
Abstract
Context:
Reverse shoulder arthroplasties (RSAs) have become significantly more common in recent decades, and shoulder arthroplasties are increasingly performed on younger, active patient populations. However, the body of evidence evaluating return to sport after RSA is limited.
Objective:
To evaluate the rates of return to sport after RSA as well as patient-reported outcomes for pain and function.
Data Sources:
A comprehensive search of MEDLINE, EMBASE, and CENTRAL identified studies from inception through October 10, 2023.
Study Selection:
Studies evaluating return to sport after RSA in adult patients (>18 years) were included. Reviews, meta-analyses, non-English language, and studies that did not report return to sport data were excluded. Outcomes included rates of return to sport at any level, and at the same level or higher, as well as patient-reported outcomes.
Study Design:
Systematic review.
Level of Evidence:
Level 4.
Data Extraction:
A descriptive analysis of the included studies was performed.
Results:
A total of 19 studies (3092 patients) were included. Mean patient age was 72.5 years, and most (58.8%) were female. The mean rate of return to sport at any level was 85.1% (95% CI, 84.6-85.6). The mean rate of return to the same level or higher was 69.5% (95% CI, 67.6-71.4). The mean decrease in visual analog scale pain score was 1.97, whereas ASES and CMS scores increased 64.0 and 35.5 points, respectively. All changes in patient-reported outcomes exceeded the minimal clinically important difference.
Conclusion:
This review demonstrates a high rate of return to sport after RSA, with a substantial portion of patients maintaining or exceeding their preoperative activity level. Clinically meaningful improvements in pain and function were also observed. Limitations include the predominantly retrospective study design and the high mean patient age, necessitating further research on generalizability and long-term outcomes, particularly in younger populations.
The prevalence of shoulder arthroplasty has increased significantly across the United States (US) over the last few decades. 35 Common indications for reverse shoulder arthroplasties (RSAs) include rotator cuff arthropathy, acute 3- or 4-part proximal humerus fractures, post-traumatic glenohumeral arthritis, as well as cases of failed previous shoulder arthroplasties, including hemiarthroplasties and anatomic total shoulder arthroplasties. 14 The goal of RSA surgery is to decrease pain, improve shoulder motion and strength, and increase quality of life. 12 Surgeons have utilized RSA significantly more frequently over the past decade, and this trend is driven by factors such as improved implant design and surgical techniques as well as an expansion in the eligibility of patients for this procedure. Improved implant design allows implants to offer improved function and durability and RSA survival rates have exceeded 85% within 10 years.12,15 These findings can give surgeons greater confidence when utilizing RSA, leading to a broader application of the procedure.
Furthermore, shoulder arthroplasty has been increasingly used in younger, active populations, with one-third of shoulder replacements performed in the US being in patients who are <65 years old.13,16 Whereas patient expectations in older populations may have been limited to decreasing pain and improved daily function, younger patients are more likely to have more aggressive functional objectives, such as returning to sporting activity after the surgery. 16 Although there are many studies evaluating return to sport (RTS) after hip and knee arthroplasties with a satisfactory rate of return, the body of evidence evaluating RTS after RSA is limited. 25 Furthermore, existing systematic reviews evaluating RTS focus primarily on anatomic total shoulder arthroplasty, 8 highlighting a critical knowledge gap with regard to RSA. 8 This gap necessitates a dedicated review to address the specific needs and considerations of younger, active, patients undergoing RSA.
This review aims to determine the rate of return to any level of sport after RSA as well as RTS at the same level or above. This information will aid in informing clinicians and patients about the probability of returning to sport as well as the level of sports participation that may be plausible after an RSA. We hypothesize that the majority of patients will return to sporting activity with a moderate rate of return to the preoperative level of sport.
Methods
This review was performed according to the guidelines set out by the Cochrane handbook and is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines. 23
Comprehensive Search Strategy
EMBASE, MEDLINE, and CENTRAL were searched from inception to October 10, 2023. Search terms included “return to activity,” “arthroplasty,” and “return to sport” (see Table 1 and Online Appendix for full search strategy). The inclusion criteria are outlined as follows: (1) studies on RSA evaluating RTS, (2) adult patients with no age restriction (>18 years), and (3) randomized or nonrandomized studies. Exclusion criteria were (1) reviews of the literature, (2) meta-analyses, (3) studies that did not report on RTS, (4) non-English language studies, and (5) case reports. If there was a conflict regarding the eligibility of a study, the senior author was consulted.
