
Abstract
Background:
The surgical indications for reverse shoulder arthroplasty (RSA) have continued to expand as it continues to be effective in restoring functionality in older, less active populations. The effect of RSA on return to sport (RTS) in the athletic population has been sparsely studied.
Purpose:
To systematically review the RTS rate after primary RSA.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, a systematic review of the PubMed, Embase, and Web of Science online databases was conducted and included articles published from database inception until December 22, 2024. Inclusion criteria consisted of studies reporting on RTS after primary RSA. Rates of RTS or activity were collected. Patient-reported outcome measures (PROMs) and range of motion (ROM) data were collected when available. Delta values, the change from preoperative to postoperative values, were calculated for each PROM and ROM when available. Study quality was assessed using the Methodological Index for Non-Randomized Studies (MINORS) criteria.
Results:
Overall, 15 studies reporting on a total of 937 patients (954 shoulders) were included in this review. Mean patient age was 72.7 years (range, 68.0-76.5 years), and 58.1% were female. Mean follow-up was 40.5 months (range, 31.6-57.6 months). The RTS for the studies ranged from 48% to 100%. Swimming (n = 188 athletes) was the most reported sport, followed by golf (n = 151 athletes). Sport-specific RTS rates ranged from 50% to 100% for golf and 64% to 67% for swimming. Patients returned to a higher level of performance 11% to 74% of the time. Postoperative delta values ranged from −7 to −2.1 for the visual analog scale for pain (VAS Pain) during sport, −6.1 to −3 for VAS Pain, 24.4 to 59 for the American Shoulder and Elbow Surgeons score, and 3.8 to 8 for the Simple Shoulder Test. The mean MINORS score of the included studies was 16.8 (range, 16-19) for comparative studies and 10.0 (range, 9-11) for noncomparative studies.
Conclusion:
Our study showed that primary RSA allows for variable rates of RTS ranging from 48% to 100%, with 50% to 100% of patients returning to golf and 64% to 67% returning to swimming. Overall, patients reported improved postoperative outcomes scores and range of motion.
Reverse shoulder arthroplasty (RSA) is frequently used to treat individuals with glenohumeral osteoarthritis, rotator cuff tear arthropathy, and proximal humerus fractures. Due to its growing indications, there has been an increase in the frequency of elective RSA procedures in recent years. 59 This expansion has broadened the target population to include younger and more active adults, many who are interested in returning to their previous active lifestyles. 12 The postoperative expectations of athletes undergoing RSA have increasingly focused on achieving a successful return to sport (RTS). 27
While RSA has proven effective in restoring function in elderly populations, conflicting evidence exists regarding patients’ ability to return to preoperative levels of physical activity and sport after RSA.34,41 The minimal literature that exists demonstrates that overhead athletes and those in high-demand sports have more modest rates of return.12,16,47 Furthermore, a previous investigation found that patients undergoing anatomic total shoulder arthroplasty (TSA) had higher rates of RTS than those undergoing RSA, with the RSA cohort showing particularly low levels of complete return to athletic function. 43
As indications for RSA continue to expand, it is paramount for both surgeons and patients to thoroughly understand the likelihood of RTS for the active population. Therefore, the purpose of this study was to systematically review the RTS rate after primary RSA. We hypothesized that rates of return to sport would vary among athletes undergoing RSA.
Methods
Search Strategy and Eligibility Criteria
A systematic review of the existing literature following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines 38 was performed using the PubMed, Embase, and Web of Science online databases, examining articles published from database inception until December 22, 2024. Inclusion criteria consisted of level 1 to 4 studies published in English that reported on patients undergoing primary RSA; studies must also report RTS or athletic activity. Primary RSA was defined as the initial shoulder arthroplasty and did not preclude patients with previous ipsilateral shoulder procedures such as rotator cuff repair, labral debridement/repair, or open reduction and internal fixation. Exclusion criteria included case reports, review articles, cadaveric studies, technique articles, editorial commentaries, biomechanical studies, laboratory studies, meta-analyses, and articles not written in the English language.
The following Medical Subject Headings (MeSH) were used: (((((return to play) OR (return to sport)) OR (return to activity)) AND (RSA)) OR (RTSA)) AND (shoulder arthroplasty). Title and abstract screening were completed by 2 independent authors (B.T.L. and J.T.C.); any studies meeting initial criteria were considered for full-text screening. No disagreements between the two authors were encountered. Any duplicate studies were removed during the screening process.
