21%) of the entire cohort and 5 of 23 (22%) for the clinical outcomes cohort. These occurred in 5 male and 3 female patients (mean age, 16 years; range, 10-22 years) and included the 3 youngest patients in the entire cohort (ages 10, 10, and 12). Laceration items included glass (n = 3), ceramic fountain, mirror, rock, and hockey skate. Where documented, laceration location was distal (n = 3) and middle (n = 2). Of the 18 patients with known tear location, 4 were distal including 3 lacerations and 1 nonlaceration.
All patients underwent surgical repair with 1 of 3 primary repair techniques except for one patient who had a hybrid Krakow repair technique combined with calcaneal anchor fixation and Haglund’s deformity excision (Table 3). All cases were primary repairs, although 1 patient (healthy adolescent female basketball player) had a prior tear, and repair, of her contralateral Achilles.
Surgical Characteristics (n = 24) a

Data are presented as mean ± SD or n (%). PRO, patient-reported outcome.
Number column shows how many patients had the data available.
Excluding the 2 “delayed surgical repair” cases described in the text.
There were 2 cases of delayed surgical repair. One patient was a 22-year-old hammer thrower with an acute mechanism for sustaining a partial-thickness Achilles tear in the setting of a Haglund lesion, which led to chronic pain and weakness. Because this patient failed 6 months of nonoperative treatment with rest and platelet-rich plasma injections, surgical treatment consisted of Krakow suture repair with an anchor placed into the calcaneus to augment fixation, in addition to partial/minimal Achilles tendon debridement and excision of the Haglund deformity. The other patient was a 16-year-old hockey player who sustained a partial-thickness (approximately 66%) Achilles laceration from another player’s skate. He was treated initially with immobilization but had persistent symptoms of pain and weakness that required operative repair at approximately 3 months postinjury. At the time of surgery, scar and hypertrophic tissue was removed from the tear site and the tendon edges were reapproximated.
PRO Results
The median ATRS score at a minimum of 1 year postinjury was 96 (IQR, 82-100) and the median TAS score was 6 (4-8) (Table 4). FAOS outcome scores were excellent for symptoms (median, 91; IQR, 79-96), pain (100; 87-100), ADL (100; 94-100), and sports (98; 71-100), and were good for QOL (88; 67-100) (Table 4). No differences were detected in any outcome across sexes, age, tear type, tear location, sport, or method of injury.
Outcome Summary a
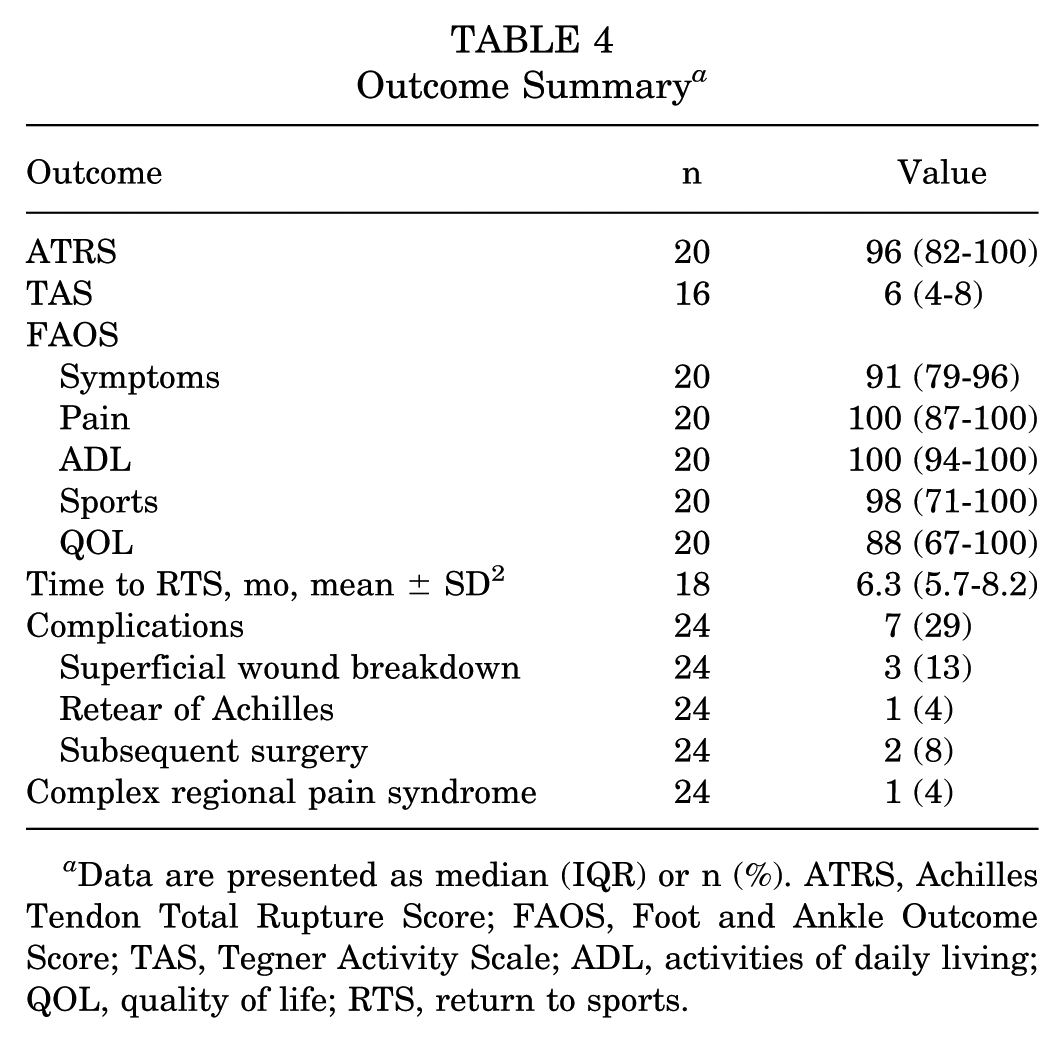
Data are presented as median (IQR) or n (%). ATRS, Achilles Tendon Total Rupture Score; FAOS, Foot and Ankle Outcome Score; TAS, Tegner Activity Scale; ADL, activities of daily living; QOL, quality of life; RTS, return to sports.
Return to Sports