Overview of included studies
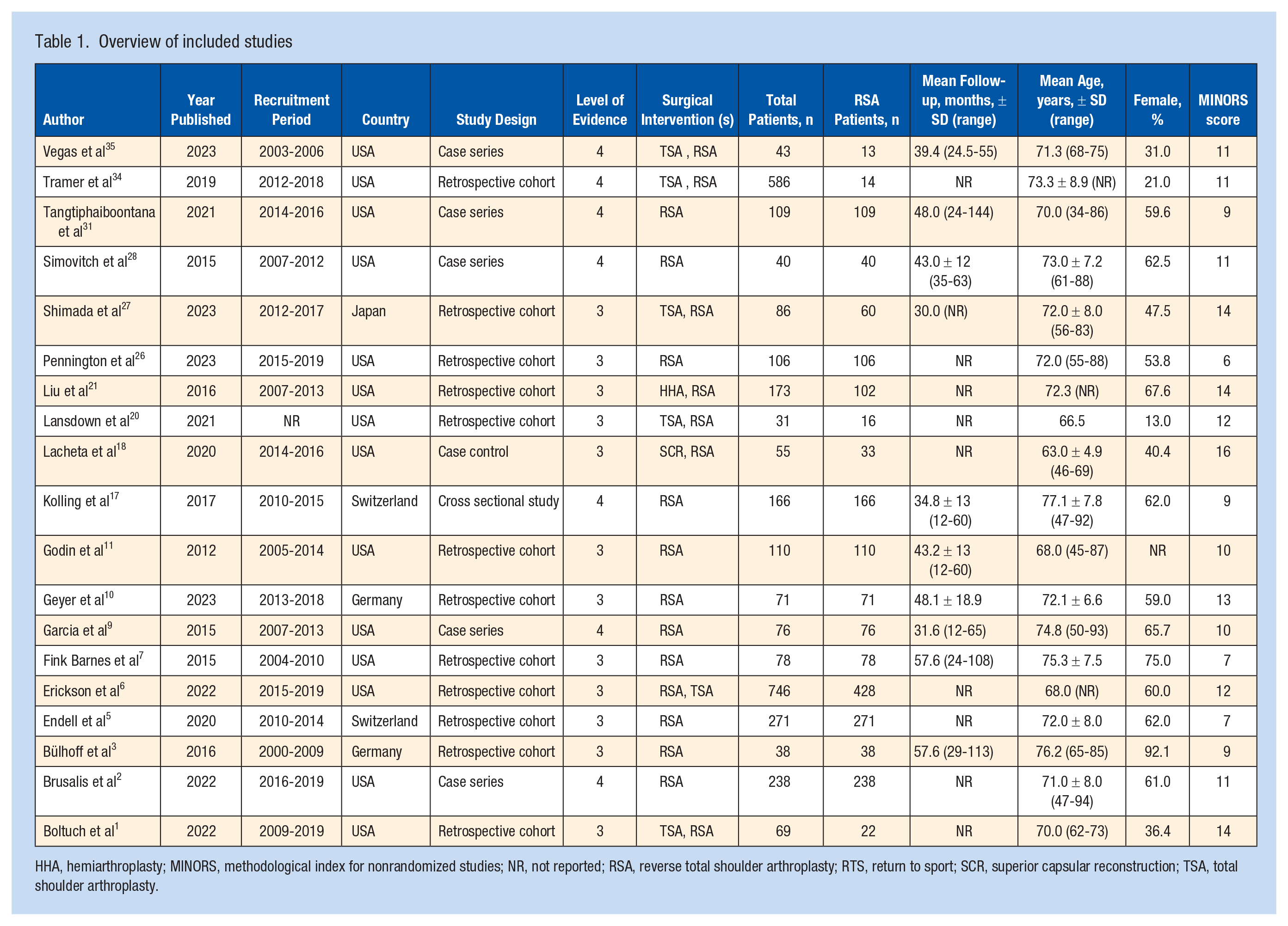
HHA, hemiarthroplasty; MINORS, methodological index for nonrandomized studies; NR, not reported; RSA, reverse total shoulder arthroplasty; RTS, return to sport; SCR, superior capsular reconstruction; TSA, total shoulder arthroplasty.
