
Abstract
Background:
The anterior intermeniscal ligament (AIML) footprint and dimensions in skeletally immature knees have not been well documented. The AIML may play an important role in tibial spine fracture (TSF) reduction and meniscal repair/stability. The AIML is vulnerable to injuries during drill hole placement in anterior cruciate ligament (ACL) reconstruction. Therefore, it is necessary to characterize the anatomy of the AIML in skeletally immature knees to prevent iatrogenic injuries.
Purpose:
To evaluate AIML dimensions, its meniscal attachment patterns, and its relationship to the ACL.
Study Design:
Descriptive laboratory study.
Methods:
A total of 12 fresh-frozen cadaveric knees, 6 male and 6 female, were dissected (mean age, 9.8 years [range, 9-11 years]). The distal aspect of the quadriceps tendon was transected, and the joint capsule was opened. The infrapatellar fat pad was dissected and the AIML identified. Photographs were taken with an in-frame ruler, and the AIML length and distance to the anterior aspect of the ACL were measured. The AIML insertion type was determined according to the classification system reported by Nelson and LaPrade.
Results:
The mean length of the AIML was 23.6 mm (range, 19.8-31.9 mm). In 11 specimens, the mean distance between the AIML and the most anterior aspect of the ACL was 3.7 mm (range, 2.5-4.6 mm). In the remaining knee, the footprint of the anterior root of the medial meniscus, ACL, and AIML were nearly indistinguishable. The AIML was found with a type I insertion in 7 cases and a type II insertion in 5 cases.
Conclusion:
This study demonstrated the smaller dimensions of the AIML in skeletally immature patients and its relationship to key adjacent structures compared with previously reported adult data. These anatomic relationships highlight the AIML's vulnerability during ACL reconstruction, TSF reduction, and meniscal repair. Although the biomechanical consequences of the AIML remain unclear, we recommend avoiding injuries to this structure during procedures that may place it at risk.
Clinical Relevance:
This study characterized the anatomy of the AIML in pediatric knees, highlighting its consistent presence, smaller dimensions, and proximity to critical structures. Understanding the AIML's anatomy will help to minimize iatrogenic injuries during surgery, particularly in ACL reconstruction, TSF reduction, and meniscal repair.
The anterior intermeniscal ligament (AIML) is an often-overlooked anatomic structure of the knee that may play an important role in meniscal stability and overall joint biomechanics.8,10,20,22,25,27 Although the AIML is present in most knees,4,15,21 its function and anatomic footprint remain incompletely understood, particularly in skeletally immature patients. Prior research suggests that the AIML represents the most anterior part of the “meniscal belt” and potentially contributes to the transmission of circumferential hoop stresses in the knee, which may influence the load distribution across the knee joint.8,18,20,22,25 Studies have demonstrated that transection or injuries to the AIML can lead to increased meniscal extrusion, increasing femorotibial contact pressure, and altered knee biomechanics, which may accelerate the development of osteoarthritis and impair joint function.20,22 Others have found that the AIML contains neural mechanoreceptors, which may contribute to structural and proprioceptive function of the knee.2,7,35 These biomechanical consequences underscore the clinical relevance of the AIML, especially in pediatric populations in which the proximity of the AIML to nearby structures raises concerns during surgical procedures and injuries.
In pediatric tibial spine fractures (TSFs), meniscal tissue and the AIML may cause interposition or entrapment, leading to malreduction and poor outcomes.1,13,19,28,29,33 Similarly, repair of meniscal tears and meniscal transplantation may be affected by the AIML, as it sometimes serves as the primary attachment site for the anterior horn of the medial meniscus.9,10,12,21,23 Furthermore, the close anatomic relationship between the anterior cruciate ligament (ACL) tibial footprint and AIML, sometimes used as a landmark for tibial tunnel placement,6,16,26 raises concerns for iatrogenic injuries during ACL reconstruction. 14 Failure to recognize and preserve the AIML during such procedures may inadvertently compromise meniscal stability and native knee biomechanics. Despite these considerations, detailed anatomic data surrounding the AIML in the skeletally immature knee remain limited.
