
Abstract
Background:
Although several studies report the incidence of musculoskeletal injuries in ballet dancers, few studies evaluate return to dance (RTD) after surgery.
Purpose:
To describe characteristics of professional ballet dancers who underwent surgery for musculoskeletal injuries/pathologies and to report their RTD, physical health, and mental health.
Study Design:
Case series; Level of evidence, 4.
Methods:
The records of all professional ballet dancers registered at the Opéra de Paris in September 2024 were reviewed to identify dancers who had undergone surgeries (excluding infiltrations and injections) to treat musculoskeletal injuries/pathologies. A questionnaire was completed, including RTD data, pain at the operated site, satisfaction with surgery, University of California–Los Angeles activity score, and 12-item Short-Form Health Survey (SF-12). Descriptive statistics were used to summarize the data.
Results:
Of 165 registered professional ballet dancers, 18 had undergone at least 1 surgery during their professional career, and all 18 responded to the questionnaire. The cohort comprised 11 women and 7 men who had undergone a total of 31 surgeries (only 1 unrelated to dance), with a mean age at time of surgery of 30.7 ± 6.2 years (range, 18-42 years). There were 13 knee procedures, 8 foot/ankle procedures, 5 hip procedures, 3 hand/wrist procedures, and 2 thoracolumbar procedures. All 18 dancers eventually returned to dance (100%) at 7 ± 4 months (range, 1-17 months). At 83 ± 67 months (range, 11-305 months) after surgery, pain at the operated site was 1.6 ± 2.4 (range, 0-8), satisfaction with surgery was 8.3 ± 3.4 (range, 0-10), UCLA activity score was 9.1 ± 1.5 (range, 6-10), SF-12 physical component was 88.1 ± 12.5 (range, 45-100), and SF-12 mental component was 65.3 ± 19.2 (range, 25-100).
Conclusion:
Our study demonstrated that, of the 165 professional ballet dancers registered at the Opéra de Paris in September 2024, 18 dancers (11%) had undergone 31 surgeries to treat musculoskeletal injuries and/or pathologies during their professional career. After surgery, the RTD rate was 100%, with dancers reporting little to no pain and excellent physical health, but satisfactory mental scores. High rates of return to dance and good clinical scores are possible in professional ballet dancers who undergo surgeries for musculoskeletal injuries.
Dancers aspiring to join a ballet company must train extensively from an early age to meet the physical, technical, and artistic demands. 25 This results in a high risk of injury, reported to reach 63.9% in a systematic review that included 21 studies on amateur and professional ballet dancers. 26
Although a number of studies have reported the incidence of musculoskeletal injuries and pathologies in professional ballet dancers,2,11,16,23-25 few studies evaluated return to dance after surgical treatment. Several articles evaluated outcomes after specific surgeries, such as total hip arthroplasty (THA),21,22 hip arthroscopy, 5 and flexor hallucis longus tendon release.7,12,14 However, there is little published regarding the types of surgeries that professional ballet dancers often undergo, as well as their rates of return to dance and clinical outcomes.
The purpose of the present study was to describe the surgical procedures undergone by professional ballet dancers to treat musculoskeletal injuries and/or pathologies and to report the rate and time to return to dance after surgery. The hypothesis was that most dancers would be able to return to dance after surgery.
Methods
Study Design and Participants
The records of all professional ballet dancers registered at the Opéra de Paris in September 2024 were reviewed to identify dancers who had undergone 1 or more surgical procedures (excluding infiltrations and injections) to treat a musculoskeletal injury and/or pathology, whether dance related or not. The Opéra de Paris is a hierarchical ballet company, with each dancer assigned a rank. Quadrille, coryphée, and sujet make up the corps de ballet, who typically perform as an ensemble, with sujet being the most experienced and sometimes performing featured solo roles. Premier danseur (principal dancer) have major leading roles consistently; finally, etoile (star dancer) are often the most senior, and perform the most prestigious roles. Of note, all dancers registered at the Opéra de Paris have social security, as well as personal health insurance provided by the institution; therefore, the dancers’ medical costs and time from work were covered in all cases. Dancers provided informed consent for their data to be used for research and publication purposes, and research was carried out in accordance with the Declaration of Helsinki. This study was approved by the institutional review board of GCS Ramsay Santé pour l’Enseignement et la Recherche (IRB COS-RGDS-2022-02-001-NOGIER-A).
