
Abstract
Background:
Few reports have examined the relationship between anterolateral ligament (ALL) injury or deep medial collateral ligament (dMCL) and meniscal injury in an acute anterior cruciate ligament (ACL)–injured knee.
Purpose/Hypothesis:
The purpose of this study was to investigate the association between ALL or dMCL injury observed on magnetic resonance imaging (MRI) in acute ACL injury with meniscal ramp lesions and lateral meniscus (LM) oblique radial tears (LMORTs) or localization of bone marrow lesions (BML), preoperative anterior tibial translation (ATT), and rotational instability. It was hypothesized that ALL or dMCL injuries accompanying acute ACL-injured knees are linked to meniscal injuries, such as ramp lesions or LMORT, BML, and increased knee instability.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
This study included 164 patients who underwent MRI ≤1 month after primary ACL injury. All participants underwent evaluation of the side-to-side difference in ATT on stress radiographs and manual pivot-shift test preoperatively. ALL or dMCL injury and BML localization were diagnosed using MRI, and meniscal injuries were diagnosed via arthroscopy during ACL reconstruction. The relationship between concomitant meniscal injuries, BML, and knee instability in the ALL-injured and -intact groups, as well as in the dMCL-injured and -intact groups, was evaluated.
Results:
Overall, 89 of 164 (54.3%) knees had ALL injuries, 101 (61.6%) knees had dMCL injuries, and 64 (39.0%) knees had both ALL and dMCL injuries on MRI. ALL injuries were significantly correlated with ramp lesions, other LM injuries, and BML in both the lateral femoral condyle (LFC) and the lateral tibial plateau (LTP) (P < .05). dMCL injury was significantly correlated with LMORT, other LM injuries, BML in the LFC, and BML in the LTP (P < .05). ALL or dMCL injuries observed on MRI did not increase knee instability. Ramp lesions (odds ratio [OR], 3.70; P = .001), BML in LFC (OR, 2.17; P = .03), and BML in LTP (OR, 2.00; P = .04) were independent factors that increased the odds of finding associated ALL injury, whereas LMORT (OR, 3.01; P = .04) and BML in LTP (OR, 2.90; P = .002) independently increased the odds of dMCL injury.
Conclusion:
In the acute phase of ACL injury, ramp lesions and BML in LFC, and BML in LTP were an independent factor that increased the odds of finding ALL injury, whereas LMORT and BML in LTP independently increased the odds of having associated dMCL injury.
Keywords
In 2013, Claes et al 5 mentioned that the ALL was a distinct ligament on the lateral side of the knee joint. The ALL contributes to rotational control of the knee and, in conjunction with the ACL, resists anterolateral rotational instability.3,13,17,21,49 The MCL is divided into the superficial MCL (sMCL) and dMCL.20,47 The dMCL comprises the meniscofemoral and meniscotibial ligaments, which stabilize the meniscus. 31 While the sMCL primarily resists valgus forces in extension, the dMCL works with the posterior oblique ligament to provide rotational stability to the knee.1,35 These ligaments are known to sustain concomitant injuries in patients with ACL injury.10,18,48 Similarly, characteristic meniscal injuries associated with ACL tears, such as ramp lesions of the medial meniscus and lateral meniscal oblique radial tears (LMORTs), have been well recognized.2,6,8,11,22,24,40,45,46 Meniscal and ligamentous injuries significantly increase the force in the ACL graft during varus/valgus and internal/external rotational torque, and untreated injuries are factors that cause graft failure following ACLreconstruction (ACLR).1,13,16,26,29,41 ACL injury rarely occurs in isolation, and awareness of concomitant ligamentous and/or meniscal injuries is essential since overlooked associated peripheral laxities are one of the common causes of ACL graft failure even in the absence of technical error in ACLR.7,8,37,48
Sonnery-Cottet et al 39 reported favorable outcomes following ACLR combined with ALL reconstruction in patients with ACL tears and concomitant ramp lesions. However, the association between ALL or dMCL injury and meniscal injury, such as ramp lesion or LMORT in ACL-deficient knees, remains unclear. In addition, localization of bone marrow lesion (BML) observed on MRI can provide data for determining the underlying mechanism of injury in ACL ruptures; however, the relationship between these lesions and concomitant soft tissue injuries mentioned above has not been well-defined. 28 Recognizing concomitant peripheral injuries in ACL-injured knees and understanding their relationships would greatly assist arthroscopic surgeons in identifying and treating these crucial ligaments and associated meniscal tears.
This study aimed to determine whether ALL or dMCL injuries observed on MRI in acute ACL-deficient knees were associated with concomitant meniscal injuries, BMLs, and greater knee instability. We hypothesized that ALL or dMCL injury accompanying an ACL-injured knee is linked to meniscal injuries, such as ramp lesion or LMORT, BML localization, and greater rotational knee instability.