The purpose of this study was to provide an anatomic analysis of the AIML in pediatric cadaveric specimens, focusing on its dimensions, insertion patterns, and spatial relationship with the ACL. Awareness of the AIML's footprint in the skeletally immature knee may help surgeons to minimize the risk of iatrogenic injuries, improve surgical outcomes, and preserve knee stability in the growing population.
Methods
An institutional review board deemed that approval was not necessary for this study, as it was based on cadaveric tissue and did not include patient identifiers, the use of genetic information, or contact with the patient's family per guidelines of the United States Department of Health and Human Services (www.hhs.gov). A tissue harvesting facility (AlloSource) sourced cadaveric tissue with family consent, allowing tissue use for research purposes before conducting this study.
A total of 12 fresh-frozen pediatric cadaveric knees with a mean age of 9.8 years (range, 9-11 years; 6 male and 6 female specimens) were utilized (Table 1). Specimens were stored at −20°C and thawed at room temperature for 24 hours before dissection. All dissections were performed in a systematic fashion, and data were recorded on a standardized collection sheet. Dissections and measurements were performed under the supervision of a fellowship-trained pediatric orthopaedic sports surgeon.
Specimen Characteristics

The distal aspect of the quadriceps tendon was first transected to expose the proximal femoral condyles. The joint capsule was then carefully opened proximally, medially, and laterally to allow for visualization of the intra-articular structures. The infrapatellar fat pad was dissected to expose the AIML. Each knee was flexed to 90° to facilitate clear visualization of the tibial plateau and associated structures. The presence or absence of the AIML was noted, and when present, its insertion pattern was documented and classified based on the criteria described by Nelson and LaPrade. 21
The AIML exhibits 3 distinct insertion patterns (Figure 1). 21 Type I attaches directly to the anterior horn of the medial meniscus and the anterior margin of the lateral meniscus. Type II attaches to the anterior margin of the medial meniscus and the joint capsule anterior to the lateral meniscus. Type III lacks direct attachments to either meniscus, instead anchoring solely to the anterior capsule on both the medial and lateral sides. This classification system was used for this study.

The 3 types of insertion patterns of the anterior intermeniscal ligament (AIML).
Measurements were obtained with ImageJ (National Institutes of Health) using high-resolution digital photographs taken with an in-frame ruler for calibration. 30 The length of the AIML was measured from its medial attachment to its lateral attachment. The shortest distance from the AIML to the most anterior aspect of the ACL tibial footprint was also recorded.
The relationships between age, AIML-to-ACL distance, and AIML length were analyzed using the Spearman correlation coefficient, while differences in the AIML-to-ACL distance between insertion types and sexes were analyzed using the Mann-Whitney test. Analyses were completed using RStudio (Posit) with a 2-sided level of significance of .05.
Results
A distinct AIML was identified, either within or obscured by the retropatellar fat pad, in all 12 specimens (100%). The mean length of the AIML was 23.6 mm (range, 19.8-31.9 mm). In 11 specimens (92%), the mean distance between the AIML and the most anterior aspect of the ACL was 3.7 mm (range, 2.5-4.6 mm) (Table 2 and Figure 2). The AIML-to-ACL distance was significantly associated with age (rs = 0.65 [95% CI, 0.08-0.90]; P = .030). The shortest distance between the AIML and ACL tibial footprint was consistently observed to be at the medial third of the AIML. In the remaining knee, the footprint of the anterior aspect of the medial meniscus, ACL, and AIML were closely approximated, and the AIML-to-ACL distance could not be measured. The AIML was found with a type I insertion in 7 cases (58%) and a type II insertion in 5 cases (42%) (Figure 3). Notably, no type III insertions were observed in this cohort (0%). The AIML-to-ACL distance was not significantly associated with AIML length, insertion type, or sex (P > .05).
