
Abstract
Background:
Anterior shoulder dislocation is a common and functionally limiting injury in professional martial arts (MA) athletes. While arthroscopic Bankart repair is widely performed, data on long-term functional and sport-specific outcomes in elite-level MA athletes after a first-time dislocation remain scarce.
Purpose:
To evaluate the 5-year clinical and functional outcomes of arthroscopic Bankart repair using bioabsorbable suture anchors in elite MA athletes who sustained a first-time traumatic anterior shoulder dislocation without bony Bankart lesions.
Study Design:
Case series; Level of evidence: 4.
Methods:
A total of 27 elite international-level MA athletes who experienced a first-time anterior shoulder dislocation and underwent arthroscopic Bankart repair with bioabsorbable suture anchors were included. All surgeries were performed within 3 weeks after the injury. Patients with bony Bankart lesions and those who had undergone either remplissage for large Hill-Sachs lesion or previous shoulder surgery were excluded. Functional evaluation included pre- and postoperative assessments using Rowe, Athletic Shoulder Outcome Scoring System, Shoulder Sport Activity Score, forward flexion, and external rotation in adduction. Return to sport and return to preinjury competitive level were also recorded. Postoperative magnetic resonance imaging (MRI) at 6 months assessed anchor position, stability, and cartilage or bony lesions. Outcomes were compared between athletes who returned to their previous competition level and those who did not.
Results:
The mean age was 24.3 years and the mean follow-up was 63.0 ± 2.5 months (range, 54-69 months). All athletes returned to sports, with 85.2% (n = 23) resuming competition at their preinjury level. Significant improvements were observed in all functional scores (P < .001 for all), while a slight postoperative decrease in range of motion parameters was noted. No significant differences were found in clinical scores between those who returned to their preinjury level and those who did not. Recurrent dislocation occurred in 2 athletes (7.4%) during competition. Radiological follow-up with postoperative MRI was available for all 27 athletes. At 6 months, all patients demonstrated proper anchor position and stability, with no evidence of displacement or loosening. No cartilaginous or bony lesions were detected.
Conclusion:
Arthroscopic Bankart repair with bioabsorbable suture anchors is a safe and effective treatment for first-time anterior shoulder dislocation in elite MA athletes. This approach results in excellent long-term functional outcomes and a high rate of return to elite-level competition, with a low risk of recurrence when patients are properly selected.
Keywords
A Bankart injury is defined as the avulsion of the anterior and inferior glenoid labrum from the glenoid cavity, primarily caused by a traumatic incident. 3 Bankart injury is a frequent sports-related trauma, particularly of athletes involved in contact and throwing sports, and consists of an avulsion of the glenohumeral ligaments from the anterior glenoid and in some cases involves a fracture of the glenoid. 5
Surgical treatment of a Bankart injury is a common procedure in athletes, as there is a tendency of dislocations to recur, mainly in the first few years after the initial injury, and possibly progress to recurrent anterior shoulder instability, which may hinder the athlete from resuming sports activities and continuing at his or her previous level before the injury.6,22
More than half of the young patients who get a Bankart lesion will experience redislocation of the shoulder despite rehabilitation, and surgical treatment is in most cases necessary in athletes with a high demand for shoulder stability. 8
With the advancement of arthroscopic instruments and improved knowledge of the technique, arthroscopic Bankart repair has shown positive outcomes in terms of shoulder stabilization, as well as minimal required dissection and enhanced patient comfort, since its initial description 3 decades ago. Being an anatomically oriented technique, arthroscopic Bankart repair primarily reestablishes the tension of the capsuloligamentous complex, thereby restoring shoulder stability. 21
Judo and Taekwondo are recognized as martial arts (MA) and are included in the Olympic Games. On the other hand, wrestling, considered a subset of mixed MA, is one of the oldest forms of combat sport and holds significant traditional value in ancient Greek and Turkish cultures. 24 Participation in all types of MA is linked to a higher risk of injuries compared with noncombat or low-contact sports, owing to the repetitive throwing, grappling, and striking maneuvers involved. Research has shown that the sports most commonly linked with shoulder instability are football, basketball, and wrestling, with the predominant type of instability being occasional, traumatic, anterior dislocation. 29 Athletes with recurrent dislocations were more likely to undergo surgical treatment, whereas nonoperative management of anterior shoulder dislocation in contact-sport athletes has been reported to carry considerably higher recurrence rates. 8 Additionally, the incidence of shoulder instability injuries in collegiate sports was reported at 31.30 injuries per 100,000 exposures, with anterior subluxation and dislocation comprising more than half of these injuries. These injuries negatively affect the ability to return to sports, and for athletes who have had a Bankart repair for a traumatic anterior shoulder dislocation there is an increased risk for recurrence in relation to these types of MA. Preoperative recurrent instability is recognized as an independent risk factor for postoperative recurrence, with competitive wrestlers who had multiple dislocations before their initial evaluation being nearly 4 times more likely to face postoperative recurrent instability.13,27
There is an enduring interest in and growing body of recent studies on outcome reports that focus on the treatment of traumatic anterior instability and Bankart lesions, particularly in young elite professional athletes participating in contact sports. Hence, the primary aim of our study was to assess and report the follow-up outcomes of elite athletes competing in MA who underwent arthroscopic Bankart operations utilizing bioabsorbable suture anchors as the primary treatment approach for anterior shoulder instability without bony Bankart lesions.
