
Abstract
Background:
Irreducible knee dislocation (IKD) is a rare but severe injury, accounting for approximately 4% of all knee dislocations and characterized by soft tissue incarceration that precludes closed reduction. Current management remains debated, particularly regarding the optimal timing of ligament reconstruction (single- vs. two-stage) and the choice of surgical approach.
Purpose:
To investigate the short-term efficacy and outcomes of 1-stage arthroscopic reduction combined with reconstruction of knee stability for irreducible knee dislocation (IKD).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 16 patients with IKD, treated with 1-stage arthroscopic surgery between June 2015 and July 2022, were included in this study. The surgery involved arthroscopic knee reduction and simultaneous multiligament reconstruction or repair. Side-to-side differences determined with a KT-1000 arthrometer and physical examinations—including the Lachman test, the pivot shift test, the drawer test, and the varus and valgus stress test—were performed for the evaluation of knee joint stability. Other assessments included the International Knee Documentation Committee (IKDC) score, the Lysholm score, pain scores, and satisfaction scores. A paired t test was used to determine the difference between the pre- and postoperative clinical outcomes.
Results:
One patient experienced traumatic redislocation at 1 month due to noncompliance with bracing and was excluded from functional outcome analysis. The remaining 15 patients completed a 2-year follow-up. For all patients included in this study, the mean time from injury to surgery was 5.5 ± 1.4 days, and the mean follow-up time was 27.4 ± 2.6 months. At the last follow-up, all patients had normal or nearly normal Lachman, pivot shift, drawer, and varus and valgus stress tests. The IKDC score was 76.07 ± 2.84 (range, 70-82), the Lysholm score was 81.87 ± 4.22 (range, 74-87), and the pain score was 1±1 (range, 0-3). The satisfaction score was 8.53 ± 0.74 (range, 7-10), which significantly improved compared with the preoperative score (P < .05). No severe complications—including infection, compartment syndrome, neurovascular complications, graft ruptures, or deep vein thrombosis —were observed during follow-up.
Conclusion:
One-stage arthroscopic reduction, combined with reconstruction of knee stability, can effectively restore knee stability and improve clinical outcomes in the treatment of IKD.
Irreducible knee dislocation (IKD) is a rare and severe type of knee injury, accounting for nearly 4% of all knee dislocations.17,19,20 This injury typically occurs during dynamic lower-extremity valgus, which involves a combination of knee flexion and tibial external rotation.8,16 The medial femoral condyle (MFC) then buttonholes through the medial capsule and retinaculum, causing the tibia to dislocate posterolaterally. 1 As the external valgus force around the knee joint decreases or disappears, the medial joint space narrows, leading to the incarceration of invaginated soft tissue within the intercondylar notch, with or without patellar dislocation.13,28 This describes the specific mechanism leading to an IKD.
The dimple sign (pucker sign) refers to a curvilinear skin pucker along the medial joint line.2,3 The presence of this sign is a critical indicator of an IKD, suggesting that early open exploration and reduction are essential when closed manipulation fails.9,27 Additionally, multiple attempts at closed manipulation should be avoided to prevent further soft tissue injury and damage to the blood supply. 12 According to current literature, the most commonly incarcerated soft tissues in the intercondylar notch during closed manipulation include the medial capsuloligament complex (such as the medial capsule, medial retinaculum, and medial collateral ligament [MCL]),8,16,19,20,25 the patellar tendon, 22 the vastus medialis muscle,8,23 or the gastrocnemius muscle.15,26 Early surgical reduction is necessary for this injury, as delayed reduction may lead to immediate and long-term complications—including nerve and blood vessel traction or injury, soft tissue necrosis, contractures, and knee flexion deformities.
Given the extremely low incidence of IKD, there have been very few studies on standard surgical procedures for this condition, and no quantifiable empirical evidence of efficacy has been established. To address this issue, researchers are focusing on several key questions: (1) Open reduction versus arthroscopic reduction? (2) Should ligament reconstruction/repair be performed simultaneously with 1-stage urgent knee reduction, or should it be delayed and performed as a 2-stage procedure after intermediate rehabilitation? (3) Which intra- and extra-articular structures must be repaired?