Methods
Study Design and Participants
This retrospective study of prospectively collected data was approved by the institutional review board of our institution. Informed consent was obtained from all participants. Between August 2018 and May 2024, a total of 251 consecutive patients underwent ACLR in our hospital. Patients who underwent 1.5-T MRI at a nearby affiliated clinic or 3-T MRI (Siemens) at our institute ≤1 month following ACL injury were enrolled in this study. Patients who underwent an MRI scan >1 month following ACL injury, underwent revision ACLR, had a posterior cruciate ligament (PCL) injury or lateral collateral ligament (LCL) injury that required primary repair or reconstruction, or had previous injury or surgery of the ipsilateral knee were excluded from this study. The study participants were divided into ALL injury (ALL+) and ALL intact (ALL–) groups or dMCL injury (dMCL+) and dMCL intact (dMCL–) groups. Participants’ characteristics are listed in Table 1.
Participants’ Characteristics (N = 164) a

Data are presented as mean ± SD or n (%) unless otherwise indicated. ALL, anterolateral ligament; BML, bone marrow lesion; dMCL, deep layer of medial collateral ligament; LFC, lateral femoral condyle; LM, lateral meniscus; LMORT, lateral meniscus posterior oblique tear; LTP, lateral tibial plateau; MFC, medial femoral condyle; MM, medial meniscus; MRI, magnetic resonance imaging; MTP, medial tibial plateau.
MRI Assessment
All participants were evaluated for the presence or absence of ALL and dMCL injury on MRI ≤1 month following ACL injury by an arthroscopic surgeon with >15 years of experience in musculoskeletal interpretation (S.N.) and a junior resident of radiology (E.S.) in a blinded manner. Since one of a MRI reader (S.N.) was involved in the surgery, the results of this study are adopted the interpretation by E.S., who was not involved in the surgery. To assess intraobserver agreement, interpretation by E.S. was performed twice, with an interval of ≥2 months between each analysis, and interpretation by S.N. was used to assess interobserver agreement. ALL tears were defined as partial or complete discontinuous low signal intensity fibers (Figure 1).14,43 The bony avulsion of the tibial insertion (Segond fracture) was also defined as one of the ALL injuries (Figure 2). 4 Irregularities and periligamentous edema were included in ALL tear (Figure 3).5,15 A dMCL injury was defined as a tear in the meniscofemoral and/or meniscotibial ligament (Figure 4).20,32 The presence of all meniscal injuries was confirmed using arthroscopy during ACLR. To avoid overlooking ramp lesions during arthroscopy, preoperative hyperflexion MRI, as reported by Nonaka et al., was performed in all patients to improve the preoperative detection of ramp lesions. 30
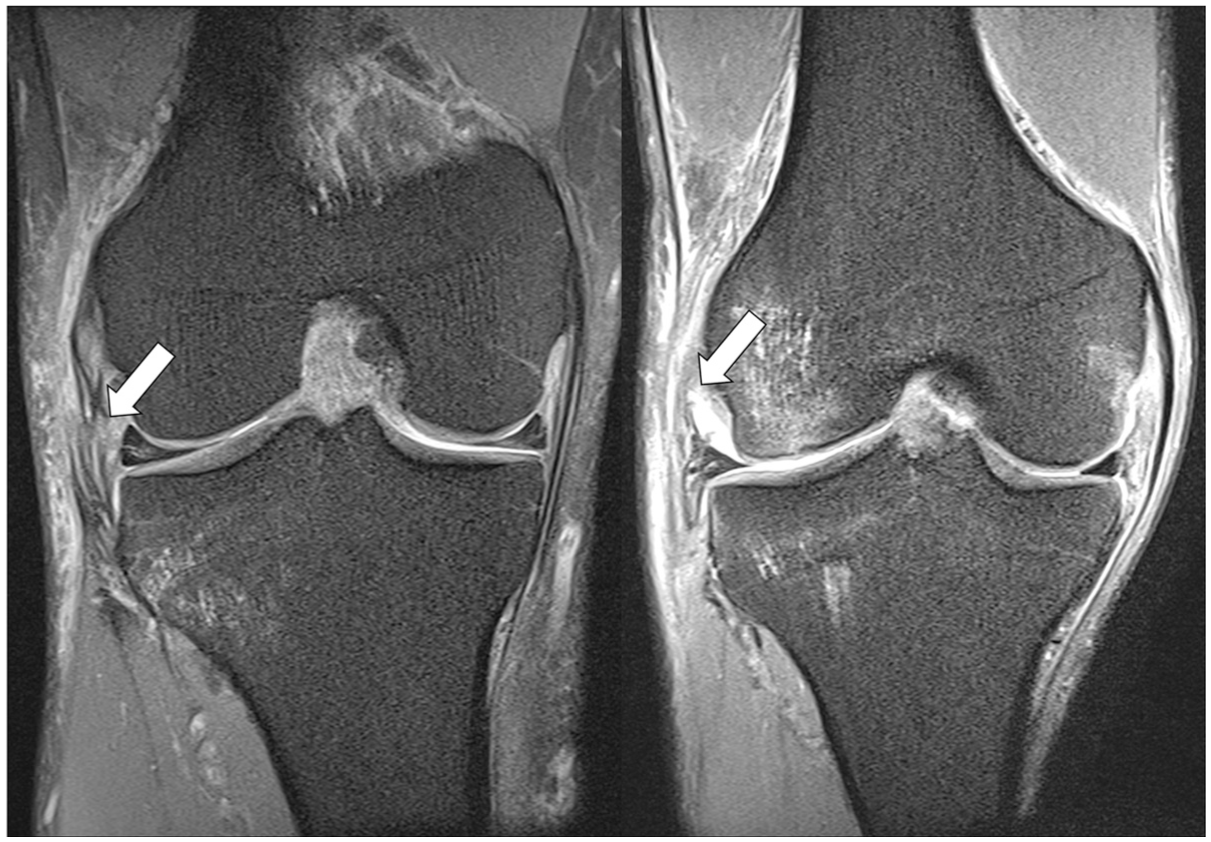
Anterolateral ligament injury (ALL) on coronal view of magnetic resonance imaging (MRI). Complete discontinuous ALL fibers (left panel) and partial rupture (right panel) on the coronal view of the proton density fat–saturating MRI (white arrows).