We hypothesized that arthroscopic Bankart repair with bioabsorbable suture anchors in elite MA athletes without bony Bankart lesions would result in significant functional improvement, high rates of return to sport, and low recurrence rates at midterm follow-up.
Methods
The study group consisted of professional elite athletes who experienced a shoulder dislocation and subsequently underwent arthroscopic Bankart repair using bioabsorbable suture anchors. All participants were operated 3 weeks after dislocation. It was the first dislocation in all patients. According to the magnetic resonance imaging (MRI) and computed tomography performed after the dislocation of the affected shoulder, there was no bony Bankart.
All participants were actively involved in international competitions, including those at the Olympic level. The study period was October 2014 to March 2024. The following were the requirements for inclusion: (1) athletes who experienced their first dislocation, (2) patients who had arthroscopic Bankart (Bankart lesion including anterior labral periosteal sleeve avulsion) repair without any further intra-articular procedures such as bone Bankart repair, and (3) athletes who participated in competitive club or team sports at an international level. Patients with a bony Bankart lesion and those who had undergone a remplissage procedure for large Hill-Sachs lesions were excluded from the study.
Other exclusion criteria were (1) a previous history of shoulder dislocation and surgery, (2) previous surgical procedures on the region of interest, (3) cases that required additional procedures on the head of the humerus, and (4) fracture dislocation. The study was conducted in accordance with the Declaration of Helsinki, and informed consent was obtained from all participants.
Patients were evaluated weekly until the third postoperative week, every 3 months during the first year, and annually thereafter. The mean follow-up was 63 months (range, 54-69 months), during which complications such as redislocation were monitored. Functional outcome scores (Rowe, Athletic Shoulder Outcome Scoring System [ASOSS], Shoulder Sport Activity Score [SSAS]), and range of motion parameters (forward flexion and external rotation in adduction23,26) were recorded preoperatively and at 12 months postoperatively. Radiological follow-up was performed with MRI at 6 months postoperatively in all athletes. The evaluation focused on the position and stability of the suture anchors (intact vs loosened), as well as the presence or absence of cartilaginous or bony lesions. All MRI evaluations were performed independently by 2 experienced orthopaedic surgeons (Y.İ. and T.K.). In addition, patient statements and their ability to return to sports were considered, along with their rate of returning to previous competitive activity levels. The criterion for return to previous competitive activity level was defined as the athlete's participation in national and international tournaments in which he or she had competed before the injury and surgery.
Surgical Technique
All patients underwent arthroscopic Bankart repair performed by a single experienced orthopaedic surgeon (Y.İ.) using the same technique and instrumentation. Under general anesthesia, each patient was positioned in the beach-chair position. The direction and magnitude of shoulder instability were first assessed. The shoulder was then prepared and draped in a sterile fashion, and anatomic landmarks were marked for proper orientation during the procedure.
Three arthroscopic portals—posterior, anterior, and anterosuperior—were established. The procedure began with diagnostic arthroscopy to evaluate the glenoid labrum, joint capsule, rotator cuff, and glenohumeral ligaments. The anterior labrum was mobilized using a periosteal elevator to achieve superior and lateral capsulolabral shift. Mobilization was continued up to a 180° arc from the subscapularis fascia, exposing the subscapular muscle fibers to allow sufficient mobilization and repositioning of the labrum.