Since Dubberley et al 5 first introduced arthroscopic reduction as a treatment for IKD decades ago, arthroscopy has evolved significantly with the advancement of various techniques. The ideal surgical approach aims to restore knee stability and function as much as possible in a 1-stage operation, with minimal trauma, reduced pain, and faster recovery. We initiated a protocol of 1-stage arthroscopic reduction combined with knee stability reconstruction for patients with IKD admitted to our hospital. The study aimed to evaluate the clinical performance, safety, and outcomes of our surgical approach. We hypothesized that the proposed 1-stage arthroscopic approach would result in favorable clinical outcomes—including improved knee stability, reduced pain, and functional recovery.
Methods
Patients
This retrospective study was approved by the Medical Ethics Committee of The First People's Hospital of Lianyungang. From June 2015 to July 2022, a total of 20 patients with IKD were admitted to The First People's Hospital of Lianyungang. Of these, 18 patients underwent 1-stage arthroscopic reduction combined with knee stability reconstruction. Although 2 patients were lost to follow-up and 1 patient experienced a recurrence of traumatic redislocation of the knee without knee brace protection 1 month after surgery, the remaining 15 patients completed a 2-year follow-up. Figure 1 illustrates patient enrollment and exclusion criteria. Computed tomography angiography was performed preoperatively to exclude vascular injury. Open wounds and advanced osteoarthritis (Kellgren-Lawrence grade 3 or 4) were excluded to avoid confounding factors related to infection risk and baseline joint degeneration. The exclusion criteria aimed to homogenize the cohort for a focused analysis of arthroscopic feasibility in isolated medial complex injuries. All patients had a minimum follow-up period of 24 months.
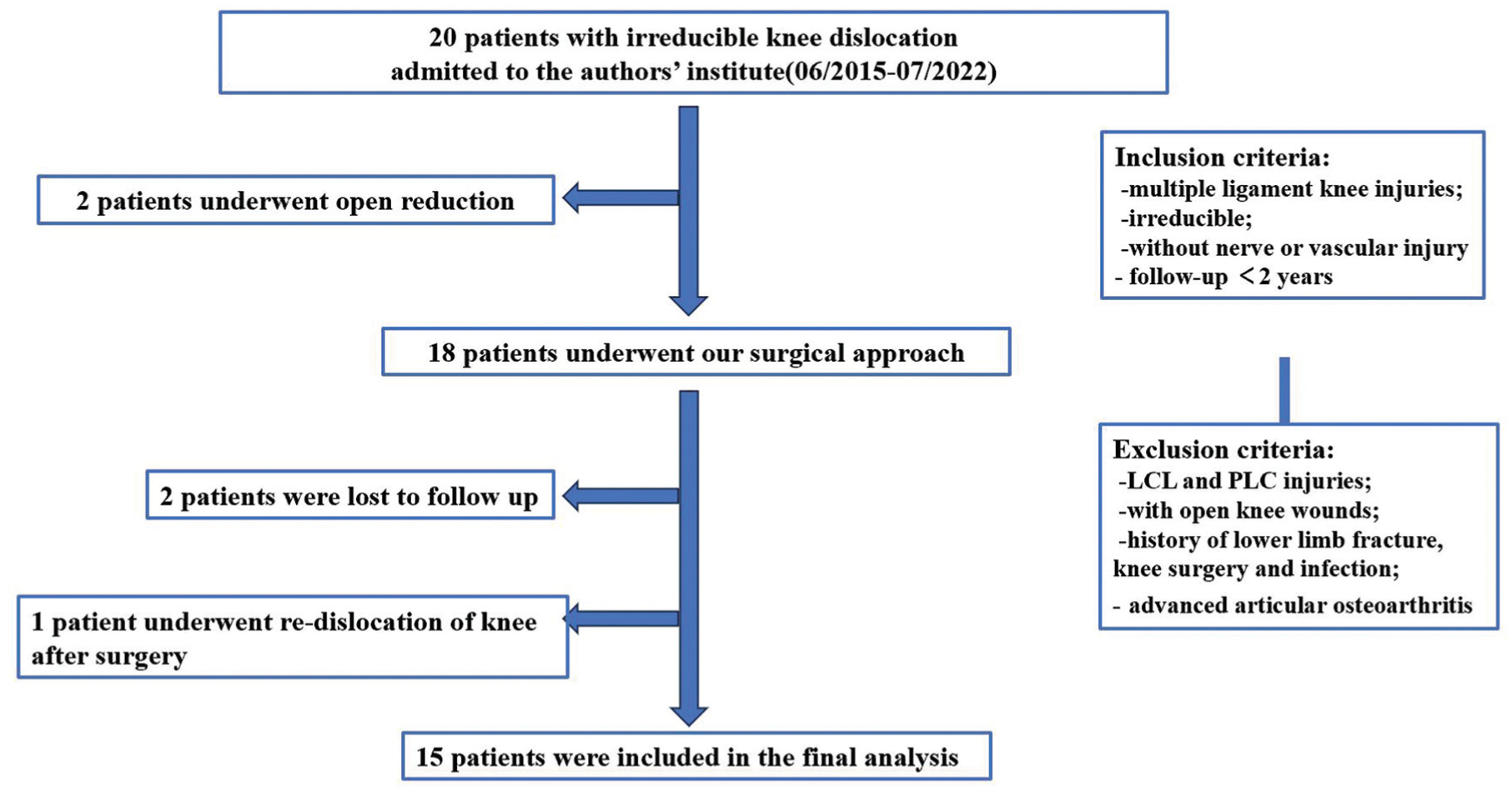
Flowchart and eligibility. ACL, anterior cruciate ligament; LCL, lateral collateral ligament; MCL, medial collateral ligament; MLKI, multiple ligament knee injuries; PCL, posterior cruciate ligament; PLC, posterolateral complex.
Surgical Technique
Arthroscopic Reduction
