
Abstract
Background:
Hip flexor tightness is common in ice hockey players because of postural demands. It remains unknown whether hip tightness plays a role in the occurrence of low back pain (LBP).
Hypothesis:
It was hypothesized that ice hockey players with hip flexor tightness would be at increased risk of developing LBP.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Preseason hip flexor tightness was measured annually for 4 seasons in a boy's high school team, a college men's team, and a college women's team providing a total of 289 player-seasons. A digital level was placed on the anterior thigh during the Thomas test. “Tight” was defined as a Thomas test >5° above horizontal with the remaining players defined as normal. Game and practice injuries with associated time loss and diagnosis were recorded. LBP was defined as an injury in the lumbar region requiring the player to miss ≥1 game or >2 practices. Prevalence and incidence of LBP were compared between players with tight versus normal hip flexor flexibility, and relative risks were computed. Additionally, hip flexion abduction and adduction strength was assessed with a handheld dynamometer. Incidence and prevalence of LBP was compared between weak, average, and strong players within each team.
Results:
There were 33 cases of LBP resulting in 97 missed games and 377 missed practices. The incidence of LBP was 1.02/1000 athlete-exposures (95% CI 0.72-1.43). Of 172 players with hip flexor tightness, 27 (15.7%) developed LBP compared with 6 of 117 (5.1%) with normal flexibility (P = .006). LBP incidence was higher for players with tight (1.42; 95% CI, 0.98-2.06) versus normal (0.55; 95% CI, 0.21-0.98) hip flexor flexibility (relative risk, 3.17; 95% CI, 1.31-7.67; P = .007). Players with hip flexor tightness missed 85 games and 318 practices because of LBP compared with 12 games and 59 practices for players with normal hip flexor flexibility (P < .001). LBP incidence was not different between teams (P = .91). Incidence of LBP was not different between players weak, average, or strong in hip flexion (P = .53), abduction (P = .48) or adduction (P = .35).
Conclusion:
Hip flexor tightness was associated with increased risk of LBP. Hip flexor stretching and postural training is indicated for players with hip flexor tightness.
Ice hockey is a demanding, high-intensity sport that places significant stress on the musculoskeletal system, particularly the lumbar spine. Ice hockey players are consistently subjected to repetitive movements in a hip flexed posture with rapid changes in direction and then they return to the bench to sit in a similar hip flexed posture. These factors can contribute to the development of shortened hip flexors and may predispose ice hockey players to low back pain (LBP). 20
Ice hockey players have a high prevalence of LBP.5-7,16 Compared with soccer or floorball (an indoor hard floor derivative of ice hockey played in rubber-soled footwear), ice hockey players have a 2.18 times increased risk of developing LBP. 6 The unique physical demands and musculoskeletal adaptations to ice hockey may predispose players to back injuries.5,6,15 The prevalence and incidence of LBP in ice hockey players has been studied exclusively in male players. However, female players are exposed to the same performance demands as male players and may have a similar risk of LBP.
The Thomas test, first described by Hugh Owen Thomas in 1876 18 to diagnose inflammation of the hip joint, is the most common test of hip flexor tightness. Hip flexor stretching improves Thomas test range of motion (ROM) in patients with LBP 22 and patellofemoral pain syndrome. 21 Thomas test ROM also improves with a psoas nerve block in patients with hip flexor spasticity. 9 Hip flexor stretching in patients with LBP and lumbar hyperlordosis provided symptom relief, reduced lordosis, and improved Thomas test ROM. 11
An association between hip flexor tightness and LBP has been reported in several studies.3,8,13 Patients with chronic LBP had markedly greater hip flexor tightness, measured by the Thomas test, compared with healthy controls. 3 A positive Thomas test (tight) was more prevalent in baseball players with previous LBP compared with players with no previous LBP. 8 Similarly, a positive Thomas test (tight) was more prevalent in adolescent volleyball players with previous LBP compared with players with no previous LBP. 13
Hip flexor tightness has been documented in professional hockey players. 20 Hip strength is routinely measured in hockey players, but it is not known if there is an association between hip strength and flexibility and whether this affects LBP risk.
Given the hip-flexed postural demands of ice hockey and the documented hip flexor tightness in ice hockey players, the purpose of this study was to test the hypothesis proposed by Tyler et al 20 that hip flexor tightness predisposes ice hockey players to LBP. Additionally, the association between hip flexor tightness and weakness and the role of hip strength in risk of developing LBP were examined.