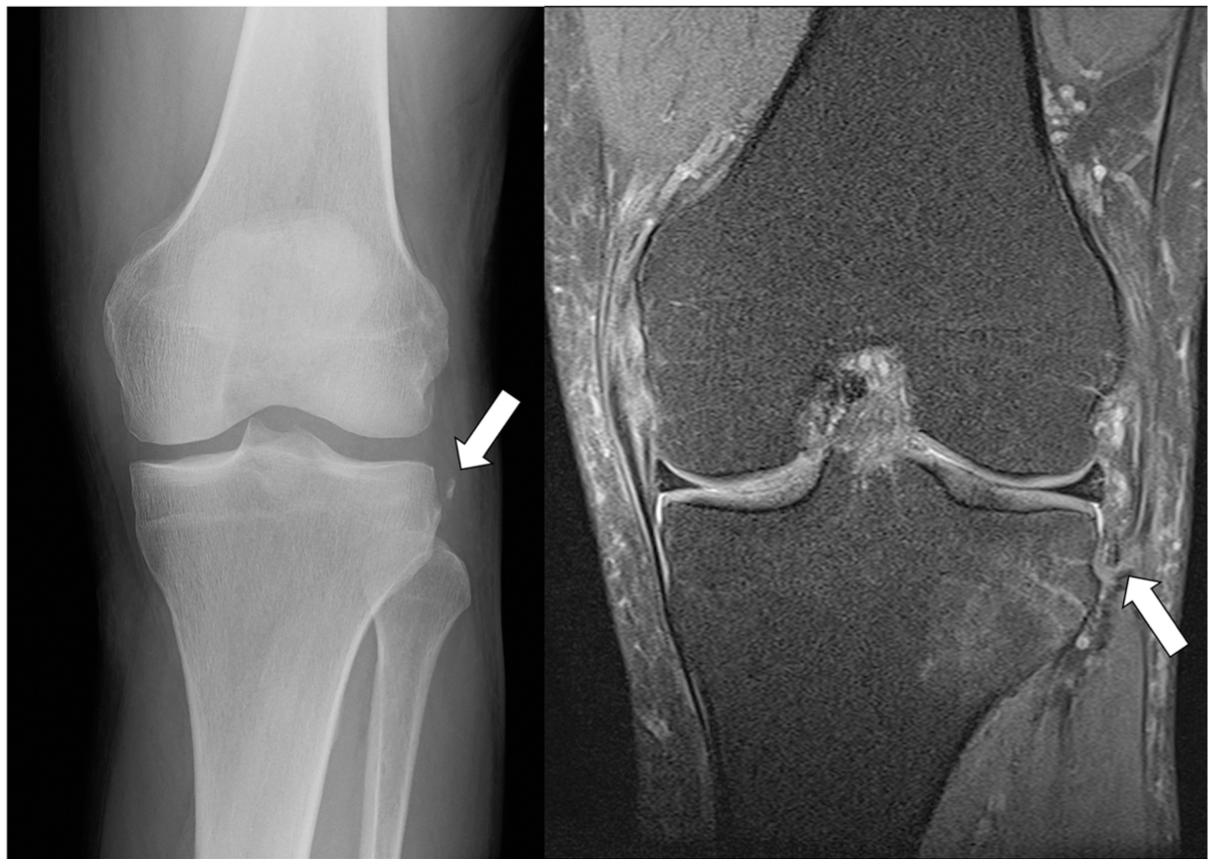
Anterolateral ligament injury in case of Segond fracture. Segond fracture (white arrows) on radiography (left panel) and coronal view on magnetic resonance imaging (right panel).

Irregularities and perligamentous edema of the anterolateral ligament (ALL) on coronal view of magnetic resonance imaging. Irregularity (left panel) and periligamentous edema (right panel) of the ALL injury (white arrows) without visible ALL fibers.

Deep collateral ligament injury on coronal view of magnetic resonance imaging. Meniscofemoral ligament tears (solid white arrow) and complete anterolateral ligament tears (white dotted arrow) observed in the same slice.
The localization of BML has been evaluated using MRI.25,28,33 The BML areas associated with ACL injury were localized on MRI in 4 areas: the MFC, medial tibial plateau, lateral femoral condyle (LFC), and lateral tibial plateau (LTP).