The same experienced senior surgeon (X.L.) performed all surgeries. After induction of general anesthesia, the patient was placed in a supine position. The knee joint was examined by arthroscope through a standard anterolateral and anteromedial approach (Figure 2). The medial capsuloligament complex was found incarcerated in the medial compartment, tightly adherent to the MFC and button-holed by the condyle, preventing knee joint reduction. Both the anterior and posterior cruciate ligaments (PCL) were found to be completely torn. The incarcerated medial capsuloligament complex was carefully debrided using a motorized shaver and released from the MFC until the condyle was well visualized and the knee was fully reduced. Subsequently, a comprehensive arthroscopic examination of the affected knee joint was performed to evaluate the overall condition of the joint, with or without concomitant injuries of other structures such as the meniscus, the medial patellofemoral ligament (MPFL), and the MCL (Please refer to the Supplemental video for details of the surgical procedure).

One-stage operation procedure. Arthroscopic views of a right knee via anterolateral portal. (A) The intra-articular anatomic structures were severely disrupted, with complete ruptures of both the ACL and PCL (▵). (B) The MFC buttonholes through the medial capsule (*) and entraps the medial capsuloligament complex. (C, D) The incarcerated medial capsuloligament complex (
ACL and PCL Reconstruction
All patients underwent arthroscopic anatomic single-bundle anterior cruciate ligament (ACL) and PCL reconstruction using the ipsilateral hamstring tendon and peroneus longus tendon autografts at the aforementioned institution. Ipsilateral hamstring and peroneus longus tendons were used for reconstruction because of their availability and the absence of allografts at our institution. These tendons provide robust support and are routinely used in our practice. The reconstruction began with the drilling of transosseous tunnels: first the PCL tunnel, then the ACL tunnel. The guide pin was inserted 7 mm posterior to the distal articular cartilage border of the MFC (equivalent to the 1 to 2 o'clock position in the right knee). The PCL tibial tunnel was drilled in the PCL fossa, 15 mm below the articular surface. The guide pin for the ACL femoral tunnel was inserted with the knee in 20° of flexion, using the original ACL femoral footprint as a landmark. The tibial tunnel was drilled in the center of the ACL anatomic tibial footprint, located at the posterior border of the anterior horn of the lateral meniscus, using an ACL tibial tunnel guide. 10 After the tendon autografts were passed, a fixed-loop device was used for femoral suspensory fixation. In contrast, tibial fixation was achieved using a hybrid technique combining intratunnel aperture fixation and extracortical suspensory fixation.