Data Collection and Outcome Assessment
The following information was extracted from the medical records of each dancer: age, sex, weight, height, description of musculoskeletal injuries and/or pathologies, and surgical procedures from the start of their professional career. The surgical data were saved in the dancers’ medical records by the doctor at the Opéra de Paris but contained the original surgical report from the hospital where each dancer was operated on. Furthermore, each dancer was contacted and asked to complete a questionnaire, including information regarding return to dance, pain at the operated site on the numeric rating scale (NRS), satisfaction with surgery on the NRS, University of California–Los Angeles (UCLA) activity score, and 12-item Short-Form Health Survey (SF-12).
Data Analysis
Descriptive statistics were used to summarize the data. Analyses were conducted using R version 3.6.1 (R Foundation for Statistical Computing).
Results
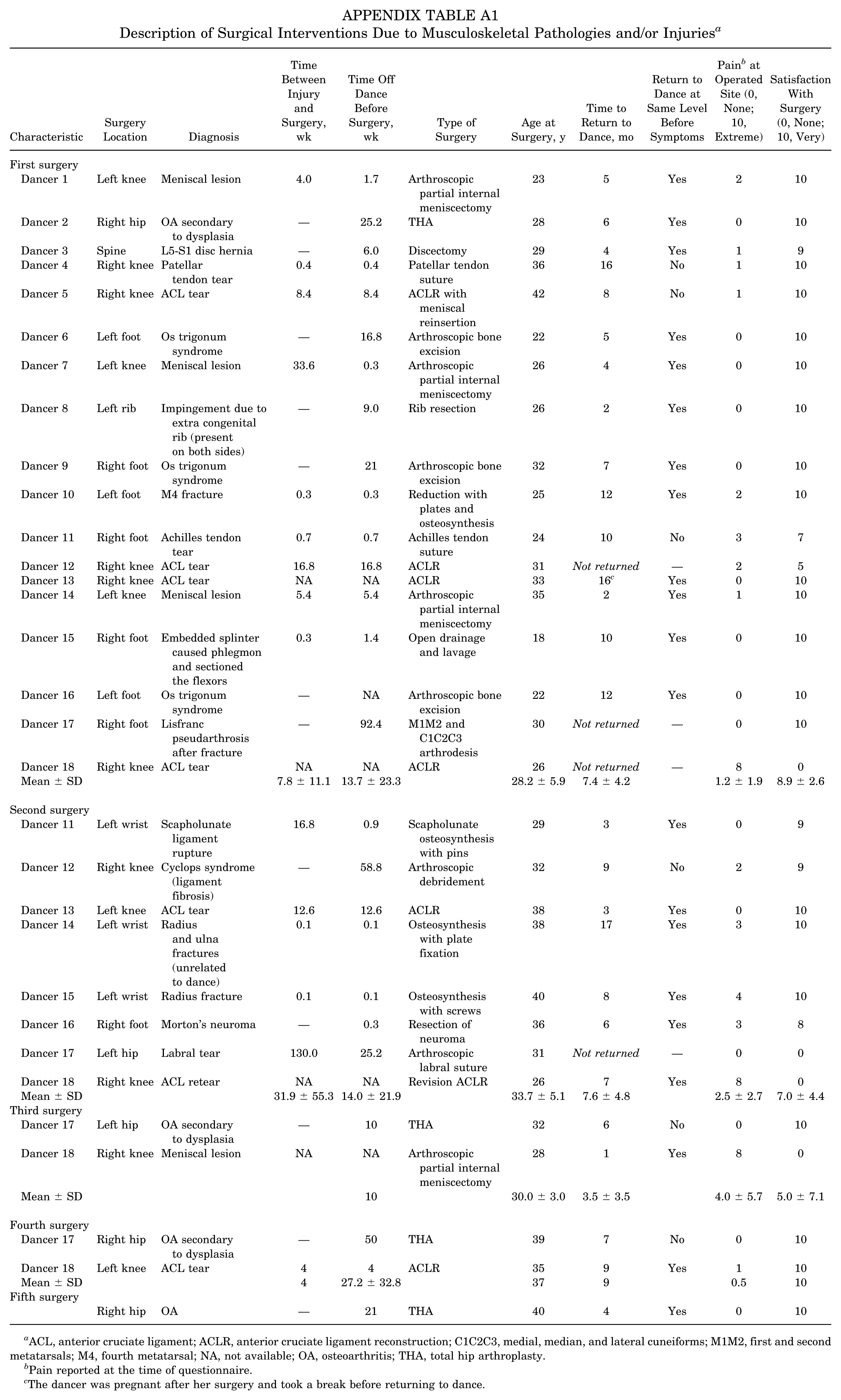
Of 165 registered professional ballet dancers, 18 had undergone at least 1 surgery during their professional career. The 18 registered professional ballet dancers, comprising 11 women and 7 men, had undergone a total of 31 surgeries (only 1 unrelated to dance) (Table 1). Ten dancers had undergone 1 surgery, 6 dancers had undergone 2 surgeries, 1 dancer had undergone 4 surgeries, and 1 dancer had undergone 5 surgeries. At the time of surgery, the mean age of dancers was 30.7 ± 6.2 years (range, 18-42) (Appendix Table A1). The mean time between injury and surgery for dancers with acute injuries was 15.6 ± 33.0 weeks (range, 0.1-130.0 weeks), while the mean time off dance before surgery was 15.0 ± 21.8 weeks (range, 0.1-92.4). The 31 surgeries comprised the following:
13 knee procedures, including 7 anterior cruciate ligament (ACL) reconstructions (6 primary and 1 revision), 4 meniscectomies, 1 ACL debridement due to cyclops syndrome, and 1 patellar tendon suture
8 foot/ankle procedures, including 3 os trigonum excisions, 1 Achilles tendon suture, 1 reduction and osteosynthesis of the fourth metatarsal due to fracture, 1 arthrodesis of the metatarsals and cuneiforms due to Lisfranc pseudarthrosis after a fracture, 1 open drainage and lavage due to phlegmon formation from an embedded splinter, and 1 resection of Morton's neuroma in the foot
5 hip procedures, including 4 THAs and 1 labral suture