Data Extraction
Upon completion of full-text screening, Excel version 16.63 (Microsoft) was used to conduct data extraction. Rates of RTS or activity were collected. Study demographics, including publication year, mean follow-up time, mean age, number of patients reported, level of sporting, and sport type, were also collected. Patient-reported outcome measures (PROMs) and range of motion (ROM) data were collected when available. The PROMs that were extracted included the American Shoulder and Elbow Surgeon (ASES) score, Simple Shoulder Test (SST), visual analog scale for pain (VAS Pain) score, and Single Assessment Numeric Evaluation (SANE) score. ROM data included external rotation, forward flexion, and internal rotation. Delta (Δ) values for PROMs and ROM were reported, defined as the change from preoperative to postoperative.
Risk of Bias Assessment
A methodological quality assessment was performed using the Methodological Index for Non-Randomized Studies (MINORS) criteria 46 by 2 independent authors (B.T.L. and C.C.M.). The MINORS criteria are a numerical scale consisting of 8 questions for noncomparative studies and 12 questions for comparative studies, with each question scored as follows: 0 if not reported, 1 if reported but inadequate, or 2 if reported and adequate. The highest achievable score for a noncomparative, nonrandomized study meeting all criteria is 16, while the highest achievable score for a comparative, nonrandomized study is 24. If a score difference ≥2 was encountered for any study between the 2 authors, a third author (G.R.J.) was consulted. No score difference ≥2 was recorded between the 2 authors.
Statistical Analysis
Given the low level of evidence and the lack of homogeneity among the studies included, data were not pooled, necessitating a descriptive analysis. Excel version 16.63 (Microsoft) was used to calculate descriptive variables such as mean, median, and range. Forest plots were generated in Spyder IDE version 5.4.3 (Anaconda) to illustrate RTS rates, with confidence intervals calculated using the binomial proportion formula to determine the standard error using the probability of returning to sport and the sample size of the study. Forest plots were also generated, illustrating the mean change and standard deviation for a PROM or ROM when reported by at least 3 studies included in this review.
Results
Study Demographics
The initial literature search yielded 3347 articles, of which 1431 duplicates were removed (Figure 1). After abstract screening, full texts were investigated for 41 studies. Overall, 15 studies* met the final inclusion criteria reporting on 937 patients (954 shoulders) (Table 1). Level of evidence of the included studies was 3 (n = 6 studies20,21,25,28,31,35) and 4 (n = 9 studies † ). The mean MINORS score of the included studies was 16.8 (range, 16-19) for comparative studies and 10.0 (range, 9-11) for noncomparative studies (Appendix Figure A1).

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) criteria.
Study Demographics a

aTSA, anatomic total shoulder arthroplasty; BL, bilateral; BMI, body mass index; CTA, cuff tear arthropathy; GHOA, glenohumeral osteoarthritis; L, left; LOE, level of evidence; NR, not reported; OA, osteoarthritis; ORIF, open reduction internal fixation; PHF, proximal humerus fracture; R, right; RA, rheumatoid arthritis; RCR, rotator cuff repair; RCT, rotator cuff tear; TSA, total shoulder arthroplasty.
Denotes a specific ipsilateral shoulder procedure not reported.
Denotes a value that corresponds to the entire study cohort, not just the population of interest.
Sex demographics of the studies included 353 (41.9%) men and 490 (58.1%) women (1 study 21 did not report sex [n = 94 patients]). The mean age of the cohort was 72.7 years (range, 68.0-76.5). The mean follow-up across 14 studies was 40.5 months (range, 31.6-57.6 months) (2 studies40,51 did not report mean follow-up). The mean body mass index of the included studies ranged from 25.3 to 29.7 kg/m2. Surgical indications were reported by 11 studies. ‡ All 9 studies § that reported surgical approach employed the deltopectoral approach. Implant type was reported in 10 of the included studies. ‖ Previous ipsilateral shoulder surgery occurred in 4% to 74% of patients (n = 5 studies18,20,40,45,47), with the most common procedure being rotator cuff repair, which occurred in 20.0% to 24.5% of patients.
