
Abstract
Background:
The absence of a comprehensive classification system for Achilles tendon (AT) injuries contributes to the lack of consensus regarding optimal treatment strategies, as it hinders accurate differentiation of injury types.
Purpose:
To evaluate epidemiology of AT ruptures to develop a magnetic resonance imaging–based classification system for rupture location.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A search was conducted for all patients with acute AT injuries between 2016 and 2023. Tear locations were classified as follows: type 1 (musculotendinous junction; MTJ), type 1A (2-cm zone distal to MTJ), type 2 (midsubstance), type 3 (2-cm zone proximal to insertion), type 3A (soft tissue “peel-off”), type 3B (calcaneal bony avulsion). Clinicodemographic data were collected, and rupture gap size, tendon thickness, tibiotalar, and plantarflexion angle were measured.
Results:
A total of 428 patients were included (age 45 ± 15 years; 17% female). Mean rupture gap size was 30 ± 16 mm in 73°± 8° tibiotalar flexion. AT tear distribution: type 1, 62.7%; type 1A, 16.3%; type 2, 13.8%; type 3, 0.7%; type 3A, 5.8%; and type 3B, 0.7%. Female patients demonstrated lower tendon thickness (P < .001) and a significantly higher prevalence of type 3, 3A, and 3B (P < .001). Multivariate analysis revealed that proximal AT tears were associated with presence of tendinopathy (odds ratio [OR], 2.19; 95% CI, 1.24-3.83), while younger age and larger gap size were significant but with a weak effect size. Midsubstance tears were predicted by older age and increased tendon thickness (OR, 1.02-1.17). Distal tears were associated with absence of tendinopathy (OR, 0.17; 95% CI, 0.07-0.39), while age only had a small effect. Tear location measurements demonstrated substantial to almost perfect interobserver (3 observers; n = 35; Cohen's kappa = 0.93; 95% CI, 0.74-0.99) and intraobserver (1 observer; n = 35; Cohen's kappa = 0.93; 95% CI, 0.86-0.99) reliability.
Conclusion:
This study introduces an AT tear classification system that demonstrated substantial to almost perfect reliability. AT ruptures at the MTJ were most common (63%). Presence of tendinopathy, age, gap size, and tendon thickness were significant predictors for AT tear type. Female patients exhibited lower tendon thickness and a significantly higher prevalence of distal tear location. Studies with larger cohort sizes are necessary to confirm the current findings.
Achilles tendon (AT) rupture is a common injury, with an incidence ranging from 2 to 50 cases per 100,000 persons per year.20,22,34 Despite numerous clinical studies, the literature lacks a clear consensus on the optimal treatment for acute AT injury, including use of nonoperative or surgical methods. 27 While indication for surgical treatment is multifactorial, a comprehensive classification to differentiate injuries and compare outcomes is necessary.
Published studies commonly use only a broad classification dividing the AT into the musculotendinous junction (MTJ), midsubstance, and distal regions.6,7,14 Introduction of more differentiated tear location classification systems for other tendon and ligament injuries has led to significant shifts that have challenged previously established treatment algorithms.26,33,37,38 Previous studies have reported the most common rupture location (>80%) to be within the midsubstance between 2 and 6 cm proximal to the calcaneal insertion, although some studies suggest more proximal or distal rupture sites are more common.2,6,24,28 Surgical outcomes have been found to depend on tear location, potentially due to decreased vascularity in the midsubstance region of the tendon.7,8,18 Despite this, a reliable and more specific magnetic resonance imaging (MRI)–based tear location classification system for rupture location has not yet been described.
The study aim was to evaluate the epidemiology of AT rupture patterns to develop an MRI-based classification system for rupture location. The hypothesis was that tear location is associated with patient age and sex, but not with tendon thickness, gap size, and tendinopathy.
Methods
Patient Selection and Study Setting
This retrospective, cross-sectional study received institutional board approval prior to initiation. The study was performed according to the ethical standards in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Using an institutional electronic health record (EHR) system (Epic), a comprehensive search was conducted to identify patients who presented with complete AT tears, defined by full-thickness discontinuity of tendon fibers on MRI, between January 1, 2016, and August 1, 2023, at the study center. The electronic search employed using International Classification of Diseases, 10th Revision (ICD-10), codes for the following search terms and combinations: S86.012A and S86.011A (acute injury), and M66.361 and M66.362 (spontaneous rupture). This search resulted in a total of 552 MRI studies at a single institution (Figure 1). Screening failures were excluded for final analysis and comprised MRIs demonstrating no complete AT rupture (partial AT tears, longitudinal splint-type tears, isolated intratendinous signal abnormality without discontinuity; n = 77), status postsurgery (n = 26), or patient cases with no available MRI (n = 22). All available and eligible MRIs were assessed for tear location analysis.