Repair of Other Knee Structures
Meniscal lesions were addressed with either partial meniscectomy or meniscal repair under arthroscopy, depending on the tear pattern and location. Additionally, for patients with MPFL and MCL injuries, a longitudinal incision was made along the medial side of the knee joint to separate the skin and muscles, exposing the medial femoral epicondyle. The MPFL and MCL femoral remnants were identified and reattached to their original femoral attachment site with suture anchors. The torn medial capsule and retinaculum were simultaneously repaired. In the case of MPFL and MCL repairs, a semi-open approach was required due to the severity of the injury and to ensure knee stability during the early phase of recovery. However, this was only performed when strictly necessary and is considered an adjunct to the overall arthroscopic approach. The semi-open adjunct did not compromise the arthroscopic minimally invasive nature, as the additional incision length was 3.5 cm.
Rehabilitation
All patients wore a hinged knee brace for 3 months, with their knee joints immobilized in full extension for the first 2 weeks postoperatively. After 2 to 3 weeks, patients were allowed to begin passive and active gentle flexion and extension exercises. Patients were encouraged to increase knee flexion to 90° by 4 weeks and to 120° (or full range of motion) by 6 weeks. In addition to joint motion exercises, ankle pump exercises, and muscle strengthening are integral components of the rehabilitation process. Weightbearing was strictly prohibited for the first 6 weeks postoperatively. Partial weightbearing with knee brace protection was allowed at 6 weeks postoperatively, with full weightbearing permitted at 3 months.
Follow-up and Clinical Assessments
The follow-up commenced postoperatively and continued for a minimum of 2 years. Demographic parameters included age, sex, body mass index, cause of trauma, and time from injury to surgery. The clinical assessment included evaluation of knee joint stability and knee function. Knee physical examinations—including the Lachman test, pivot shift test, 24° drawer test, and varus and valgus stress test—were performed to evaluate knee joint stability. 24 The side-to-side difference (SSD) in anterior tibial translation was measured using a KT-1000 arthrometer by the same senior surgeon at 6 weeks, 1 year, and 2 years postoperatively. Laxity was assessed according to International Knee Documentation Committee (IKDC) standards based on SSD: normal (<3 mm), nearly normal (3-5 mm), abnormal (6-10 mm), and severe (>10 mm). 29 Knee function was evaluated using the Lysholm score and the IKDC score at 1- and 2-year follow-ups. Additionally, numerical rating scales for pain and satisfaction were recorded. Pain (0-10, 0 = no pain) and satisfaction (0-10, 10 = very satisfied) were rated. All the data were collected by trained clinical research staff (S.M., H.L.) and later cross-checked.
Statistical Analysis
All statistical analyses were performed using SPSS software (IBM-SPSS Statistics 22.0). Continuous variables were expressed as mean ± standard deviation. A paired t test was used to determine the difference between the pre- and postoperative clinical outcomes. The significance level was set at P = .05.
Results
Finally, 16 patients (10 men and 6 women), with a mean age of 48.4 ± 7.3 years, were included in this study (Table 1). The mean time from injury to surgery was 5.5 ± 1.4 days, and the mean follow-up time was 27.4 ± 2.6 months. Before admission to our hospital, 9 of all patients were injured in traffic accidents, 2 in falls, 3 in sporting activities, and 1 in an industrial accident. One 71-year-old man (patient No. 16) sustained a traumatic redislocation at 1 month postoperatively due to noncompliance with brace wear and weightbearing restrictions. He was excluded from functional outcome analysis due to a lack of follow-up data beyond the failure event. The patient was a 71-year-old man with poor compliance to postoperative rehabilitation—including wearing the knee brace and avoiding weightbearing. In addition, he was referred to our hospital and underwent surgery 1 month after the first accident, which indicated a higher probability of the incarcerated soft tissue necrosis. Several factors—including the patient's age and expectations, underlying conditions, compliance, and soft-tissue status—should be considered when planning revision surgery. We eventually performed an open reduction and arthrodesis of the knee in this patient using crossing Kirschner wires and an external fixator.
Demographic Data a

ACL, anterior cruciate ligament; BMI, body mass index; F, female; LCL, lateral collateral ligament; M, male; MCL, medial collateral ligament; PCL, posterior cruciate ligament.