RTS
The RTS rates were reported by all 15 studies, with rates ranging from 48% to 100% (Figure 2, Table 2). Level of competition of the included athletes was reported by 8 studies,5,18,20,21,25,45,51,54 with all athletes categorized as recreational (n = 331 athletes). All studies reported sport type, with swimming (n = 188 athletes) being the most common, followed by golf (n = 151 athletes), fitness (n = 72 athletes), and tennis (n = 61 athletes). Sport-specific RTS rates in the reporting studies ranged from 50% to 100% for golf5,18,28,51 and 64% to 67% for swimming.18,35 Mean time to RTS ranged from 3.0 to 9.1 months (n = 4 studies18,20,25,35). Patients returned to a higher level of performance from 11% to 74% of the time, the same level from 21% to 78% of the time, and a lower level from 5% to 50% of the time. Reasons for not returning to sport included persistent pain, limited range of motion, weakness, and concerns unrelated to the operative shoulder. Postoperative enjoyment of sport increased from 22% to 71% of the time, stayed the same from 29% to 67% of the time, and decreased from 9% to 22% of the time (n = 4 studies5,35,51,54).
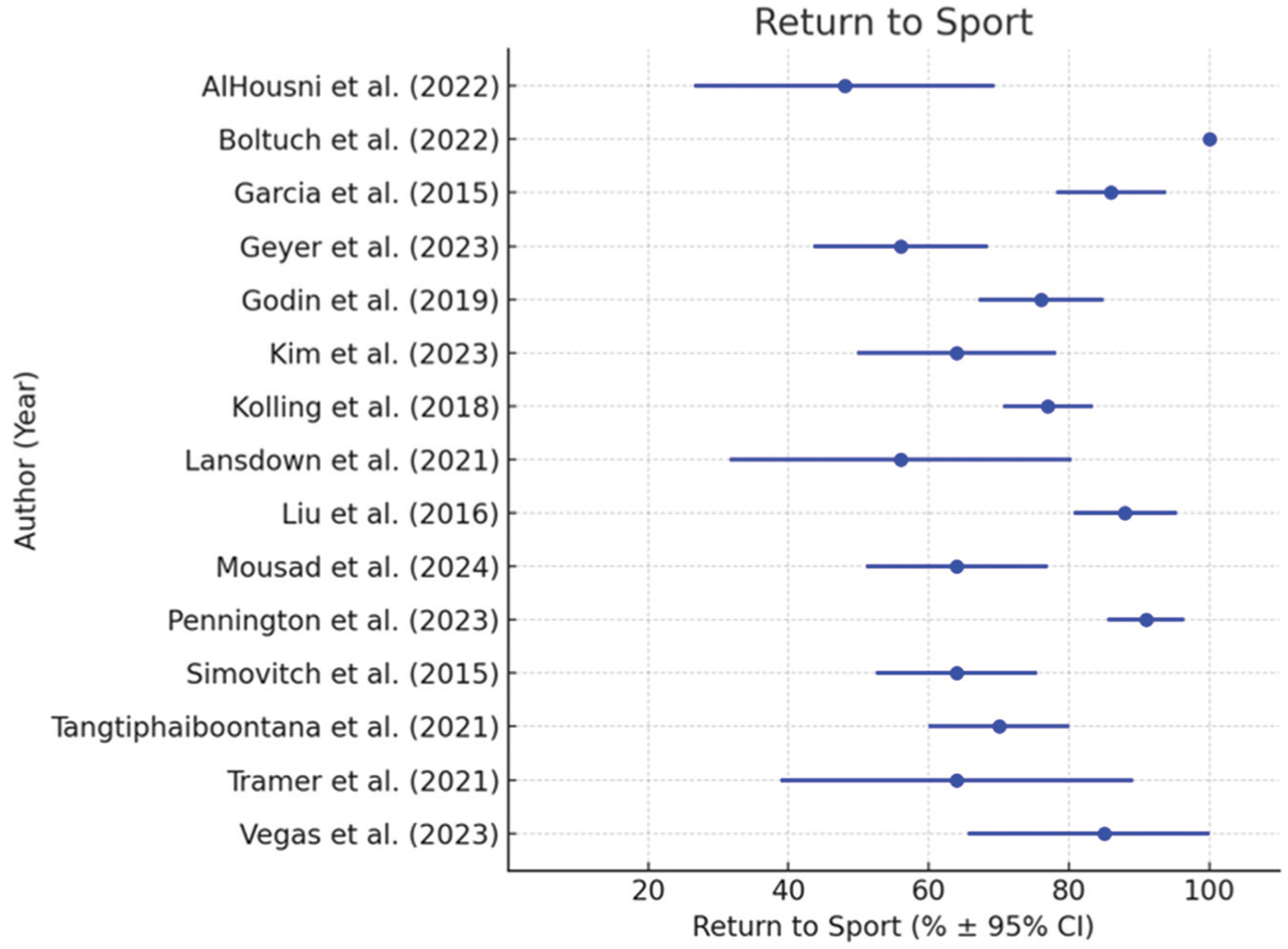
Return to sport.