Arthroscopic Confirmation
After enrollment and MRI, all participants underwent ACLR. The ACLR was performed by an arthroscopic surgery team (K.H. and S.N.). During ACLR, the presence of ramp lesions, other medial meniscal (MM) injuries, LMORT, and other lateral meniscus (LM) injuries were confirmed via arthroscopy using a 4 mm–diameter, 45º arthroscope (Stryker) (Figure 5). In ACLR, systematic confirmation, including transnotch view and posteromedial view, was performed in all patients. Thaunat et al 44 classified meniscotibial ligament tears of the ramp lesion as type 3, which was difficult to confirm arthroscopically. In cases where a tear was suspected, a surgeon probed the area with signs of thinning, and the lesion was validated through probing or penetration using a 22-gauge cathelin needle (TERUMO) as previously described 38 and confirmed through the posteromedial view.

Meniscal ramp lesion and lateral meniscus posterior oblique tear (LMORT) via arthroscopy. Meniscal ramp lesion (black arrow) via transnotch view and LMORT (white arrow) from the anterolateral portal on arthroscopy. LFC, lateral femoral condyle; LM, lateral meniscus; LMPH, lateral meniscal posterior horn; LTP, lateral tibial plateau; MFC, medial femoral condyle; MM, medial meniscus.
Measurement of Knee Instability
Before surgery, to evaluate anterior knee laxity, the side-to-side difference (SSD) in anterior tibial translation (ATT) on stress radiographs was measured using a Telos stress device (type SE 2000; Telos Medical) at 20º of knee flexion under an anterior drawer force of 150 N. Rotational knee instability was evaluated intraoperatively on manual pivot-shift test under general anesthesia and graded into 4 categories (0, negative; 1, glide; 2, clunk; and 3, gross shift).
Statistical Analysis
Data are presented as mean ± SD, number (%), or odds ratio (OR) with 95% CI. The Kolmogorov–Smirnov test was used to evaluate data distribution. Mann-Whitney U test was used to compare age, height, weight, body mass index, SSD in ATT, pivot-shift grade, and duration from injury to the MRI between the ALL+ and ALL– groups or dMCL+ and dMCL– groups. The chi-square test was used to determine sex differences and to investigate the association between ALL or dMCL tears and meniscal lesions or BML between groups. Stepwise forward multiple binary logistic regression analyses were used to identify the variables independently associated with ALL or dMCL injury. Statistical significance was set at P < .05. The intra- and interobserver agreements for detecting ALL and dMCL injuries were investigated using a simple kappa coefficient. All statistical analyses were performed using IBM SPSS Statistics for Windows (Version 21.0; IBM Corp).
Results
In total, 66 patients without MRI ≤1 month following ACL injury, 3 without 1.5- or 3-T MRI, 13 who underwent revision ACLR, 2 who had LCL injury that required primary repair or reconstruction, and 3 who had undergone previous operation in their ACL-injured knee were excluded. No concomitant PCL injuries were observed. Finally, 164 patients (79 male and 85 female; mean age, 28.3 ± 11.5 years) were included in this study. The mean duration from injury to MRI was 5.0 ± 6.0 days (range, 1-30; median, 4.0). A flow diagram for participant enrollment is shown in Figure 6.
