
Abstract
Introduction:
There is a lack of in vivo studies comparing the functional outcome and knee stability after anterior cruciate ligament reconstruction (ACLR) using fixed loop (EndoButton (EB) CL) and adjustable loop (TightRope (TR) RT) devices for femoral fixation of soft tissue grafts.
Materials and methods:
Functional outcomes were assessed in terms of the International Knee Documentation Committee (IKDC) and Lysholm scores, knee stability by anteroposterior laxity and side-to-side difference (SSD) using KT-1000 arthrometer. The evaluation was performed preoperatively and post-operatively at 6 months and 2 years.
Results:
Both groups were matched in terms of demographic, preoperative, intraoperative and post-operative covariates. EB (n = 52) appeared to have better IKDC and Lysholm scores at 6 months post-operative when compared to TR (n = 50). However, at a final follow-up of 2 years, the results were similar. The anterior tibial translation and SSD were statistically insignificant between the two groups at 6 months and 2 years.
Conclusion:
ACLR using EB or TR for femoral fixation gives substantially equivalent functional results and knee stability at mid-term follow-up.
Introduction
Arthroscopic anterior cruciate ligament reconstruction (ACLR) is currently the gold standard treatment for anterior cruciate ligament (ACL) tear, and the most commonly used free tendon grafts are autologous bone-patellar tendon-bone and hamstring tendons. 1 The objectives of ACLR are early rehabilitation and return to pre-injury activity. 2 Numerous graft fixation options are available for both tibia and femur, with continuous advancement in technology. 1 The weakest link in the early post-operative period are the fixation points of the graft in femoral and tibial tunnels. 3 Cortical suspensory fixation is the current standard femoral fixation method for soft tissue grafts and is in widespread use. 4 EndoButton (EB) CL (Smith & Nephew Inc, Andover, Massachusetts, USA) is one such device. But it is not without limitations, as it requires over-drilling of the femoral socket to allow for it to flip at lateral femoral cortex. As a result of this over-drilling, some part of the socket is not filled by the graft, hence leaving scope for graft motion within the tunnel, which can hamper graft incorporation and cause tunnel widening. 4 Secondly, an error in measuring the length of the socket to be drilled can lead to either inability to flip the button or an insufficient graft length within the bone. 5 Thirdly, as recent trend towards an anatomic tunnel placement can lead to short tunnel length, there is a concern for adequate graft length in the bone. 5
In order to overcome these problems, intention to conserve bone and to achieve a better functional outcome, second generation suspensory fixation devices were introduced, for example, TightRope (TR) RT (Arthrex Inc, Naples, Florida, USA) and ToggleLoc with ZipLoop (Biomet Inc, Warsaw, Indiana, USA). These adjustable loop devices can be tightened intraoperatively, thus obviating the need for over-drilling. 4,6
There are a few in vitro studies comparing biomechanical properties of these two devices. 4,5,7 –10 Although the study designs and testing mechanisms are heterogeneous, they clearly demonstrate that fixed loop devices are biomechanically superior to adjustable loop devices. To the best of our knowledge, there are only three studies in the literature which compare the two devices in vivo. 11 –13 None of them have shown clinical superiority of one device over the other. We conducted this prospective study to find out which device fared better in terms of functional outcomes and laxity measurements at a final follow-up of 2 years.
Materials and methods
Patients undergoing primary arthroscopic ACLR using autologous hamstring graft, performed at a tertiary centre between November 2012 and August 2014, were included in the study. In EB group, the femoral fixation of quadrupled graft was done using EB CL Ultra (Smith & Nephew Inc, Andover, Massachusetts, USA) and in TR group using the TR (Arthrex Inc, Naples, Florida, USA). The inclusion criteria were a clinical and radiological evidence of ACL tear, age between 18 and 50 years with normal contralateral knee. Patients with posterior cruciate ligament tear, associated tibial plateau fracture, bilateral knee injury, suspected infection, and patients not consenting for inclusion in the study were excluded. Patients were allotted to either group using an online random number table generator. Institutional ethics committee clearance was obtained in accordance with the 1964 Helsinki declaration and its later amendments and informed consent was taken from all participants.