Methods
Study Sample
Players from a boys’ high school team, a women's college team, and a men's college team (National Collegiate Athletic Association Division III) were followed for 4 seasons each. A total of 161 players were followed (54 high school, 47 college women, 60 college men). Of these 161 players, 2 were followed for 4 consecutive seasons, 34 were followed for 3 seasons, 54 for 2 seasons, and 71 for 1 season for a total of 289 player-seasons. At the time of preseason testing, ages were mean ± SD 16.2 ± 1.0 years for high school, 20.4 ± 1.6 years for college women, and 22.4 ± 1.4 years for college men. Body mass was 71.2 ± 10.5 kg for high school, 66.6 ± 9.6 kg for college women, and 86.1 ± 9.1 kg for college men. Height was 1.77 ± 0.06 m for high school, 1.65 ± 0.08 m for college women, and 1.83 ± 0.07 m for college men. Age, body mass, and height differed significantly between each team (P < .01). The study received ethical and player approval (and legal guardians where necessary gave informed consent).
Procedures
All players completed preseason screening each year for measurement of hip flexor flexibility (Thomas test) and hip flexion, abduction, and adduction strength. All players were required to be injury-free and cleared for full participation at the time of preseason screening.
During the season, the number of games and practices were recorded with missed games and practices logged. This enabled an accurate measure of exposure. LBP that resulted in any missed game or practice was recorded and the total number of games and practices missed due to LBP were also recorded for each player. LBP was defined as an injury in the lumbar region requiring the player to miss ≥1 game or >2 practices.
For the Thomas test, each player was placed supine with the lumbar spine at the end of the treatment table and with the knees flexed to the chest. The examiner (T.F.T.) slowly lowered the test leg while holding the contralateral leg in the knee to chest position (Figure 1). With the test leg hanging in a relaxed position, a second examiner aligned a digital level with the femur on the lateral aspect of the thigh and the angle was recorded relative to the horizontal (negative being above horizontal and positive below horizontal). Care was taken to ensure that the lumbar spine remained in contact with the table during testing to prevent anterior pelvic tilt. The measurement was then repeated on the contralateral leg. The same examiner (T.F.T.), who had >20 years clinical experience in hockey making this measurement on a routine basis, made all Thomas test measures each season. The digital level displayed angles to one decimal place. Angles were recorded to the nearest whole degree. It was anticipated that most players would have a Thomas test above horizontal given the postural demands of hockey and the previously reported hip flexor tightness in professional hockey players using a modified Thomas test. 20 Therefore, Thomas tests were classified as tight (thigh ≥5° above horizontal) or normal. Any player with either leg classified as tight was categorized as having tight hip flexors.

Thomas test measurement of hip flexor tightness.
Strength measures were made by the same tester (M.P.M.) using a handheld dynamometer (Lafayette Manual Muscle Tester; Lafayette Instruments) as previously described. 12 This tester made all strength measures each season and had >20 years’ experience making these measurements in hockey players. Hip flexion strength was tested in the seated position with the dynamometer placed just proximal to the patella. The hip was flexed, with the knee flexed in a relaxed position. The examiner applied resistance against hip flexion until the patient's contraction was overcome (break test). Hip abduction strength was tested in a side-lying position with the dynamometer placed just proximal to the lateral malleolus. The hip was abducted approximately 30°, and a break test was applied. Hip adduction strength was tested in a side-lying position with the hip adducted approximately 15°. The dynamometer was placed just proximal to the medial malleolus, and the break test was applied. Force values were converted to torque and expressed relative to body mass (N·m/kg). The lever arm for abduction and adduction was defined as the distance from the greater trochanter to the lateral malleolus. The lever arm for hip flexion was defined as the distance from the greater trochanter to the lateral femoral condyle. For each of the 3 strength tests, players within each team were categorized as strong, average, or weak based on within-team z scores (strong = z score >0.50; weak = z score <-0.50).
Statistical Analysis
Incidence of LBP was calculated and reported as injuries per 1000 exposures (games plus practices) with 95% CIs. Chi-square analyses were used to compare LBP incidences between the 3 teams, between players with tight versus normal hip flexors, and between players with strong, average, and weak hip strength (chi-square linear trend for comparison of strength groups). Relative risks (RRs) with 95% CIs are reported for analyses with significant chi-square analysis. The number of missed games per 1000 games and number of missed practices per 1000 practices are reported with 95% CIs if LBP incidence differed between groups. Descriptive data for continuous variables are reported as mean ± SD with normality of distribution tested by Shapiro-Wilk tests (data were normally distributed unless noted in the Results section). One-way analysis of variance was used to compare strength tests between teams with Bonferroni corrections for pairwise comparisons.