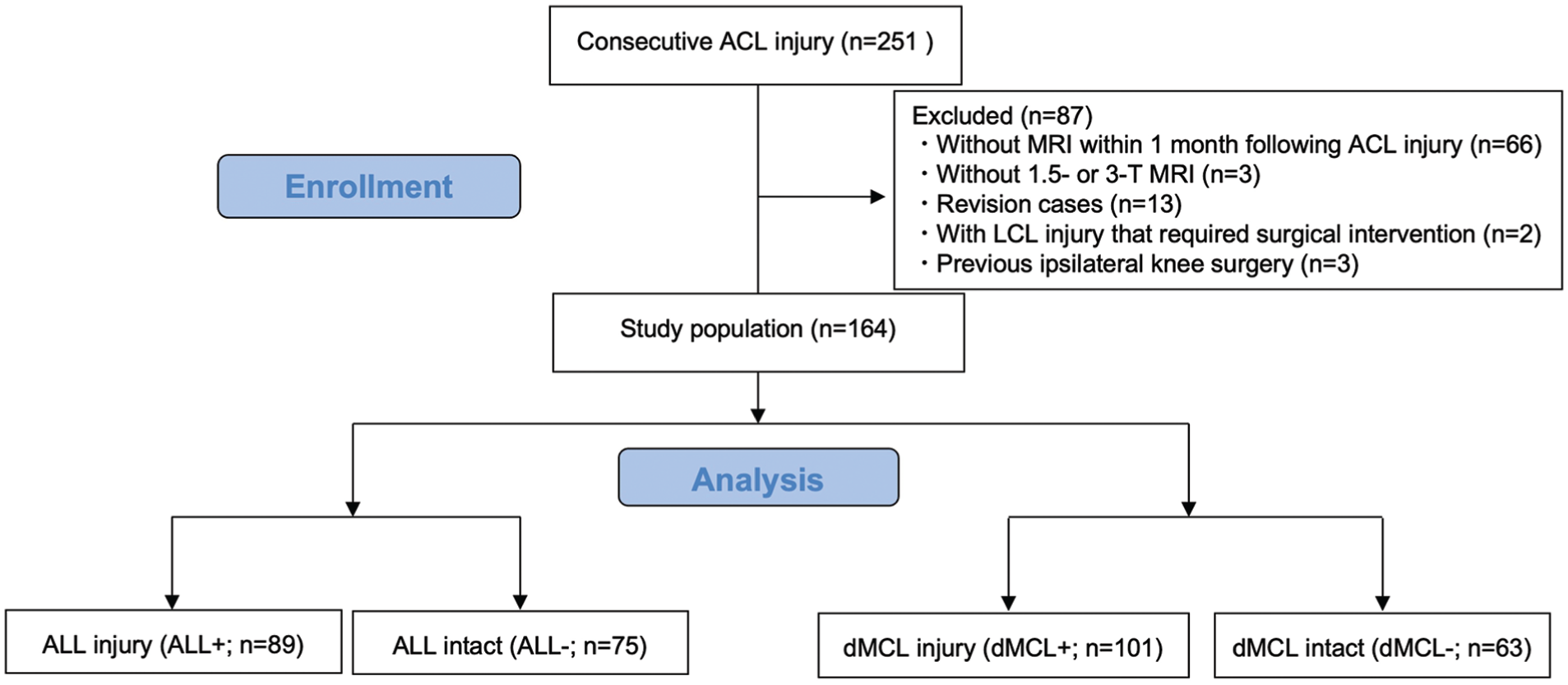
Patient enrollment flow diagram. ACL, anterior cruciate ligament; ALL+/–, anterolateral ligament injury/intact; dMCL+/–, deep medial collateral ligament injury/intact; LCL, lateral collateral ligament; MRI, magnetic resonance imaging.
Prevalence of ALL Injury, dMCL Injury, Ramp Lesion, Other MM Injury, LMORT, Other LM Injury, and BML
Overall, ALL and dMCL injuries were identified after acute ACL injury in 89 (54.3%) and 101 (61.6%) knees, respectively. Both ALL and dMCL injuries occurred in 64 knees (39.0%). The participant characteristics are summarized in Table 1.
Associations of ALL Injury, dMCL Injury, Meniscal Injuries, BML, and Knee Instability
There were significant associations between ALL injury and ramp lesions (P = .001), LM (P = .01), BML in the LFC (P = .007), and BML in the LTP (P = .009), as well as between dMCL and LMORT (P = .01), other LM (P = .03), BML in the LFC (P = .02), and BML in the LTP (P = .001). ALL and dMCL injuries were significantly associated with ramp lesion (P = .007), LMORT (P = .003), other LM (P = .003), BML in the LFC (P = .001), and LTP (P = .003). No significant association was observed between ALL or dMCL injury and SSD in ATT or pivot-shift grade (Table 2).
Associations of ALL Injury, dMCL Injury, Meniscal Injuries, and BML a

Data are presented as mean ± SD or n (%) unless otherwise indicated. Bold indicates a significant difference. ALL, anterolateral ligament; ATT, anterior tibial translation; BML, bone marrow lesion; dMCL, deep layer of medial collateral ligament; LFC, lateral femoral condyle; LM, lateral meniscus; LMORT, lateral meniscus posterior oblique tear; LTP, lateral tibial plateau; MFC, medial femoral condyle; MM, medial meniscus; MRI, magnetic resonance imaging; MTP, medial tibial plateau; SSD, side-to-side difference.
Independent Factors Associated With ALL and dMCL Injury
Stepwise forward binary logistic regression analyses revealed that ramp lesion (OR, 3.70; 95% CI, 1.76-7.78; P = .001), BML in LFC (OR, 2.17; 95% CI, 1.10-4.28; P = .03), and BML in LTP (OR, 2.00; 95% CI, 1.01-3.97; P = .04) were independent factors, increasing the odds, when present, of also having an ALL injury (Table 3). Stepwise forward binary logistic regression analyses also revealed that LMORT (OR, 3.01; 95% CI, 1.06-8.59; P = .04) and BML in LTP (OR, 2.90; 95% CI, 1.49-5.66; P = .002) were independent factors, increasing the odds, when present, of also having an dMCL injury (Table 4). ALL and dMCL injuries were independently associated with ramp lesion (OR, 2.11; 95% CI, 1.02-4.36; P = .045), LMORT (OR, 3.37; 95% CI, 1.09-8.39; P = .009), other LM (OR, 2.30; 95% CI, 1.09-4.85; P = .03), and BML in LFC (OR, 2.55; 95% CI, 1.24-5.23; P < .001) (Table 5).
