
Abstract
Background:
The glenohumeral joint is one of the most frequently dislocated joints in the body, particularly in young, active adults.
Purpose:
To conduct a systematic review and meta-analysis to evaluate and compare outcomes between anterior versus posterior shoulder instability.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review was performed using the PubMed, Cochrane Library, and MEDLINE databases (from inception to September 2019) according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Studies were included if they were published in the English language, contained outcomes after anterior or posterior shoulder instability, had at least 1 year of follow-up, and included arthroscopic soft tissue labral repair of either anterior or posterior instability. Outcomes including return-to-sport (RTS) rate, postoperative instability rate, and pre- and postoperative American Shoulder and Elbow Surgeons (ASES) scores were recorded and analyzed.
Results:
Overall, 39 studies were included (2077 patients; 1716 male patients and 361 female patients). Patients with anterior instability had a mean age of 23.45 ± 5.40 years (range, 11-72 years), while patients with posterior instability had a mean age of 23.08 ± 8.41 years (range, 13-61 years). The percentage of male patients with anterior instability was significantly higher than that of female patients (odds ratio [OR], 1.36; 95% CI, 1.04-1.77; P = .021). Compared with patients with posterior instability, those with anterior instability were significantly more likely to RTS (OR, 2.31; 95% CI, 1.76-3.04; P < .001), and they were significantly more likely to have postoperative instability (OR, 1.53; 95% CI, 1.07-2.23; P = .018). Patients with anterior instability also had significantly higher ASES scores than those with posterior instability (difference in means, 6.74; 95% CI, 4.71-8.77; P < .001). There were no significant differences found in postoperative complications between the anterior group (11 complications; 1.8%) and the posterior group (3 complications; 1.6%) (OR, 1.12; 95% CI, 0.29-6.30; P = .999).
Conclusion:
Patients with anterior shoulder instability had higher RTS rates but were more likely to have postoperative instability compared with posterior instability patients. Overall, male patients were significantly more likely to have anterior shoulder instability, while female patients were significantly more likely to have posterior shoulder instability.
Keywords
The glenohumeral joint is exceedingly unstable and therefore is one of the most frequently dislocated joints in the body, particularly in young, active adults. 4,16,18,33 A study on shoulder instability performed by the Multicenter Orthopaedic Outcomes Network (MOON) Shoulder Instability Group 37 concluded that most patients who undergo shoulder stabilization are in their early 20s or younger and that anterior instability is more prevalent than posterior instability. These findings have also been found by numerous other studies. 4,33,46 Although posterior instability is not as common, there are certain subgroups that have a high prevalence, including weightlifters, football players, and rugby players. 26,38
The presenting symptoms of anterior instability are very different from posterior instability. A cohort study by Bernhardson et al 4 comparing outcomes of anterior versus posterior instability between 200 patients determined that patients with anterior instability typically present after an identifiable mechanism of injury (requiring reduction by a medical provider) and complaints of instability. On the other hand, patients with posterior instability primarily presented with pain, but no mechanism of injury nor complaints of instability. This frequently occurs in the setting of repetitive microtrauma, such as long-term bench press, incline bench, or push-ups. Thus, weightlifters, football players, and rugby players are found to have a higher prevalence of posterior shoulder instability. 26,38
Finally, the decision of whether to treat shoulder instability operatively or nonoperatively is of considerable debate. With regard to anterior instability, patients traditionally have initially been managed nonoperatively with a period of immobilization and rehabilitation, but this can lead to an unacceptably high recurrence rate, which has increased the prevalence of early operative stabilization. 5,34,45,54 On the other hand, treatment for posterior instability is largely controversial, owing to the overall low prevalence of patients with posterior instability and the even lower number of patients undergoing surgical stabilization. 26
Thus, numerous studies have observed outcomes after arthroscopic labral repair for anterior and posterior shoulder instability. The purpose of this study was to conduct a systematic review and meta-analysis to evaluate and compare outcomes between anterior versus posterior shoulder instability. We hypothesized that patients suffering from posterior shoulder instability would have superior outcomes after operative treatment.