Labral reattachment and capsular advancement were performed using bioabsorbable polyetheretherketone (PEEK) GRYPHON suture anchors (DePuy Synthes; Johnson & Johnson MedTech). Each anchor was placed with care to apply individualized tension to ensure optimal fixation. Three or 4 anchors were used in all patients. In younger patients or those with a narrower glenoid surface, 3 anchors were generally sufficient, positioned sequentially at the 5-, 4-, and 3-o’clock positions on the glenoid rim (right shoulder orientation). A fourth anchor was placed if additional fixation was required, depending on the lesion characteristics and the extent of the labral separation. The intraoperative preparation phase, including portal placement and glenoid exposure, is demonstrated in Figure 1. Figure 2 illustrates the arthroscopic appearance of the Bankart lesion before repair and the restored capsulolabral complex after primary fixation with bioabsorbable PEEK GRYPHON suture anchors.

Arthroscopic view demonstrating preparation of the glenoid rim with a shaver for soft-tissue debridement (left) and use of a rasp during tissue preparation (right).

Arthroscopic image of the Bankart lesion (left) and result after the primary repair with bioabsorbable polyetheretherketone GRYPHON suture anchors (right).
After the procedure, the arthroscopic portals were closed, and the shoulder was immobilized in a sling for 3 weeks. All patients followed an identical postoperative rehabilitation protocol supervised by one of the authors (Y.İ.). During the initial 3 weeks, patients were instructed to limit external rotation and begin passive and assisted active range of motion exercises. At 6 weeks, active exercises were initiated. Muscle strengthening and endurance training were started at 3 months. Weightbearing activities were allowed at 6 months, and return to overhead and contact sports was recommended after a 7-month transition period.
Statistical Analysis
Statistical analysis was carried out using the GraphPad Prism for Windows (Version 10.0.0; GraphPad Software). Paired and unpaired 2-tailed t tests were used for parametric comparisons, while nonparametric data were evaluated using the Mann-Whitney U test. The level for statistical significance was set to an alpha level of P < .05.
Results
The study included 27 elite athletes competing in contact sports: Taekwondo (n = 7), Judo (n = 3), and wrestling (n = 17). Six additional operated athletes—Taekwondo (n = 2) and wrestling (n = 4)—were excluded because of loss to follow-up.
During the follow-up period, the operating surgeon and the rehabilitation team maintained regular communication with the athletes and their respective agencies to ensure the preservation of the initial outcomes.
The data of the patient group is presented in Table 1.
Patient Data

The mean age of the 27 included patients was 24.3 years at the time of their primary stabilization procedure. Among them, 23 (85.2%) were male, while 4 (14.8%) were female.
Table 2 presents a comparison of pre- and postoperative scores of Rowe, ASOSS, SSAS, forward flexion, and external rotation in adduction.
Comparison of Pre- and Postoperative Activity Scores of the Patients (N = 27) a

Bold values indicate statistical significance at P < .05. ASOSS, Athletic Shoulder Outcome Scoring System; ER, external rotation; SSAS, Shoulder Sport Activity Score.
We found a statistically significant difference between the measurements for all variables; however, a decrease was observed specifically in external rotation and forward elevation (P < .001).
After the surgery, 23 out of 27 patients (85.2%) were able to resume competing at the same level as before. The mean time to return to sports activity was 5 months (range, 4-6 months; minimum 4 months), while the duration of return to competitions was 8 to 10 months. Furthermore, all 27 patients (100%) successfully returned to sports and were eligible to participate in national and international competitions. The outcome scores of athletes depending on their professional competition status are presented in Table 3.
