
Abstract
Background:
Multiligament knee injuries (MLKIs) are complex and present significant challenges in achieving optimal long-term outcomes. This systematic review aims to evaluate clinical and functional results, complications, and return-to-sport rates following MLKIs, with a minimum 7-year postoperative follow-up.
Purpose:
To report the long-term clinical and functional outcomes after MLKIs at a minimum 7-year follow-up.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A comprehensive literature search was performed in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, identifying 16 studies encompassing 730 knees. Extracted data included patient-reported outcomes, return-to-sport rates, osteoarthritis development, complications, reoperations, and revision procedures. Due to study heterogeneity, a qualitative analysis was conducted.
Results:
Postoperative patient-reported outcomes demonstrated considerable variability, with mean scores generally modest at long-term follow-up (reported in 13 studies). Return-to-sport rates, available from 8 studies, ranged from 60.4% to 85%. Osteoarthritis progression was reported in 7 studies, with the proportion of patients exhibiting Kellgren-Lawrence grades 3 or 4 at final follow-up ranging from 12% to 71.7%. Reoperation rates were reported in 7 studies and ranged from 1.7% to 34.3%, most commonly for manipulation under anesthesia and lysis of adhesions due to postoperative stiffness. Conversion to total knee arthroplasty was reported in 6 studies, with rates ranging from 0% to 10.9%. Repeat ligamentous surgery varied across 7 studies, with posterior cruciate ligament reconstruction failures most frequently reported.
Conclusion:
Outcomes >7 years after treatment of MLKIs demonstrate meaningful restoration of function and sport participation but remain tempered by significant rates of osteoarthritis and reoperation for stiffness. Advances in surgical technique and early rehabilitation have improved results in contemporary cohorts. Continued prospective evaluation using standardized protocols is essential to enhance joint preservation and patient quality of life.
Registration:
PROSPERO (CRD 420251078013).
Multiligament knee injuries (MLKIs) represent a challenging clinical entity with potentially devastating consequences for affected patients, despite their relatively low incidence. 28 MLKIs are defined as injuries involving ≥2 of the 4 principal knee ligaments. 25 The mechanisms underlying MLKIs are diverse, typically categorized as either low-velocity trauma (eg, sports injuries, falls) or high-velocity trauma (eg, motor vehicle accidents), and may occur with or without concurrent knee dislocation. 6 The presence of a knee dislocation increases the risk of neurovascular compromise, which can further worsen clinical and functional outcomes. 37
Management strategies for MLKIs remain heterogeneous, with ongoing debate regarding optimal preoperative stabilization, surgical techniques, timing of intervention, and postoperative rehabilitation protocols. 29 The lack of consensus in the literature underscores the need for a deeper understanding of how MLKIs affect long-term functional and clinical outcomes. Such insights are essential to inform evidence-based management and improve patient prognosis.
Previous systematic reviews have primarily focused on aspects such as return to sport, surgical timing, injury mechanisms, and comparisons between repair and reconstruction of ligaments.6,15,24,32,40 There is a paucity of data specifically addressing long-term patient-reported outcomes (PROs) following MLKI. The purpose of this systematic review was to report the clinical and functional outcomes after MLKIs at a minimum 7-year follow-up. We hypothesize that most postoperative International Knee Documentation Committee (IKDC) and Lysholm scores reported at a minimum 7-year follow-up will meet or exceed published Patient Acceptable Symptom State (PASS) thresholds reported for MLKI surgery.
Methods
Literature Search Methodology
A comprehensive search of PubMed, Embase, and Scopus Library databases was performed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines in July 2025 and was prospectively registered with PROSPERO (registration number: CRD420251078013). The following search strategy was used: (“Knee Dislocation” OR “knee dislocation” OR “knee instability”) AND (“Ligaments, Articular/surgery” OR “multiligament” OR “multi-ligament” OR “multiple ligament” OR “ligament injury”) AND (“treatment Outcome” OR “outcomes” OR “functional outcome” OR “return to sport” OR “clinical outcome” OR “complications”). The search was performed by 2 authors (L.D.M. and J.T.M.).