Methods
Search Strategy and Study Selection
This study was reported in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. 60 Two authors (R.G.C., N.E.G.) performed a manual study selection using the PubMed, Cochrane Library, and MEDLINE databases with any discrepancies being resolved through discussion with a third author (M.L.V.). The following search terms were utilized: “anterior shoulder instability,” “anterior shoulder dislocation,” “posterior shoulder instability,” “posterior shoulder dislocation,” “anterior labral tear,” “anterior labral repair,” “posterior labral tear,” “posterior labral repair,” “Bankart repair,” and “Reverse Bankart repair.” These databases were searched from inception to September 2019. All selected articles were then screened for additional studies using the reference lists provided in each article. After duplicates were removed, the titles and abstracts were screened for relevance. The full text was reviewed for the remaining articles to assess for eligibility using the criteria stated below.
Eligibility Criteria
Studies that met the following criteria were included: published in the English language, contained outcomes (defined below) after anterior or posterior shoulder instability, only included patients with at least 1 year of follow-up, and treated with arthroscopic soft tissue labral repair of either anterior or posterior instability. Studies were excluded if any of the following were present: published in a non-English language, no mention made of anterior or posterior instability, no stated data on outcomes, contained or used nonhuman subjects, included any other shoulder pathologies at the time of treatment, utilized open soft tissue labral repair, or utilized open and/or arthroscopic bony repair or reconstruction for shoulder instability. Patients from the included studies were separated into an anterior instability group and a posterior instability group based on their demographics, injury history, and postoperative outcomes and complications.
Outcomes
Patient demographics included sex, age, and whether the study reported on anterior or posterior instability. Outcomes that were used for a study to meet inclusion criteria required 1 of the following: pre- and postoperative functional scores specified by the American Shoulder and Elbow Surgeons (ASES) shoulder score, percentage of patients who returned to sport (RTS), recurrence of instability postoperatively, and postoperative complications. Recurrence of instability was defined as 1 or more of the following parameters: postoperative traumatic instability/dislocation, instability preventing return to full activity or sport, or necessity for postoperative surgical intervention. RTS was defined as percentage of patients who returned to sport at or above their preinjury level without any episodes of recurrence/instability.
Statistical Analysis and Meta-analyses