Comparison of Athletes Depending on Professional Competition Status a
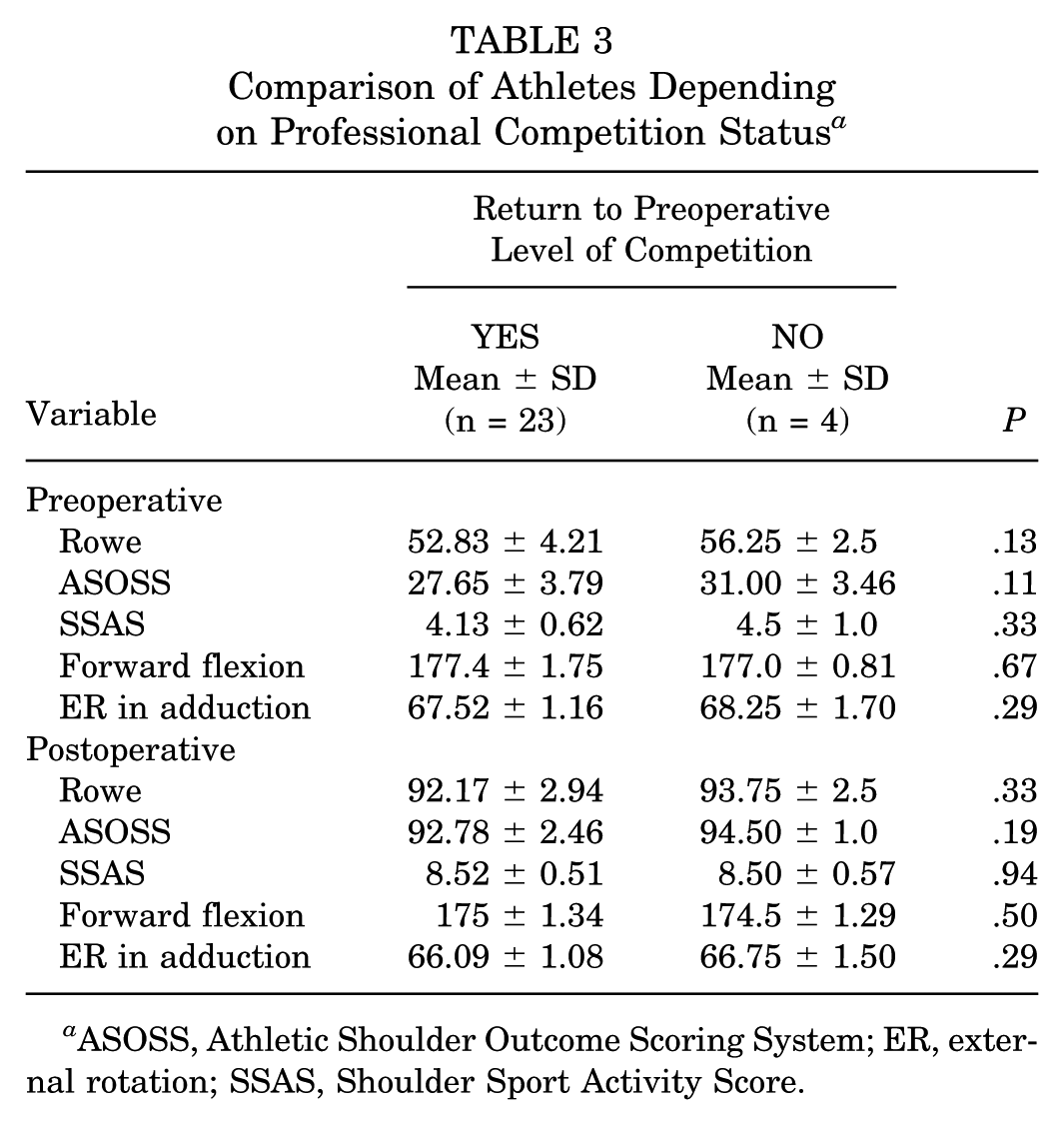
ASOSS, Athletic Shoulder Outcome Scoring System; ER, external rotation; SSAS, Shoulder Sport Activity Score.
All patients completed all of the clinical follow-up scores, and statistical analysis indicated no significant difference between the groups of patients who were able to return to the same level of competition and those who could not, in terms of both pre- and postoperative variables.
Out of the total patient population, 2 individuals (7.4%) encountered dislocation episodes during competitions (Figure 3). The first athlete experienced the incident 17 months after the initial surgery, while the second patient had a dislocation 61 months after surgery (Table 4). These 2 patients later were operated with the Latarjet procedure.

The specific moment of redislocation in an elite athlete who underwent a primary Bankart repair (red shirt athlete; right shoulder). At the time of the injury, the athlete was competing in an international tournament and the injury took place on the 17th month of follow-up.
Cases With Recurrence After Bankart Repair

Radiological follow-up with postoperative MRI was available for all 27 athletes. At 6 months, all patients demonstrated proper anchor position and stability, with no evidence of displacement or loosening. No cartilaginous or bony lesions were detected.
The total time for follow-up was 63 ± 2.5 months (range, 54-69 months) with a minimum follow-up of 54 months. We did not encounter any complications during and after the surgery.