Results
There were 33 cases of LBP resulting in 97 missed games and 377 missed practices. The incidence of LBP was 1.02/1000 athlete-exposures (95% CI, 0.72-1.43). LBP incidence was not different between teams (P = .91) (Table 1) or playing positions (P = .91).
Prevalence and Incidence of LBP a

Data are presented as n, n (%), or injuries/1000 athlete-exposures (95% CI). Comparison of LBP prevalence between teams: chi-square, P = .34; comparison of LBP incidence between teams: chi-square, P = .91. LBP, low back pain.
Games and practices missed due to LBP.
The Thomas test results for the whole study sample (N = 289) was 4°± 7° above the horizontal but was not normally distributed (Shapiro-Wilk test statistic, 0.985; P = .004). A total of 172 players were classified as having hip flexor tightness (60%); 109 had bilateral tightness, and 63 had unilateral tightness. The prevalence of hip flexor tightness was not different between teams (P = .87) with 59% of college women, 59% of college men, and 60% of high school boys having tight hip flexors.
Of 172 players with hip flexor tightness, 27 developed LBP (15.7%) compared with 6 of 117 (5.1%) with normal flexibility (P = .006) (Table 2). LBP incidence was higher for players with tight versus normal hip flexor flexibility (RR, 3.17; 1.31-7.67; P = .007) (Table 2). Players with hip flexor tightness missed 85 games and 318 practices due to LBP compared with 12 games and 59 practices for players with normal hip flexor flexibility; missed games due to LBP per 1000 games and missed practices due to LBP per 1000 practices were 5.08 and 3.78 times higher for players with tight hip flexors; P < .001) (Table 2).
Association Between Hip Flexor Tightness and LBP a

Data are presented as n, n (%), or injuries/1000 athlete-exposures (95% CI). LBP, low back pain; RR, relative risk.
Greater prevalence in players with hip flexor tightness (chi-square test, P = .006; RR, 3.06; 95% CI, 1.30-7.18).
Greater incidence in players with hip flexor tightness (chi-square test with Yates correction, P = .007; RR, 3.17; 95% CI, 1.31-7.67).
More missed games (P < .001; RR, 5.08; 95% CI, 2.78-9.29) and missed practices (P < .001; RR, 3.78; 95% CI, 2.86-4.98) in players with hip flexor tightness.
Hip strength differed significantly between teams (P < .001) with lowest values for college women (hip flexion, 1.52 ± 0.28 Nm/kg; hip abduction, 1.93 ± 0.43 Nm/kg; hip adduction, 1.64 ± 0.40 Nm/kg), intermediate values for high school players (hip flexion, 1.83 ± 0.43 Nm/kg; hip abduction, 2.12 ± 0.54 Nm/kg; hip adduction, 2.12 ± 0.54 Nm/kg), and highest values for college men (hip flexion, 2.11 ± 0.33 Nm/kg; hip abduction, 2.51 ± 0.44 Nm/kg; hip adduction, 2.38 ± 0.42 Nm/kg). Relative strength within each team was not associated with the prevalence or incidence of LBP (Table 3).
Association Between Hip Strength and LBP a

Comparison of LBP incidence between groups; chi-square linear trend, P = .35.
Data are presented as n, n (%), or injuries/1000 athlete-exposures (95% CI). LBP, low back pain.
Hip flexion weakness was associated with hip flexor tightness (chi-square linear association, P = .04): of the 94 players with weak hip flexors, 61 had hip flexor tightness (65%); of the 116 players with average hip flexion strength, 72 had hip flexor tightness (62%); and of the 79 players with strong hip flexors, 39 had hip flexor tightness (49%). Players with a combination of hip flexor tightness and hip flexion weakness (n = 61) did not have a significantly higher incidence of LBP than players without hip flexor tightness who were strong in hip flexion (n = 40; RR, 3.34; 95% CI, 0.74-15.05; P = .12) (Table 4).