3 hand/wrist procedures, including 1 osteosynthesis of the scaphoid and lunate bones due to scapholunate ligament rupture, 1 osteosynthesis of the radius and ulna due to fracture (unrelated to dance, bicycle fall), and 1 osteosynthesis of the radius due to fracture
2 thoracolumbar procedures, including 1 rib resection due to impingement and 1 lumbar discectomy
Dancer Characteristics a

Characteristics reported at the time of the questionnaire. BMI, body mass index.
Rank: Quadrille, coryphée, and sujet make up the corps de ballet, who typically perform as an ensemble, with sujet being the most experienced and sometimes performing featured solo roles. Premier danseur (principal dancer) have major leading roles consistently; finally, etoile (star dancer) are often the most senior, and perform the most prestigious roles.
All 18 dancers eventually returned to dance (100%) at 7 ± 4 months (range, 1-17 months) (Appendix Table A1). However, it is important to note that 3 of the dancers who had >1 surgery were unable to return to dance after their first or second surgery but did so after their second or third surgery. Furthermore, 14 of the 18 dancers eventually (after 1 or more surgeries) were able to return to dance at the same level as before symptoms. For each of the 31 surgical procedures, the questionnaires administered at 83 ± 67 months follow-up (range, 11-305 months) indicated pain at the operated site of 1.6 ± 2.4 (range, 0-8) and satisfaction with surgery of 8.3 ± 3.4 (range, 0-10). The UCLA activity score was 9.1 ± 1.5 (range, 6-10), the SF-12 physical component was 88.1 ± 12.5 (range, 45-100), and the SF-12 mental component was 65.3 ± 19.2 (range, 25-100) (Table 2).
Description of Clinical Outcomes After Surgery a

SF-12, 12-item Short-Form Health Survey; UCLA, University of California–Los Angeles.
Of the 18 dancers, 8 had undergone >1 surgery, and only 3 of these had undergone >1 surgery at the same location:
Dancer 12 had 2 ipsilateral knee procedures: primary ACL reconstruction and then debridement of the ACL due to cyclops syndrome. This dancer did not return to dance after her primary ACL reconstruction but did after debridement.
Dancer 17 had 2 ipsilateral hip procedures: left hip labral suture, followed by left hip THA due to coxarthrosis secondary to dysplasia. This dancer did not return to dance after her labral suture but did return after THA. It is worth noting that this dancer underwent a total of 4 surgeries: first arthrodesis of the right foot metatarsals and cuneiforms due to Lisfranc pseudarthrosis and then the 2 left hip procedures, followed by right hip THA.