All patients had an obvious knee dislocation with a characteristic dimple sign on the medial aspect of the knee. The IKD was further confirmed by imaging examinations (radiograph and magnetic resonance imaging [MRI]) (Figure 3). Several attempts at closed manipulation under sedation and anesthesia were made but failed. It was observed that vascular or nerve damage did not occur in any of the patients. All the patients underwent 1-stage arthroscopic reduction combined with ligament reconstruction or repair. Among them, 10 patients underwent ACL/PCL reconstruction and MCL repair, 3 patients underwent ACL/PCL reconstruction, 1 patient underwent ACL/PCL reconstruction + MCL repair + meniscal repair, 1 patient underwent ACL/PCL reconstruction + MCL/MPFL repair, and 1 patient underwent ACL/PCL reconstruction + meniscal repair.

Representative clinical and imaging findings. (A) The dimple sign (arrow). (B, C, D) Preoperative imaging revealed knee dislocation, soft tissue incarceration, and ligament rupture. (E, F, G, H) Postreduction and ligament reconstruction imaging revealed restored anatomic alignment of the knee joint, resolution of soft tissue incarceration, and favorable morphology and alignment of the reconstructed ligaments. The arrow on F indicates the reconstructed anterior cruciate ligament (ACL) graft. The arrow on G indicates the reconstructed posterior cruciate ligament (PCL) graft.
In the early postoperative period, all patients had negative Lachman, pivot-shift, and KT-1000 test results. Both the posterior drawer test finding and the valgus stress test finding were normal in 13 patients and nearly normal in 2 patients. At 1- and 2-year follow-up, the vast majority of patients' physical examination and test findings remain normal or nearly normal (Table 2).
Postoperative Physical Examinations at Different Time Points a
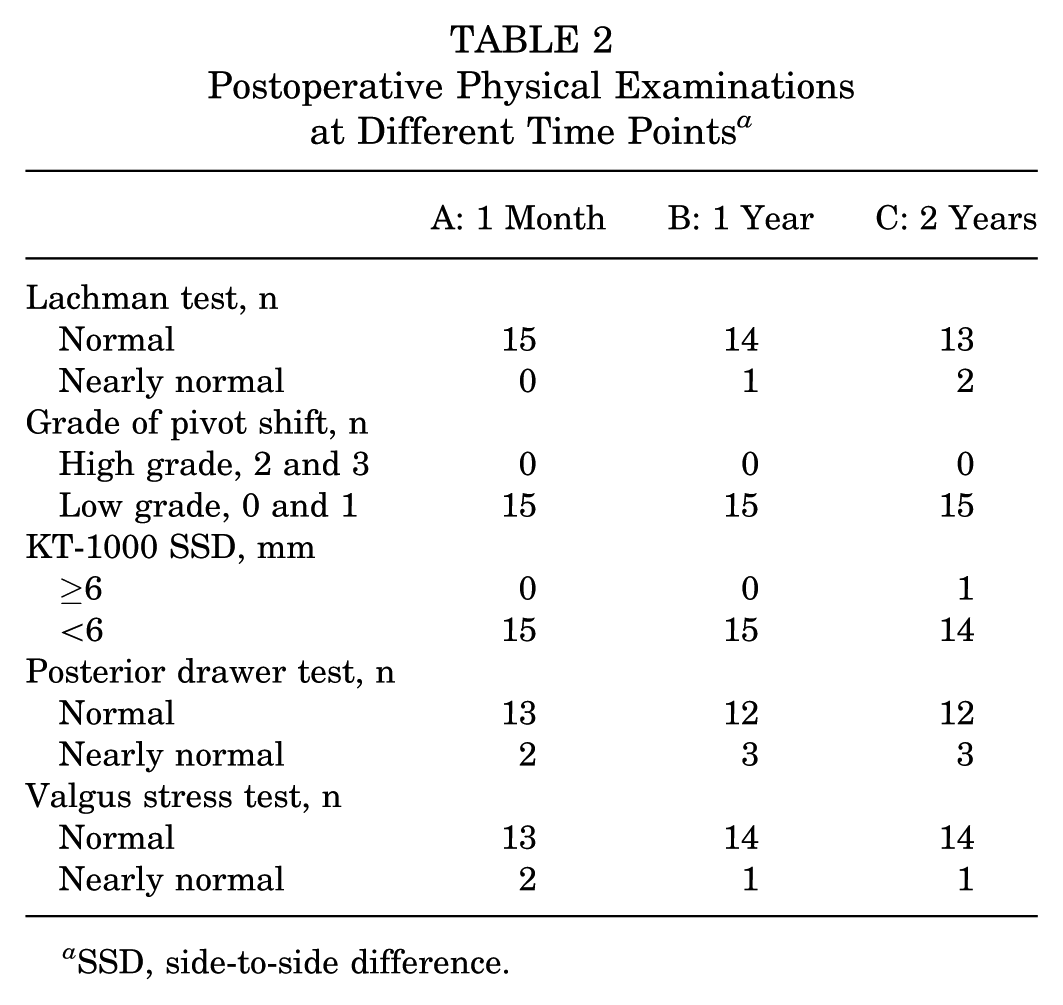
SSD, side-to-side difference.