Stepwise Forward Binary Logistic Regression Analysis for ALL Injury a
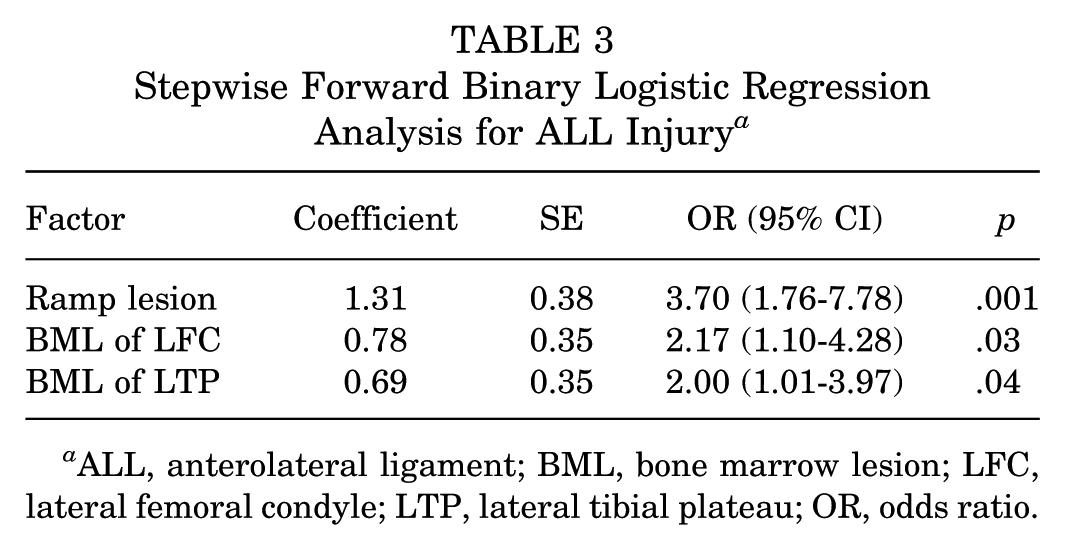
ALL, anterolateral ligament; BML, bone marrow lesion; LFC, lateral femoral condyle; LTP, lateral tibial plateau; OR, odds ratio.
Stepwise Forward Binary Logistic Regression Analysis for dMCL Injury a
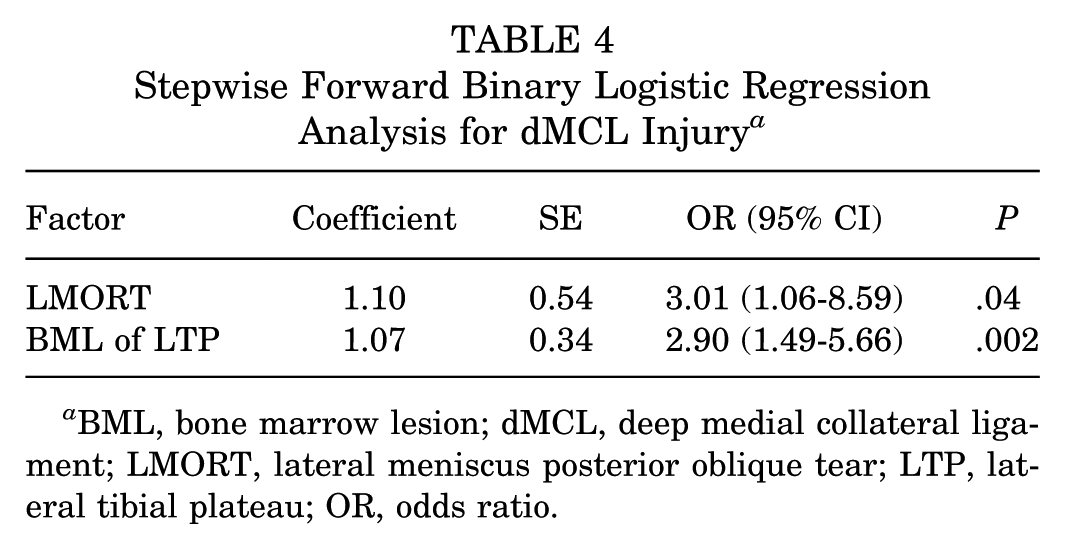
BML, bone marrow lesion; dMCL, deep medial collateral ligament; LMORT, lateral meniscus posterior oblique tear; LTP, lateral tibial plateau; OR, odds ratio.