Study flowchart. “No complete rupture” includes partial Achilles tendon tears, longitudinal splint-type tears, and isolated intratendinous signal abnormality without discontinuity. MRI, magnetic resonance imaging.
AT Tear Location
The AT rupture classification system was adapted from existing systems but significantly expanded to capture the full spectrum of AT injury patterns.2,12,28 Tear location was defined according to the most proximal extent of the tear, based on the hypothesis that tear proximity may influence treatment outcomes. Tear locations were classified based on AT remnant length as follows (Figure 2): type 1 (at or above the border of the MTJ), type 1A (2-cm zone distal to the MTJ), type 2 (midsubstance), type 3 (2-cm zone proximal to insertion), type 3A (soft tissue “peel-off”), type 3B (calcaneal bony avulsion). These subclassifications were introduced to provide a more granular and standardized anatomical description and to improve reproducibility. A 2-cm transition zone was defined, as surgical technique in this region is influenced by the proximity of the MTJ or the calcaneal bone, while bony avulsions require a different surgical treatment. 29

Sagittal plane magnetic resonance imaging using an intermediate echo time sequence demonstrates the proposed Achilles tendon tear location classification. MTJ, musculotendinous junction.
Additionally, proximal and distal AT remnant length (proximal: distance from MTJ; distal: distance from calcaneal insertion), rupture gap size (in mm), presence of tendinopathy (yes/no), tibiotalar and plantarflexion angle (in angular degree), and tendon thickness (in mm) of an unaffected area of the tendon distal to the rupture (or proximal in the case of type 3, 3A, and 3B) were measured. AT tendinopathy was defined as tendon thickening of the remnant with increased intratendinous signal intensity and loss of normal fibrillar architecture, while preserved fiber continuity and without a discrete fluid-filled defect or tendon discontinuity.32,36
Reliability Analysis
A senior musculoskeletal radiologist from the study institution supervised and validated the MRI measurement procedure. Before study initiation, the measurement technique to determine the tear location was elucidated to all observers. Then, tear locations of 35 MRIs were independently evaluated by 3 observers (M.M.M., A.E., and R.E.B.). All evaluators were unaware of the results of the radiology reports and their peers' assessments during the process. For intraobserver reliability analysis, 8 weeks after the initial assessment, 1 observer (M.M.M.) repeated the measurements blinded to the first evaluation in random sample order.
The required sample size for the reliability analysis was estimated according to the guidelines by Bujang and Baharum. 5 The study aimed to detect an expected kappa of 0.90 with a minimally acceptable value of 0.60 (α = .05; power = 0.80). For a 6-category ordinal scale, the tabulated minimal sample sizes for adjacent kappa values of 0.6 versus 0.9 are between 34 and 37 under the assumption of nonproportional category frequencies. Therefore, a selection of 35 MRIs was used for reliability analysis.
Last, demographic data were gathered for each patient including age, sex, and body mass index.
Statistical Analysis
Normality of distribution of the samples was tested with Shapiro-Wilk test. Normally distributed data were expressed as means with standard deviation when appropriate. Two-way analysis of variance for nominal scaled data and Pearson chi-square or Fisher exact test for ordinal data was used (P≤ .05) to test for between-group differences in outcome measures (univariate analysis). In sex-stratified analysis, continuous variables were compared using independent-samples t tests, while categorical variables were analyzed using chi-square or Fisher exact tests, as appropriate. To determine the interobserver reliability, Cohen kappa was calculated. The range of Cohen kappa was −1 to 1 and was rated according to the criteria of Landis and Koch. 19 Reliability was interpreted to be as the following: >0.80 = almost perfect; 0.61 to 0.80 = substantial; 0.41 to 0.60 = moderate; 0.21 to 0.40 = fair; and 0.00 to 0.20 = slight. Multivariate analysis using logistic regression was performed to evaluate the influence of patient sex, age, gap, and tendon thickness, as well as presence of tendinopathy as predictors of AT tear types. Additionally, the influence of those variables on tendon thickness and extent of rupture gap were evaluated. Statistical analyses were performed with BlueSky Statistics (Version 10.3.4, BlueSky Statistics; Version 8.95, R Package).
Results
Baseline Demographics and Reliability Analysis
A total of 429 patients (mean age, 45 ± 15 years; 17% female) were included. The total AT length was 75 ± 21 mm (length of proximal + distal AT remnant). Mean rupture gap size was 30 ± 16 mm in 73°± 8° tibiotalar flexion (5°± 9° plantarflexion). Tendinopathy was present in 327 (76.9%) cases.