Anatomic Characteristics a
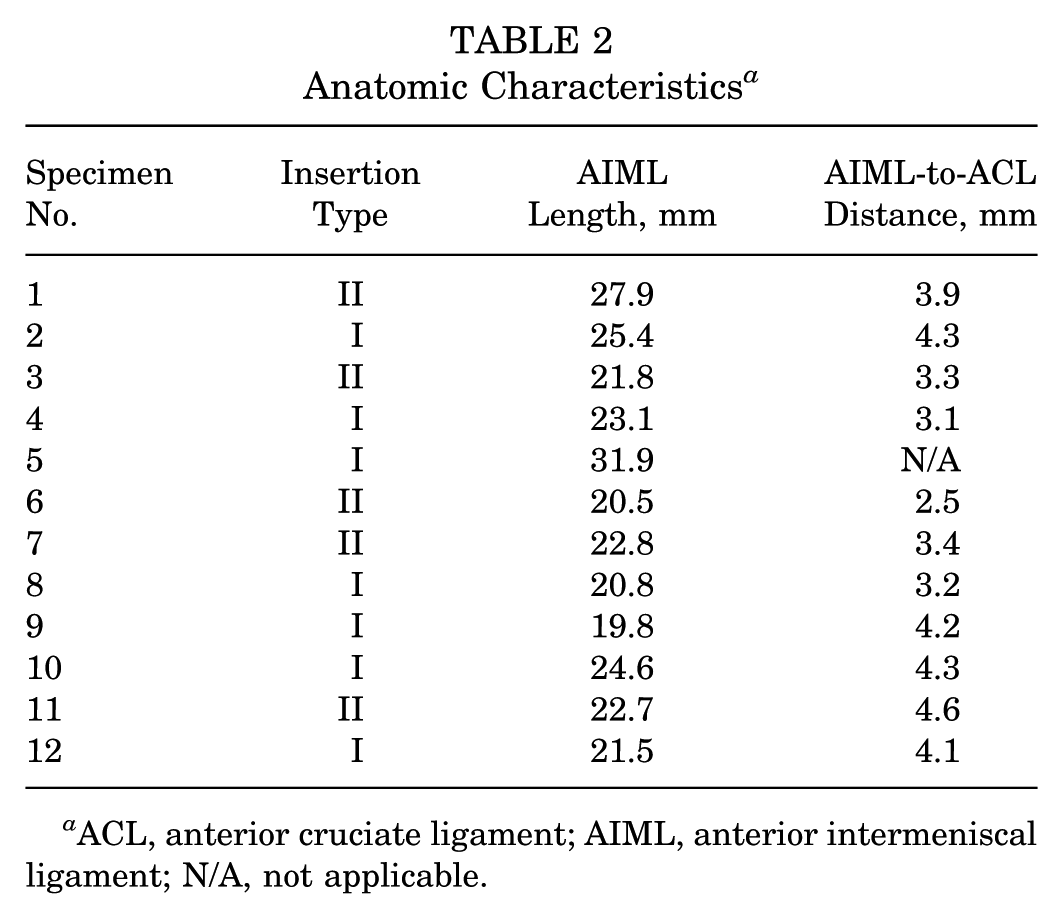
ACL, anterior cruciate ligament; AIML, anterior intermeniscal ligament; N/A, not applicable.
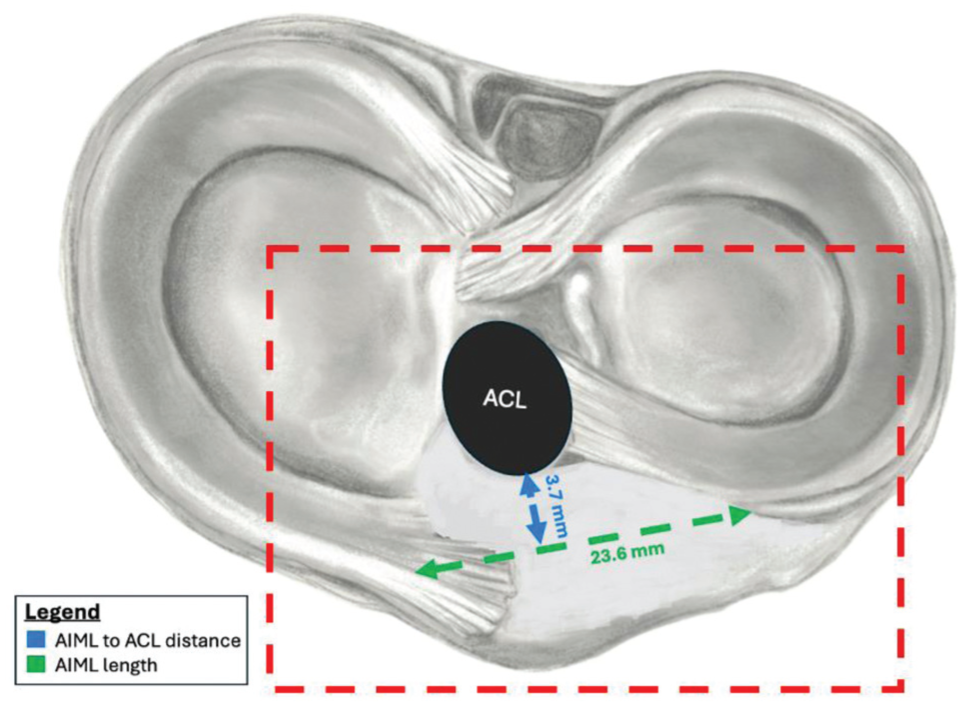
Anterior intermeniscal ligament (AIML) length and distance to the anterior cruciate ligament (ACL) footprint in skeletally immature knees.