After arthroscopic confirmation of a complete ACL tear, ipsilateral semitendinosus and gracilis were harvested and prepared. The femoral tunnel was drilled at 110—120° of knee flexion via the accessory anteromedial portal. The tibial tunnel was made using the tibial jig set at 55°. Diameter of the tunnels was decided based on the graft thickness. The graft fixation on the femoral side was done either with EB or TR. While in the EB group the femoral tunnel was over-drilled by 10 mm above the desired intraosseous graft length, the same was not required in case of TR. The fixation on the tibial side was done using interference screw (bioscrew) in either group.
Knee brace was applied post-operatively. Antibiotics were given according to the hospital protocol. Similar post-operative physiotherapy regime was followed for both the group. Clinical outcome was assessed by two independent observers who were blinded to the implant used, by using International Knee Documentation Committee (IKDC) and Lysholm scoring. Knee stability was evaluated by measuring anterior tibial translation (ATT) using KT-1000 arthrometer and by calculating side-to-side difference (SSD) of ATT. Assessment was done at 6 months and 2 years post-operatively. Statistical analysis was done using paired and unpaired Student’s t test for continuous data and Fisher’s exact test for categorical data.
Results
A total of 109 patients were initially included in the study. Five patients were lost to follow-up and two patients refused to give consent, hence for final analysis 102 patients were available (52 in EB group and 50 in TR group). Both the groups were comparable in terms of demographic details and preoperative scores and findings (Table 1).
Demographic parameters and preoperative scores.
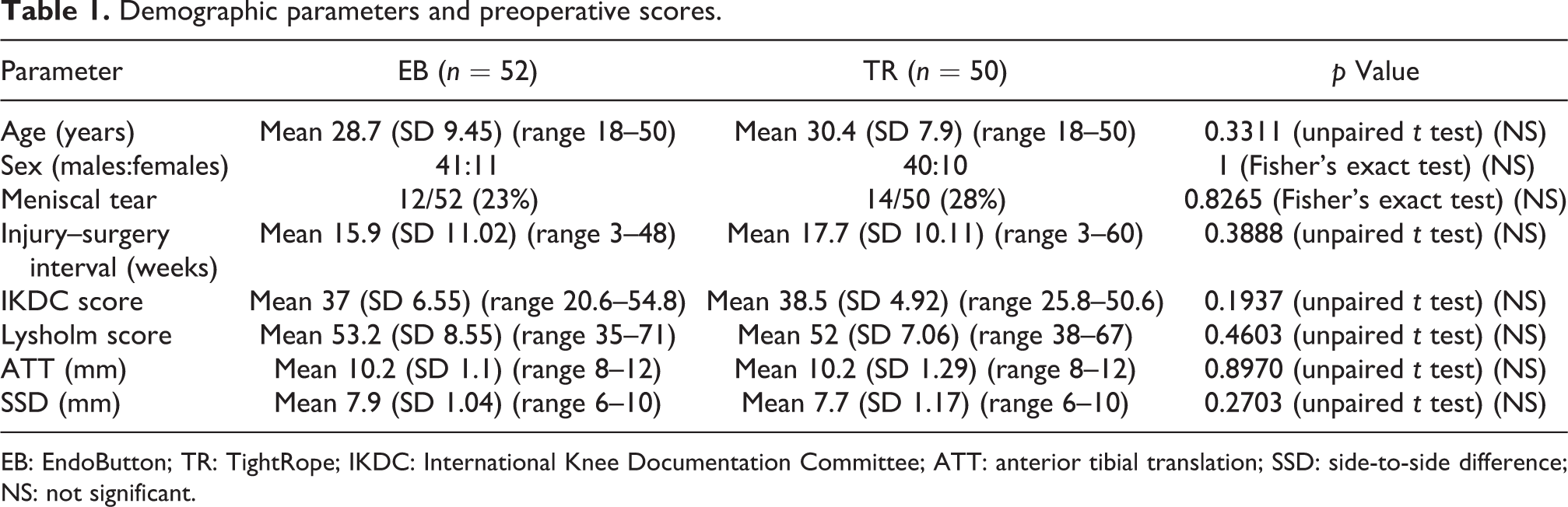
EB: EndoButton; TR: TightRope; IKDC: International Knee Documentation Committee; ATT: anterior tibial translation; SSD: side-to-side difference; NS: not significant.