When comparing the RTS percentage, instability recurrence, and postoperative complications, the Fisher exact test was used to estimate odds ratios (ORs) between the anterior and posterior instability groups. The ASES scores from reporting studies were used to assess the difference between preoperative and postoperative outcomes, and the Z test was used to estimate the difference in means between the anterior and posterior instability groups. The odds of the different sexes experiencing an anterior versus posterior instability was calculated using a Fisher exact test. Finally, age of experiencing anterior and posterior instabilities was compared using a Z test. P ≤ .05 and confidence intervals that did not contain the null value (zero) were considered significant.
Results
After identifying 4739 studies that matched our search criteria, this was narrowed to 4541 studies after duplicate removal. We then excluded 4399 studies based on the criteria mentioned previously. Only 142 full-text articles remained, which was further reduced to the final 39 studies that met criteria for the meta-analysis. Figure 1 denotes the flow diagram used for the study. Only 1 study was found to directly compare anterior versus posterior instability. 4 The included studies were then assessed based upon the following components: patient demographics, RTS rate, postoperative instability, and functional outcomes.

Flow diagram used for the study. SLAP, superior labral from anterior to posterior.
Patient Demographics
Table 1 summarizes the patient demographics in the included studies.
Patient Demographics in the 39 Included Studies a
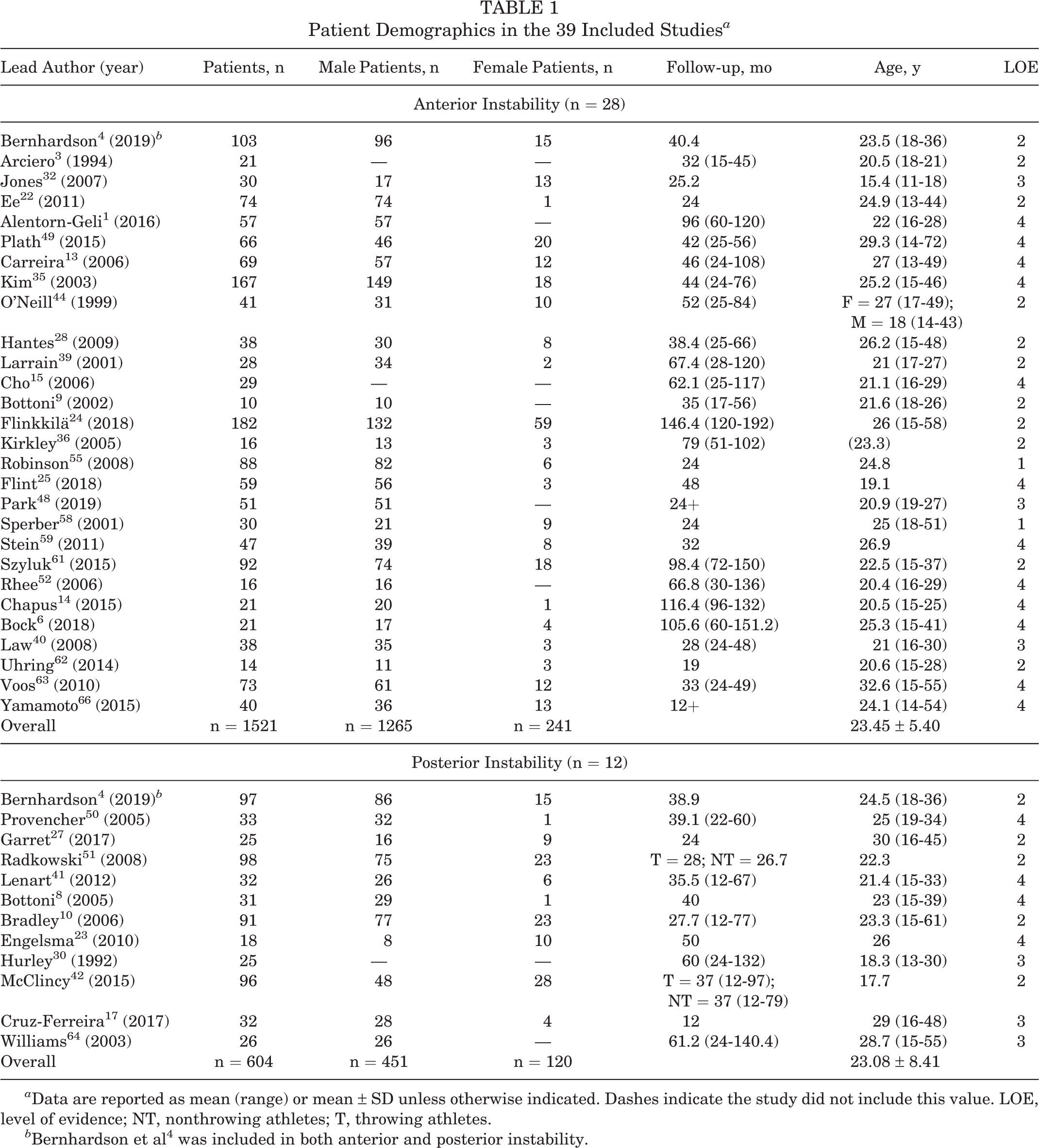
a Data are reported as mean (range) or mean ± SD unless otherwise indicated. Dashes indicate the study did not include this value. LOE, level of evidence; NT, nonthrowing athletes; T, throwing athletes.
b Bernhardson et al 4 was included in both anterior and posterior instability.
For the analysis of patient sex, 36 studies (92.3%) were included, with 1716 male and 322 female patients. ∥ The percentage of male patients with anterior instability was significantly higher than that of female patients (OR, 1.36; 95% CI, 1.04-1.77; P = .021, Fisher exact test), and the percentage of female patients with posterior instability was significantly higher than that of male patients (OR, 1.36; 95% CI, 1.04-1.77; P = .021, Fisher exact test) (Table 2).
Overall Prevalence of Instability Between Sexes a

a Data are reported as n (%) unless otherwise indicated.
b Statistically significant (P ≤ .05).
For the age analysis, 9 studies (23.8%) were used. 6,10,14,25,51,53 –55,59 Of the 425 patients included, 236 (55.5%) had anterior instability 6,14,25,53 –55,59 while 189 (44.5%) had posterior instability. 10,51 There was no significant difference between the groups (difference in means, 0.37; 95% CI, –1.02 to 1.75; P = .302, Z test) (Table 3).