Photographs with (A) type III, (B) type II, and (C) type I insertions of the anterior intermeniscal ligament (AIML) in fresh-frozen skeletally immature cadaveric specimens. Note how the AIML usually connects the leading edge of the anterior horn of the medial meniscus to the external portion of the anterior horn of the lateral meniscus. Also note the relationship of the AIML to the anterior aspect of the insertion of the anterior cruciate ligament (ACL) and the potential for AIML entrapment in tibial eminence avulsion fractures in children.
Discussion
This is the first anatomic study of the AIML in skeletally immature cadaveric specimens, demonstrating its consistent presence in all specimens examined, smaller dimensions, and closer proximity to the ACL compared to prior adult data. Given the AIML's clinical relevance to injuries such as displaced TSFs, the risk of iatrogenic injuries during intra-articular knee surgery including ACL reconstruction, and its importance in native knee biomechanics, this improved anatomic understanding will contribute to optimizing the management of pediatric knee abnormalities.
We identified the AIML in 100% of specimens (12/12), comparable to the prevalence reported by Nelson and LaPrade 21 (94.0%) and Marcheix et al 15 (90.0%) and markedly higher than the Ghanaian (34.3%), Kenyan (62.3%), and Turkish (58.8%) cohorts reported by Brown et al, 3 Ouko et al, 23 and Ozcanli et al, 24 respectively. The mean AIML length in our pediatric cohort was 23.6 mm, shorter than the adult mean values reported by Nelson and LaPrade 21 (33.0 mm), Marcheix et al 15 (31.2 mm), and Tubbs et al 34 (35.4 mm), suggesting growth-related increases in ligament dimensions. The AIML-to-ACL distance in our study was 3.7 mm, notably closer than that of Nelson and LaPrade 21 (7.8 mm) and Marcheix et al 15 (12.0 mm) but comparable to that of Tubbs et al 34 (2.5 mm), indicating potential age-related spatial changes. Insertion patterns in this cohort were composed of type I (58%) and type II (42%) configurations, with no type III insertions observed. This aligns with Nelson and LaPrade’s 21 findings (type I: 46%; type II: 26%; type III: 12%) and Marcheix et al’s 15 results (type I: 66.7%; type II: 33.3%). Although the Nelson and LaPrade 21 classification system was applicable to our pediatric cohort, future studies with larger numbers of skeletally immature specimens may help to determine whether refinements to this system are warranted for children.
Previous research has highlighted the importance of the AIML as a component of the “meniscal belt,” where it acts as an anterior stabilizer that anchors the anterior horns of the medial and lateral menisci, preventing excessive translation, facilitating hoop stress transmission, and distributing tibiofemoral contact forces. In a study of adult specimens by Ollivier et al, 22 sectioning of the AIML led to increased tibiofemoral contact pressure, a decreased tibiofemoral contact area, and a more centralized force center of application. These findings could be explained by induced meniscal extrusion and how loss of the AIML leads to a reduction in the meniscus's ability to effectively distribute loads. In a similar study, Muhle et al 20 reported increasing anterior-posterior excursion of the anterior horn of the medial meniscus after AIML sectioning. Similarly, Paci et al 25 reported increased peak contact pressure in the medial compartment of the knee after transection of the AIML. In a study of 6 adult specimens, Poh et al 27 found a nonstatistically significant variation in global contact pressure and contact area after AIML resection in both medial and lateral knee compartments. While their findings did not reach statistical significance, this may have been influenced by a limited sample size. Although no prior studies have investigated tibiofemoral contact pressure changes in pediatric specimens after an AIML injury, surgeons should strive to preserve this structure to reduce any risk of long-term alterations in tibiofemoral forces within the knee.