Inclusion criteria were studies involving male and female patients of any age group who had an MLKI and/or a knee dislocation with clinical and/or functional outcome data at ≥7 years postoperatively, published between 2000 and 2025. Exclusion criteria were studies that were cadaveric or translational, did not report PROs, reported outcomes at <7 years postoperatively, or had study designs that were systematic reviews, narrative reviews, conference abstracts, technical notes, letters to editors, or meta-analyses. Also, studies with overlapping cohorts based on the reported years of data collection by the same authors were excluded due to the risk of bias inherent in using overlapping cohorts for data extraction purposes. However, if it met the other inclusion criteria, the most recently published study from the author group with the largest sample size was included. Two authors (L.D.M. and J.T.M.) independently screened titles, abstracts, and full article texts using the online software program Covidence (Veritas Health Innovation Ltd). Any disagreements were resolved with discussion, leading to consensus between 2 authors (L.D.M. and N.T.).
Data Extraction and Quality Assessment
Data items extracted from each study included demographic information such as age, mean follow-up time, ligaments involved in injury, Schenck classification for knee dislocations, 13 the presence of a vascular injury or a nerve injury, the mean time from injury to surgery, surgical staging and technique(s) implemented, primary or revision surgery status, and postoperative PROs, including the IKDC score, Tegner Activity Scale score, Lysholm knee score, and revisions, reoperations, complications, and conversions. Data on osteoarthritis (OA) development based on radiographic evidence of OA or Kellgren-Lawrence grades were collected, as well as return-to-sport data. Functional outcomes were recorded, including range of motion (ROM), Lachman assessment, KT-1000, valgus/varus laxity noted on clinical examination, and pivot shift. Assessment of data quality for each of the nonrandomized prospective and retrospective studies included in this systematic review was performed with the Methodological Index for Non-Randomized Studies (MINORS) criteria. 38
Statistical Analysis
Pooling of data was avoided due to a high risk of bias inherent in retrospective studies and heterogeneity among included studies. A qualitative data comparison was conducted. For studies only reporting ranges, the standard deviation was approximated as the range divided by 4. Eligible studies were entered into Open Meta Analyst (Brown University) to create single-leg forest plots illustrating mean postoperative PROs. These forest plots served as visual aids to summarize these means.
Results
Of the 2023 studies identified in the initial search, 1031 were duplicates and subsequently excluded. Of the remaining 992 studies that underwent title and abstract screening, 927 were found to be irrelevant to the study aims and therefore excluded. The remaining 65 studies were assessed for eligibility with full-text review. After excluding 48 studies for having the wrong follow-up duration, study design, outcomes, intervention, an overlapping cohort, or no full text available, 16 studies* were ultimately included for data extraction (Figure 1). Each study included in this systematic review evaluated clinical outcomes after MLKIs and/or knee dislocation with a minimum 7-year postoperative follow-up.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) study selection flow diagram. The numbers of screened, excluded, and included studies are shown.
Table 1 summarizes study quality based on the MINORS criteria for nonrandomized studies. The ideal MINORS score for noncomparative studies is 16, with scores ≤8 being the accepted cutoff for poor study quality. Each of the included studies had a score ≥9, indicating a sufficiently low risk of bias. 38 The ideal MINORS score for comparative studies is 24, with scores ≥18 being the accepted cutoff for high study quality, ≥12 to <18 for moderate study quality, and <12 for poor study quality. Of note, no study received points for prospective calculation of data, unbiased assessment of study endpoints, or prospective calculation of study size. Overall, the risk of bias was low for the included studies in this systematic review.
Summary of Study Quality and Risk-of-Bias Assessment a

Each included study was scored as moderate or high quality based on the MINORS criteria. LOE, level of evidence; MINORS, Methodological Index for Non-Randomized Studies.
Demographic Characteristics
Six of the included studies4,17,18,27,35,36 were retrospective comparative studies, while the 10 other studies † were retrospective case series.
Across all the included studies, there were a total of 730 knees. The mean age reported ranged from 18.1 to 44.0 years, and the mean follow-up time ranged from 7.0 to 13.1 years. A summary of demographic characteristics for each study included in this systematic review is included in Table 2.
Summary of Demographic Characteristics of Included Studies and Patient Cohorts a

NR, not reported.
Injury Details
The number and type of ligaments injured varied across the included studies. The overall percentage of KD1s across the included studies was 8.4% (61 of 730 knees). Twelve studies ‡ reported data on knee dislocations, with incidence ranging from 55.2% to 100%. Twelve studies § reported data on vascular injuries, and 13 studies ‖ reported on nerve injuries, with incidence ranges of 0% to 37.5% and 0% to 45.0%, respectively. The peroneal nerve was the most commonly injured nerve. Table 3 summarizes the knee injuries reported by the included studies.