Study Screening
All titles and abstracts were screened by 2 reviewers to identify eligible studies. Disagreements were advanced to the full-text review. Conflicts after the full-text stage were resolved by consulting the senior author. After each screening stage, inter-rater reliability for study eligibility was calculated through a Kappa (k) score to determine the level of agreement between reviewers. The categorization of k scores was defined in accordance with previously established thresholds. 19
Quality Assessment
The methodological index for nonrandomized studies (MINORS) was used to assess the quality of included papers. 29 Two authors independently assessed the quality of each study using the MINORS questionnaire, which consists of 8 items for noncomparative studies, and 4 additional items for comparative studies. Each item can be assigned a maximum of 2 points if it is reported adequately, 1 point if reported inadequately, and none if not reported at all. Comparative studies can have a maximum score of 24, and noncomparative studies can have a maximum score of 16.
Data Abstraction From Included Studies
Two reviewers independently abstracted data from half of the included studies, while also verifying the accuracy of the other author’s data abstraction. Data were abstracted into a Google Sheets spreadsheet designed a priori. Data abstracted included the following: study characteristics, patient demographics, surgical interventions, follow-up length, number of shoulders at final follow-up, sporting activity levels, RTS at same level or above, RTS at any level, and patient-reported clinical outcomes. The level of evidence for all studies was determined based on the American Academy of Orthopaedic Surgeons (AAOS) Evidence Based Practice Committee guidelines. 37