Kaplan-Meier analysis determined that the median time to RTS was 6.3 months (95% CI, 5.8-9.2 months) (Figure 2). The 6-month RTS probability was 47% (95% CI, 19%-66%) and at 12 months was 95% (65%-99%). Median RTS for proximal injuries was 5.8 months, for middle injuries was 6.9 months, and for distal injuries was 5.6 months (P = .048). The median time to RTS for partial tears was 5.6 months versus 6.6 months for complete tears (P = .05). There were no differences in time to RTS by age, sex, sport, or method of injury.

Kaplan-Meier curve for the probability of return to sport.
Seven patients (6 female, 86%; mean age, 19.5 years, range, 16-22) experienced complications, which included 3 patients (13%) who either reported reinjury (n = 1; 4%) or need for additional/repeat surgical treatment (n = 2; 8%) (total of 12%; 95% CI, 3%-32%). The retear patient was a 22-year-old female collegiate gymnast who had an Achilles tendon retear at 25 months postoperatively, which required revision repair. The other 2 revision surgeries included 1 patient who underwent arthroscopy for anterior ankle impingement and talonavicular spurring at 1 year post–Achilles repair, and another patient who underwent surgery for excision of Haglund deformity at 2.5 years following Achilles repair. Both conditions were present at the time of initial Achilles repair. There were 3 cases of delayed wound healing that responded to oral antibiotics and local wound care and 1 patient who was diagnosed with complex regional pain syndrome at the 6-month visit, which was resolved through physical therapy with desensitization techniques and acupuncture by the time of the 9-month postoperative visit.
Discussion
This retrospective multicenter study reports good to excellent PROs and RTS in a group of 24 children, adolescents, and young adults (mean age, 18.9; range, 10.4-22.8) following surgical treatment of an Achilles tendon injury. There are several salient findings regarding this relatively rare injury in a younger population. While this was not a comparative study of operative versus nonoperative treatment, surgical repair was associated with favorable outcomes. A relatively high rate of lacerations as the mechanism of injury (8/38; 21%) was seen in this younger age group, including the 3 youngest patients in the cohort. Favorable results may provide some guidance for the optimal primary treatment in the setting of high-grade or complete lacerations in this population. Moreover, the case of an adolescent who could not regain a high activity level with nonoperative treatment of a partial tear may serve as a gentle caveat. Perhaps the most important finding is the persistence of excellent PROs in the 20 patients with relatively long-term follow-up, with median of 6.3 years postoperatively. Given the high PROs and rarity of retears (1/24; 4%) in our cohort, adolescents and young adults who undergo surgical repair for achilles tears should expect a favorable recovery and stable achilles repair even with continued athletic activity over time.