Difference in Age Between Anterior and Posterior Instability Patients a
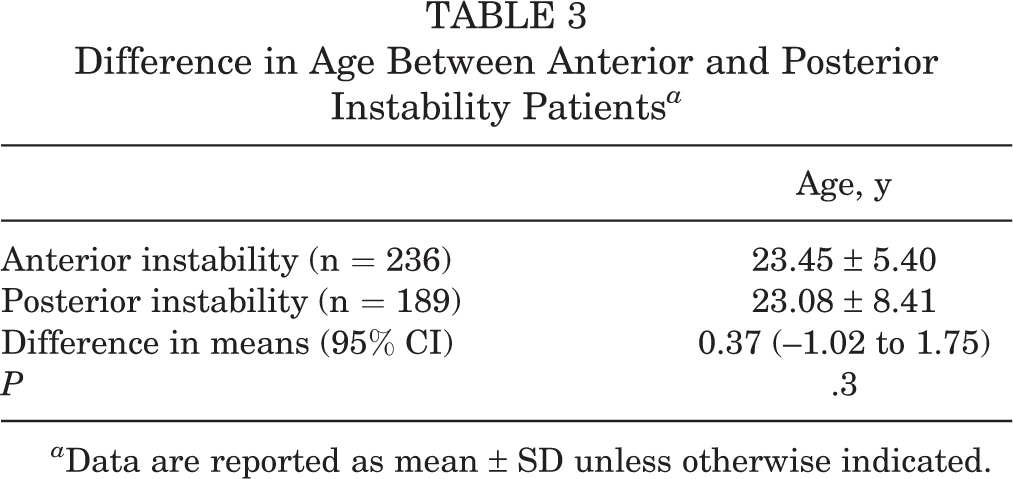
a Data are reported as mean ± SD unless otherwise indicated.
Return to Sport
For the comparison of RTS between anterior and posterior instability, 25 studies (64.1%) with a total of 1257 patients were included. ¶ The range of follow-up time varied between the 2 groups. The anterior instability subset ranged from 15 months (1.25 years) to 132 months (11 years), while the posterior instability subset ranged from 12 months (1 year) to 132 months (11 years). There were 874 patients (69.5%) with anterior instability, of which 695 (79.5%) returned to sport, # and 383 patients (30.5%) with posterior instability, of which 240 (62.7%) returned to sport. 10,27,30,41,42,51,66 Patients with anterior instability were significantly more likely to RTS (OR, 2.31; 95% CI, 1.76-3.04; P < .001, Fisher exact test) (Table 4).
Difference in Return to Sport Between Anterior and Posterior Instability Patients a

a Data are reported as n (%).
b Statistically significant (P ≤ .05).
Postoperative Instability
There were 35 studies (89.7%) included in the analysis of postoperative instability, with a total of 1846 patients. ** The range of follow-up time varied between the 2 groups. The anterior instability subgroup ranged from 15 months (1.25 years) to 192 months (16 years), while the posterior instability subgroup ranged from 12 months (1 year) to 140.4 months (11.7 years). There were 1406 patients (76.2%) with anterior instability, of which 195 (13.9%) had postoperative instability, †† and 440 patients (23.8%) with posterior instability, of which 42 (9.5%) had postoperative instability. 8,10,23,27,41,50,51,64 Patients with anterior instability were significantly more likely to have postoperative instability (OR, 1.53; 95% CI, 1.07-2.23; P = .018, Fisher exact test) (Table 5).
Difference in Postoperative Instability Between Anterior and Posterior Instability Patients a

a Data are reported as n (%).
b Statistically significant (P ≤ .05).
Functional Scores
Figure 2 provides a breakdown of functional outcome measures reported by the included studies. The ASES score was used as the primary functional outcome of interest, as it provided the most comparable data between studies. There were 6 studies (15.4%), with a total of 547 patients, that reported ASES scores. 10,35,41,42,51,63 The difference between preoperative and postoperative scores was used to analyze the data. The follow-up time for anterior instability studies that reported ASES scores ranged from 24 months (2 years) to 76 months (6.3 years), while posterior instability studies ranged from 12 months (1 year) to 97 months (8.1 years). There were 240 patients with anterior instability (43.9%) 35,63 with a mean difference of 35.71 ± 19.91 between preoperative and postoperative scores, and 307 patients with posterior instability (56.1%) 10,41,42,51 with a mean difference of 35.71 ± 33.73 between preoperative and postoperative scores. The functional scores in patients with anterior instability were not significantly different than in patients with posterior instability (difference in means, 0.001; 95% CI, –4.54 to 4.54; P = .999, Z test). However, when looking at just postoperative ASES scores, patients with anterior instability scored significantly higher (difference in means, 6.74; 95% CI, 4.71-8.77; P < .001, Z test). These results are shown in Table 6.