Summary of Knee Injuries a

ACL, anterior cruciate ligament; KD, Schenck's knee dislocation grade; LCL, lateral collateral ligament; MCL, medial collateral ligament; NR, not reported; PCL, posterior cruciate ligament; PLC, posterior lateral corner; PMC, posterior medial corner.
Surgical Techniques
Ten studies2-5,9,11,14,17,26,27 reported data on staging of the surgical procedures used; however, 1 study 2 reported specifics of the staging procedures implemented. Combinations of varying ligamentous repair and reconstruction techniques were reported by the included studies. In general, most studies performed ligament reconstruction with allograft or autograft for the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL), with 9 studies2,4,5,9,11,17,26,27,30 using arthroscopy, 1 study 14 using an open approach, and the other studies3,18,34-36,43 not indicating their approach. Surgical management of injuries to the lateral collateral ligament, medial collateral ligament, posterior medial corner, and posterior lateral corner differed. A summary of the surgical techniques and staging used is included in Table 4.
Summary of Surgical Techniques a

ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; BTB, bone-tendon-bone; LARS, ligament augmentation and reconstruction system; LCL, lateral collateral ligament; LCLR, lateral collateral ligament reconstruction; MCL, medial collateral ligament; MCLR, medial collateral ligament reconstruction; NR, not recorded; PCL, posterior cruciate ligament; PCLR, posterior cruciate ligament reconstruction; PLC, posterior lateral corner; PLCR, posterior lateral corner reconstruction; PMC, posterior medial corner; PMCR, posterior medial corner reconstruction.
Postoperative Rehabilitation
Twelve studies ¶ included in this review reported postoperative rehabilitation plans. The plans implemented varied greatly regarding brace utilization, weightbearing status, initiation of range of motion (ROM), and return-to-sport timeline. A summary of the postoperative rehabilitation plans reported is included in Table 5.
Summary of Postoperative Rehabilitation Plans a

ACL, anterior cruciate ligament; LCL, lateral collateral ligament; PCL, posterior cruciate ligament; PLC, posterior lateral corner; PO, postoperative; PWB, partial weight bearing; ROM, range of motion; NR, not reported.