The mean Lysholm scores and IKDC scores at 6 months and 2 years after surgery were significantly improved as compared with mean preoperative scores in both the groups. At 6 months’ follow-up, both scores were significantly better in the EB group (Table 2). However, this difference was not apparent at 2 years’ follow-up (Table 2). Hence, at final follow-up of 2 years, both groups were comparable with respect to Lysholm and IKDC scores.
Outcome analysis at 6 months and 24 months after surgery.

EB: EndoButton; TR: TightRope; IKDC: International Knee Documentation Committee; ATT: anterior tibial translation; SSD: side-to-side difference; SS: statistically significant; NS: not significant.
ATT also improved significantly at 6 months and 2 years post-operatively when compared with the preoperative value in both the groups. Also, ATT was similar in both the groups at 6 months and 24 months follow-up. Similar trend was also observed for the SSD (Table 2). Failure of ACLR was observed in two patients in EB group and one patient in TR group. All cases of failure were due to significant re-injury.
Discussion
In suspensory fixation, the recent shift from EB to TR has been due to the ease of use and variability of length with the shorter femoral tunnel, but post-operative laxity (due to loosening over time) has been an issue for some surgeons. 4,5 The rationale behind TR design is that a shorter vacant tunnel length between button of TR and lateral most end of hamstring graft will potentially reduce the ‘bungee cord’ effect, hence decreasing tunnel widening. 13 However, biomechanical studies have shown that as time progresses, adjustable loop devices lengthen, which may result in loosening of the graft and clinical failure. 4,5,7 –10 It is a well-known observation that biomechanical testing data do not always translate into clinical and functional results, because in vitro conditions can be very different from in vivo conditions. Only a handful of clinical studies comparing fixed loop to adjustable loop devices have been done. 11 –13 None of these studies have shown a significant difference in terms of clinical scores, tunnel widening and KT-1000 readings. Our study also corroborates these findings. Table 3 summarizes the findings of previous clinical and biomechanical studies.
A review of biomechanical and clinical studies comparing EB and TR devices.

EB: EndoButton; TR: TightRope; TL: ToggleLoc; BS: biodegradable screw; RB: RetroButton; XOB: XO Button; IKDC: International Knee Documentation Committee; SSD: side-to-side difference.
EB is currently the most accepted device for the fixation of soft tissue grafts in arthroscopic ACLR, despite of having potential disadvantage that it requires 6–10 mm of over-drilling of the femoral tunnel in order to flip the button on the lateral femoral cortex. 6 Theoretically, this may lead to excessive graft motion in the tunnel, tunnel widening and delay in graft tunnel healing. It has been shown that new bone ingrowth around the tendon graft is inversely related to the magnitude of graft motion within the tunnel. 14,15 As over-drilling is not needed in TR, it has a potential of improving graft healing within the tunnel, possibly resulting in a better clinical outcome. 6 Another advantage of TR is the intraoperative flexibility it provides to the surgeon, as it can be tightened even after flipping.
An interesting finding in the present study was better functional results at 6 months in EB group as compared to TR group; however, the results at the end of 2 years were similar. Although the explanation for this discrepancy is unclear, it may be due to small sample size or difference in rehabilitation capacity of patients. In contrast to the IKDC and Lysholm scores, the ATT and SSD measurements were similar in both the groups at 6 months and 2 years’ follow-up.
A comprehensive review of previous biomechanical and clinical studies is presented in Table 3. Advantages and disadvantages of both fixation devices are present in Table 4.
A comparison between EB and TR.
