
Abstract
Background:
Anterior cruciate ligament (ACL) injuries of the knee in skeletally immature patients are increasingly prevalent, yet limited data exist regarding the mechanical properties of pediatric knee ligaments.
Purpose:
To evaluate and compare the biomechanical properties of the ACL, posterior cruciate ligament (PCL), medial collateral ligament (MCL), lateral collateral ligament (LCL), and iliotibial band (ITB) in pediatric cadaveric knee specimens.
Study Design:
Controlled laboratory study.
Methods:
Eighteen fresh-frozen pediatric knee specimens (aged 8-12 years) underwent dissection and uniaxial tensile testing to failure. Mechanical parameters, including maximum load, stiffness, linear modulus, tensile strain, and tensile strength, were calculated. Results were analyzed using linear mixed-effects models with Tukey-adjusted P values.
Results:
The ITB demonstrated comparable mechanical properties to the ACL and MCL. The ITB also exhibited lower stiffness than the PCL (P = .004) and a higher maximum load than the LCL (P = .001).
Conclusion:
The ITB shows biomechanical properties similar to the ACL and MCL, supporting its use as a graft in pediatric knee ligament reconstruction. These findings enhance the understanding of pediatric ligament mechanics and inform graft selection in surgical planning.
Clinical Relevance:
The study highlights the ITB's biomechanical similarity to the ACL, informing graft selection for ACL reconstruction in pediatric patients.
In the skeletally immature patient population, injuries to the knee that require ligament reconstruction are increasingly common. 5 Pediatric anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) injuries are rising, likely due to increased participation in youth sports and additional potential factors, such as year-round practice and higher levels of competition.1,4 The management of pediatric ACL tears, for one, is a topic of intense interest; the operative timing, technique used, and graft used for reconstruction vary by treating surgeon. PCL injuries in the pediatric population are less common and are less likely to be treated surgically, but they do require surgery in some situations. 8 Similarly, minor collateral ligament injuries (medial or lateral) may be treated with nonoperative management, but high-grade tears of the collateral ligaments may require surgical repair or reconstruction. 2
There is currently substantial cadaveric research about the mechanical and microstructural properties of the ligaments of the adult knee. However, comparatively little is known about the properties of pediatric knee ligaments. In the pediatric population, the process of choosing a graft for surgeries that involve cruciate or collateral ligament reconstruction in pediatric patients is limited by the lack of specific knowledge of the mechanical properties of those ligaments, as well as the periarticular tendons (eg, iliotibial band [ITB], patellar tendon) that may serve as a graft. Pediatric cadaver tissue is rare, and to date, only 2 studies by Schmidt et al11,12 have examined the properties of human skeletally immature knee ligaments. The first study by Schmidt et al 11 examined the mechanical (Young’s modulus, stress, strain) and microstructural (collagen fibril diameter, crimp wavelength) properties of the native pediatric PCL and collateral ligaments (mean age, 9.2 years), while the second study examined those properties in pediatric ACLs, patellar tendons, quadriceps tendons, semitendinosus tendons, and ITBs. 12
The lack of empirical data on ligaments in the pediatric knee currently limits surgical planning for pediatric orthopaedic injuries. The purpose of this study was to evaluate the biomechanical properties of the ACL, PCL, lateral collateral ligament (LCL), medial collateral ligament (MCL), and ITB in pediatric knee specimens. In previous studies of pediatric knee ligaments and periarticular tendons by Schmidt et al,11,12 the ITB exhibited increased strength but was similar to the ACL. The MCL demonstrated a higher transition stress and Young's modulus than the PCL. Otherwise, comparisons were similar. With a larger sample size, we hypothesize that we might not find statistically significant differences in the mechanical properties among the grafts tested. The null hypothesis was that there would be no difference in mechanical properties among the ITB, ACL, PCL, MCL, and LCL.
Methods
Study Design
The tissue used in this study was donated to AlloSource in Colorado (a graft harvesting facility) expressly for use in medical research. Institutional review board approval was not required for this study, as no genetic information was analyzed, no contact was made with donor families, and families gave permission for the tissues to be used for research. Specimens that showed gross deformity, abnormal range of motion, or muscular or ligamentous underdevelopment (eg, due to wheelchair confinement) were excluded.