Historically, there is a paucity of literature on Achilles tendon injuries in patients <25 years old, and it comprises mostly case reports and small case series.2,7,9,10,12 Chen etal 7 retrospectively reported on 24 patients with a mean age of 16.3 ± 1.6 years, two-thirds of whom (aged 4-15 years) suffered Achilles lacerations. In their report of the remaining 8 patients, all skeletally mature adolescents (aged 13-18 years) sustained acute ruptures playing sports, most commonly basketball. Thus, while this subcohort was reported to have undergone successful surgical repair with no postoperative complications, no functional outcomes or PROs were included. 7 Recently, Ashebo etal 3 retrospectively reported successful management of 39 patients of median age 15 with Achilles injuries with median RTS at 6 months postinjury in the 22 patients with adequate follow-up data.
A high number of lacerations were seen in our study, including 5 in the clinical outcomes cohort and 3 in the short-term follow-up group.Patients who sustained a laceration were younger and included the 3 youngest patients in our cohort, at 10, 10, and 12 years old. The youngest patient with a confirmed acute Achilles tendon tear in our analyzed clinical outcomes cohort was 13 years of age. A high rate of lacerations (67%) was also reported in the series by Chen etal, of which 69% involved broken glass and 50% were complete lacerations. 7 A recent clinical series of 322 open Achilles tendon lacerations in Qatar was published by Alhammoud etal. 1 In their series, 98% were male, mean age was 32.1, and most common cause was slipping in the bathroom (82%). Treatment was with primary repair, and postoperative infection rate was 8.7%.
The current study also revealed 2 cases of failed initial nonoperative management, one of whom was a partial-thickness laceration in a 16-year-old hockey player. This patient continued to have marked symptoms of pain and weakness in the Achilles tendon 3 months after nonsurgical management, which was felt to be out of proportion to the symptoms expected for this postinjury time period, prompting a shift in the shared decision-making process toward delayed surgical repair. While a previous multicenter randomized controlled trial supported accelerated functional rehabilitation and nonoperative treatment for acute Achilles tendon ruptures in the adult population, it should be noted that no pediatric or adolescent patients were included in that report. 27
Spontaneous tears of the Achilles tendon have been rarely reported in the younger population. Our series included 3 patients under age 16 (aged 13, 14, and 15) with traumatic tears (including 1 basketball player and 1 cheerleader). In Chen etal’s 7 report, all acute tears occurred in skeletally mature patients, with the most common mechanism being basketball. Eidelman etal 10 described the case of a 7-year-old girl with an “acute rupture,” but which actually was a complete bony avulsion of the bony attachment of the Achilles tendon from the calcaneus that was treated successfully without surgery. Basketball was the most common sport involved in complete acute tears in our series and that of Chen etal, followed by gymnastics and soccer. Hagen and Pandya also reported on a case series of 3 teenage female basketball players who sustained complete ruptures that underwent surgical repair. 12 Another study reported a high rate of Achilles tendon rupture in women’s collegiate gymnastics, especially in elite athletes performing difficult floor and vault skills and competing in all 4 events. 5
Our surgical repairs utilized nonabsorbable sutures in all Achilles repair cases and we report 3 cases of delayed wound healing (13%). It should be noted that a recent 20-year study on Achilles repairs with a single-surgeon percutaneous and open technique showed a higher rate of wound complications associated with open repair and nonabsorbable suture use. 23 Following repair, a conservative rehabilitation protocol as described above was followed. Costa etal 8 have advocated for immediate weightbearing mobilization for both operatively and nonoperatively treated Achilles injury patients because of practical advantages based on randomized controlled trials in both groups. However, the operative trial had 2 reruptures in the early mobilization group, and no functional benefits (or complications such as rerupture or evidence of tendon lengthening) were seen in the conservative management trial.