Discussion
In our study series, we present the data of 27 professional MA athletes competing at the international and Olympic levels who underwent arthroscopic Bankart repair for anterior shoulder dislocation. For elite athletes, a prompt return to sport is crucial. We suggest that the arthroscopic approach improves functional outcomes and increases the likelihood of returning to preinjury competition levels. In our cohort, all patients resumed sporting activities, and 85.2% returned to their original competitive level. The mean return-to-sport time was 5 months, and return to the competition level averaged 8 months.
According to the 2022 Bern consensus statement, the return-to-sport continuum consists of 3 phases: return to participation, return to sport, and return to performance. 24 In our cohort, 23 athletes returned to full performance, while 4 competed below their preinjury level. Interestingly, the clinical outcome scores of those who did not return to their original level were comparable with the rest of the cohort, and all were cleared for return by both the surgeon and the rehabilitation team. In a comparative study, Rossi et al 22 identified fear of reinjury, reduced confidence in the shoulder, and concern over undergoing another rehabilitation process as primary factors in failure to return to sport. Thus, a comprehensive rehabilitation program should also address psychological factors. Incorporating cognitive behavioral and compartmental therapies may help reverse injury-induced neural changes and enhance return-to-sport outcomes. 15
MA places considerable biomechanical stress on the shoulder due to such maneuvers as grappling, pinning, and takedown.14,28 These high-stress demands inherently increase the risk of recurrence. 16 While arthroscopic repair has historically been associated with a slightly higher recurrence rate than open procedures, it provides significant advantages in terms of reduced intraoperative blood loss, shorter hospital stays, and lower postoperative pain scores.1,10-12
A randomized controlled trial by Pougés et al 19 compared arthroscopic Bankart repair to nonoperative treatment with immobilization in individuals aged <25 years with a first-time dislocation. Results showed that surgery significantly reduced recurrence rates and improved functional outcomes at 2 years.
Recurrence risk also varies across sports. In MA, the recurrence rate is typically 20% to 25%, which aligns with our findings. 9 In comparison, rugby players and boxers experience similarly high recurrence rates, whereas soccer and field hockey athletes—because of lower contact intensity—have recurrence rates of <5%.2,14,20 Long-term follow-up studies have reported higher recurrence rates in patients treated with nonabsorbable suture anchors.7,20 In contrast, our study used bioabsorbable suture anchors, which may partly explain the relatively lower recurrence observed during the 5-year follow-up.
In our series, 2 athletes experienced recurrence. The first had a premature return to high-contact activity despite completing postoperative rehabilitation. The second dislocation occurred during a competition. Both were competitive wrestlers—a sport known for repetitive shoulder abduction and rotation forces—and both athletes’ injuries were subsequently managed with the Latarjet procedure.
Our findings are consistent with reports from other high-impact sports such as rugby, American football, and ice hockey. 2 In these sports, return-to-sport rates after arthroscopic Bankart repair range from 75% to 90%, while recurrence varies between 15% and 30%, depending on physical demands. 2 Athletes in these disciplines often return to play at 6 to 8 months, with peak performance recovery taking up to 10 to 12 months. 25 Our MA athletes demonstrated comparable recurrence but achieved slightly faster return-to-play timelines (5 months for participation, 8 months for performance).
In lower-risk sports such as tennis, baseball, or pivoting sports such as soccer, recurrence rates after Bankart repair with bioabsorbable suture anchors are significantly lower—typically <10%—because of reduced trauma mechanisms.4,17,18 These athletes usually return in 6 to 9 months depending on biomechanics and neuromuscular demands. 24
Limitations
Despite the homogeneity of our sample, the study has limitations, including the absence of a control group and relatively short follow-up. However, we achieved full follow-up for all participants over 5 years, and the population comprised high-risk individuals because of age and sport intensity. Still, recurrence was limited to 2 cases (7.4%), and we continue to collect long-term outcome data for ongoing evaluation.
Conclusion
We conclude that arthroscopic Bankart stabilization using bioabsorbable suture anchors represents a treatment for managing primary anterior shoulder dislocation without bony Bankart lesions in young, highly demanding professional MA athletes. With proper patient selection, this technique yields excellent functional recovery, high return-to-performance rates, and a low incidence of complication and recurrence.
Footnotes
Final revision submitted September 30, 2025; accepted November 9, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. This study was approved by the Institutional Review Board (approval No. E-96317027-514.10-275310325).
Data Accessibility Statement
Data are available upon reasonable request.