Dissection
Eighteen skeletally immature fresh-frozen whole knee specimens from 9 human cadavers (8 males, 1 female, aged 8-12 years, mean age 9.8 years) were thawed at room temperature for 24 hours and grossly dissected by a group of fellowship-trained pediatric and sports orthopaedic surgeons (Figure 1). The soft tissues surrounding the ITB, LCL, MCL, ACL, and PCL (in order) were resected outside-in for all specimens. ACLs and PCLs were harvested with bony attachments remaining on the distal and proximal ends to aid in securing ligaments as part of mechanical testing. The MCLs and LCLs were harvested with their periosteal entheses intact on either end of the specimen. Lastly, the ITB was harvested with a distal segment of bone and periosteum, with a tissue width of 1 cm and a length of 5 cm, proximally. We were blinded to the cause of death, and each specimen was inspected for gross musculoskeletal pathology or obvious knee injury; 2 knees were excluded for this reason. For some specimens, paired knees from a single donor were available, while for other specimens, only a single knee was available for mechanical testing. Additionally, we were unable to use all harvested ligaments/tendons for this study, as concurrent studies were analyzing this rare tissue for different analyses, rendering it unusable for mechanical testing. Thus, our analysis includes n values <18.

Exposure of a lateral collateral ligament (left = proximal) for an 11-year-old male.
Anatomic Measurements
Before testing, the width (lateral to medial) and thickness (anterior to posterior) of each ligament were measured with a high-precision caliper (manufacturer-reported accuracy of ±0.02 mm) at the distal, proximal, and mid-substance regions, with the mean of 3 measurements recorded. The length of each specimen (gauge length) was recorded directly from the universal testing frame readouts.
Mechanical Testing
For mechanical testing, specimens were tested as a single unit and kept hydrated throughout. The PCLs, MCLs, and LCLs were not combined or folded over into multiple bundles, and the ACLs were tested as a single unit containing both the anteromedial and posterolateral bundles. Before testing, specimens without a bone block at one end (eg, ITB) were wrapped with aluminum wire to improve fixation within the actuator clamp. Specimens were vertically oriented in an anatomic position, with tension exerted along the longitudinal fibers of the ligament (Figure 2). The proximal and distal ends of each specimen were rigidly secured in wave-profile, screw-side action grips in the actuator and base of an Instron 5944 universal testing frame fitted with a 2-kN load cell (Instron). Measurement error is certified to be <±0.01 mm and <±1 N.
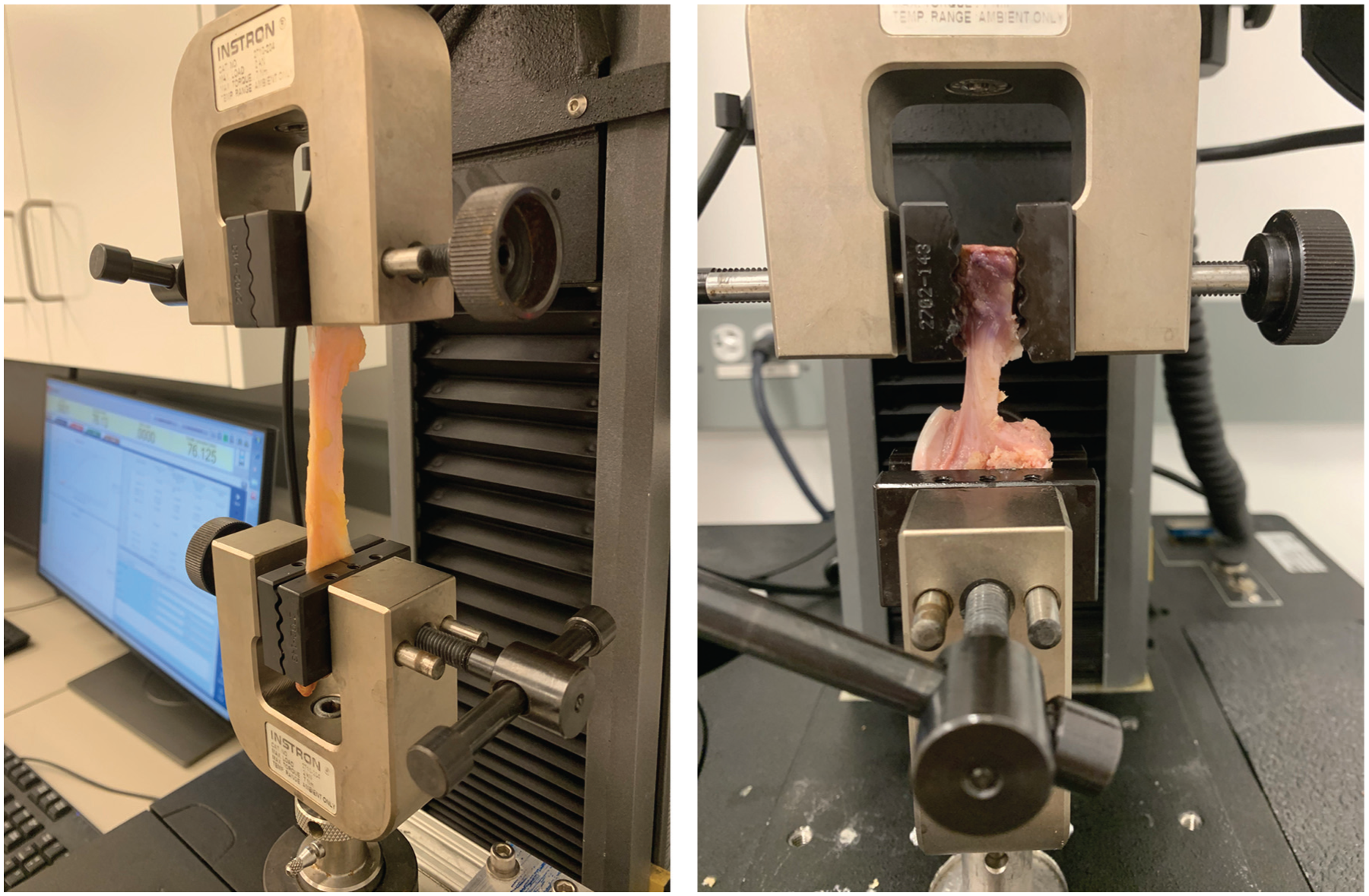
Left: iliotibial band (8-year-old male, left). Right: posterior cruciate ligament (9-year-old male, right).