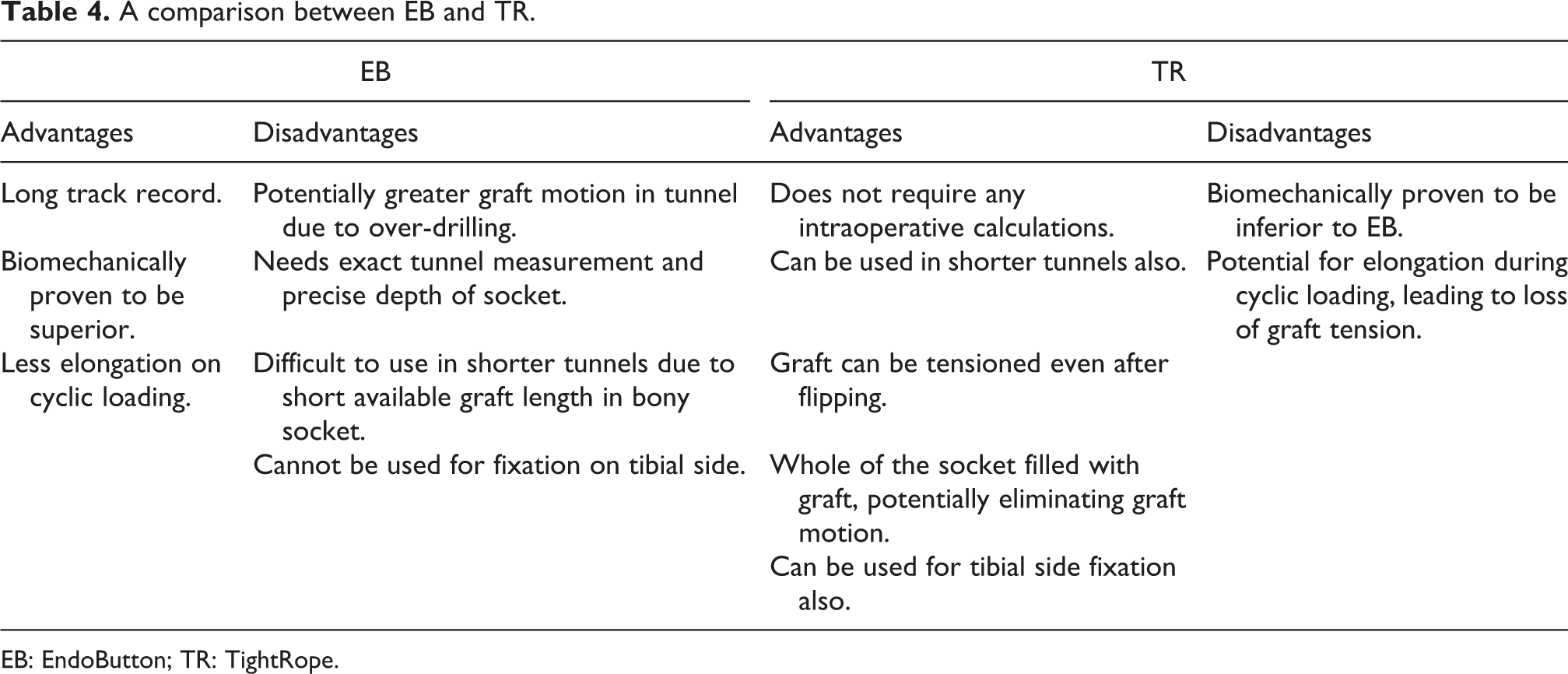
EB: EndoButton; TR: TightRope.
Limitations of our study include a small sample size, and lack of measurement of tunnel widening at final follow-up.
Conclusions
Final follow-up of 2 years revealed similar knee scores and laxity in the two groups. Although many in vitro studies have shown that adjustable loop devices lengthen with cyclic displacement and are biomechanically inferior to fixed loop devices, previous clinical studies as well as our study fail to corroborate this. Hence, the biomechanical data must be interpreted with caution. The logical step forward would be to conduct well-designed Randomized Control Trials comparing the two devices. Until further evidence clearly shows the superiority of one device over the other, both can be expected to yield similar results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.