Combination of Hip Flexor Flexibility and Hip Flexion Strength on Prevalence and Incidence of LBP a
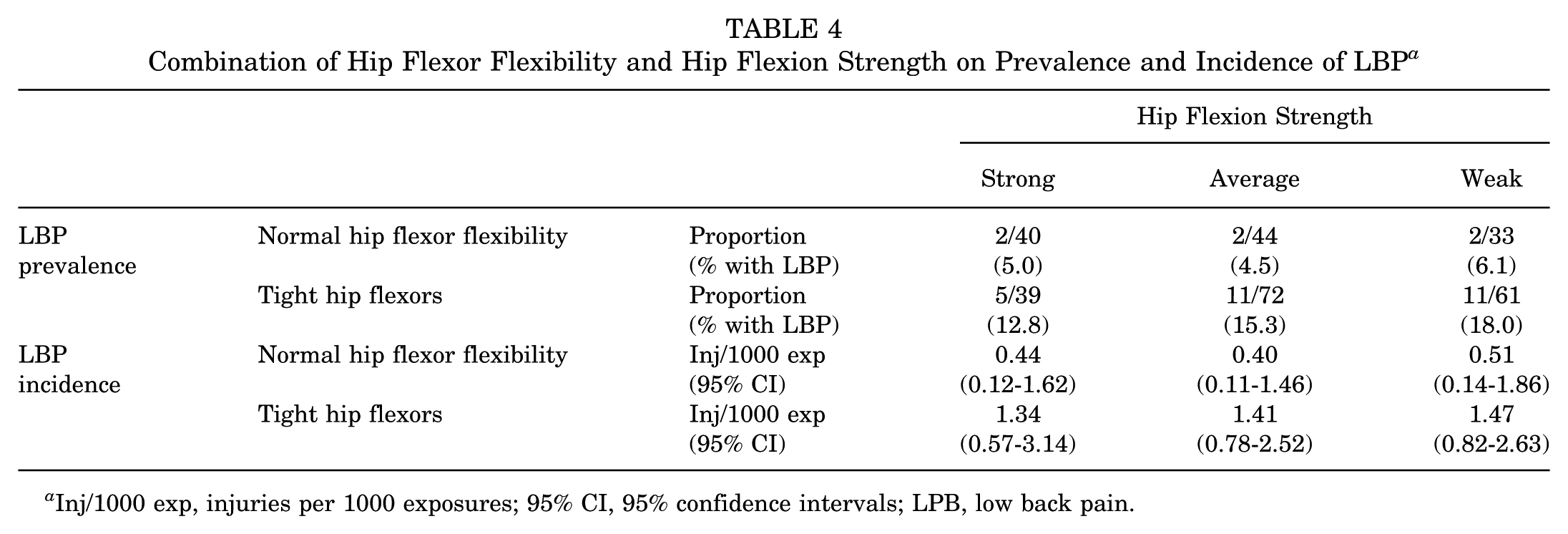
Inj/1000 exp, injuries per 1000 exposures; 95% CI, 95% confidence intervals; LPB, low back pain.
Discussion
Our hypothesized hip flexor tightness was associated with increased risk of LBP in ice hockey players. This effect was independent of sex (college women vs college men) or age (college vs high school). The prevalence and incidence of LBP was similar between the 3 teams, as was the prevalence of hip flexor tightness. Considering that female athletes are generally more flexible than male athletes and have more flexible hip flexors, 10 the similar prevalences of hip flexor tightness and LBP across the 3 teams highlight the effect of the postural demands in ice hockey. Surprisingly there are very limited data on hip flexor flexibility in hockey players. Tyler et al 20 reported professional hockey players having a mean of 0.56° hip extension in the Thomas test compared with 10.08° hip extension for controls. In the present study, the mean was 4° hip flexion. However, Tyler et al 20 used a modified Thomas test. It was performed with the knee in full extension, held in a knee immobilizer, to remove the contribution of the rectus femoris. This creates a much greater limb mass stretch torque due to gravity pushing the leg into extension. Because the traditional Thomas test allows the knee to flex freely, there is a much lower leg mass stretching the leg into extension. This could explain the differences in the findings between studies.