Return to Sport a

NR, not reported; ROM, range of motion; RSA, reverse shoulder arthroplasty; RTS, return to sport.
Patient-Reported Outcomes
Overall, PROMs were reported by 11 studies, ¶ with the most commonly reported score being ASES (n = 9 studies # ), followed by VAS Pain (n = 8 studies5,18,20,21,25,35,40,45), VAS Pain during sport (n = 5 studies5,20,35,51,54), SST (n = 4 studies5,20,25,35), and SANE (n = 4 studies5,21,35,40) (Table 3). Postoperative delta (Δ) values ranged from −7 to −2.1 for VAS Pain during sport, 24.4 to 59 for ASES (Figure 3), 3.8 to 8 for SST, 33 to 70 for SANE, and −6.1 to −3 for VAS Pain (Figure 4).
Patient-Reported Outcomes a

P < .05 is considered significant. ASES, American Shoulder and Elbow Surgeons; NR, not reported; Post, postoperatively; Pre, preoperatively; SANE, Single Assessment Numeric Evaluation; SST, Simple Shoulder Test; VAS, visual analog scale; Δ, delta.
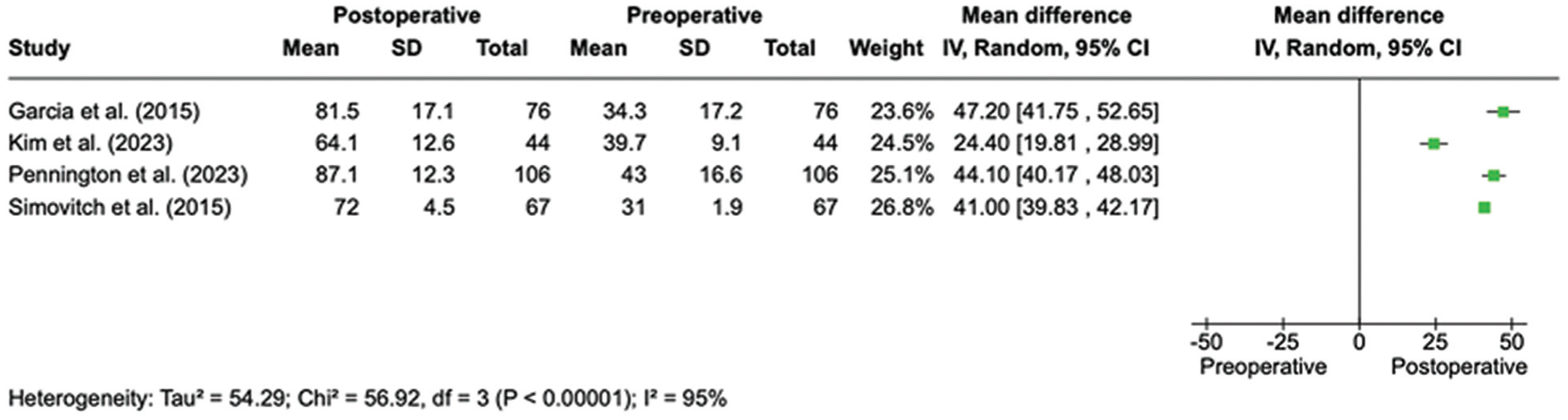
Forest plot illustrating mean change in American Shoulder and Elbow Surgeons (ASES) score from pre- to postoperative assessment.

Forest plot illustrating mean change in visual analog scale for pain (VAS Pain) from pre- to postoperative assessment.
ROM
Shoulder ROM was reported by 7 studies, with external rotation (n = 7 studies5,20,21,25,35,40,45) being the most reported, followed by forward flexion (n = 5 studies5,20,25,40,45) and internal rotation (n = 5 studies5,25,35,40,45) (Table 4). Delta (Δ) values ranged from 23° to 74° for flexion (Figure 5), −2.8° to 27° for external rotation (Figure 6), and 0° to 2.5° for internal rotation. Two studies35,45 reported internal rotation using anatomic landmarks instead of degrees.