Outcomes of Interest
Outcomes of interest included rate and level of RTS after RSA, and patient-reported outcomes assessed using the Constant-Murley Shoulder Outcome Score (CMS), American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Score (ASES), and Visual Analog Scale (VAS) Score for pain. RTS rates were also stratified by patient age, specifically, in patients ≤70 years old and in patients >70 years old.
Statistical Analysis
Descriptive statistics were calculated using Microsoft Excel. These included weighted means, 95% CI, and standard deviations, as appropriate.
Results
Study Characteristics and Quality
The initial search identified 1105 studies, with 889 remaining after the removal of duplicates (Figure 1). A total of 19 studies were included in the final analysis (Table 1).1 -3,5 -7,9 -11,17,18,20,21,26 -28,29,34,35 Both the title/abstract and full-text stages had substantial agreement 0.805 (95% CI 0.730-0.876) and 0.704 (95% CI 0.534-0.873, respectively). The mean MINORS score was 9.0 for noncomparative studies and 13.1 for comparative studies.
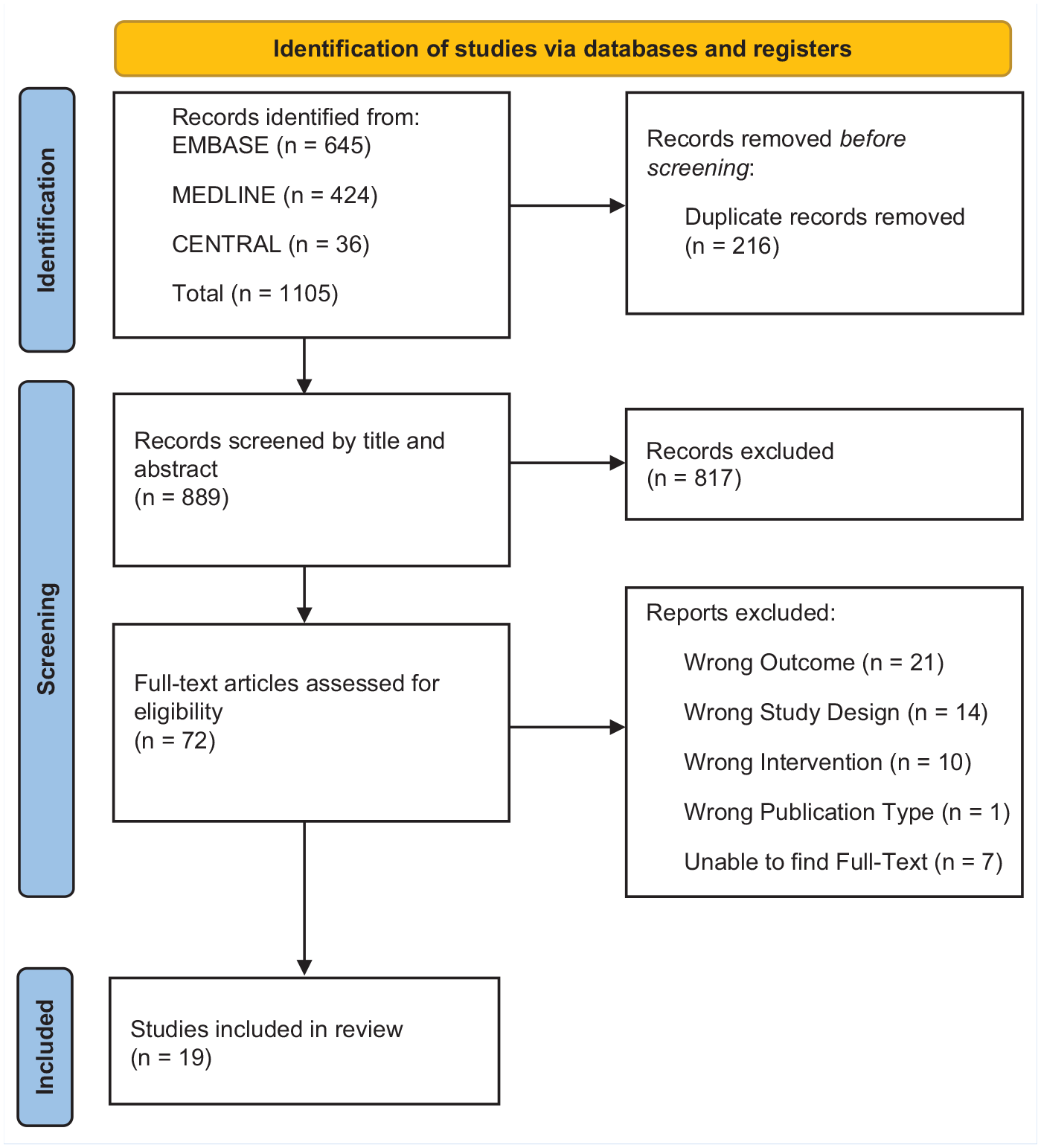
PRISMA flow diagram. Taken from Page et al. 24 For more information, visit: http://www.prisma-statement.org/.
A total of 1844 shoulders were included, with a mean age of 72.5 years, and 58.8% of patients were female. The mean follow-up period was 43.7 months with the mean loss to follow-up being 7.4%.
Return to Sport
The overall rate of RTS at any level after RSA across all studies was 85.1% (95% CI 84.6-85.6) for the 1844 shoulders at the final follow-up (Table 2). Of the 19 studies included for analysis, 11 reported RTS at the same level or higher.9,10,17,19,21,26-27,34,35 The rate of RTS at the same level or higher before surgery was 69.5% (95% CI 67.6-71.4) across studies that reported this metric at final follow-up (Online Appendix Tables a1 and a2).