Specimens underwent a tensile loading protocol consisting of preconditioning cycles and a load to failure. For preconditioning, specimens were loaded from 0% to 5% of the gauge length for 5 cycles. For the load-to-failure test, specimens were loaded at a rate of 1% of the gauge length per second until a peak load occurred. Force and displacement were continuously recorded during the test. Failure was confirmed with a rapid decrease in peak load by at least 25% and visual confirmation of broken fibers of the ligament. The location of failure along the specimen was also recorded.
Data Analysis
After tensile loading, ultimate tensile strength and linear modulus were calculated algorithmically by the testing frame recording software, after a force-displacement curve was produced. For stiffness, a least squares regression analysis was used to find the maximum slope of the force-displacement curve. The cross-sectional area of each specimen was calculated using pi * 0.5w * 0.5t (w = width, t = thickness). We used linear mixed-effects models for each measure, using a random subject ID (for each donor) as the random factor. To account for multiple comparisons, P values were Tukey-adjusted.
Results
Location of Failure, All Specimens
For mechanical failure location, the ACL ruptured at the femur insertion 6 (of 10) and tibia insertion 4 (of 10), and the PCL ruptured at the femur insertion 5 (of 10) and tibia insertion 5 (of 10) (Table 1). There was variability in the location of failure for the LCL and MCL specimens. For the LCL, 5 of 11 failed at the femur insertion, and 6 of 11 failed at the fibula insertion. For the MCL, 5 of 12 failed at the femur insertion, 2 of 12 failed at the tibia insertion, and 5 of 12 failed mid-substance (Table 1). There was variability in the location of failure for the ITB specimens, with 5 of 13 failing at the top clamp, 2 of 13 failing at the tibia insertion, and 6 of 13 failing mid-substance (Table 1).
Sites of Failure During Tensile Testing Categorized by Specimen Type and Location Along Each Specimen a

For the ITB, there was no proximal bone block; therefore, “proximal attachment” refers to the proximal clamp fixation. ACL, anterior cruciate ligament; ITB, iliotibial band; LCL, lateral collateral ligament; MCL, medial collateral ligament; PCL, posterior cruciate ligament.
Mechanical Testing Results
This study evaluated the mechanical properties of pediatric knee ligaments and the ITB through tensile testing (Table 2). The PCL demonstrated the highest maximum load capacity at 374.8 ± 240.7 N, followed closely by the ITB at 367.0 ± 200.5 N, while the LCL showed the lowest at 172.6 ± 88.3 N. The MCL exhibited the highest linear modulus at 116.6 ± 103.1 MPa, substantially greater than the other structures tested. In terms of stiffness, the PCL showed the greatest value at 89.5 ± 74.7 N/mm, followed by the ACL at 63.3 ± 43.7 N/mm. The collateral ligaments (LCL and MCL) demonstrated higher tensile strength values (23.3 ± 9.9 MPa and 26.7 ± 18.5 MPa, respectively) compared with the ITB (15.6 ± 8.2 MPa).