Dancer 18 had 3 ipsilateral knee procedures: right knee primary ACL reconstruction and then revision ACL reconstruction, followed by meniscectomy. This dancer did not return to dance after her primary ACL reconstruction but did return after revision ACL reconstruction. It is worth noting that this dancer underwent a total of 5 surgeries. After the 3 right knee surgeries, she underwent left knee primary ACL reconstruction, followed by right hip THA due to coxarthrosis.
Discussion
The major findings of our study revealed that, of 165 professional ballet dancers registered at the Opéra de Paris in September 2024, 18 dancers (11%) had undergone 31 surgeries to treat musculoskeletal injuries and/or pathologies during their professional career. All 18 dancers were able to return to dance after surgery (100%), thus confirming our hypothesis, although some required >1 surgery before returning to dance. Furthermore, 14 of the 18 dancers eventually (after 1 or more surgeries) were able to return to dance at the same level as before symptoms. At final follow-up, the dancers had little to no pain at the operated site, were very satisfied with the surgery, and had excellent UCLA activity scores. Interestingly, although the SF-12 physical component scores were good, the SF-12 mental component scores tended to be lower.
The present study found that the most commonly operated site was the knee (n = 12), followed by the foot/ankle (n = 8) and the hip (n = 5). A previous study 2 reporting on injuries in professional ballet dancers registered at the Opéra de Paris found that the most commonly injured site was the foot/ankle (n = 201), followed by the knee (n = 72), lower leg (n = 67), lumbar spine (n = 51), thigh (n = 49), and hip (n = 48). This suggests that although the foot/ankle is more often injured, knee injuries are more severe, requiring surgery more often. Similarly, the hip was the sixth most commonly injured site but the third most commonly operated site. This could be explained by the fact that during the study period there were no preventive measures implemented at the Opéra de Paris to reduce the likelihood of injuries in dancers. We therefore hope that this distribution may be different in the future, now that preventive strategies have been introduced. These findings are not necessarily in agreement with the literature on surgical interventions in ballet dancers, which reports many cases of foot/ankle surgeries, including os trigonum excisions1,8,15,19,27 and several cases of THA,21,22 but few cases of ACL reconstructions. 17
The rate of return to dance after surgery in the present cohort was 100%. This rate is at the high end of previously reported rates in the literature, which ranged from 50% to 100%.1,8,15,17,19,21,22,27 However, it is difficult to directly compare rates of return to dance across studies because the surgical interventions varied widely. Three of the 18 dancers underwent THA, and all 3 returned to dance at a professional level, which is an excellent result. Few published studies have evaluated outcomes of THA in dancers, with most being case reports, and return-to-dance rates varying from 70% to 100%, although in most cases, dancers did not return to professional dance after surgery.4,13,18,20,22 The largest published cohort on professional ballet dancers undergoing THA, which evaluated 23 current or former professional ballet dancers who actively danced before THA, reported that 16 returned to ballet dance, 3 resumed other types of dance, and 3 did not resume dance at all. 22 Furthermore, Buyls et al 4 reported pain relief and return to dance in 9 dancers but stated that most were disappointed with the prolonged rehabilitation period.
After surgery, dancers in the present study had little to no pain at the operated site, were very satisfied with surgery, had excellent UCLA activity scores, and had good SF-12 physical component scores. Nonetheless, it is worth noting that the SF-12 mental component scores were considerably lower than the physical component scores (65.3 ± 19.2 vs 88.1 ± 12.5). Because this study was retrospective and the SF-12 scores were not assessed before surgery, the net change in scores cannot be calculated. It is possible that the mental component was already worse than the physical component presurgery, as several studies have shown that ballet dancers are prone to mental health problems, with rates of depression reported as high as 25%.6,9,10 The Opéra de Paris hired a psychologist in 2020 to support ballet dancers with both sports-related (professional) and personal mental health issues, although it is not obligatory for dancers to seek appointments with her.