RTS outcome rates
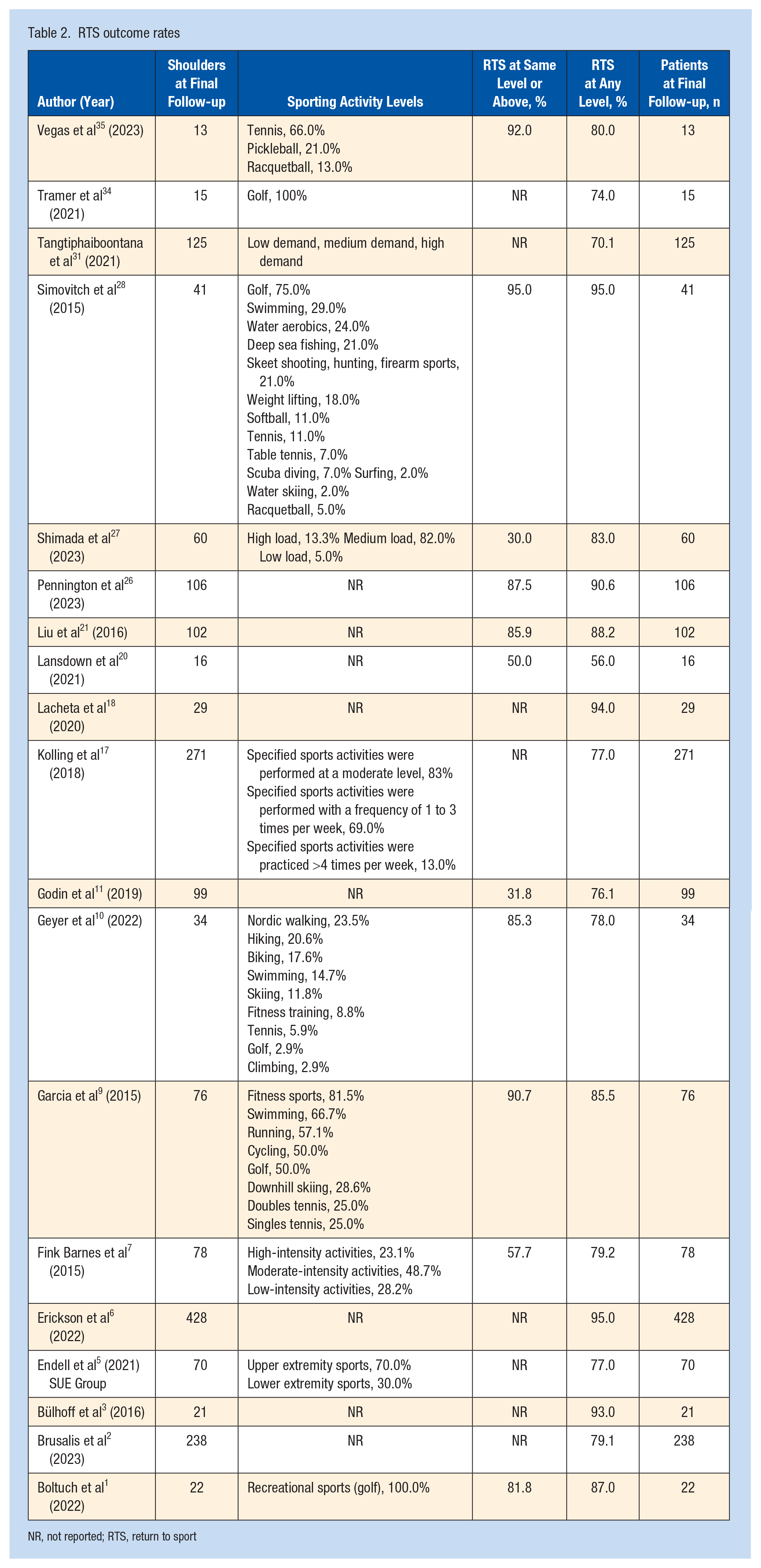
NR, not reported; RTS, return to sport
Five studies reported on RTS at any level in patients aged ≤70 years.1,6,10,20,30 Subgroup analysis demonstrated a mean RTS in this patient population of 88.4% (95% CI 74.8-94.1). Conversely, 13 studies reported a mean rate of RTS to any level in patients older than 70 of 81.5% (95% CI 78.7-87.3).17,21,26,27,30,34,35
Further, 6 out of 19 studies reported RTS rates stratified by activity intensity wherein RTS rates to high-intensity activities ranged from 23.1% to 62.9%, and to low/moderate intensity activities (grouped for ease of reporting) from 50.0% to 87.0%.1,7,17,27,31,34 However, it was possible to determine RTS by activity intensity for only 5 out of 6 studies.1,7,27,31,34
Patient-Reported Outcomes
Visual analogue scale evaluating pain after surgery was reported by 6 studies (Table 3). Preoperative and postoperative VAS pain scores were 5.73 (95% CI, 5.66-5.80) and 3.76, (95% CI, 3.61-3.91), respectively. Mean decrease VAS pain scores across studies was 1.97. Eight studies reported the ASES score (Table 3). Mean preoperative scores were 18.3 (95% CI, 17.2-19.3) and postoperative score was 82.3 (95% CI, 81.8-82.7). Mean increase of ASES score across all studies was 64.0 points. Constant-Murley score was reported by 5 studies (Table 3). Mean preoperative scores was 35.5 (95% CI, 33.5-37.5) and postoperative score was 73.8 (95% CI, 72.5-74.0). CMS scores increased across all studies with a mean increase of 38.4.