The preoperative pain, Lysholm, and IKDC scores were 8.27 ± 0.80, 5.40 ± 0.83, and 7.07 ± 1.44, respectively. The postoperative Lysholm and IKDC scores at 1-year follow-up were 1.40 ± 1.05, 79.80 ± 3.95, and 74.20 ± 2.65. The scores were further increased at the 2-year follow-up. The mean patient satisfaction score increased during the follow-up period, from 7.93 ± 0.46 at 1 year postoperatively to 8.53 ± 0.74 at 2 years postoperatively (Table 3).
Comparison of Pre- and Postoperative Functional Numerical Rating Scale Scores for Pain, Function, and Patient Satisfaction a

Data are presented as mean ± SD, unless otherwise indicated. IKDC, International Knee Documentation Committee; Preop, preoperative.
During the 2-year follow-up, none of the 15 patients included in the study had any severe postoperative complications, such as incisional infection, compartment syndrome, neurovascular complications, or graft rupture. Two patients had a transient fever (38°C) within 3 days, which resolved within 24 hours. Two patients experienced persistent stiffness with limited flexion of less than 90° at 3 months postoperatively. One of the patients had an arthroscopic arthrolysis followed by manipulation, while the other patient had manipulation under anesthesia alone. At the final follow-up, both patients had returned to full knee range without any flexion or extension deficit.
Discussion
In this study, 16 patients with IKD underwent 1-stage arthroscopic reduction combined with knee stability reconstruction. During the 2-year follow-up period, 16 patients achieved normal or nearly normal knee stability and satisfactory clinical outcomes. The results suggest that the 1-stage arthroscopic surgical treatment for IKD yields good short- and mid-term clinical outcomes.
Knee dislocation is a rare condition that can be catastrophic if not diagnosed promptly or accurately. 21 Most knee dislocations can be treated with closed reduction, but in rare cases, closed manipulation under anesthesia fails, resulting in IKD. Soft tissue incarceration is widely considered the primary characteristic of IKD. The incarcerated soft tissue typically involves the medial structures of the knee—including the medial capsule, medial retinacular, MCL, patellar tendon, vastus medialis muscle, or gastrocnemius muscle. The joint structures most vulnerable to damage include the ACL, PCL, and MCL. However, Wei Chen et al 10 reported 2 cases of IKD with incarceration of the lateral femoral condyle in the posterolateral capsuloligamentary structures, in which the ACL, PCL, MCL, and LCL were avulsed concurrently.
In an IKD, the MFC buttonholes through the medial capsule, entrapping the medial capsuloligament complex and pushing it into the joint with gentle traction. 11 The resultant skin dimple along the medial joint line is referred to as the dimple sign. The dimple sign was present in all our cases in this study, indicating that surgical management was unavoidable. Delayed surgery and multiple attempts at closed reduction significantly increase the risk of neurovascular and soft tissue injury. The mean time from injury to surgery was 5.5 ± 1.4 days. The delay in surgery was due to logistical issues, patient condition stabilization, and the complexity of the injuries. Despite the delay, no major complications, such as ischemic tissue damage, were observed in the patients.
Meticulous preoperative planning is essential for achieving favorable long-term clinical results. Most existing studies are case reports because IKD is rare. Currently, there is no consensus on the optimal surgical approach for this condition. Quinlan and Sharrard 16 performed an open reduction, delivering the medial ligament and capsule out of the joint, which allowed complete reduction of the dislocation. Polyzois et al 14 reported that gradual reduction using the Ilizarov technique, followed by arthroscopic ligamentous reconstruction, is a reliable alternative to open surgery. Soheil Samim et al 3 first showed us the arthroscopic view of an IKD: the MFC was buttonholed through the anteromedial capsule and retinaculum. However, their attempt to reduce the dislocation arthroscopically failed, necessitating an open reduction. Dubberley et al 5 demonstrated that arthroscopic debridement of the incarcerated soft tissue enabled joint reduction without the need for open surgery. In recent years, arthroscopic and arthroscopically assisted techniques have been increasingly employed for the treatment of IKD.6,18 However, there have been reports on failed arthroscopic reduction of the joint. 7 In this study, all surgical reduction procedures were performed arthroscopically, some with success.