The AIML is also an important consideration during the management of displaced TSFs in the skeletally immature.28,32,33 Entrapment of the AIML and/or meniscal horns, particularly in Meyers and McKeever type 2 (posteriorly hinged) and type 3 (completely displaced) fractures, represents a significant block to anatomic reduction with either nonoperative or operative treatment.1,11,29 In a study by Quinlan et al, 28 the AIML with or without meniscal incarceration prevented fracture reduction in 67% of TSF cases. Kocher et al 13 found that 54% of pediatric patients with TSFs undergoing arthroscopic fixation had an incarcerated anterior horn of the medial or lateral meniscus or AIML. Similarly, Hunter and Willis 11 reported AIML interposition in 59% of patients with TSFs treated with arthroscopic fixation, often causing incomplete reduction and requiring retraction and resection. In 2015, Edmonds et al 5 found meniscal or AIML entrapment in 32% of pediatric patients presenting with a TSF. While recent work suggests that malreduction may not consistently lead to functional deficits, 17 inadequate reduction of TSFs can, in some cases, result in persistent pain, restricted range of motion, and the need for surgery. 1 Therefore, awareness of the AIML, its typical type I or II insertion pattern, and its proximity to the ACL footprint/tibial eminence in the skeletally immature is crucial for ensuring successful fracture reduction and minimizing the risk of long-term complications.
The results of this study also highlight the AIML's close proximity to the ACL tibial footprint in pediatric knees. In one case, the AIML footprint was nearly confluent with the footprints of the anterior horn of the medial meniscus and ACL, indicating a high risk of iatrogenic injuries during tibial tunnel placement in ACL reconstruction. This risk is even greater in all-epiphyseal ACL reconstruction, as the drill hole starts above the physis and creates a larger elliptical hole with a more anterior position. 31 Although rigid nail fixation of tibial fractures in skeletally immature patients is uncommon, this study also demonstrated how the AIML may be at risk during drilling and reaming of the nail entry site on the anterior edge of the tibial plateau. In this location, the AIML represents the rear boundary of the nail entry site or “safety zone.” 7
This study has its limitations. First, access to pediatric cadaveric tissue is limited, and the small sample size restricts generalizability, statistical power, and conclusions about the AIML footprint in the skeletally immature. Second, while ImageJ was used for digital analysis, minor variations in specimen positioning, dissection technique, and calibration could introduce measurement inaccuracies, particularly for small structures such as the AIML. Despite these limitations, we believe that these findings can help surgeons to preserve and restore native AIML anatomy during open and arthroscopic procedures in children.
Conclusion
To our knowledge, this is the first anatomic study of the AIML in skeletally immature cadaveric specimens, highlighting its consistent presence, smaller dimensions, and close proximity to key knee structures. Given its location less than 4 mm from the ACL attachment on the tibia, the AIML is at a high risk of injuries during tibial tunnel drilling in ACL reconstruction, particularly in pediatric patients and those with all-epiphyseal tibial drill holes. Understanding the anatomy of the AIML in the growing knee may also help to minimize iatrogenic injuries and optimize outcomes for pediatric patients with anterior meniscus root tears and TSFs. Although the biomechanical consequences of the AIML remain unclear, we recommend avoiding injuries to this structure during procedures that may place it at risk.
Footnotes
Final revision submitted November 17, 2025; accepted November 30, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: I.H. and K.M. have received support for education from Evolution Surgical. H.B.E. has received consulting fees from OrthoPediatrics and support for education from Pylant Medical. M.R.S. has received consulting fees from WishBone Medical and support for education from MedInc of Texas. M.T. has received consulting fees from OrthoPediatrics. Y.-M.Y. has received consulting fees from Smith & Nephew and OrthoPediatrics. T.G. has received support for education from Paladin Technology Solutions and is an associate editor for AJSM. K.G.S. has received consulting fees from OrthoPediatrics and support for education from Evolution Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.