Breakdown of the various shoulder functional outcome scores used in the included studies. ASES, American Shoulder and Elbow Surgeons; ASOSS, Athletic Shoulder Outcome Scoring System; DASH, Disabilities of the Arm, Shoulder and Hand; ISIS, Instability Severity Index Score; OIS, Oxford Instability Score; SANE, Single Assessment Numeric Evaluation; SST, Simple Shoulder Test; SSV, Subjective Shoulder Value; UCLA, University of California Los Angeles Shoulder Score; VAS, visual analog scale; WOSI, Western Ontario Shoulder Instability Index.
Difference in ASES Scores Between Anterior and Posterior Instability Patients a

a Data are reported as mean ± SD unless otherwise indicated. ASES, American Shoulder and Elbow Surgeons.
b Statistically significant (P ≤ .05).
Postoperative Complications Other Than Recurrence
Table 7 outlines the various complications listed among our subgroups of interest. Among the 39 included studies, only 19 ‡‡ (48.7%) indicated whether or not there were postoperative complications, and only 6 of these studies 3, 10, 44, 55, 61, 63 (15.4%) actually had complications listed.There was no significant difference found between the anterior group (11 complications; 1.8%) and the posterior group (3 complications; 1.6%) (OR, 1.12; 95% CI, 0.29-6.30; P = .999). Of note, 1 study (Arciero et al 3 ) had 3 postoperative complications but did not delineate whether the complications fell in the anterior operative or anterior nonoperative subgroups. Therefore, these complications were not included in the data analysis but were included in Table 7 to be more all-inclusive.
Postoperative Complications Between Subgroups a

a Arciero et al 3 included both anterior operative and anterior nonoperative but did not specify which complications were attributed to each group.
Quantitative Bias Analysis
The results of the quantitative bias analysis can be found in Appendix Figure A1. We were only able to find 2 studies 55,58 in our literature review that were level 1 evidence; however, none of these studies directly compared anterior versus posterior shoulder instability. While only 4 included studies were randomized controlled trials, 9,36,55,58 there were also 13 prospective cohort and 9 retrospective cohort studies that carried a somewhat low risk of bias. However, the fact that 13 included studies were case series may partially skew our results due to their heightened risk of bias. Furthermore, only 1 level 3 study 4 directly looked at anterior versus posterior instability, thus putting the overall results of this study at high risk of compounding bias.
Discussion
To our knowledge, this is the first systematic review that has shed light on the differences in outcomes after anterior versus posterior shoulder instability. The most noteworthy conclusion was that overall, patients with anterior shoulder instability were 2.31 times more likely to RTS than patients with posterior instability. Even though patients with anterior instability were more likely to RTS, they still had a 1.53 times greater risk of suffering from postoperative instability. Our study also found that patients with anterior instability may have statistically significant higher ASES scores postoperatively, although this 7-point difference may not be clinically significant. Thus, our hypothesis was partially true because patients with posterior shoulder instability had less postoperative instability; however, they were also less likely to RTS. Finally, our results showed that there was no significant difference in postoperative complications when comparing anterior and posterior instability.
Our finding that patients with anterior shoulder instability have significantly better outcomes if they undergo surgery is widely supported throughout the published literature. 3,12,20,21 However, one of the limitations of our study was the lack of published studies that directly compared anterior and posterior shoulder instability. As this is the first systematic review and meta-analysis to do so, we were limited in our ability to relate some of our major results to other published literature.
The only included study that directly compared anterior versus posterior instability outcomes was the cohort study by Bernhardson et al, 4 which found that functional outcomes for 103 patients with anterior instability were statistically superior in all domains (ASES, Single Assessment Numeric Evaluation, Western Ontario Shoulder Instability Index) compared with the 97 patients with posterior instability. This was also found to be true in our results, where we found statistically significant higher postoperative ASES functional scores in patients with anterior instability. It should also be noted that the overall preoperative and postoperative ASES scores in their study were remarkably close to those in our study. Our preoperative and postoperative ASES scores for anterior instability were 57.1 and 92.8, respectively, while they found 58.0 and 94.2, respectively. For posterior stability, we found preoperative and postoperative ASES scores of 50.4 and 86.1, respectively, while they found 60.0 and 87.7, respectively. The only major difference noted here is that our study found much lower preoperative ASES scores in patients with posterior instability. This could be attributed to our larger sample size of 307 patients compared with their 97 patients.
Although the goal of our study was to find outcomes after anterior and posterior instability to effectively compare with studies such as Bernhardson et al, 4 we were limited by the fact that no other included studies directly compared anterior versus posterior instability. Further data comparing outcomes of anterior versus posterior instability are needed to better clarify this comparison.