Hip strength was not protective against LBP. The incidence of LBP was not different between strong, average, and weak players for hip flexion strength, hip abduction strength, and hip adduction strength. Of note, hip strength was markedly different between the 3 teams with male college players strongest and female college players weakest. The effect of hip strength on LBP incidence was based on the relative strength of the players within each team (eg, strongest college female players vs weakest college female players, etc). It is possible that strength may play a role in LBP incidence in a sample of hockey players more homogeneous with respect to strength and not differing in age and sex. There was an association between hip flexor tightness and hip flexion weakness; 65% of players weak in hip flexion had hip flexor tightness compared with 49% of players strong in hip flexion. The combination of hip flexion weakness and hip flexor tightness did not compound the risk of LBP, but the sample size was inadequate to definitively assess this relationship. Only 21% of the study sample were classified as weak and tight, with only 14% classified as strong and normal flexibility. Hip flexor tightness was the only significant contributor to LBP risk.
An association between hip flexor tightness and LBP has been reported in adolescent soccer players. 17 Additionally, in these young soccer players hip flexor tightness was associated with lumbar pedicle stress reaction. 17 However, in a subsequent study by the same authors, hip flexor tightness as assessed by the Thomas test was not different between adolescent soccer players with and without lumbar bone stress injury. 19 The postural demands in soccer may not be as stressful on the lumbar spine as in ice hockey. Hockey players spend most of their time on the ice in a forward-flexed position. The forward trunk position in skating brings the center of gravity in front of the body and allows for greater hip motion, thereby increasing forward skating speed. 2 But this also creates a greater torque around the lumbopelvic complex. Repeated bouts of sustained spinal flexion can cause hip flexor shortening and stress the lumbar spine. A 15-year follow-up study comparing spinal changes on magnetic resonance imaging in athletes from 4 different sports found that ice hockey players had the highest prevalence of disc degeneration at follow-up. 1 Importantly, when assessing hip flexor tightness using the Thomas test, it is important to eliminate anterior pelvic tilt during the test to avoid a false negative result; an 11° change in lumbosacral angle (anterior pelvic tilt) changed the Thomas test from 4° hip flexion to 5° hip extension. 20
While a relatively strong association between hip flexor tightness and LBP was found in this study (RR, 3.17), other factors can contribute to LBP in hockey players. In a sample of 25 hockey players with LBP, 44% were diagnosed with spondylolysis, and in 73% of those players the injury occurred on the shooting side. 4 Thoracic spine rotation is associated with wrist shot velocity, and lack of thoracic rotation may increase the stress on the lumbar spine leading to LBP. 14
It remains to be determined if hip flexor stretching can reduce the risk of LBP in ice hockey players. In clinical studies, hip flexor stretching has been effective in improving Thomas test ROM in patients with LBP 22 and patellofemoral pain syndrome. 21 Furthermore, hip flexor stretching in patients with LBP and lumbar hyperlordosis provided symptom relief, reduced lordosis, and improved Thomas test ROM. 11 Based on these clinical studies, it is likely that hip flexor stretching can correct hip flexor tightness. A combination of hip flexor stretching and postural training to avoid lumbar lordosis can possibly reduce the risk of LBP in ice hockey players. Because the Thomas test is easy to administer in preseason screening, it would make sense to screen players to identify those with tight hip flexors, place them on a stretching and postural training program, and assess the subsequent incidence of LBP. However, other contributors to LBP such as thoracic rotation deficits and spondylolysis would be confounding factors that would need to be addressed.
One surprising result was that the college women were not more flexible than the men in the Thomas test. Because women are generally more flexible than men, it would be interesting to compare flexibility in other joints between male and female hockey players.
Limitations
Some limitations in this study include the lack of reliability data on the independent variables and, somewhat related, the potential that some statistically insignificant findings lacked sufficient power. With respect to reliability, the same testers were used year to year for range of motion and strength tests, but the measurement error was not quantified for these measurements in this population. While the overall sample size was quite large (N = 289 player-seasons) the number of LBP injuries was relatively small (n = 33). Consequently, analysis of the combined effects of hip flexor tightness and weakness on LBP risk is likely underpowered. Similarly, the prevalence on LBP varied from 7.8% in high school boys to 14.1% in college women and there was insufficient power to assess if the risk associated with hip flexor tightness varied across teams.
Conclusion
Hip flexor tightness in hockey players was associated with increased risk of developing LBP over the course of a season. This effect was independent of age (high school vs college) and sex (college men vs women). Hip flexor stretching and postural training is recommended for ice hockey players identified with hip flexor tightness in preseason screening.
Footnotes
Final revision submitted November 6, 2025; accepted November 13, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.J.N. has received educational support from Gotham Surgical Solutions & Devices Inc and receives royalties from Arthrex Inc. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Feinstein Institutes of Medical Research, Northwell Health, Human Research Protection Program (No. 20-0649).