Patient-reported outcomes
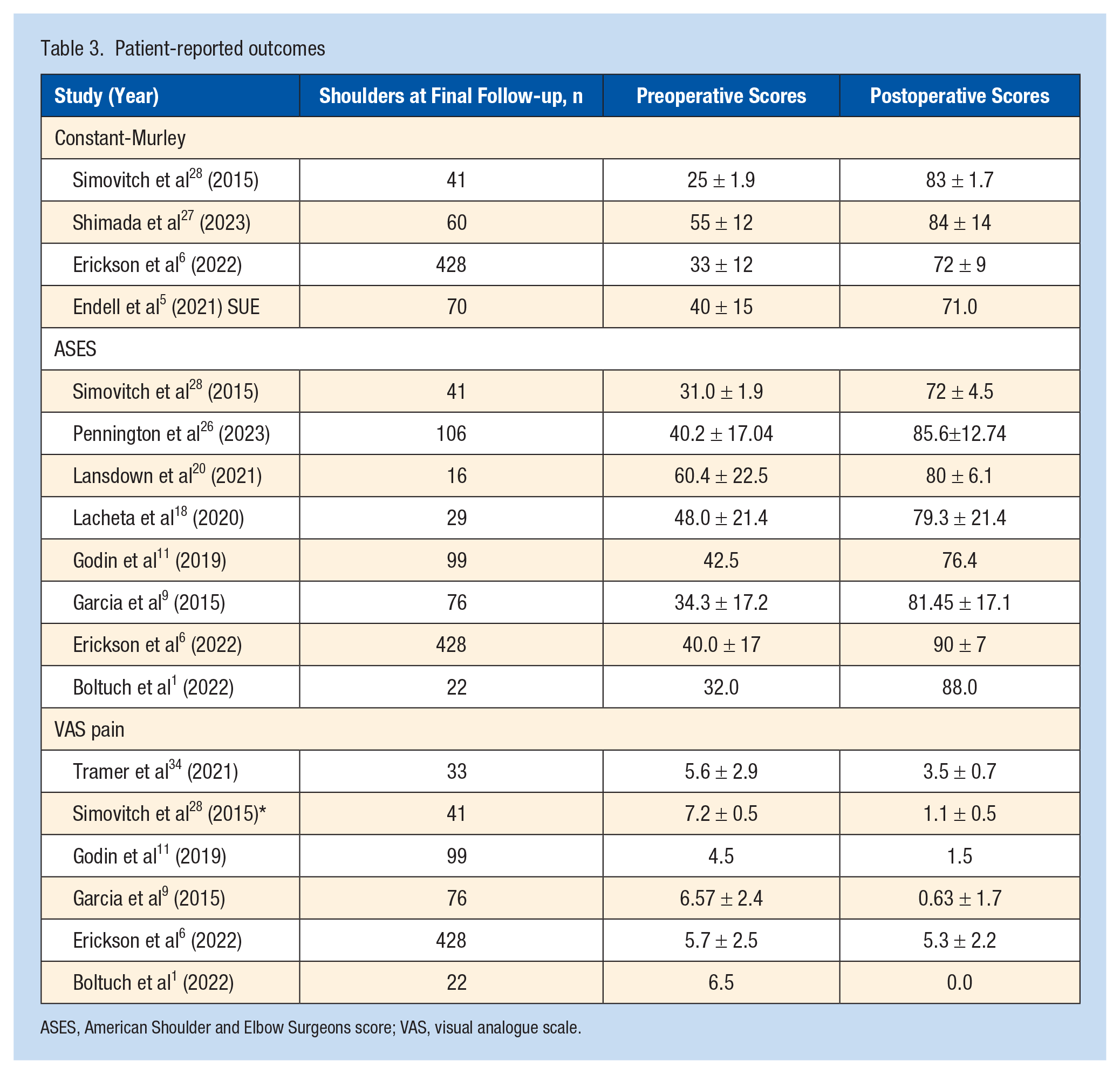
ASES, American Shoulder and Elbow Surgeons score; VAS, visual analogue scale.
Discussion
This is the largest systematic review to date evaluating RTS after RSA, with the inclusion of 19 studies. The primary finding of this study was that a large proportion of patients were able to RTS after RSA, with younger patients having a slightly higher RTS rate. Second, patient-reported outcomes all favorably improved after RSA with minimally clinically important differences (MCIDs) being surpassed. Ultimately, the findings show success in enabling older adults to resume athletic activities postsurgery along with improvements in pain and function, indicating promising prospects for those seeking to RTS after RSA.