Results for Pediatric Knee Ligaments and the Iliotibial Band (n = 67) a

Values are reported as a mean ± SD. ACL, anterior cruciate ligament; ITB, iliotibial band; LCL, lateral collateral ligament; MCL, medial collateral ligament; PCL, posterior cruciate ligament.
Significant to the 95% confidence interval.
Statistical comparisons between the ITB and other structures revealed significant differences in only 2 parameters. The ITB demonstrated significantly higher maximum load capacity compared with the LCL (P = .001) and significantly lower stiffness compared with the PCL (P = .004). No significant differences were observed between the ITB and other ligaments for linear modulus, tensile strain, or tensile strength measurements (all P > .05). The tensile strain values showed consistent behavior across structures, ranging from 36.3% ± 16.1% for the MCL to 54.4% ± 20.8% for the ACL, with no significant differences detected between the ITB (41.2% ± 14.1%) and other ligamentous structures.
Discussion
This study contributes to the sparse available literature regarding pediatric biomechanics with a precise characterization of the mechanical properties of pediatric knee ligaments. In studies of rabbits, 16 skeletal maturation accompanies increases in linear stiffness, ultimate load, and energy absorption, although it is not known whether these trends are caused by increasing size, microstructural properties, or another reason. Compared with studies of other pediatric knee ligaments,11,12 our study shows that the ITB has a high load-bearing capacity, with tensile strength and linear modulus comparable to those of the ACL. The ITB can withstand similar forces experienced by the ACL without excessive elongation or failure, and the ITB has a lower but statistically similar stiffness compared with the ACL. We believe these findings confirm the ITB as a reasonable graft choice for ACL reconstruction, while recognizing that we are limited in our understanding of how graft properties change within the knee after surgical reconstruction.
A pair of studies by Schmidt et al11,12 examined the mechanical properties of pediatric knee ligaments. The first study 12 found that the ITB demonstrated significantly greater tensile strength and linear modulus than the ACL, with no significant differences in tensile strain and stiffness. That study did not make direct comparisons between the ITB and other knee ligaments or periarticular structures. Of note, their study was methodologically different in that they prepared their specimens in a “dog-bone shape” (so that the mid-substance of each tendon would have a consistent cross section) to help standardize measurement of intrinsic properties, such as linear modulus and tensile stress. In contrast, this study tested the tensile properties of whole ligaments, with bone blocks intact whenever possible.
In preadolescent or adolescent skeletally immature patients, an ITB autograft may be used for a nonanatomic ACL reconstruction without tunnels, sparing the physis. 3 Kocher et al 7 have performed a technique that includes extra-articular and intra-articular reconstruction of the ACL in skeletally immature patients with wide, open physes. An important finding in our study was that the ITB demonstrated no significant difference in linear modulus or tensile strength compared with the ACL. Also, stiffness and tensile strain among those structures were not significantly different. A concern when choosing a graft for ACL reconstruction is that the graft tissue may be significantly stiffer and, depending on the technique used by the surgeon, could overconstrain the knee, increase contact pressures, and raise the risk of osteoarthritis and graft failure. 13 The ITB remains a reasonable choice for ACL reconstruction in anatomic, all-epiphyseal techniques, given that it demonstrates similar stiffness, tensile strain, and ultimate tensile strength among skeletally immature patients.
Based on our findings, the ITB may also serve as a reasonable graft or graft augment for PCL reconstruction. Although not commonly performed, the PCL may be reconstructed, usually after a multiligament knee injury. 10 Autografts that have been used for PCL reconstruction include the hamstring tendon, quadriceps tendon, and bone–patellar tendon–bone,14,15 while allografts, including the Achilles tendon with a bone block and a maternal hamstring tendon, have been used. 8 Similar to comparisons with the ACL, the ITB demonstrated comparable linear modulus, tensile strain, and tensile strength compared with the PCL, although stiffness was significantly different. Additionally, this study supports that a segment of the ITB may be a suitable replacement for the LCL and MCL in skeletally immature patients, given that significant differences were only found between the mechanical properties of the ITB and LCL in terms of maximum load.