Clinical Outcomes
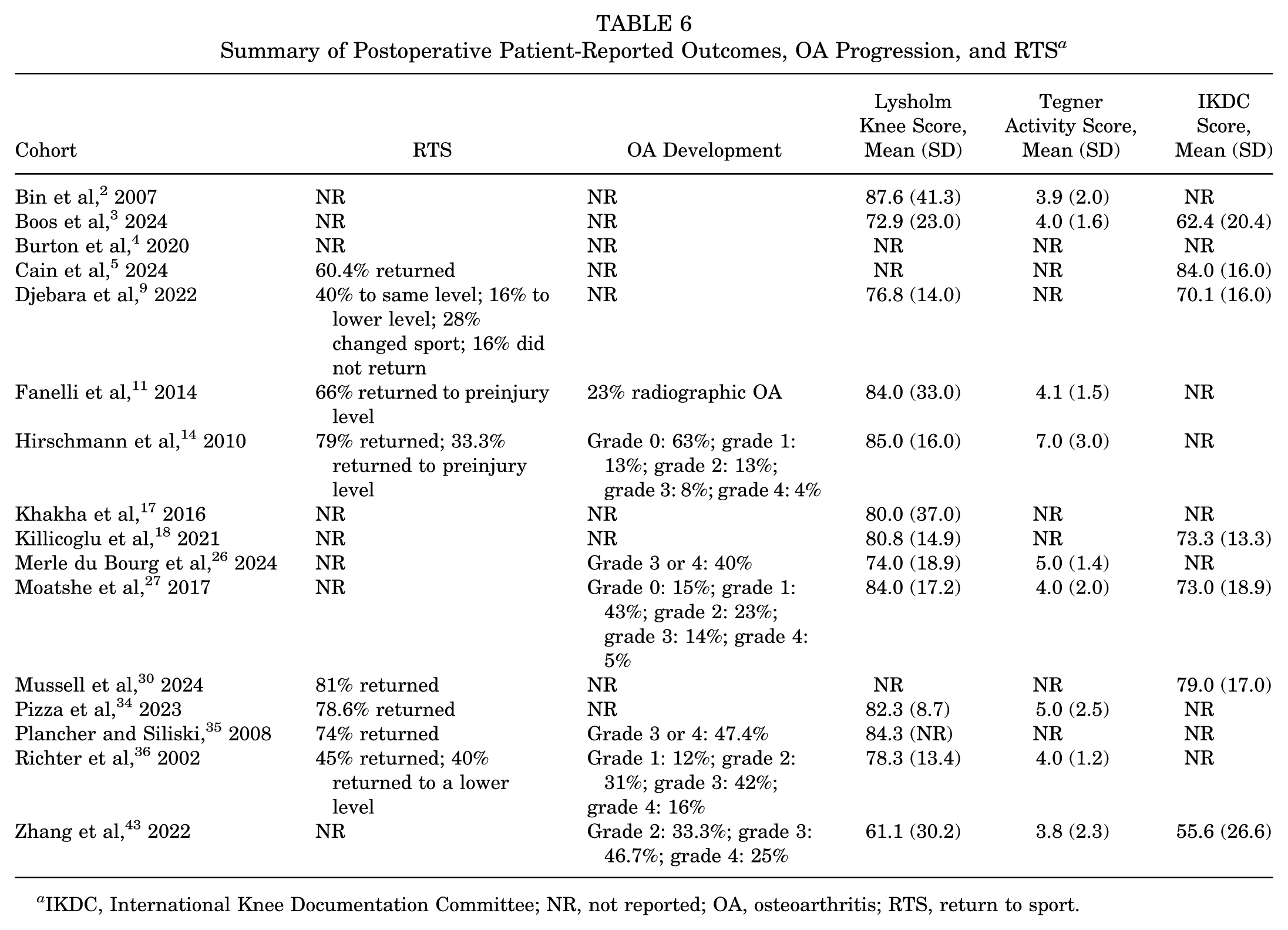
Due to the acuity of most MLKIs, preoperative PROs were not reported. Thirteen studies # reported postoperative Lysholm knee scores at final follow-up, with mean values ranging from 61.1 to 87.6. Nine studies** reported postoperative Tegner Activity Scale scores, with mean values ranging from 3.8 to 7.0 at final follow-up. Seven studies3,5,9,18,27,30,43 reported postoperative IKDC scores, with mean values ranging from 55.6 to 84.0 at final follow-up.
Eight studies5,9,11,14,30,34-36 reported data on return-to-sport (RTS) outcomes, with ranges from 60.4% to 85% of patients returning to sport. Regarding the level that patients were able to return to sport, Djebara et al 9 reported that 40% returned to the preinjury level and 16% returned to a lower level. Fanelli 10 reported that 66% of patients returned to the preinjury level, Hirschmann et al 14 indicated that 33.3% of patients returned to the preinjury level, and Richter et al 36 reported that 45% returned to the preinjury level and 40% returned to a lower level. Table 6 summarizes the mean postoperative PROs and RTS data for the included studies. Figure 2 displays a forest plot illustrating mean postoperative Lysholm, Tegner, and IKDC scores for the included studies.
Summary of Postoperative Patient-Reported Outcomes, OA Progression, and RTS a
IKDC, International Knee Documentation Committee; NR, not reported; OA, osteoarthritis; RTS, return to sport.

Forest plot showing mean postoperative International Knee Documentation Committee (IKDC), Lysholm, and Tegner scores. Black dots represent the mean value of each study, with lines extending to the 95% confidence intervals.
OA Development
OA progression, as evidenced by radiographic follow-up or Kellgren-Lawrence (KL) scale grades, was reported by 7 studies.11,14,26,27,35,36,43 Fanelli et al 11 reported that 23% of patients showed radiographic evidence of OA progression at final follow-up of 10 years. The 6 other studies reported OA development through the KL scale grading system at final follow-up. Table 6 summarizes the postoperative OA progression at final follow-up.