Another topic of discussion is the wide variety of functional scores used throughout the studies included in this systematic review. There was a total of 17 different functional scores used throughout the 39 included studies, as noted in Figure 2. This wide variety made it very difficult to directly compare functional outcomes between the studies. We chose to compare ASES functional scores, as they provided the most comparable data between studies and are also accepted as a good measure of shoulder function. 2,56 The wide variation in functional tests used throughout the papers in our study certainly limited our ability to compare them in a meta-analysis. This problem of overabundance in functional tests is a commonality among other studies as well, including a meta-analysis by DeLong et al 19 looking at posterior instability. They discussed the same inability to effectively compare shoulder instability studies via meta-analysis due to the overabundance of functional tests prevalent throughout the literature and cited other studies that had the same dilemma. 57,65 This raises the need for a more well-rounded functional test that can be used throughout shoulder studies, allowing for proper comparison via meta-analysis. Additionally, although functional tests may be a good measure of postoperative outcomes, one may want to consider recurrence of instability as the best measure to delineate good versus poor outcomes in shoulder instability. However, what is considered the best measure of instability is certainly up for debate.
Limitations
We understand that our study comes with several limitations. Our study did not differentiate whether patients who underwent surgical intervention were treated nonoperatively before surgery. We also did not differentiate whether patients presented after their first traumatic event or if they had a history of multiple episodes of instability. These discrepancies could have altered patients’ postoperative outcomes from further compounding bias.
Regarding RTS, because of the limited reporting of sport type and level of competition in the current literature, we were unable to analyze how the type of sport (contact vs noncontact) or level of competition (high school, college, recreational, and professional) affected patient RTS. As the current literature has proven, these variables can largely affect a patient’s RTS prognosis. 11,43,47 This limits our overall RTS conclusion between anterior versus posterior shoulder instability. Also, because of the limited reported time to RTS, we were unable to comment on how fast patients should expect to RTS. More randomized controlled studies looking at time to RTS for patients experiencing either anterior or posterior instability would be beneficial.
Another limitation is that even though we tried to standardize our results by only including studies that treated patients with arthroscopic soft tissue repair, we still understand there can be heterogenicity in both these treatment modalities. Nonoperative treatment can differ concerning time in sling, type of sling, and type of physical therapy. Similarly, another confounding factor is that previous studies have shown that surgeons’ experience, type of fixation, and amount of fixation used can alter patients’ surgical outcomes after shoulder instability. 7 Thus, even though we tried to standardize the treatment methods, we were limited by variability within each study. We also tried to limit our review to studies that only included patients with at least 1 year of follow-up. However, there was still a wide range in time to follow-up in all variables measured. Thus, we understand there is a higher risk of rate of instability the longer the follow-up, and this can overall skew our results and weaken our conclusion.
The most notable limitation involves the small quantity of published literature regarding outcomes after posterior instability. As the main goal was to compare anterior versus posterior outcomes, the small sample size in posterior instability may be poorly representative of the entire population. However, since posterior instability is already less prevalent than anterior instability, this may not be a substantial limitation. Finally, we included many studies with a high risk of bias, likely due to the fact that only a few were randomized controlled trials. Although this may have skewed the results, we believe the large number of included studies and large cohort could correct for this issue.
Conclusion
In the current review, patients with anterior shoulder instability were associated with better outcomes with regard to RTS but were more likely to have postoperative instability compared with patients with posterior instability. Overall, men were significantly more likely to have anterior shoulder instability while women were significantly more likely to have posterior shoulder instability.
Footnotes
Final revision submitted January 6, 2021; accepted February 18, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: The article processing charges related to the publication of this article were supported by the University of Kansas (KU) One University Open Access Author Fund, sponsored jointly by the KU Provost, KU Vice Chancellor for Research & Graduate Studies, and KUMC Vice Chancellor for Research and managed jointly by the Libraries at the Medical Center and KU-Lawrence. M.L.V. has received education payments from Titan Surgical Group and hospitality payments from DePuy and Zimmer Biomet. J.P.S. has received education payments from Arthrex and consulting fees from Vericel. M.T.P. has received consulting fees from Arthrex and JRF, nonconsulting fees from Arthrex and Arthrosurface, honoraria from Flexion and JRF, and royalties from Arthrex and Arthrosurface. B.G.V. has received education payments from Titan Surgical Group, consulting fees from DePuy, and hospitality payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.