Statistical analysis showed substantial to almost perfect interobserver and intraobserver reliability of tear type measurements. Cohen's kappa for interobserver was 0.93 (95% CI, 0.74-0.99), and intraobserver reliability was 0.93 (95% CI, 0.86-0.99).
AT Tear Type: Study Participant Characteristics
Mean tear location was 65 ± 26 mm proximal to the calcaneal insertion and 10 ± 18 mm distal from the MTJ (Table 1). AT tear distribution was type 1, 62.7%; type 1A, 16.3%; type 2, 13.8%; type 3, 0.7%; type 3A, 5.8%; and type 3B, 0.7%. Univariate analysis of tear locations demonstrated that sex, age, presence of tendinopathy, tendon thickness, and rupture gap differed significantly between tear types.
Tear Location and Study Participant Characteristics (N = 429) a

Data are presented as mean ± SD or n (%). Bold values denote statistical significance at P≤ .05. MTJ, musculotendinous junction; NA, not available.
Sex-stratified analysis revealed significant differences between men and women (Table 2). Female patients demonstrated significantly lower tendon thickness than male patients (10 ± 2 mm vs 11 ± 2 mm, respectively; P < .001) and a significantly more distal tear location (distance from distal insertion: 52 ± 29 mm vs 68 ± 24 mm, respectively; P < .001). Particularly, women were found to have a higher proportion of type 3A tears than men (15.1% vs 3.9%, respectively), while men demonstrated more type 1 tears than women (64.3% vs 54.8%, respectively).
Study Participant Characteristics by Sex a
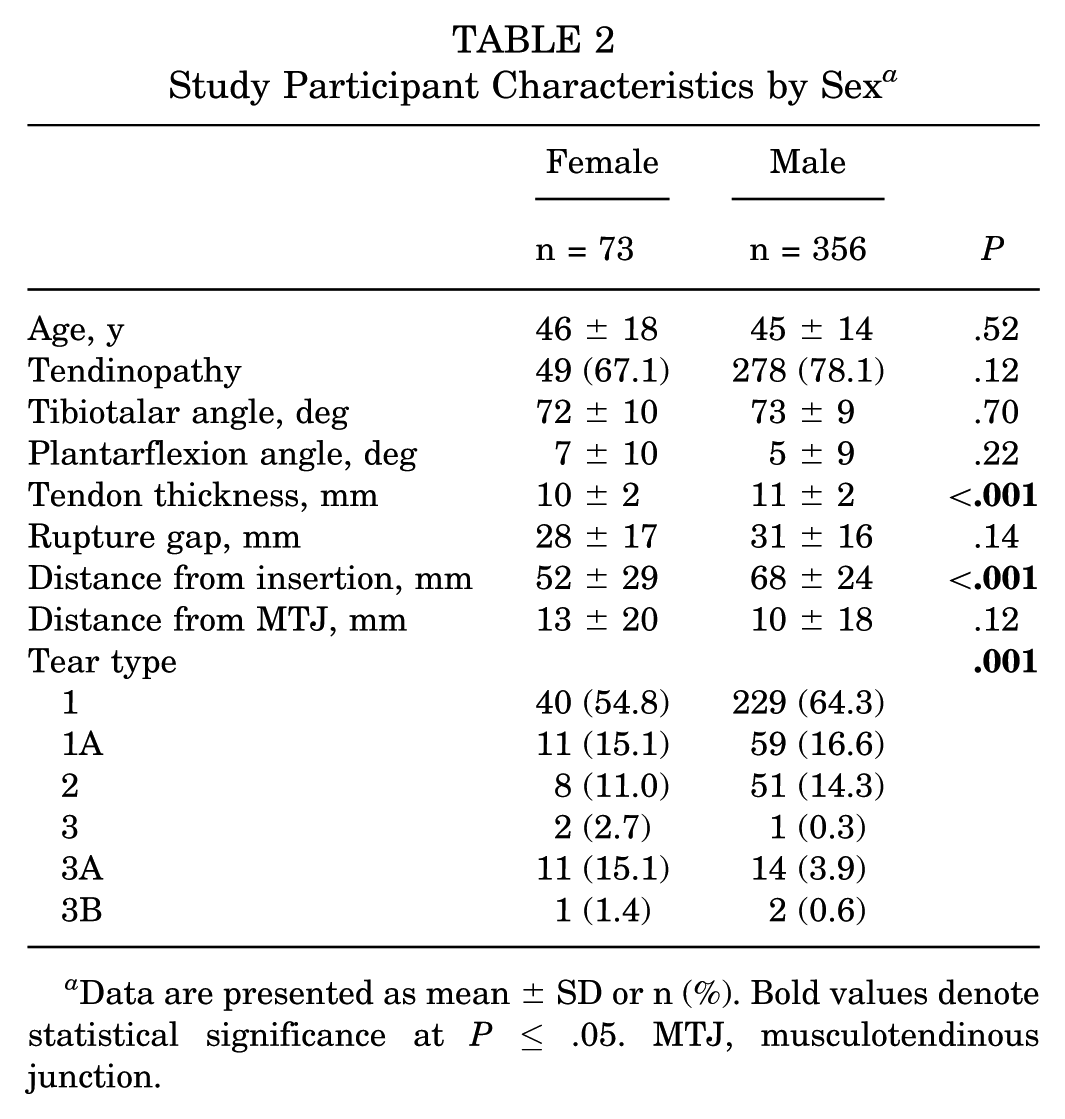
Data are presented as mean ± SD or n (%). Bold values denote statistical significance at P≤ .05. MTJ, musculotendinous junction.