Functional Outcomes
ROM data were reported by 10 studies, †† although there is heterogeneity in the way these data were presented. Some reported mean active flexion and extension, others described extension or flexion deficits in comparison to the contralateral limb, and some indicated the percentage of patients who regained full ROM or exhibited a ROM deficit. Lachman test data at final follow-up were reported by 5 studies11,14,26,27,35 with an abnormal Lachman test, as evidenced by the presence of an asymmetric examination relative to the contralateral limb, no firm endpoint noted with examination, or a 2+ and 3+ rating ranging from 4% to 54.3% of patients. Data on pivot-shift examination at final follow-up were reported by 6 studies,9,11,14,26,27,43 with a positive test incidence ranging from 9% to 25%. Varus and valgus laxity at final follow-up was reported by 4 studies,11,26,27,35 with the incidence of varus and valgus laxity ranging from 2.8% to 26% and 2% to 43%, respectively. Posterior drawer test data at final follow-up were reported by 3 studies,11,27,35 with the incidence of a positive test ranging from 2% to 41%. KT-1000 data were reported by 4 studies.11,14,26,35 Table 7 summarizes the functional outcomes for the included studies.
Summary of Postoperative ROM and Stability Tests a

NR, not reported; ROM, range of motion.
Complications, Reoperations, Conversions, and Revisions
Complications, defined as an adverse event that did not result in needing another surgical procedure, were reported by 3 studies,2,35,43 with overall incidence rates ranging from 0% to 17.5% and permanent nerve palsy as the most commonly cited complication.
Reoperations, defined as an additional surgical procedure after the index procedure that was not a revision or conversion to total knee arthroplasty (TKA) surgery, were reported by 7 studies.2,3,5,9,14,26,30 Overall reoperation rates ranged from 1.7% to 34.3%, with manipulation under anesthesia (MUA) and lysis of adhesions (LOA) for postoperative stiffness being the most reported and the highest-incidence reoperation from the included studies (range, 1.8%-34.3%). Hardware removal and meniscus surgery were the next most common reoperations.
Conversion to TKA data was reported by 6 studies.2,9,11,14,30,36 Radiographic OA progression remained a dominant finding, with 40% to 72% of knees demonstrating KL ≥3 at ≥7 years. Conversion to TKA, although relatively infrequent (0%-10.9%), represents the end stage of this degenerative continuum. Boos et al 3 reported that the mean time to conversion was 12.0 ± 4.9 years. The 2 TKAs reported by Richter et al 36 occurred at 5 and 10 years postoperatively.
Failures, defined as a repeat ligamentous surgery after the index procedure or radiologic evidence of a retorn ligament, were reported by 7 studies.2,3,5,9,26,30,34 Overall revision rates ranged from 0% to 31.4%. The revision procedure with the greatest incidence was PCL reconstruction (PCLR). Four of the 7 studies3,5,26,30 reported an incidence of revision ACL reconstructions ranging from 0% to 22.9%, and 3 of the 7 studies26,30,34 reported revision PCLRs with an incidence range of 0% to 28.0%. No revision procedures for other ligaments were reported by the included studies. Table 8 summarizes the complications, reoperations, conversions, and revisions for the included studies.
Summary of Adverse Events a

ACLR, anterior cruciate ligament reconstruction; ALL, anterolateral ligament; DVT, deep venous thrombosis; LOA, lysis of adhesions; MUA, manipulation under anesthesia; NR, not reported; PCLR, posterior cruciate ligament reconstruction; PMCR, posterior medial corner reconstruction; TKA, total knee arthroplasty.
Stratified Trend Analysis
To address the heterogeneity among included studies, a qualitative stratified analysis was conducted based on study era, surgical timing, repair versus reconstruction, and postoperative rehabilitation approach (Table 9). When studies were grouped by era, early-series cohorts2,14,35,36 (2000-2014) typically utilized nonanatomic or single-bundle reconstructions with prolonged immobilization, whereas modern-series cohorts ‡‡ (2015-2025) more frequently employed anatomic techniques and early controlled motion. Modern-era studies demonstrated higher mean IKDC and Lysholm scores and lower rates of stiffness-related reoperations, although OA progression remained common. Regarding surgical timing, patients managed acutely4,5,14,17,26,27,35,36 (≤21 days from injury) achieved better long-term functional outcomes and less postoperative stiffness compared with delayed (>21 days) reconstructions. Reconstruction-based techniques generally yielded superior stability and lower failure rates than primary repairs. Finally, cohorts that implemented early ROM protocols5,9,14,17,30,36 showed improved postoperative flexion and reduced need for MUA or LOA, without compromising long-term stability.
Stratified Summary of Key Subgroup Trends in Long-Term Multiligament Knee Injury Outcomes a

IKDC, International Knee Documentation Committee; KL, Kellgren-Lawrence; LOA, lysis of adhesions; MUA, manipulation under anesthesia; OA, osteoarthritis; PRO, patient-reported outcome; ROM, range of motion; TKA, total knee arthroplasty.