Range of Motion a
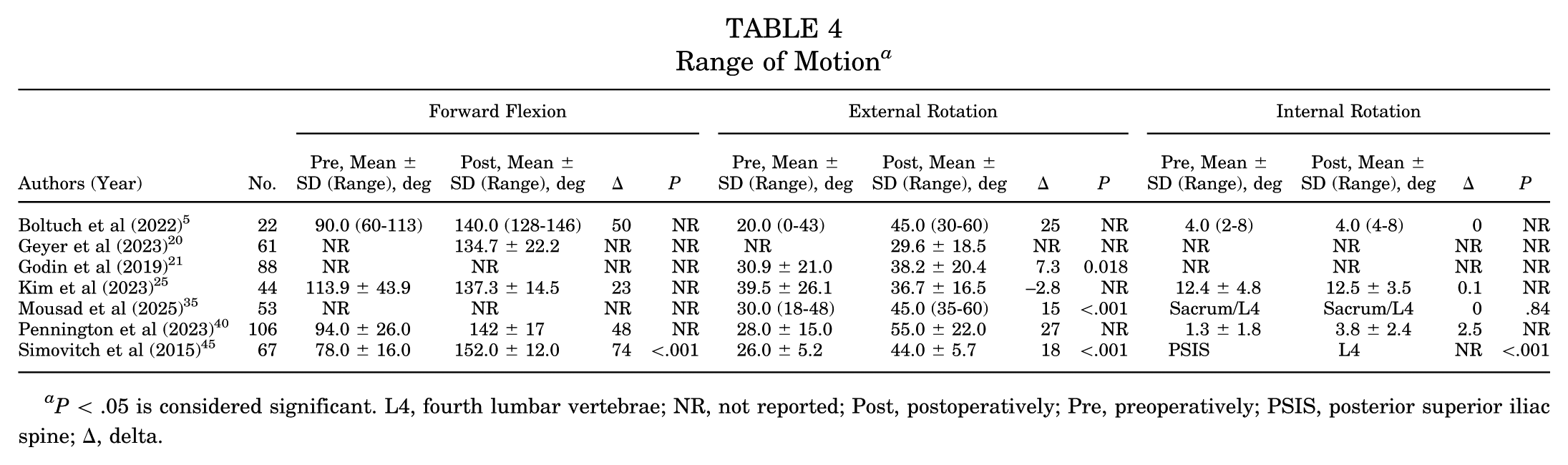
P < .05 is considered significant. L4, fourth lumbar vertebrae; NR, not reported; Post, postoperatively; Pre, preoperatively; PSIS, posterior superior iliac spine; Δ, delta.

Forest plot illustrating mean change in forward flexion from pre- to postoperative assessment.

Forest plot illustrating mean change in external rotation from pre- to postoperative assessment.
Discussion
The major findings of this systematic review demonstrated that patients who undergo primary RSA may experience variable rates of RTS ranging from 48% to 100%, with 50% to 100% of patients returning to golf and 64% to 67% returning to swimming. Furthermore, the patients experienced improvements in PROMs and ROM. These outcomes highlight the ability of RSA to restore function and alleviate pain, especially in the active population.