This study observed a high rate of RTS after RSA, even amongst a patient population with a preponderance of older people. Although lower than the mean RTS after TSA, which was 92.6% in the paper by Liu et al, 22 our overall mean of 85.1% for RTS is comparable with the mean of 85.1% for all types of shoulder arthroplasty as reported by Liu et al. 22 The lower rate of RTS for RSA is expected, as patients undergoing TSA inherently have better shoulder function and stability due to the presence of a functional rotator cuff. 23 Our findings on RTS are consistent with previous research as a systematic review by Franceschetti et al 8 demonstrated a high RTS rate after RSA, with 79% of patients returning to sport. The mean return to the same level of sport or higher was 69.5%, which suggests that a substantial portion of patients, despite their age, can potentially maintain or even improve their preoperative athletic performance after undergoing RSA. These results are lower than those of Franceschetti et al, 8 who showed that 94.8% of patients returned to sport at the same level or at an improved level after RSA. 8 However, not all included studies reported on the rate of RTS at the same level or above as only 647 shoulders were evaluated for the level of return.
Subgroup analysis by patient age demonstrated that patients <70 years of age had a higher RTS rate compared with the original unstratified group, whereas patients >70 years had a lower rate, but this difference between groups was not significant. However, it is important to note that, although 5 studies reported on RTS at the same level or above for the older subgroup, only 2 studies included patients in the younger subgroup and also reported on RTS at the same level or above. This limitation restricts a more meaningful analysis comparing rates of RTS at the same level or above in older versus younger patients. Further studies with a larger sample size specifically targeting this younger demographic are necessary to draw more definitive conclusions.
VAS scores demonstrated a clinically meaningful decrease in pain postsurgery, with a mean decrease of 1.97 points, which exceeded the MCID of 1.4 points. 31 However, the VAS improvement to 3.76 is higher than typically seen in the literature. We speculate that this may be because of the patient demographics included in this study. This study involves a higher percentage of female participants (58.8%) compared with male and this has been associated with worse postoperative VAS pain scores. 33 Further, the study with the greatest decrease in pain score had the smallest sample size (1), whereas the study with the smallest decrease in pain score had the largest sample size (6). A small sample size is more susceptible to the influence of extreme values or outliers. If a few participants in a small sample experience a significant benefit or lack thereof from the treatment, it can inflate the effect size. 30 Scores on the CMS and American Shoulder and ASES assessments increased after surgery. The mean increase in CMS scores was 38.4 points, and the mean increase in ASES scores was 64.0 points, which also met the MCID. Specifically, these MCIDs ranged from 5.7 to 9.4 points for CMS and from 6.3 to 20.9 points for ASES in those undergoing shoulder arthroplasty.4,32 These outcomes results further highlight the broader benefits of RSA for patients beyond just athletic participation. Improved pain scores and functional outcomes can translate to a better quality of life and potentially a return to various activities beyond just competitive sports.
This study was not without its limitations. First, all included studies were either Level 3 or 4 evidence, and the majority of studies were retrospective in nature. The second limitation of this review concerns the lack of detailed information on the types of sports in which patients participated. The studies included likely exhibited variance in the specific sports reported. In addition, there were incomplete data, with some studies not collecting or reporting specific sports participation details. This missing information renders it difficult to discern the level of athletic demand associated with RTS across the studies. The third limitation is the relative concentration of procedures in the US as 70% of all RSA patients originated from the US; this geographic distribution of the population may also limit the generalizability of the findings to other countries. Further research in different countries with varying healthcare systems and population needs should be conducted.
Conclusion
This review demonstrates a high rate of RTS after RSA, with a substantial portion of patients maintaining or exceeding their preoperative activity level. Clinically meaningful improvements in pain and function were also observed. Limitations include the predominantly retrospective study design and the high mean patient age, necessitating further research on generalizability and long-term outcomes, particularly in younger populations.
Supplemental Material
sj-docx-1-sph-10.1177_19417381251343083 – Supplemental material for Return to Sport After Reverse Shoulder Arthroplasty: A Systematic Review
Supplemental material, sj-docx-1-sph-10.1177_19417381251343083 for Return to Sport After Reverse Shoulder Arthroplasty: A Systematic Review by Aanya Singh, Victoria Cho, Hassaan Abdel Khalik, Danielle Dagher, Ujash Sheth and Moin Khan in Sports Health
Footnotes
The authors declare the following conflicts of interest: M.K. is a paid Associate Editor for Sports Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.