Stepwise Forward Binary Logistic Regression Analysis for Both ALL and dMCL Injury a
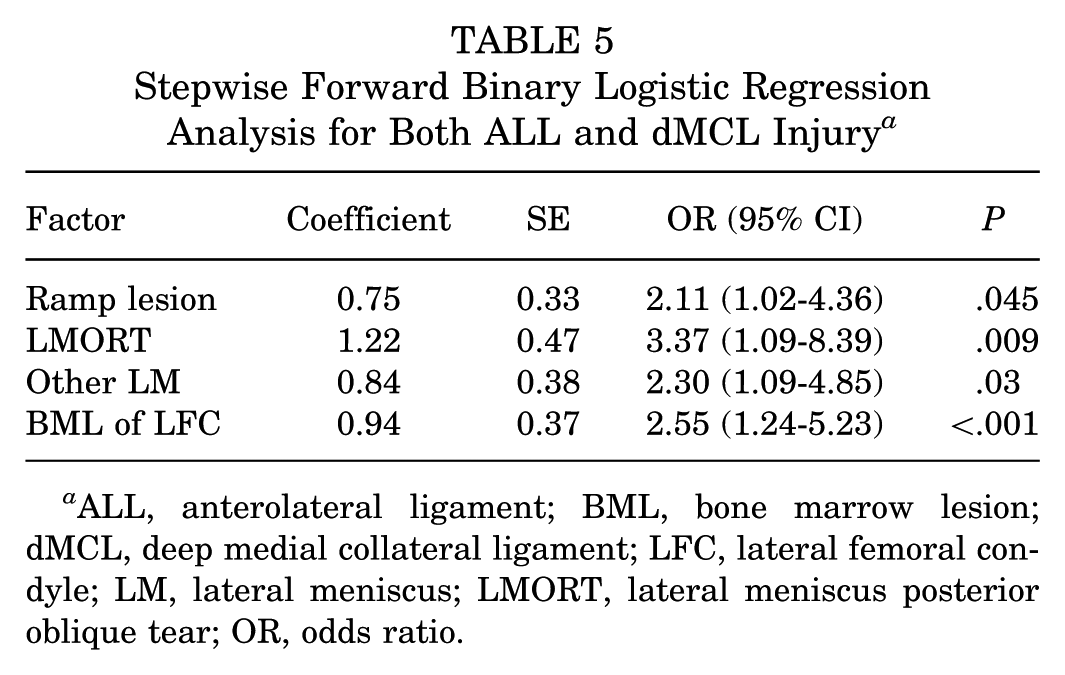
ALL, anterolateral ligament; BML, bone marrow lesion; dMCL, deep medial collateral ligament; LFC, lateral femoral condyle; LM, lateral meniscus; LMORT, lateral meniscus posterior oblique tear; OR, odds ratio.
The intra- and interobserver agreements for detecting ALL injury on MRI between 2 interpreters were good (κ = 0.86 and 0.72, respectively), and those for detecting dMCL were very good (κ = 0.93 and 0.86, respectively).
Discussion
The key finding of the present study was that the overall rates of concomitant ALL and dMCL injury found on MRI in acute ACL injuries were 54.3% and 61.6%, respectively. Moreover, ALL injury was significantly associated with meniscal ramp lesions and LM tears, except for LMORT and BML in the LFC and LTP. dMCL injury was significantly associated with LM tears, including LMORT and BML in the LFC and LTP. The present study also revealed that meniscal ramp lesions, BML in the LFC, and LTP were independent factors that increased the odds of ALL injury, and LMORT and BML in the LTP were independent factors that increased the odds of dMCL injury. Additionally, ramp lesion, LM injury including LMORT, and BML in LTP were independent factors that increased the odds of both ALL and dMCL injury. In contrast, ALL or dMCL injuries observed on MRI in acute ACL injuries were not associated with knee anterior or rotational instability.
The mechanisms underlying ALL, dMCL, and BML occurrence in ACL injuries can be explained using the biomechanical model proposed by Koga et al. 23 Within 40 ms of the ACL injury, valgus stress is applied first. Owing to its weaker shear strength than the sMCL, 47 the dMCL is primarily injured, leading to impaction and BML in the LTP. Subsequently, the tibia undergoes internal rotation; and secondary restraints, including the ALL, may be injured as the ACL ruptures. ALL injuries are associated with exacerbation of the pivot-shift phenomenon. A previous report also showed that BMLs in the LFC and LTP are associated with greater pivot-shift movement following ACL injury. 33
The ALL, together with the superficial and deep layers of the iliotibial band attached to the Kaplan fibers of the distal femur, forms the anterolateral complex, which functions as a secondary ACL stabilizer, providing anterolateral rotational stability.13,36 Hohmann et al 18 reported that the incidence of ALL injuries associated with ACL injuries was 61.7% (45.8%-82.0%). MCL injuries are also frequently associated with ACL injuries. Recently, Cristiani et al 9 reported that dMCL injuries were seen more frequently than sMCL injuries in patients with ACL injuries (16.5% vs 24.8%) and identified MCL injuries as a significant risk factor for concomitant LM injuries (OR, 3.94; 95% CI, 1.73-8.94). In the present study, ALL injuries were observed in 54.3% of cases, whereas dMCL injuries were observed in 61.6%. The prevalence of ALL injuries is consistent with that previously reported, although the rate of dMCL injuries was higher.9,18
This discrepancy may be attributed to the acute-phase nature of our study. We included MRI-diagnosed injuries ≤1 month after the ACL injury before sufficient natural healing process could occur, which explains the high detection rate of dMCL injuries. This contrasts with previous studies, which may have included cases where the healing process had progressed. 9
Distinct meniscal injuries associated with ACL, such as meniscal ramp lesions and LMORT, are well known.11,12,36,40 However, to our knowledge, data on the relationship between ALL or dMCL injuries and meniscal injuries are limited. Stranger et al 42 reported a significant association between ALL injuries and ramp lesions, while Cristiani et al 8 highlighted an independent relationship between MCL and LM injuries. In these studies, meniscal injuries were exclusively diagnosed using MRI. The diagnostic accuracy of MRI is suboptimal for ramp lesions. Although Nonaka et al 30 demonstrated high diagnostic accuracy for ramp lesions using hyperflexed knee MRI, arthroscopic visualization during ACLR remains the gold standard for diagnosing ramp lesions. In our study, preoperative diagnoses of ramp lesion were made using hyperflexed knee MRI, as previously described, 29 with the final diagnoses confirmed via arthroscopy during ACLR. This methodological approach offers advantages over previous studies.