Recreational activities like golf and swimming are generally less demanding on the shoulder joint.18,32 These sports involve lower levels of repetitive overhead motion and less intense physical exertion, which makes them more compatible with the functional limitations of the reverse prosthesis.12,26 For instance, in a systematic review by Davey et al, 12 the authors found that 66.7% of golfers and 74.3% of swimmers returned to their sports, compared with only 50% of tennis players, highlighting the biomechanical constraints of RSA in higher-demand sports. While their review reported an overall RTS rate of 79.1%, they did not assess PROMs or ROM outcomes, which may have provided a more comprehensive picture of recovery. High-demand, overhead sports such as tennis and weightlifting place significant stress on the shoulder joint, requiring greater strength, ROM, and stability. These demands can be challenging to meet post-RSA due to the biomechanical constraints of the reverse prosthesis.11,57 The reverse prosthesis is designed to improve stability and function in the absence of a functional rotator cuff, but it often results in limited rotational movements and strength, particularly in external rotation and abduction.1,12,26 The RSA changes the shoulder's center of rotation, which improves deltoid function at the expense of limiting the ability to perform high-demand activities. 33 High-demand activities, particularly those requiring significant external rotation and overhead motion, remain challenging due to the limited rotational capacity of the reverse prosthesis.4,37 This is supported by findings that overhead athletes, such as tennis players, have lower RTS rates (50%) due to these biomechanical constraints. 12
Our findings also indicate a positive relationship between improved PROM scores and the likelihood of RTS. For instance, Mousad et al 35 reported significant gains in postoperative ASES (59 points) and SST scores (8 points), which coincided with high RTS rates in lower-demand sports like swimming. This suggests that improvements in pain, strength, and functional capacity play important roles in successful RTS after RSA.18,20,55 Psychological factors, such as fear of reinjury or lack of confidence in the shoulder, may also play a role in limiting RTS rates.9,42 Addressing this through patient education and gradual exposure to sport-specific movements during rehabilitation could improve outcomes and speed up recovery time.6,8,18,55 However, limited reporting on factors such as time to RTS and reasons for not returning to sport prevents a more comprehensive understanding of recovery times. 30
Although the included studies reported improvements in PROMs, it is important to consider their clinical significance regarding the minimal clinically important difference (MCID). The MCID is defined as the smallest improvement in a score that patients perceive as beneficial and clinically meaningful.10,23 For example, the MCID for the ASES score after RSA is typically 12 to 17 points,48,56 a threshold exceeded in most studies included in this review, such as Mousad et al, 35 in which a 59-point improvement was reported. Similarly, SST improvements ranging from 6 to 8 points consistently exceeded the MCID of 2 points, indicating that patients experienced meaningful functional gains.50,58
While the SST and ASES scores did achieve the MCID, rotational improvements often failed to meet their respective MCID thresholds. For instance, Kim et al 25 reported a minimal improvement of 0.2 points for internal rotation, while external rotation decreased by 2.8 points, falling short of the MCID of 2 points, which has been previously established. 44 Mousad et al 35 also reported no meaningful improvement in internal rotation, with patients maintaining function at the “sacrum/L4” level postoperatively. Strength improvements, although statistically significant in some studies, also frequently fell below the MCID threshold of 11.5 points. 50 The failure of rotational and strength improvements to consistently meet their respective MCID thresholds despite some statistically significant results emphasizes the importance of considering patient-specific factors such as age, body mass index, and preoperative functional status, which can significantly influence postoperative outcomes.2,15,17,49,56 Younger, more active patients may achieve higher RTS rates due to better baseline function and greater capacity for rehabilitation, whereas older patients may face greater challenges.8,17,20,29 Sex differences also play a role, as highlighted by Mowers et al, 36 who reported that male and female patients experience similar improvements in PROMs and ROM after RSA, although male patients have significantly higher revision rates. While RSA reliably improves forward elevation, its effect on strength and rotational capacity remains limited, which may influence RTS rates, particularly in high-demand sports.12,45 However, it must be noted that return to acceptable athletic functionality is not uniform among athletes of all ages, as elderly populations are often engaging in less demanding iterations of the same sports as their younger counterparts. The mean patient age of the included studies was 72.7 years (range, 68.0-76.5 years), indicating an older athletic population. Thus, 1 explanation for the discrepancy in meeting the MCID for certain functional outcomes (eg, SST, ASES) yet not others (eg, rotation, strength) is that athletic functionality in elderly patients is limited more by pain than objective functional deficit of the shoulder. Acknowledging the clinical necessities and differences in functional demands between young and old athletic populations in returning to their respective sports emphasizes the need for tailored rehabilitation protocols and treatments to address specific patient needs and optimize outcomes.
Regarding range of motion, the present study found that RSA provided minimal improvement in internal rotation (Δ, 0° to 2.5°). Persistent functional deficit in internal rotation is a known limitation of RSA when compared with TSA.19,24,53 In athletic populations, a lack of internal rotation may provide difficulty in performing movements reliant on this motion, such as throwing, swimming pull-through, tennis serve, and the generation of clubhead speed in golf.7,14,22,52 Persistent deficit of internal rotation in athletes who partake in these sports may diminish their ability to return to their previous playing ability. Surgeons must make their athletes, considering RSA, aware of these potential limitations and provide sport-specific counseling regarding how limited internal rotation may impact certain movements.