The present retrospective study has a number of limitations. First, the Opéra de Paris does not systematically collect joint pain levels and SF-12 scores for each dancer. Collecting these data at different time points of the year (such as at the start, middle, and end of the season) could provide the medical director with interesting information regarding the trends in pain levels, as well as physical and mental well-being. Furthermore, these data could be used to compare pre- and postoperative scores. Second, a questionnaire was sent only to the 18 dancers who had undergone surgery. Therefore, factors associated with the risk of surgery, as well as differences in pain levels, physical well-being, and mental well-being between injured and noninjured dancers, could not be assessed. Third, all types of surgical procedures were included in the study, which makes the cohort heterogeneous. For this reason, the questionnaire did not include joint-specific clinical scores, such as the Oxford hip score after THA or the International Knee Documentation Committee (IKDC) score after ACL reconstruction. No subgroup analyses were performed to evaluate differences across surgical interventions due to the small cohort size. Fourth, dancers were asked via a questionnaire how long it had taken for them to return to dance after surgery, and in some cases, the questionnaires were administered years after the surgery. To confirm the accuracy of these data, the information recorded by the medical director in the medical files was checked. Furthermore, the questionnaire included the UCLA activity score, which may not have been as pertinent when including only professional ballet dancers. Instead, a dance-specific questionnaire such as the Dance Functional Outcome Survey 3 should be used. Fifth, 9 of the 31 surgeries (29%) reported in the present study occurred in 2 dancers. Furthermore, the cohort comprised only 18 dancers, although it is important to note that all dancers registered at the Opéra de Paris who underwent at least 1 surgery were included in the study. With such a small cohort and a considerable proportion of data coming from just 2 dancers, the findings in this study may not be generalizable.
Conclusion
Our study demonstrated that, of the 165 professional ballet dancers registered at the Opéra de Paris in September 2024, 18 dancers (11%) had undergone 31 surgeries to treat musculoskeletal injuries and/or pathologies during their professional career. After surgery, the return-to-dance rate was 100%, with dancers reporting little to no pain and excellent physical health but satisfactory mental scores. High rates of return to dance and good clinical scores are possible in professional ballet dancers who undergo surgeries for musculoskeletal injuries.
Footnotes
Appendix
Description of Surgical Interventions Due to Musculoskeletal Pathologies and/or Injuries a
| Characteristic | Surgery Location | Diagnosis | Time Between Injury and Surgery, wk | Time Off Dance Before Surgery, wk | Type of Surgery | Age at Surgery, y | Time to Return to Dance, mo | Return to Dance at Same Level Before Symptoms | Pain b at Operated Site (0, None; 10, Extreme) | Satisfaction With Surgery (0, None; 10, Very) |
|---|---|---|---|---|---|---|---|---|---|---|
| First surgery | ||||||||||
| Dancer 1 | Left knee | Meniscal lesion | 4.0 | 1.7 | Arthroscopic partial internal meniscectomy | 23 | 5 | Yes | 2 | 10 |
| Dancer 2 | Right hip | OA secondary to dysplasia | — | 25.2 | THA | 28 | 6 | Yes | 0 | 10 |
| Dancer 3 | Spine | L5-S1 disc hernia | — | 6.0 | Discectomy | 29 | 4 | Yes | 1 | 9 |
| Dancer 4 | Right knee | Patellar tendon tear | 0.4 | 0.4 | Patellar tendon suture | 36 | 16 | No | 1 | 10 |
| Dancer 5 | Right knee | ACL tear | 8.4 | 8.4 | ACLR with meniscal reinsertion | 42 | 8 | No | 1 | 10 |
| Dancer 6 | Left foot | Os trigonum syndrome | — | 16.8 | Arthroscopic bone excision | 22 | 5 | Yes | 0 | 10 |