The present study showed that ALL injury increased the prevalence of ramp lesions, and dMCL injury increased the prevalence of LMORT. These findings are consistent with existing reports and may be useful for preoperative detection of concomitant meniscal injuries on MRI before ACLR. Although ramp lesions and LMORT have subclassifications, this study did not have a sufficient number of cases to evaluate these subcategories with adequate statistical power, necessitating further research.
Incorporating lateral extra-articular procedures (LEAPs) into ACLR has been suggested to yield favorable postoperative outcomes. However, the universal application of LEAP in ACL-injured knees remains controversial, and its indications require further assessment. 34 Sonnery-Cottet et al 38 found that patients undergoing combined ACL and ALL reconstruction had significantly lower graft rerupture rates than those who underwent ACLR alone after >2 years of follow-up. Helito et al 16 demonstrated lower failure rates (4.6% vs 14.7%), reduced anterior instability (1.6 mm vs 2.4 mm on KT-1000 testing), and decreased residual pivot-shift tests (37.2% vs 52.2%) in patients undergoing ACLR with LEAP. However, Helito et al 16 reported increased anterolateral pain, whereas Castoldi et al 3 found that performing LEAP in ACL-injured knees with an intact ALL could excessively constrain the lateral compartment, leading to cartilage degeneration. In this study, ramp lesions were found to be independent risk factors for ALL injury and LMORT was an independent risk factor for dMCL injury. Although the ALL and dMCL are not directly visualized arthroscopically, their diagnosis relies on MRI. These findings may aid in diagnosing ALL and dMCL injuries and clarifying the indications for LEAP in ACLR. Conversely, preoperative MRI detection of ALL or dMCL injuries may facilitate the prediction of challenging-to-diagnose ramp lesions or LMORT.
However, in this study, ALL or dMCL injuries detected on MRI did not adversely affect anterior or rotational instability in vivo. Miyaji et al 27 reported that anterolateral capsular injury observed on MRI did not affect rotational instability in ACL-injured knees. Considering that the ACL is the primary restraint contributing to anterior knee instability, the results of the present study suggest that concomitant ALL or dMCL injury did not significantly affect anterior tibial instability. Of note, rotational instability in this study was assessed via a manual qualitative approach. Hoshino et al 19 reported interexaminer variability in grading the pivot-shift test. In future studies, quantitative evaluation of rotational instability is necessary.
Interestingly, BML in the LFC was significantly associated with ALL injury, whereas BML in the LTP was associated with ALL and dMCL injuries. These findings contradict those of Marot et al 25 , who reported no significant association between ALL injuries and BML in the LFC or LTP using ultrasound and MRI. In contrast, Cristiani et al 9 identified BML in the LFC as a risk factor for dMCL injury, while Willinger et al 48 associated BML in the MFC with dMCL injuries, both of which differ from our findings.
Overall, although the present study revealed independent risk factors with statistical associations, it is important to note that ramp lesions do not cause ALL injury, and LMORTs do not cause dMCL injury. These are merely associated pathologies, and the mechanistic relationship of causation remains to be elucidated.
Limitations
This study has several limitations. First, while this study included a consecutive series of ACL-injured patients, only those who underwent MRI within 1 month of injury were included in the analysis, which might have introduced a selection bias. However, this acute-phase focus also served as a strength. Second, using 1.5-T and 3-T MRI scanners might have caused variability in diagnostic performance. Nevertheless, intra- and interobserver reliability assessments were attempted to reduce potential biases. Third, this study included MRI results for the acute phase of the injury. The diagnoses on acute MRI could be false positives, of no clinical significance, and may heal without treatment. Therefore, the ALL tears diagnosed on MRI in the acute phase do not warrant additional treatment such as a LEAP procedure. Fourth, in the ACL-injured knee, a meniscal injury could occur as a result of ligamentous injury or residual laxity. However, our analyses showed that these meniscal injuries were associated with concomitant ligamentous injuries, but it could not be demonstrated that concomitant ligamentous injuries cause meniscal injuries. Fifth, regarding MRI interpretation, arthroscopists participating in ACLR were also involved in reading MRI in this study, that would be a confounder.
Conclusion
In our cohort, the overall rates of concomitant ALL and dMCL injuries in knees with acute ACL injuries were 54.3% and 61.6%, respectively. ALL or dMCL injuries observed on MRI were not associated with greater knee instability. In the acute phase of ACL injury, ALL injury, as detected on MRI, was associated with the presence of meniscal ramp lesions and LM tears except for LMORT and BML in the lateral compartment. dMCL injury was significantly associated with LM tears including LMORT and BML in the lateral compartment. Meniscal ramp lesions and BML in the lateral compartment were independent factors that increased the odds of finding associated ALL injury, and LMORT and BML in the LTP were independent factors that increased the odds of finding associated dMCL injury.
Footnotes
Final revision submitted October 22, 2025; accepted November 30, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Japan Community Healthcare Organization, Gunma Central Hospital (ID No. 2024-035).