Discussion
This systematic review of long-term outcomes following MLKIs revealed several key findings. First, while PROs varied, many studies reported modest postoperative Lysholm and IKDC scores, indicating acceptable clinical results in many patients. Second, RTS rates remained relatively high, ranging from 60.4% to 85%, although data on return to preinjury levels were limited. Third, there was a substantial incidence of OA at final follow-up, with KL grade 3 or 4 reported in up to 71.7% of patients. Finally, reoperations for stiffness were common, and PCLRs had the highest revision rates. Collectively, these findings suggest that although surgical management of MLKIs offers generally favorable long-term functional outcomes and RTS potential, high rates of OA and reoperations highlight the need for optimized surgical techniques and rehabilitation protocols. Our hypothesis that most postoperative IKDC and Lysholm scores at long-term follow-up would meet or exceed published PASS thresholds for MLKI surgery is supported, as over 60% of studies reporting these outcomes achieved the established benchmarks, as reported in the subsequent paragraph. However, it is noteworthy that approximately 40% of studies reported mean Lysholm and IKDC scores below the established PASS thresholds, underscoring that satisfactory symptom resolution and function are not universally achieved despite surgical management. This finding emphasizes the need for continued refinement in surgical techniques, patient selection, and rehabilitation strategies to improve long-term outcomes after MLKI reconstruction. Of note, the inclusion of KD1 (low-velocity, partial multiligament) injuries in several cohorts did not appear to confer superior long-term outcomes.
The PRO data from this review showed varying scores overall. The PASS for multiligament knee reconstruction, with a mean follow-up of 4.8 years for the IKDC and Lysholm knee score, has been calculated as 67.9 and 80.0, respectively. 12 Accordingly, 8 studies2,11,14,17,18,27,34,35 of the 13 (61.2%) that reported Lysholm scores achieved the PASS score, and 5 studies5,9,18,27,30 of the 8 (62.5%) achieved the PASS score for the IKDC questionnaire. Two studies3,43 reported mean IKDC and Lysholm scores substantially lower than those of the other studies included. Boos et al 3 reported that surgery was performed in a single stage at a mean of 275 days after the MLKI, which is considered a delayed surgical time (>3 weeks). 23 A recent systematic review found that delayed surgical reconstruction of MLKIs results in significant differences in PROs compared to acute surgical management. 19 Moreover, Boos et al 3 performed a subset analysis comparing outcomes based on age and reported that patients >30 years old had significantly lower Tegner scores compared to patients younger than 30 years. Zhang et al 43 reported the lowest overall mean Lysholm and IKDC (61.1 and 55.6, respectively) scores, the poorest mean active flexion ROM (106°), and 71.7% of patients with a KL grade of 3 or 4 at final follow-up. Within the cohort, 9 of the patients (45%) were treated nonoperatively and comparatively had lower PRO scores for every questionnaire than the operatively treated group, although only the Tegner Activity Scale scores were significantly different. Although a definitive reason for the low PROs was not specifically reported by Zhang et al, 43 there is strong evidence to support surgical management of MLKIs due to significant differences in PROs and ROM reported in the literature, although the decision for surgical management remains dependent on various factors.22,33,42 A 2024 systematic review and meta-analysis of 79 studies assessing yearly changes in PROs after MLKIs reported that the average decrease in Lysholm and IKDC scores from 2 years to 5 years was 0.8 and 1.99 points, respectively. 20 With respective mean scores of 86.1 and 81.4 for the Lysholm and IKDC scores reported in the 2024 review, the generally lower PRO results at a longer follow-up period in our review generally support worsening clinical outcomes over time after MLKIs. This decline in PROs over time is likely multifactorial, but progressive posttraumatic osteoarthritis, residual ligamentous laxity, and persistent stiffness are plausible contributors that have been consistently reported in long-term follow-up studies.