Limitations and Future Work
This study has several limitations that we acknowledge. First, the study is limited by a small sample size due to exceptionally rare access to pediatric cadaver tissue donated for research. Second, there were several confounders, including age, skeletal maturity, sex, and paired/unpaired knees. Also, this study was blinded to the cause of death, activity level, body mass index, and medical history. Each specimen underwent at least 2 freeze-thaw cycles during shipment, was dissected, and then was frozen for later testing. In comparison to fresh tissue, fresh-frozen tissue has a higher modulus of elasticity, reflecting greater tolerance to failure, although differences between groups are not significant. Differences in the timing of freezing/thawing and exact temperatures experienced could have differential effects on the microstructure of ligaments and minimally alter their performance during testing.6,9 The location of failure along each specimen during tensile testing was variable, and this variability could lead to differences in performance within a set of specimens.17,18 Additionally, although large variations in the mechanical properties of knee ligaments in healthy adult specimens have been reported, 13 those seen in this study could have been partially caused by differences in specimen preparation during the dissection process, testing variations (eg, graft size/shape, precise clamp placement), and an overwhelmingly male cohort. However, our limited number of available pediatric specimens underpowered meaningful comparative analysis. Finally, the precise function of pediatric knee ligaments that undergo torsional and translational forces in vivo and remodeling after reconstruction cannot be replicated via time-zero, tensile-only laboratory testing, thereby limiting extrapolation of our findings to understanding how grafts may function in vivo.
In the future, a larger sample size and robust analysis of confounding variables can improve the generalizability of the findings produced. Understanding the differences in the mechanical properties of native pediatric knee ligaments is important for maintaining those relationships when choosing grafts for surgical knee reconstruction and repair. A better understanding of the mechanical properties of pediatric knee ligaments can also inform future work evaluating the changes in knee function and stability that occur from various injuries, as well as the ability of pediatric patients to recover from those injuries.
Conclusion
The ITB has comparable properties to the ACL and MCL on all measures. The ITB may serve as a reasonable graft choice for ACL, MCL, and possibly LCL and PCL reconstruction.
Footnotes
Final revision submitted September 29, 2025; accepted October 27, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: H.S. is employed as a senior software engineer with Medtronic. C.C. has provided consulting services to Gordian Biotechnology. S.S. has received nonconsulting fees from Arthrex, Smith & Nephew, Synthes GmbH, Vericel, and Linvatec; consulting fees from Arthrex, Flexion Therapeutics, Bioventus, Biorez, ConMed, DJO LLC, DePuy Synthes Products, Joint Restoration Foundation, Kinamed, Linvatec, Medical Device Business Services, Pacira Pharmaceuticals, Smith & Nephew, Vericel, JRF Ortho, LifeNet Health, Zimmer Biomet, and Olympus America; education payments from Evolution Surgical; speaking fees from Flexion Therapeutics; royalties from ConMed; honoraria from Flexion Therapeutics; education payments from Elite Orthopedics LLC and Evolution Surgical; and a grant from DJO LLC; is a board or committee member of Epic Bio, Joint Restoration Foundation, and Vericel; holds stock or stock options in Epic Bio and Vivorte; and has performed product evaluation for ConMed and Olympus. H.B.E. is affiliated with Arthrex, Smith & Nephew, and Orthopediatric; has received grants from the Pediatric Orthopaedic Society of North America and American Academy of Orthopaedic Surgeons, hospitality payments from Stryker, and support for education from Pylant Medical; and is a board or committee member of Texas Orthopaedic Association and Pediatric Research in Sports Medicine. M.T. has received travel expenses from Aesculap Biologics. P.W. has received support for education from Arthrex. D.G. receives royalties and licenses from Arthrex and Pega Medical, has received consulting fees from Arthrex, and has received honoraria from AO Trauma International, Arthrex, and Synthes GmbH. T.J.G. has received support for education from Arthrex and Liberty Surgical, has received research support from Vericel, is an associate editor of the American Journal of Sports Medicine, and is a board or committee member of Pediatric Research in Sports Medicine, American Academy of Pediatrics Section on Orthopaedics, International Pediatric Orthopaedic Symposium, Pediatric Orthopaedic Society of North America, and American Academy of Orthopaedic Surgeons. K.G.S. is a medical advisory board member of nView, Sarcio, and Medeloop and has received education payments from Evolution Surgical and hospitality payments from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.