Tears of the MCL are the most common ligament injuries among the medial stabilizing structures of the knee. We recommend repairing the MCL in a 1-stage operation, which is important for postoperative knee joint stability. During arthroscopic release of the incarcerated soft tissue, the MFC should be carefully exposed, and excessive damage to the MCL remnant must be avoided. After knee joint reduction, which intra-articular tissue structures (such as the ACL, PCL, and meniscus) need to be repaired or reconstructed has not yet reached consensus. Saini et al 19 reported a case of IKD treated with open reduction and isolated PCL reconstruction followed by gradual rehabilitation with a good outcome at 3-year follow-up. Dubberley et al 5 performed arthroscopic debridement and reduction of the knee joint alone in the 2 patients without any ligament repair or reconstruction. After 3 months, 1 patient underwent a second arthroscopy for arthrofibrosis of the injured knee, and evidence of MCL healing was found. The other patient went on to develop symptomatic laxity and underwent ACL + PCL + MCL reconstruction. We consider it essential to repair or reconstruct the ACL, PCL, MCL, and other critical structures in a single-stage operation to improve knee stability and clinical outcomes.
Once an IKD is identified, immediate reduction is necessary to prevent soft tissue necrosis and preserve knee function. Said and Learmonth 18 performed a 2-stage surgical procedure. The first stage involved arthroscopic debridement of the incarcerated soft tissue, followed by knee reduction and open MCL repair. The second stage consisted of ACL and PCL reconstruction. Silverberg and Acus 23 reported their treatment of an IKD with interposition of the vastus medialis. They removed the muscle belly from the notch and medial compartment to expose and release the incarcerated MCL and capsule. A congruent reduction was then achieved, and the MCL and PCL were repaired. The ACL was reconstructed at 9 months after the first stage operation. Overall knee joint stability remained satisfactory to excellent after nineteen months. Cui et al 4 also demonstrated that 2-stage surgery combined with intermediate rehabilitation can achieve good efficacy and result in a satisfactory functional outcome. Hongwu and Li 6 argued that 1-stage reduction combined with multiligament reconstruction or repair is effective and reliable. Indeed, in our study, the vast majority of patients with IKD achieved excellent recovery following their personalized, professional rehabilitation protocol after the 1-stage operation. Our results suggest that concerns about potential high rates of arthrofibrosis and knee stiffness associated with 1-stage operation are unwarranted. A single-stage approach was chosen for its potential to enable faster recovery and reduce hospital stays. Compared with double-stage surgeries, the single-stage approach provided immediate stability and recovery of knee function, as shown by our clinical outcomes.
One elderly patient with poor compliance experienced early redislocation, underscoring the importance of adherence to the postoperative protocol.
Limitations
This study has several limitations. This was a retrospective study. Given the low incidence of IKD, determining an adequate sample size was difficult. No control group was included in this study. Outcome assessments by the operating surgeon may introduce observer bias. Furthermore, postoperative stability was assessed primarily through clinical examinations (eg, Lachman test, pivot-shift test) and patient-reported outcome measures (eg, IKDC, Lysholm scores), as standardized postoperative MRI or stress radiographs were not part of our protocol. While these clinical tools are validated and widely used, the lack of objective imaging confirmation of ligament healing is a recognized limitation of our methodology. Future studies would be strengthened by incorporating such imaging modalities to correlate clinical findings with anatomic outcomes. Finally, the 2-year follow-up period is relatively short to assess long-term complications such as osteoarthritis.
Conclusion
One-stage arthroscopic reduction combined with knee stability reconstruction is a safe, effective, and minimally invasive procedure for patients with IKD.
Footnotes
Final revision submitted September 22, 2025; accepted October 19, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Medical Ethics Committee of The First People's Hospital of Lianyungang.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.