Multivariate Analysis
Three separate multivariate logistic regression models were performed to identify predictors of AT tear location (proximal: 1 and 1A; midsubstance: 2; distal: 3, 3A, and 3B). For proximal tears, younger age (odds ratio [OR], 0.97 per year; 95% CI, 0.95-0.98; P < .001), larger gap size (OR, 1.03 per mm; 95% CI, 1.01-1.04; P = .005), and the presence of tendinopathy (OR, 2.19; 95% CI, 1.24-3.83; P = .006) were independently associated with a proximal tear location (McFadden pseudo-R2 = 0.106). For midsubstance tears, older age (OR, 1.02 per year; 95% CI, 1.00-1.04; P = .04) and increased tendon thickness (OR, 1.17 per mm; 95% CI, 1.01-1.35; P = .03) were independently associated with tear location (McFadden pseudo-R2 = 0.042). For distal tears, older age (OR, 1.05 per year; 95% CI, 1.02-1.08; P < .001) and absence of tendinopathy (OR, 0.17; 95% CI, 0.07-0.39; P < .001) were independently associated with distal tear location (McFadden pseudo-R2 = 0.239) (Table 3).
Multivariate Logistic Regression for Predictors of Achilles Tendon Tear Types a

Bold values denote statistical significance at P≤ .05.
Discussion
The key findings of this study were the introduction and reliability analysis of a new MRI-based AT tear location classification. AT tear location was influenced by patient-specific factors. Female patients exhibited lower tendon thickness and a significantly higher prevalence of distal AT tear locations. Finally, proximal tears were associated with presence of tendinopathy, younger age, and larger gap size, midsubstance tears with older age and greater tendon thickness, and distal tears with older age and absence of tendinopathy. These findings highlight the importance of considering demographic and anatomical characteristics in diagnostic and treatment algorithms, while overall the effect sizes of these factors were small. Rather than directly informing treatment selection, this classification provides a standardized, reliable anatomical framework that may facilitate future studies evaluating treatment strategies and outcomes across specific rupture locations.
These findings are clinically relevant, as understanding the prevalence of different AT tear types may support the development of more differentiated, injury-specific treatment strategies, which have been shown to significantly influence surgical outcomes.7,8,15,17 Particularly, the decision between nonoperative and surgical treatment of AT injury may benefit from a reproducible characterization of tear location, thereby enabling a more granular and standardized knowledge of tear locations to predict outcome. While surgical restoration of mechanical integrity in the MTJ region may be technically more challenging, 18 studies report hypovascularization in the midsubstance of the AT,7,8,24 which may hinder sufficient tendon healing following repair or nonoperative treatment. Studies have found persistent decreased biomechanic properties following surgical repair, particularly after injury of the midsubstance AT.10,11 Therefore, more exact classification may guide future translational research efforts and comparison of outcomes, while studies with larger cohort sizes are necessary to confirm the current findings.