| Dancer 7 | Left knee | Meniscal lesion | 33.6 | 0.3 | Arthroscopic partial internal meniscectomy | 26 | 4 | Yes | 0 | 10 |
| Dancer 8 | Left rib | Impingement due to extra congenital rib (present on both sides) | — | 9.0 | Rib resection | 26 | 2 | Yes | 0 | 10 |
| Dancer 9 | Right foot | Os trigonum syndrome | — | 21 | Arthroscopic bone excision | 32 | 7 | Yes | 0 | 10 |
| Dancer 10 | Left foot | M4 fracture | 0.3 | 0.3 | Reduction with plates and osteosynthesis | 25 | 12 | Yes | 2 | 10 |
| Dancer 11 | Right foot | Achilles tendon tear | 0.7 | 0.7 | Achilles tendon suture | 24 | 10 | No | 3 | 7 |
| Dancer 12 | Right knee | ACL tear | 16.8 | 16.8 | ACLR | 31 | Not returned | — | 2 | 5 |
| Dancer 13 | Right knee | ACL tear | NA | NA | ACLR | 33 | 16 c | Yes | 0 | 10 |
| Dancer 14 | Left knee | Meniscal lesion | 5.4 | 5.4 | Arthroscopic partial internal meniscectomy | 35 | 2 | Yes | 1 | 10 |
| Dancer 15 | Right foot | Embedded splinter caused phlegmon and sectioned the flexors | 0.3 | 1.4 | Open drainage and lavage | 18 | 10 | Yes | 0 | 10 |
| Dancer 16 | Left foot | Os trigonum syndrome | — | NA | Arthroscopic bone excision | 22 | 12 | Yes | 0 | 10 |
| Dancer 17 | Right foot | Lisfranc pseudarthrosis after fracture | — | 92.4 | M1M2 and C1C2C3 arthrodesis | 30 | Not returned | — | 0 | 10 |
| Dancer 18 | Right knee | ACL tear | NA | NA | ACLR | 26 | Not returned | — | 8 | 0 |
| Mean ± SD | 7.8 ± 11.1 | 13.7 ± 23.3 | 28.2 ± 5.9 | 7.4 ± 4.2 | 1.2 ± 1.9 | 8.9 ± 2.6 | ||||
| Second surgery | ||||||||||
| Dancer 11 | Left wrist | Scapholunate ligament rupture | 16.8 | 0.9 | Scapholunate osteosynthesis with pins | 29 | 3 | Yes | 0 | 9 |
| Dancer 12 | Right knee | Cyclops syndrome (ligament fibrosis) | — | 58.8 | Arthroscopic debridement | 32 | 9 | No | 2 | 9 |
| Dancer 13 | Left knee | ACL tear | 12.6 | 12.6 | ACLR | 38 | 3 | Yes | 0 | 10 |
| Dancer 14 | Left wrist | Radius and ulna fractures (unrelated to dance) | 0.1 | 0.1 | Osteosynthesis with plate fixation | 38 | 17 | Yes | 3 | 10 |
| Dancer 15 | Left wrist | Radius fracture | 0.1 | 0.1 | Osteosynthesis with screws | 40 | 8 | Yes | 4 | 10 |
| Dancer 16 | Right foot | Morton’s neuroma | — | 0.3 | Resection of neuroma | 36 | 6 | Yes | 3 | 8 |
| Dancer 17 | Left hip | Labral tear | 130.0 | 25.2 | Arthroscopic labral suture | 31 | Not returned | — | 0 | 0 |
| Dancer 18 | Right knee | ACL retear | NA | NA | Revision ACLR | 26 | 7 | Yes | 8 | 0 |
| Mean ± SD | 31.9 ± 55.3 | 14.0 ± 21.9 | 33.7 ± 5.1 | 7.6 ± 4.8 | 2.5 ± 2.7 | 7.0 ± 4.4 | ||||
| Third surgery | ||||||||||
| Dancer 17 | Left hip | OA secondary to dysplasia | — | 10 | THA | 32 | 6 | No | 0 | 10 |
| Dancer 18 | Right knee | Meniscal lesion | NA | NA | Arthroscopic partial internal meniscectomy | 28 | 1 | Yes | 8 | 0 |
| Mean ± SD | 10 | 30.0 ± 3.0 | 3.5 ± 3.5 | 4.0 ± 5.7 | 5.0 ± 7.1 | |||||
| Fourth surgery | ||||||||||
| Dancer 17 | Right hip | OA secondary to dysplasia | — | 50 | THA | 39 | 7 | No | 0 | 10 |
| Dancer 18 | Left knee | ACL tear | 4 | 4 | ACLR | 35 | 9 | Yes | 1 | 10 |
| Mean ± SD | 4 | 27.2 ± 32.8 | 37 | 9 | 0.5 | 10 | ||||
| Fifth surgery | ||||||||||
| Right hip | OA | — | 21 | THA | 40 | 4 | Yes | 0 | 10 |
ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; C1C2C3, medial, median, and lateral cuneiforms; M1M2, first and second metatarsals; M4, fourth metatarsal; NA, not available; OA, osteoarthritis; THA, total hip arthroplasty.
Pain reported at the time of questionnaire.
The dancer was pregnant after her surgery and took a break before returning to dance.
Final revision submitted September 24, 2025; accepted October 19, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: Clinique Trenel provided funding for data analysis and manuscript writing. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from GCS Ramsay Santé pour l’Enseignement et la Recherche (IRB COS-RGDS-2022-02-001-NOGIER-A).