A previous meta-analysis by Papalia et al 39 demonstrated that despite worse ROM outcomes, TSA (90%) (95% CI, 0.80-0.99; P < .01) demonstrated a clinically greater, yet not statistically significant, difference in RTS rates to RSA (77%; 95% CI, 0.69-0.85; P < .01). While swimming demonstrated the highest RTS rate (84%) across both RSA and TSA, sports such as golf (77%) and tennis (69%) exhibited much lower rates of return. 39 While ROM is a limitation of RSA, the specific biomechanics of each individual sport may be a greater influence on RTS. One possible hypothesis is that the relatively higher velocity of the tennis stroke and golf swing places a greater physiologic demand on the glenohumeral joint and thus makes them less able to tolerate shoulder arthroplasty compared with the pull phase of a swimming stroke. Overall, a persistent deficit in internal rotation after RSA in athletes who partake in these sports may severely diminish their ability to return to their previous playing ability, but this complication seems to be sport- and patient-specific. Surgeons must make their athletes, considering RSA, aware of these potential limitations and provide sport-specific counseling regarding how limited internal rotation may affect certain movements. Future studies must further characterize how TSA and RSA, respectively, affect RTS rates in various sports, as the current literature is inconclusive despite biomechanical and clinical evidence that TSA would provide better outcomes due to less limited internal rotation.19,24
The definition of RTS demonstrates a binary split in methodology across the included studies. While 13 studies relied on asking patients to complete self-reported questionnaires or direct patient questioning (eg, Were you able to return to your sport?), only 2 studies20,25 applied stricter definitions of what constituted a true return to sport. Kim et al 25 defined RTS as “participating in sports at least once per week,” while Geyer et al 20 used the definition of “resumed at least one sport for more than two hours per week after RSA.” The variability of what qualified as returning to sport stems from a lack of specific criteria in most included studies. Previously, Doege et al 13 described the degree to which definitions of RTS vary across the available literature. The authors found that many studies defined RTS as returning to training/practice, general competition, or a specific competition level. Unfortunately, these more specific definitions are not as applicable to the present study as many of the athletes were recreational or hobbyists, making it difficult to define what constitutes a “game” or “training.” Doege et al 13 suggested that more precise examinations of the recovery process be used, such as “return to participation” and “return to previous level of performance.” The standardization of reporting more precise definitions of the recovery process after RSA in future studies allows for more accurate comparisons across studies, and the precise definitions would allow surgeons to set more realistic expectations for athletes after RSA.
Limitations
This systematic review has several limitations. First, the studies included primarily consisted of level 3 and 4 evidence, along with significant heterogeneity among the included studies in terms of patient populations, sports-specific outcomes, and follow-up duration. These factors prevented data pooling and limited the ability to perform a meta-analysis. Second, the studies included had varying definitions of RTS. Some studies considered any level of activity resumption as RTS, while others required a return to preoperative levels of performance, introducing variability in reported rates. Furthermore, detailed reporting on sport-specific outcomes was limited, particularly for overhead or high-demand athletes. Lastly, the studies included had a relatively short mean follow-up period (range, 31.6-57.6 months). This may underestimate the long-term durability of RTS.
Conclusion
Our study showed that primary RSA allows for variable rates of return to sport, ranging from 48% to 100%, with 50% to 100% of patients returning to golf and 64% to 67% returning to swimming. Overall, patients reported improved postoperative outcomes scores and range of motion.
Footnotes
Appendix
Final revision submitted September 10, 2025; accepted October 6, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.J.S. is a board or committee member of the American Shoulder and Elbow Surgeons; is an editorial or governing board member of Current Orthopedic Practice; receives royalties from DePuy, A Johnson & Johnson Company, and Ignite Orthopedics; is a paid consultant for DePuy, A Johnson & Johnson Company; is a paid presenter or speaker for DePuy, A Johnson & Johnson Company; and holds stock or stock options in Ignite Orthopedics. K.K. is involved in other professional activities with the American Orthopaedic Association, American Shoulder and Elbow Surgeons, Southern Orthopaedic Association, American Orthopaedic Society for Sports Medicine, The Orthopaedic Journal of Sports Medicine, The American Journal of Sports Medicine, and American Board of Orthopaedic Surgery; is a board or committee member of American Orthopaedic Association, American Shoulder and Elbow Surgeons, and American Board of Orthopaedic Surgery; is Associate Editor of The Orthopaedic Journal of Sports Medicine; and is an editorial or governing board member of The American Journal of Sports Medicine and The Orthopaedic Journal of Sports Medicine. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.