The majority of AT tears (79.0%) were proximal (type 1 and 1A), whereas midsubstance (type 2) and distal tears (type 3, 3A, and 3B) were less common. Prior studies evaluated AT tear locations using varying classification systems. Bäcker et al 2 found 44% proximal, 42% middle third, and 13% distal third AT tears. In contrast, Giordano et al 14 reported 3.9% proximal AT ruptures, 82.9% midsubstance, and 12.2% distal insertional tears. Their use of different methodologies, particularly postoperative MRI or operative notes, may have led to a lower detection rate of proximal tears compared with the present study. Giordano et al defined midsubstance tears by the distance (2-6 cm) from the calcaneal insertion, while distal insertional tears included distal tears within 2 cm from the insertion site. Myotendinous tears were not further differentiated. As demonstrated in the current study, AT dimensions vary significantly between individuals (75 ± 21 mm), arguing against use of a general metric (2-6 cm) to define the midsubstance region. Barrios-Cárdenas and Lazo-Vera 3 found only 66% midsubstance tears (2-5 cm). Geng et al 12 reported intraoperatively measured length of the distal remnant of 4.07 ± 1.57 cm. Surprisingly, the current cohort found a more proximal mean tear location, 6.5 ± 2.6 cm distant from the insertion. This is also reflected by the high number (79%) of proximal (1 and 1A) tears, located in the zone of the MTJ.
Several risk factors have been reported to influence AT rupture and outcomes following treatment. As expected, female patients tend to have lower tendon thickness, which may not have significant clinical impact 13 ; however, differences in the distribution of tear locations may carry important implications for the treatment algorithm of AT injuries. In this regard, studies found higher degree of deficit and inferior self-reported outcomes in female patients following surgical treatment of AT ruptures.21,35 Bäcker et al 2 reported a higher proportion of female patients with injuries in the distal third of the AT. The higher proportion of distal peel-off injuries suggests a favorable potential for surgical management through direct tendon-to-bone repair, for which several reinsertion techniques are available.4,9,16,23,31,40 The present study confirms prior studies reporting age and male sex to be risk factors for AT rupture. 1 The current findings suggest more proximal tear locations are associated with larger gap sizes, which may indicate that injuries in the MTJ zone lead to greater retraction of the tendon remnants. This is clinically relevant, as some studies evaluating nonoperative treatment have shown that gap size >5 mm predict lower patient-reported outcomes, 41 while other studies show contradicting results.25,30 Presence of AT tendinopathy has been identified as a risk factor for AT rupture. 39 The findings of the current study expand this, as it was observed that tendinopathy influences tear location. The relatively small ORs observed in multivariable analyses likely reflect per-unit effect estimates and adjustment for shared variance among predictors. Importantly, even modest ORs may translate into clinically meaningful effects across the observed range of the predictor.
Limitations
This study has limitations. First, tear location assessments were not validated against another diagnostic modality, such as intraoperative findings. Second, the markedly unequal distribution of tear types, together with the small sample size of certain subcohorts, limits the robustness of between-group comparisons and the ability to draw definitive conclusions. Third, tear type classification was not correlated with clinical and functional outcomes or histopathological findings. Clinical outcome correlation is an important next step, and the present findings should be interpreted as hypothesis generating rather than outcome defining. Fourth, it should be noted that the injury itself affects the MRI appearance of AT tissue, thereby potentially limiting the accuracy of tendinopathy assessment. Fifth, an EHR-based search may not have captured all patients presenting with AT injuries if ICD-10 codes were inconsistently applied, as patients lacking AT-specific ICD-10 codes could not be identified.
Conclusion
This study introduces an AT tear classification system that demonstrated substantial to almost perfect reliability. AT ruptures at the MTJ were most common (63%). Presence of tendinopathy, age, gap size, and tendon thickness were significant predictors for AT tear type. Female patients exhibited lower tendon thickness and a significantly higher prevalence of distal tear locations. Studies with larger cohort sizes are necessary to confirm the current findings.
Footnotes
Final revision submitted January 10, 2026; accepted January 14, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: W.M.R. receives support from AO North America and the Center for Orthopaedic Trauma Advancement; receives royalties from Smith & Nephew, Wolters Kluwer, MicroPort, and OsteoCentric Technologies; consulting fees from Smith & Nephew; and ownership interest in Cable Fix LLC, Crooked Foot Medical LLC, McGinley Orthopaedic Innovations LLC, Primo MC LLC, and HS2. He is also a board member of the Orthopaedic Trauma Association, the Journal of Orthopaedic Trauma, and the Hospital for Special Surgery. G.S.D. receives royalties, owns stock in, and is a paid consultant for Zimmer Biomet; receives royalties from Arthrex; has received stock options and provides consulting services for and participates in funded research with Miach Orthopaedics; and receives stock options and provides consulting services for OSSIO Inc. S.B.B. reports stock from restor3d inc, Vitalis Inc, Pressio Spine, and Turner Imaging Systems Inc; and reports professional activities with Panther Orthopedics Inc, Medline Industries Inc, Andiem, Gramercy Extremity Orthopedics LLC, Celling Biosciences, Johnson & Johnson/Depuy Orthopedic, and American Orthopaedic Foot & Ankle Society (program committee member). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the institutional review board of Hospital for Special Surgery (No. 2022-2367).