RTS rates were generally high (60.4%-85%) in this systematic review. Cain et al 5 reported the lowest RTS rate (60.4%), although they included 11 patients who did not RTS because they graduated and were not talented enough for the next level, rather than due to surgical limitations. A systematic review of 9 studies reporting RTS data after MLKIs calculated a 77.9% mean RTS rate, which is similar in general to the reported RTS rates in this review, although the ability for patients to continue sports participation at long-term follow-up was not reported by the included studies. 6
Multiligament knee injuries have been associated with high rates of OA development in the literature, although long-term studies are limited.27,39 In this review, the rate of KL grades 3 and 4 at final follow-up ranged from 12% to 71.7%.14,26,35,36,43 Hirschmann et al 14 reported that 63% of patients had KL grade 0 at final follow-up, although the patient cohort had the lowest mean age (24.0 years) and primarily included soccer players with MLKIs. Shorter-term follow-up studies have demonstrated a wide range of progression to knee OA; Jacobs et al 16 reported that 9.0% of patients developed OA 5 years after MLKI. In contrast, Sobrado et al 39 reported an OA rate (defined by KL ≥2) of 64.5% within 5 years. Additionally, data have shown that low-velocity (eg, sports, falls) MLKIs result in superior PROs compared to high-velocity (eg, motor vehicle accidents) injuries. Moreover, previous systematic reviews have reported that higher Schenck classification grades are associated with poorer functional outcomes, reflecting the influence of injury complexity on prognosis. 8
The relatively shorter mean follow-up time reported by Hirschmann et al 14 (mean 8.0 years), younger mean age, and low-velocity injuries could contribute to the high incidence of KL grade 0 scores reported. This review highlights the substantial risk of OA development after MLKIs at long-term follow-up, a factor that likely contributes to the suboptimal clinical outcomes observed over time. Younger patients and those who underwent reconstruction in earlier surgical eras demonstrated delayed but ultimately inevitable degenerative progression. These findings underscore the importance of joint-preserving strategies, including precise alignment correction, anatomic graft placement, and contemporary rehabilitation protocols, to reduce the risk of posttraumatic OA.
Finally, reoperation rates were high in this systematic review, with MUA and LOA due to postoperative stiffness having the greatest incidence overall. Early surgical treatment, ≥3 injured ligaments, and knee dislocations, especially with vascular injuries, have been cited as risk factors for postoperative stiffness.1,32,41 Merle du Bourg et al 26 reported the highest rate of MUA and LOA reoperations (34.3%) in the review. They noted a significant difference in rates of MUA and LOA in patients who underwent surgery acutely (<3 weeks) and delayed (>3 weeks) (P = .007), with 91.7% (11 of 12) of MUA and LOA reoperations performed in the acutely treated cohort. The high risk of postoperative stiffness is further underscored by the poor ROM data reported by the studies in this review. Conversion rates to TKA varied, with Boos et al 3 reporting the highest rate (10.9%) overall. The cohort in our review was relatively young (mean age ≤44 years at the time of surgery), which may have influenced the timing and clinical decision-making regarding conversion to TKA. However, the high prevalence of advanced osteoarthritic changes observed at final follow-up suggests that many of these patients are likely to require TKA in the future. Reinjury to the PCL was the most reported reason for failure after the index procedure. Merle du Bourg et al 26 reported the highest rate of PCL failure (28.0%) through magnetic resonance imaging evidence of a complete ligament augmentation and reconstruction system tear, but the authors did not address clinical symptoms or revision surgery for these patients. Pizza et al 34 reported the second-highest PCLR failure rate (14.2%), but they did not explicitly state the surgical technique used to reconstruct the PCL. The high rates of PCLR failure could be due to the utilization of nonanatomic and single-bundle PCLR techniques popular in the early 2000s, which have been shown to be biomechanically inferior to modern methods of reconstruction (eg, double-bundle, anatomic).7,21 Most studies included in this review collected data on patients from the early 2000s. Therefore, the heterogeneity of surgical techniques reported across long data collection periods must be contextualized within the limitations of this study when assessing complication rates. Nonetheless, postoperative stiffness and OA development contribute significantly to the adverse events after MLKIs.
Considerable heterogeneity exists across included studies regarding injury severity, surgical staging, graft source, and postoperative rehabilitation. Rather than pooling these disparate data, we qualitatively synthesized outcomes to identify consistent trends. The variability itself reflects real-world clinical complexity and evolving practice patterns. Future multicenter prospective investigations with standardized operative algorithms, rehabilitation milestones, and uniform reporting of OA and reoperation endpoints are essential to generate generalizable long-term evidence.