Risk factors for Achilles tendon tears in children and adolescents are not well understood, but may include medical comorbidities, medication use including fluroquinolone drugs, and prior Achilles tendon surgery such as clubfoot casts or Achilles lengthening procedures. In our clinical follow-up cohort of 24 patients, 19 had tears that were not from laceration and therefore may be related to underlying risk factors. Of these 19 patients, we identified 2 of 19, 11% of acute who had potential risk factors, including 1 patient who had a history of clubfoot casting and Achilles tendon Z-lengthening as a child and one 13-year-old skeletally immature patient with osteogenesis imperfecta and Ehlers-Danlos Syndrome who sustained an acute tear. In the series by Chen etal, 7 they identified 4 of 8 patients in their tear subgroup with potential risk factors, including 1 patient who was taking minocycline for acne, 1 patient with a history of clubfoot surgery, and 2 patients with BMI >99th percentile. In the recent Ashebo etal 3 series, 4 patients had a history of clubfoot treated with Achilles tenotomy. Two other case reports have described Achilles tears in a 15-year-old and 16-year-old following Ponsetti treatment for clubfoot.2,9
Many adults who sustain Achilles rupture have underlying Achilles tendinopathy. The rate of chronic Achilles tendinopathy in children and adolescents is not well known, but likely significantly lower. Cassel etal 6 recently investigated the incidence of Achilles and patellar tendinopathy in 157 adolescent elite athletes and 25 nonathletic controls. Their prospective study utilized ultrasound for diagnosis and identified an incidence of Achilles tendinopathy in 1% and intratendinous alterations in 1% to 2% of elite athletes and 0% in controls. Previous histologic studies have also shown clear evidence of tendinopathy in biopsied Achilles tendons as compared with asymptomatic tendons. 17 It is notable in our younger athlete series that there was only 1 patient with preexisting Achilles disease diagnosed prior to surgery: a 22-year-old female hammer thrower with a Haglund deformity who had prior treatment including a platelet-rich plasma injection for insertional Achilles tendinopathy/partial tearing who went on to surgical intervention in the form of acute repair with suture anchor to the calcaneus and excision of the Haglund deformity.
Limitations
The greatest limitations of the current study include its retrospective design and relatively small sample size. A high rate of patients in the entire cohort did not meetminimum clinical follow-up criteria and thus their outcomes were not analyzed. Attempts to limit the inherent biases in retrospective studies included exclusion of those with short-term follow-up from the critical analyses of the study, as well as outreach to patients, which yielded a reasonable perspective of longer-term outcomes. Thereis potential for recall bias from a retrospective query of follow-up of RTS. There were no preoperative PROs to allow for quantification of improvement after surgery. However, the inclusion of more comprehensive follow-up data from the excluded group would have beenoptimal, but is consistently difficult for clinical studies of adolescents, given what a geographically mobile population they become in their postadolescent years. Other limitations included the absence of standardized surgical techniques (including the exclusive use of an open instead of percutaneous surgical technique) and rehabilitation protocols, because of the involvement of multiple different surgeons at 2 high-volume pediatric referral centers.
Conclusion
The current case series describes 38 Achilles injuries in a pediatric population with previously minimal evidence regarding treatment outcomes. These data highlight a relatively high rate (21%) of lacerations, particularly in the youngest subpopulation, and excellent PROs, low rates of rerupture (4%), and consistent time to RTS (5-7 months) following surgical management in this population. The study also highlights a notable rate of wound complications in this cohort of Achilles injuries that underwent repair through a traditional open incision as well as cases of failed nonsurgical management and the importance of early diagnosis in this population. Further prospective and comparative research is necessary to clarify the role of nonoperative management and optimize rehabilitation protocols in this young athletic population.
Footnotes
Final revision submitted December 10, 2025; accepted December 13, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.E.K. has received consulting fees from DePuy and Miach Orthopedics and support for education from Kairos Surgical. J.J.B. has received consulting fees from OrthoPediatrics. Y-M.Y. has received consulting fees from Smith & Nephew. B.E.H. has received consulting fees from and owns stock in Imagen Technologies; has received speaking fees from Arthrex and Kairos Surgical; and has received royalties from Springer Science & Business Media and support for education from Pylant Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Boston Children’s Hospital (No. P00018287).