The 25-year span of included studies reflects substantial evolution in MLKI management. Early-era reports (2000-2014) frequently used nonanatomic, single-bundle cruciate reconstructions and prolonged immobilization, contributing to lower functional scores and higher rates of arthrofibrosis. 31 In contrast, modern-era series (2015-2025) increasingly employed anatomic graft placement, early controlled motion, and structured rehabilitation, yielding higher IKDC and Lysholm means and fewer conversions to TKA. 29 This temporal stratification underscores that improved understanding of biomechanics and early mobilization protocols likely drive superior long-term function in recent cohorts.
The findings of this systematic review must be interpreted with regard to the recently published Delphi consensus, which outlines expert-driven recommendations for future MLKI research. 29 Many of the studies included in our review predate these recommendations and exhibit limitations that the Delphi group explicitly identified, such as inconsistent injury classification, heterogeneous surgical techniques (eg, repair of the ACL and PCL), nonstandardized reporting of clinical outcomes, and variable postoperative rehabilitation plans (eg, weightbearing status, ROM initiation). 29 Additionally, only 4 studies9,11,14,36 (25.0%) reported RTS stratified by level or intensity, and the use of objective stability testing was rare. Furthermore, complications and reoperations were inconsistently defined or omitted entirely. A particularly important omission was the use of stress radiographs since the Delphi group strongly recommended obtaining them to assess ligamentous laxity, especially for quantifying posterior tibial translation in PCL injuries. 29 Only 6 studies2,9,11,14,17,27 (37.5%) in this review reported the use stress radiographs prior to surgical management. This lack of standardized imaging makes it difficult to interpret the true extent of ligamentous instability and assess surgical prognosis. Moreover, while the Delphi consensus highlights the importance of objective assessments such as KT-1000 or KT-2000 arthrometry to quantify residual laxity, only 4 studies11,14,26,35 (25.0%) in our review mentioned using these tools. 29 As a result, most included studies relied primarily on subjective measures to evaluate surgical success. This approach likely underestimates the true extent of postoperative laxity, especially in complex ligament reconstructions, where subtle instability may persist despite satisfactory subjective outcomes. Finally, the Delphi consensus on surgical staging and time to surgery (eg, 1-stage and surgical management <21 days after injury when possible) further highlights areas for improvement for the studies included in this review. 29 Going forward, adherence to the Delphi guidelines, including standardized reporting of clinical and functional outcomes, surgical technique, concomitant injuries, time to surgery, postoperative rehabilitation plans, and objective imaging usage, will be critical for generating higher-quality, generalizable data. 29 Our review reinforces the need for prospective, multicenter studies that align with these expert recommendations to improve the evidence base for long-term MLKI management and outcomes.
Limitations
This systematic review is not without limitations. There was substantial heterogeneity in injury severity, concomitant injuries, method of injury, management strategies, surgical techniques, follow-up durations, and baseline preoperative data. Variables such as injury severity, early versus delayed intervention, repair versus reconstruction, and graft type (allograft vs autograft) contribute to a wide array of variation that complicates direct comparisons across studies. Furthermore, many studies likely used outdated surgical techniques (eg, nonanatomic reconstructions) and postoperative rehabilitation plans (eg, avoiding early ROM); therefore, this must be considered when contextualizing the outcomes stated in this review. The overall level of evidence and methodological quality of the included studies were limited, as reflected by their scores on the MINORS criteria. Therefore, the findings of this review should be interpreted with caution.
Conclusion
Outcomes >7 years after treatment of MLKIs demonstrate meaningful restoration of function and sport participation but remain tempered by significant rates of OA and reoperation for stiffness. Advances in surgical technique and early rehabilitation have improved results in contemporary cohorts. Continued prospective evaluation using standardized protocols is essential to enhance joint preservation and patient quality of life.
Footnotes
Final revision submitted October 28, 2025; accepted November 4, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.S.B. has received research support from Arthrex and Smith & Nephew and hospitality payments from Medical Device Business Services. N.N.V. has received royalties from Arthrex and Smith & Nephew, has received consulting fees from Stryker and Arthrex, holds stock in Tetrous, and is on the Board of Directors for the MLB Team Physician Society. R.F.L. has received travel support from Arthrex, Ossur, and Smith & Nephew; consulting fees from Responsive Arthroscopy and Smith & Nephew; royalties from Smith & Nephew and Arthrex; support for education from Foundation Medical; and speaking fees from Linvatec. J.C. has received consulting fees and speaking fees from Smith & Nephew, speaking fees from Synthes GmbH, and support for education from Medwest Associates. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.